
Factors Influencing Disease Stability and Response to Tocilizumab Therapy in Severe COVID-19: A Retrospective Cohort Study



Abstract
:1. Introduction
2. Results
2.1. Demographic, Clinical, and Biochemical Characteristics of the Study Population
2.2. Association between the Demographic, Clinical, and Biochemical Characteristics and COVID-19 Outcomes
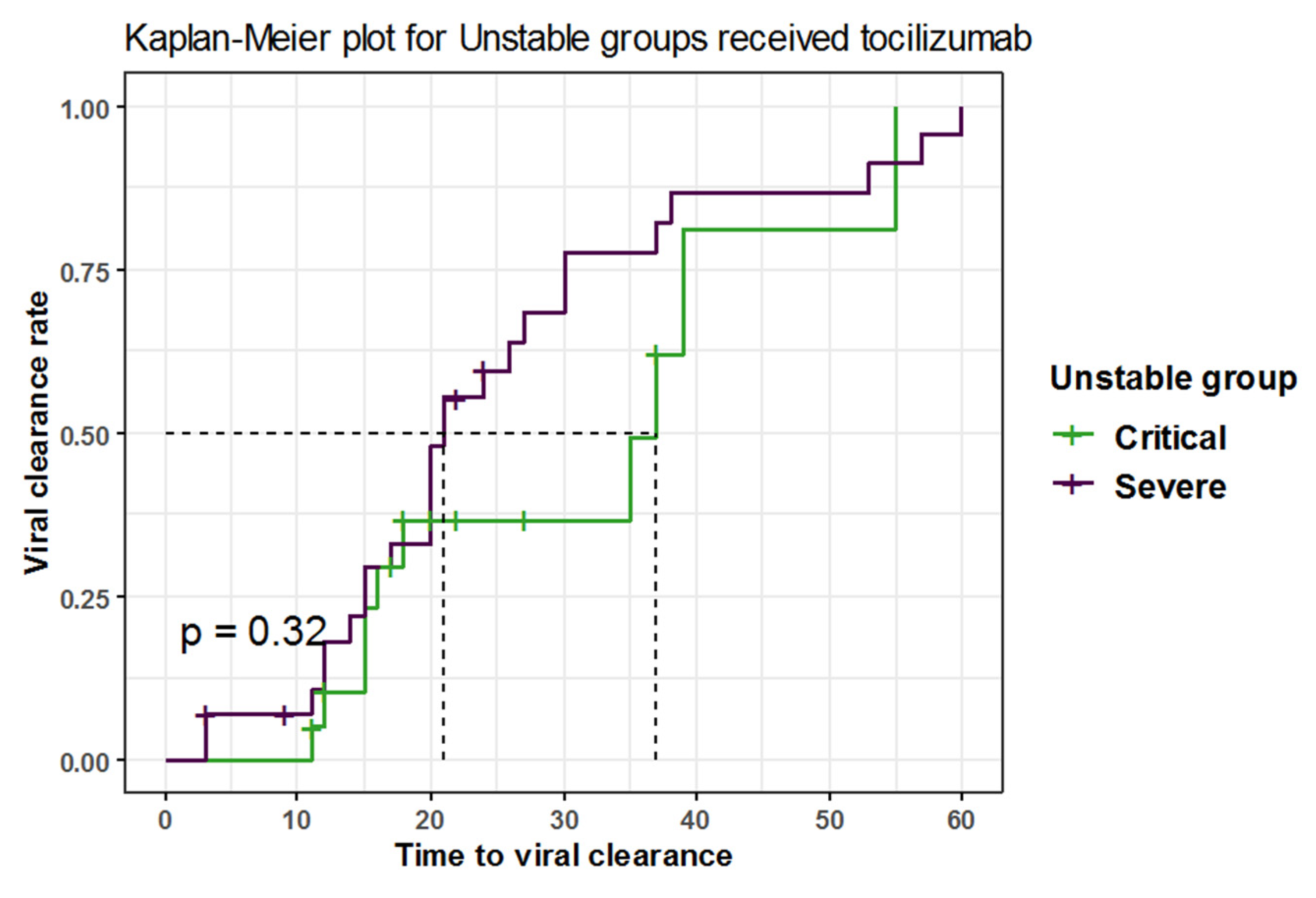
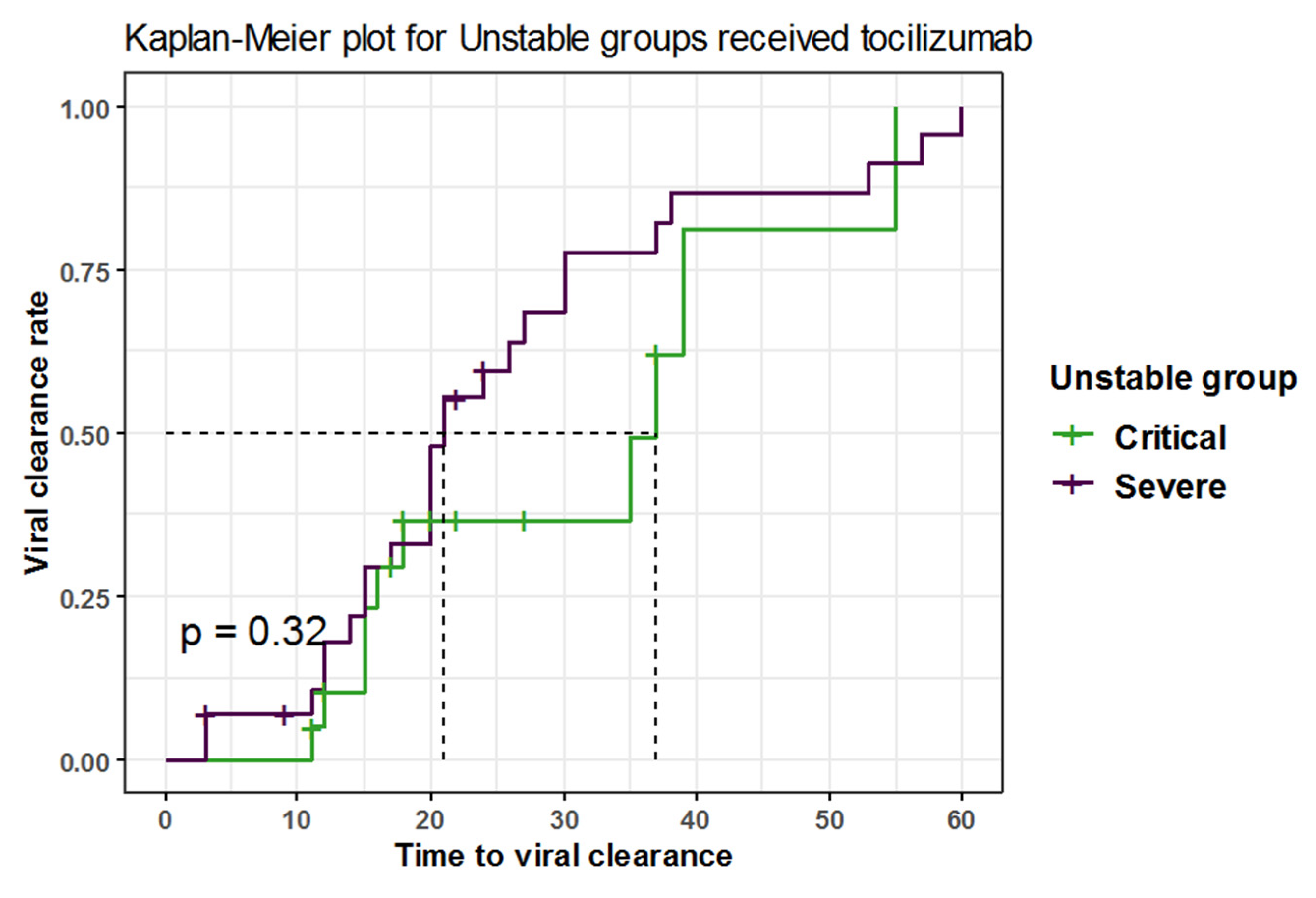
2.3. Time to Viral Clearance among Unstable COVID-19 Patients
2.4. The Effect of Combination of Vitamin D, Anticoagulants, Steroids, and Antivirals with Tocilizumab
2.5. The Rate of Adverse Events Following Tocilizumab in Different Study Groups
3. Discussion
4. Materials and Methods
4.1. Institutional Review Board IRB
4.2. Study Design and Study Population
4.3. Data Management and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. Orig. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Lu, C.C.; Chen, M.Y.; Lee, W.S.; Chang, Y.L. Potential therapeutic agents against COVID-19: What we know so far. J. Chin. Med. Assoc. 2020, 83, 534–536. [Google Scholar] [CrossRef] [PubMed]
- Uciechowski, P.; Dempke, W.C.M. Interleukin-6: A Masterplayer in the Cytokine Network. Oncology 2020, 98, 131–137. [Google Scholar] [CrossRef]
- Norelli, M.; Camisa, B.; Barbiera, G.; Falcone, L.; Purevdorj, A.; Genua, M.; Sanvito, F.; Ponzoni, M.; Doglioni, C.; Cristofori, P.; et al. Monocyte-derived IL-1 and IL-6 are differentially required for cytokine-release syndrome and neurotoxicity due to CAR T cells. Nat. Med. 2018, 24, 739–748. [Google Scholar] [CrossRef]
- Lan, S.H.; Lai, C.C.; Huang, H.T.; Chang, S.P.; Lu, L.C.; Hsueh, P.R. Tocilizumab for severe COVID-19: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2020, 56, 106103. [Google Scholar] [CrossRef]
- Liu, B.; Li, M.; Zhou, Z.; Guan, X.; Xiang, Y. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)? J. Autoimmun. 2020, 111, 102452. [Google Scholar] [CrossRef]
