
Trends of Fixed-Dose Combination Antibiotic Consumption in Hospitals in China: Analysis of Data from the Center for Antibacterial Surveillance, 2013–2019



 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Source
2.3. Data Collection
2.4. Measurement
2.4.1. Indicators
2.4.2. WHO AWaRe Classification
2.5. Data Analysis
3. Results
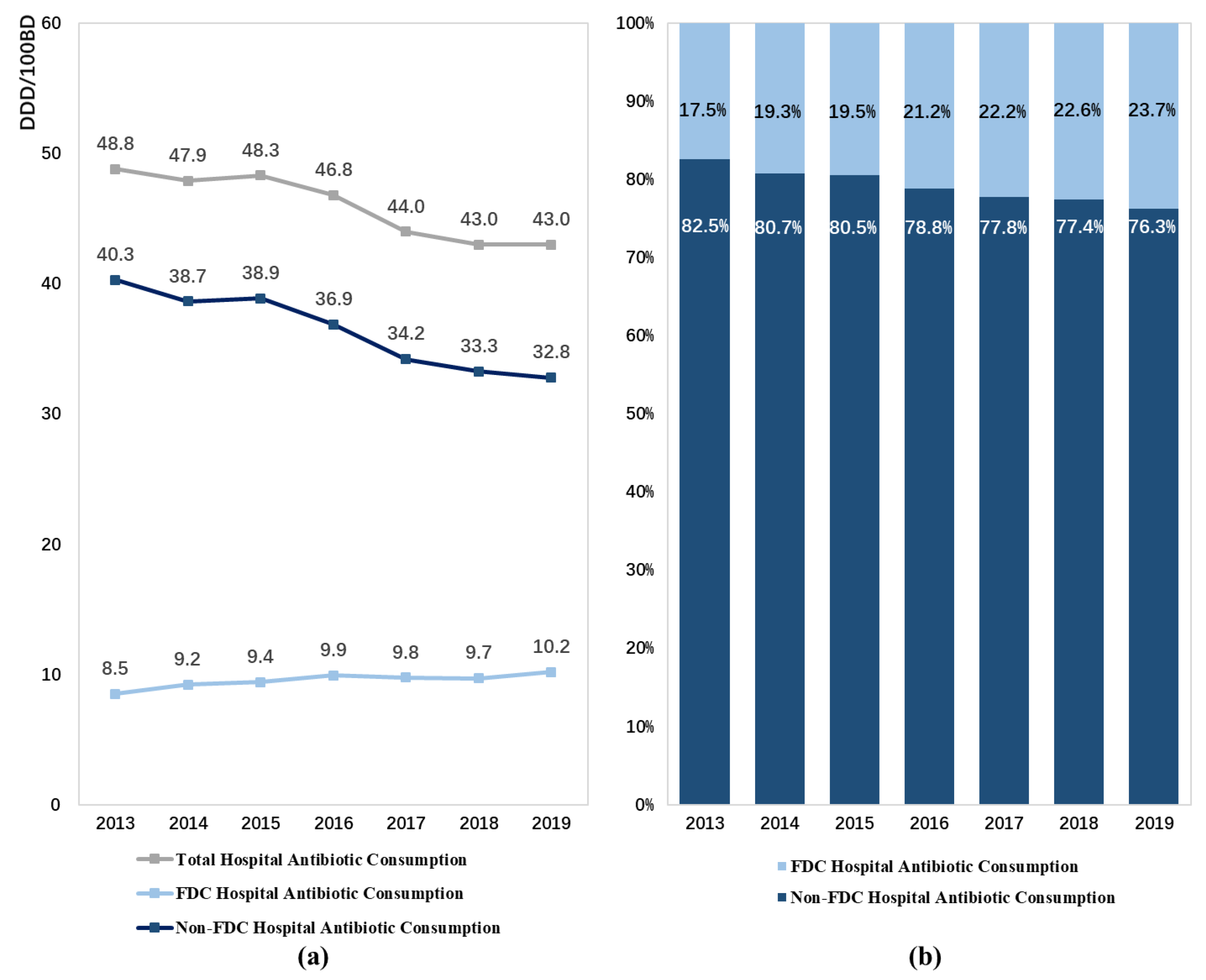
3.1. Total Consumption of FDC Antibiotics