- Luo, P.; Liu, Y.; Qiu, L.; Liu, X.; Liu, D.; Li, J. Tocilizumab treatment in COVID-19: A single center experience. J. Med. Virol. 2020, 92, 814–818. [Google Scholar] [CrossRef]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.-A.; et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, M.; Mannam, P.; Comer, R.; Pharmd, E.S.; Brent, D.; Schmidt Mph, M.L. Off-Label Real World Experience Using Tocilizumab for Patients Hospitalized with COVID-19 Disease in a Regional Community Health System: A Case-Control Study. medRxiv 2020. [Google Scholar] [CrossRef]
- Ortiz-Martínez, Y. Tocilizumab: A new opportunity in the possible therapeutic arsenal against COVID-19. Travel Med. Infect. Dis. 2020, 37, 101678. [Google Scholar] [CrossRef]
- Furlow, B. COVACTA trial raises questions about tocilizumab’s benefit in COVID-19. Lancet. Rheumatol. 2020, 2, e592. [Google Scholar] [CrossRef]
- Abaleke, E.; Abbas, M.; Abbasi, S.; Abbott, A.; Abdelaziz, A.; Abdelbadiee, S.; Abdelfattah, M.; Abdul, B.; Abdul Rasheed, A.; Abdul-Kadir, R.; et al. Azithromycin in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 605–612. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, K.; Wang, D.; Yue, X.; Song, D.; Zhu, Y.; Wu, J. Nucleocapsid protein of SARS-CoV activates interleukin-6 expression through cellular transcription factor NF-kappaB. Virology 2007, 365, 324–335. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Michot, J.M.; Albiges, L.; Chaput, N.; Saada, V.; Pommeret, F.; Griscelli, F.; Balleyguier, C.; Besse, B.; Marabelle, A.; Netzer, F.; et al. Tocilizumab, an anti-IL-6 receptor antibody, to treat COVID-19-related respiratory failure: A case report. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 961–964. [Google Scholar] [CrossRef]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V.; et al. Tocilizumab in patients with severe COVID-19: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e474–e484. [Google Scholar] [CrossRef]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Remap-Cap Investigators. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Paño-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2022, 28, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Rossotti, R.; Travi, G.; Ughi, N.; Corradin, M.; Baiguera, C.; Fumagalli, R.; Bottiroli, M.; Mondino, M.; Merli, M.; Bellone, A.; et al. Safety and efficacy of anti-il6-receptor tocilizumab use in severe and critical patients affected by coronavirus disease 2019: A comparative analysis. J. Infect. 2020, 81, e11–e17. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Nugroho, C.W.; Suryantoro, S.D.; Yuliasih, Y.; Rosyid, A.N.; Asmarawati, T.P.; Andrianto, L.; Setiawan, H.W.; Mahdi, B.A.; Windradi, C.; Agustin, E.D.; et al. Optimal use of tocilizumab for severe and critical COVID-19: A systematic review and meta-analysis. F1000Research 2021, 10, 73. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID - 19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Rubini, A. Interleukin-6 and lung inflammation: Evidence for a causative role in inducing respiratory system resistance increments. Inflamm. Allergy Drug Targets 2013, 12, 315–321. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Vale, C.L.; Godolphin, P.J.; Fisher, D.; Higgins, J.P.T.; Spiga, F.; Savović, J.; Tierney, J.; Baron, G.; Benbenishty, J.S.; et al. Association Between Administration of IL-6 Antagonists and Mortality Among Patients Hospitalized for COVID-19: A Meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar] [CrossRef]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef]
- Munshi, R.; Hussein, M.H.; Toraih, E.A.; Elshazli, R.M.; Jardak, C.; Sultana, N.; Youssef, M.R.; Omar, M.; Attia, A.S.; Fawzy, M.S.; et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J. Med. Virol. 2021, 93, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Adamo, M.; Lupi, L.; Cani, D.S.; Di Pasquale, M.; Tomasoni, D.; Italia, L.; Zaccone, G.; Tedino, C.; Fabbricatore, D.; et al. Characteristics and outcomes of patients hospitalized for COVID-19 and cardiac disease in Northern Italy. Eur. Heart J. 2020, 41, 1821–1829. [Google Scholar] [CrossRef] [PubMed]
- Apea, V.J.; Wan, Y.I.; Dhairyawan, R.; Puthucheary, Z.A.; Pearse, R.M.; Orkin, C.M.; Prowle, J.R. Ethnicity and outcomes in patients hospitalised with COVID-19 infection in East London: An observational cohort study. BMJ Open 2021, 11, e042140. [Google Scholar] [CrossRef] [PubMed]
- Oliynyk, O.; Barg, W.; Oliynyk, Y.; Dubrov, S.; Gurianov, V.; Rorat, M. Lack of Difference in Tocilizumab Efficacy in the Treatment of Severe COVID-19 Caused by Different SARS-CoV-2 Variants. J. Pers. Med. 2022, 12, 1103. [Google Scholar] [CrossRef]
- Clinical Managment of COVID-19—Intterim Guidance. 2020. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiD8On8jID3AhVDXRoKHcrIBOgQFnoECAsQAQ&url=https%3A%2F%2Fapps.who.int%2Firis%2Fbitstream%2Fhandle%2F10665%2F332196%2FWHO-2019-nCoV-clinical-2020.5-eng.pdf&usg=AOvVaw3KM (accessed on 25 April 2022).


{kind=link}
{kind=link}
| Baseline Characteristics | Not Received Tocilizumab N = 21 | Received Tocilizumab N = 49 | p Value | |
|---|---|---|---|---|
| Demographic | ||||
| Age (years) | Mean ± SD | 47.0 ± 9.0 | 50.2 ± 13.3 | 0.362 |
| Gender | Female | 3 (27.3%) | 8 (72.7%) | 1.00 |
| Male | 18 (30.5%) | 41 (69.5%) | ||
| Race | Asian | 19 (38.0%) | 31 (62.0%) | 0.066 |
| Black | 0 (0.0%) | 2 (100.0%) | ||
| White | 2 (11.1%) | 16 (88.9%) | ||
| BMI | Mean ± SD | 29.0 ±5.4 | 30.3 ± 6.5 | 0.401 |
| Clinical | ||||
| HTN | No | 11 (28.9%) | 27 (71.1%) | 0.536 |
| Yes | 4 (18.2%) | 18 (81.8%) | ||
| DM | No | 14 (34.1%) | 27 (65.9%) | 0.804 |
| Yes | 7 (28.0%) | 18 (72.0%) | ||
| CVS | No | 21 (38.2%) | 34 (61.8%) | 0.025 |
| Yes | 0 (0.0%) | 9 (100.0%) | ||
| Biochemical | ||||
| WBC | Mean ± SD | 7.6 ± 2.3 | 6.8 ± 3.9 | 0.015 |
| HEMOGLOBIN | Mean ± SD | 13.3 ± 1.6 | 13.1 ± 1.9 | 0.682 |
| PLATELETS | Mean ± SD | 427.0 ± 210.9 | 307.4 ± 135.2 | 0.036 |
| CRP | Mean ± SD | 114.0 ± 48.5 | 135.6 ± 107.1 | 0.827 |
| D.DIMER | Mean ± SD | 1.0 ± 0.5 | 8.9 ± 10.2 | <0.001 |
| IL6 | Mean ± SD | 51.4 ± 35.0 | 961.4 ± 1162.9 | 0.03 |
| LDH | Mean ± SD | 445.7 ± 141.8 | 641.3 ± 577.3 | 0.223 |
| ALT | Mean ± SD | 63.7 ± 28.3 | 62.7 ± 81.9 | 0.058 |
| AST | Mean ± SD | 70.7 ± 41.9 | 60.8 ± 40.7 | 0.175 |
| CREATININE | Mean ± SD | 0.9 ± 0.3 | 1.1 ± 0.9 | 0.893 |
| NEUTROPHIL.COUNT | Mean ± SD | 72.7 ± 13.1 | 75.3 ± 14.6 | 0.333 |
| LYMPHOCYTE.COUNT | Mean ± SD | 19.6 ± 11.7 | 18.1 ± 12.1 | 0.53 |
| NLR | Mean ± SD | 5.2 ± 3.2 | 7.9 ± 7.9 | 0.547 |
| RDW.CV | Mean ± SD | 13.0 ± 1.0 | 14.2 ± 2.6 | 0.06 |
| FIBRINOGEN | Mean ± SD | 711.5 ± 127.9 | 757.8 ± 170.6 | 0.218 |
| FERRITIN | Mean ± SD | 1284.2 ± 1905.0 | 1824.9 ± 1485.9 | 0.001 |
| COOMB.TEST | Negative | 10 (31.2%) | 22 (68.8%) | 1.00 |
| Positive | 5 (31.2%) | 11 (68.8%) | ||
| ADAMTS13 | Mean ± SD | 59.5 ± 24.3 | 60.1 ± 15.1 | 0.926 |
| BLOOD.GROUP | A | 3 (20.0%) | 12 (80.0%) | 0.646 |
| AB | 2 (33.3%) | 4 (66.7%) | ||
| B | 4 (44.4%) | 5 (55.6%) | ||
| O | 4 (28.6%) | 10 (71.4%) | ||
| RH | Negative | 2 (40.0%) | 3 (60.0%) | 0.617 |
| Positive | 11 (27.5%) | 29 (72.5%) | ||
| VITAMINA.D.LEVEL | Mean ± SD | 27.9 ± 12.5 | 21.9 ± 11.5 | 0.064 |
| PT | Mean ± SD | 13.6 ± 0.7 | 14.5 ± 1.7 | 0.156 |
| INR | Mean ± SD | 1.0 ± 0.1 | 1.0 ± 0.2 | 0.366 |
| TROP.I | Mean ± SD | 0.0 ± 0.0 | 0.3 ± 1.7 | 0.322 |
| PCT | Mean ± SD | 0.1 ± 0.1 | 0.4 ± 1.1 | 0.539 |
| GLU | Mean ± SD | 7.0 ± 1.9 | 9.8 ± 5.0 | 0.088 |
| Risk Factors | Improved | Died | OR (95% CI) | p Value | |
|---|---|---|---|---|---|
| Tocilizumab | Not received | 21 (100.0%) | 0 (0.0%) | - | 0.994 |
| Received | 35 (71.4%) | 14 (28.6%) | 125,746,406.08 (0.00-NA) | ||
| Unstable groups received tocilizumab | Severe | 25 (71.4%) | 4 (28.6%) | - | |
| Early Critical | 2 (5.7%) | 1 (7.1%) | 3.12 (0.13–41.43) | 0.394 | |
| Late Critical | 8 (22.9%) | 9 (64.3%) | 7.03 (1.80–32.32) | 0.007 | |
| Demographic | |||||
| Age (years) | Mean ± SD | 47.5 ± 13.0 | 57.2 ± 11.5 | 1.06 (1.01–1.13) | 0.027 |
| Gender | Female | 5 (14.3%) | 3 (21.4%) | - | 0.544 |
| Male | 30 (85.7%) | 11 (78.6%) | 0.61 (0.13–3.37) | ||
| Race | Asian | 24 (68.6%) | 7 (50.0%) | - | |
| Black | 1 (2.9%) | 1 (7.1%) | 3.43 (0.12–94.61) | 0.404 | |
| White | 10 (28.6%) | 6 (42.9%) | 2.06 (0.54–7.82) | 0.283 | |
| BMI | Mean ± SD | 30.5 ± 6.2 | 30.1 ± 7.5 | 0.99 (0.89–1.09) | 0.848 |
| Clinical | |||||
| HTN | No | 23 (71.9%) | 4 (30.8%) | - | 0.015 |
| Yes | 9 (28.1%) | 9 (69.2%) | 5.75 (1.49–26.01) | ||
| DM | No | 21 (65.6%) | 6 (46.2%) | - | 0.232 |
| Yes | 11 (34.4%) | 7 (53.8%) | 2.23 (0.60–8.58) | ||
| CVS | No | 26 (81.2%) | 8 (72.7%) | - | 0.551 |
| Yes | 6 (18.8%) | 3 (27.3%) | 1.62 (0.29–7.80) | ||
| Biochemical | |||||
| WBC | Mean ± SD | 6.1 ± 2.9 | 8.4 ± 5.4 | 1.16 (0.99–1.39) | 0.073 |
| HEMOGLOBIN | Mean ± SD | 13.6 ± 1.4 | 12.0 ± 2.5 | 0.59 (0.34–0.88) | 0.026 |
| PLATELETS | Mean ± SD | 334.0 ± 149.6 | 240.9 ± 47.4 | 0.99 (0.99–1.00) | 0.038 |
| CRP | Mean ± SD | 108.8 ± 82.5 | 202.4 ± 133.3 | 1.01 (1.00–1.02) | 0.013 |
| D.DIMER | Mean ± SD | 5.5 ± 8.6 | 17.4 ± 8.9 | 1.14 (1.06–1.26) | 0.002 |
| LDH | Mean ± SD | 439.8 ± 177.8 | 1145.2 ± 874.8 | 1.00 (1.00–1.01) | 0.007 |
| ALT | Mean ± SD | 72.9 ± 94.6 | 36.8 ± 16.7 | 0.97 (0.93–1.00) | 0.054 |
| AST | Mean ± SD | 64.8 ± 46.4 | 51.1 ± 19.3 | 0.99 (0.96–1.01) | 0.320 |
| CREATININE | Mean ± SD | 0.9 ± 0.6 | 1.6 ± 1.3 | 2.59 (1.18–9.47) | 0.054 |
| NLR | Mean ± SD | 6.0 ± 6.9 | 12.6 ± 8.6 | 1.11 (1.02–1.22) | 0.020 |
| RDW.CV | Mean ± SD | 13.3 ± 1.6 | 16.5 ± 3.2 | 1.86 (1.32–2.90) | 0.002 |
| TROP.I | Mean ± SD | 0.4 ± 2.0 | 0.0 ± 0.0 | 0.71 (NA-1.28) | 0.735 |
| IL6 | Mean ± SD | 451.0 ± 650.8 | 2109.8 ± 1319.0 | 1.00 (1.00–1.00) | 0.045 |
| NEUTROPHIL.COUNT | Mean ± SD | 70.9 ± 14.8 | 86.3 ± 5.6 | 1.15 (1.06–1.30) | 0.004 |
| LYMPHOCYTE.COUNT | Mean ± SD | 21.6 ± 12.5 | 9.5 ± 4.7 | 0.85 (0.74–0.93) | 0.005 |
| FIBRINOGEN | Mean ± SD | 725.9 ± 149.0 | 837.4 ± 199.6 | 1.00 (1.00–1.01) | 0.046 |
| FERRITIN | Mean ± SD | 1354.6 ± 601.7 | 3000.7 ± 2262.9 | 1.00 (1.00–1.00) | 0.026 |
| COOMB.TEST | Negative | 18 (78.3%) | 4 (40.0%) | - | 0.040 |
| Positive | 5 (21.7%) | 6 (60.0%) | 5.40 (1.13–29.64) | ||
| BLOOD.GROUP | A | 9 (45.0%) | 3 (27.3%) | - | |
| AB | 2 (10.0%) | 2 (18.2%) | 3.00 (0.26–36.57) | 0.361 | |
| B | 4 (20.0%) | 1 (9.1%) | 0.75 (0.03–8.30) | 0.825 | |
| O | 5 (25.0%) | 5 (45.5%) | 3.00 (0.51–20.42) | 0.232 | |
| RH | Negative | 2 (9.5%) | 1 (9.1%) | - | 0.968 |
| Positive | 19 (90.5%) | 10 (90.9%) | 1.05 (0.09–24.29) | ||
| VITAMINA.D.LEVEL | Mean ± SD | 22.4 ± 11.8 | 20.8 ± 11.6 | 0.99 (0.91–1.06) | 0.724 |
| PT | Mean ± SD | 14.5 ± 1.9 | 14.3 ± 1.2 | 0.92 (0.51–1.48) | 0.737 |
| INR | Mean ± SD | 1.0 ± 0.3 | 1.1 ± 0.1 | 3.42 (0.21–91.93) | 0.413 |
| PCT | Mean ± SD | 0.2 ± 0.3 | 1.0 ± 1.9 | 4.59 (1.29–34.88) | 0.065 |
| GLU | Mean ± SD | 9.8 ± 4.0 | 9.8 ± 7.0 | 1.00 (0.86–1.16) | 0.989 |
| Co-Management | Died | Improved | p Value | |
|---|---|---|---|---|
| Vitamin D | No (N = 30/41) | 12 (40.0%) | 18 (60.0%) | 0.07 |
| Usual Treatment Dose (N = 12/20) | 2 (16.7%) | 10 (83.3%) | ||
| High Dose (N = 7/9) | 0 (0.0%) | 7 (100.0%) | ||
| Anticoagulants | Non-therapeutic Dose (N = 10/12) | 10 (100.0%) | 0 (0.0%) | <0.001 |
| Therapeutic Dose (N = 39/54) | 4 (10.3%) | 35 (89.7%) | ||
| Steroids | No (N = 46/63) | 12 (26.1%) | 34 (73.9%) | 0.193 |
| Yes (N = 3/7) | 2 (66.7%) | 1 (33.3%) | ||
| Antivirals | HCQ/AVIGAN (N = 24/38) | 7 (29.2%) | 17 (70.8%) | 0.551 |
| HCQ/AVIGAN/KALETRA (N = 7/8) | 2 (28.6%) | 5 (71.4%) | ||
| HCQ/AVIGAN/KALETRA/AZI (N = 2/3) | 0 (0.0%) | 2 (100.0%) | ||
| HCQ/AZI (N = 6/7) | 0 (0.0%) | 6 (100.0%) | ||
| HCQ/AZI/AVIGAN (N = 11/14) | 4 (36.4%) | 7 (63.6%) | ||
| HCQ ALONE (N = 0/1) | 0 (0.0%) | 0 (0.0%) |
| AE and Secondary Infection | Severe | Early Critical | Late Critical | p Value | |
|---|---|---|---|---|---|
| Adverse events | Grade 1 | 10 (90.9%) | 0 (0.0%) | 1 (9.1%) | 0.006 |
| Grade 2 | 2 (40.0%) | 0 (0.0%) | 3 (60.0%) | ||
| Grade 3 | 2 (18.2%) | 1 (9.1%) | 8 (72.7%) | ||
| Grade 4 | 2 (66.7%) | 0 (0.0%) | 1 (33.3%) | ||
| Secondary infections | Bacterial | 0 (0.0%) | 1 (20.0%) | 4 (80.0%) | 0.024 |
| Fungal | 2 (66.7%) | 0 (0.0%) | 1 (33.3%) | ||
| No | 27 (65.9%) | 2 (4.9%) | 12 (29.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hafez, W.; Abdelrahman, A. Factors Influencing Disease Stability and Response to Tocilizumab Therapy in Severe COVID-19: A Retrospective Cohort Study. Antibiotics 2022, 11, 1078. https://doi.org/10.3390/antibiotics11081078
Hafez W, Abdelrahman A. Factors Influencing Disease Stability and Response to Tocilizumab Therapy in Severe COVID-19: A Retrospective Cohort Study. Antibiotics. 2022; 11(8):1078. https://doi.org/10.3390/antibiotics11081078
Chicago/Turabian StyleHafez, Wael, and Ahmed Abdelrahman. 2022. "Factors Influencing Disease Stability and Response to Tocilizumab Therapy in Severe COVID-19: A Retrospective Cohort Study" Antibiotics 11, no. 8: 1078. https://doi.org/10.3390/antibiotics11081078
APA StyleHafez, W., & Abdelrahman, A. (2022). Factors Influencing Disease Stability and Response to Tocilizumab Therapy in Severe COVID-19: A Retrospective Cohort Study. Antibiotics, 11(8), 1078. https://doi.org/10.3390/antibiotics11081078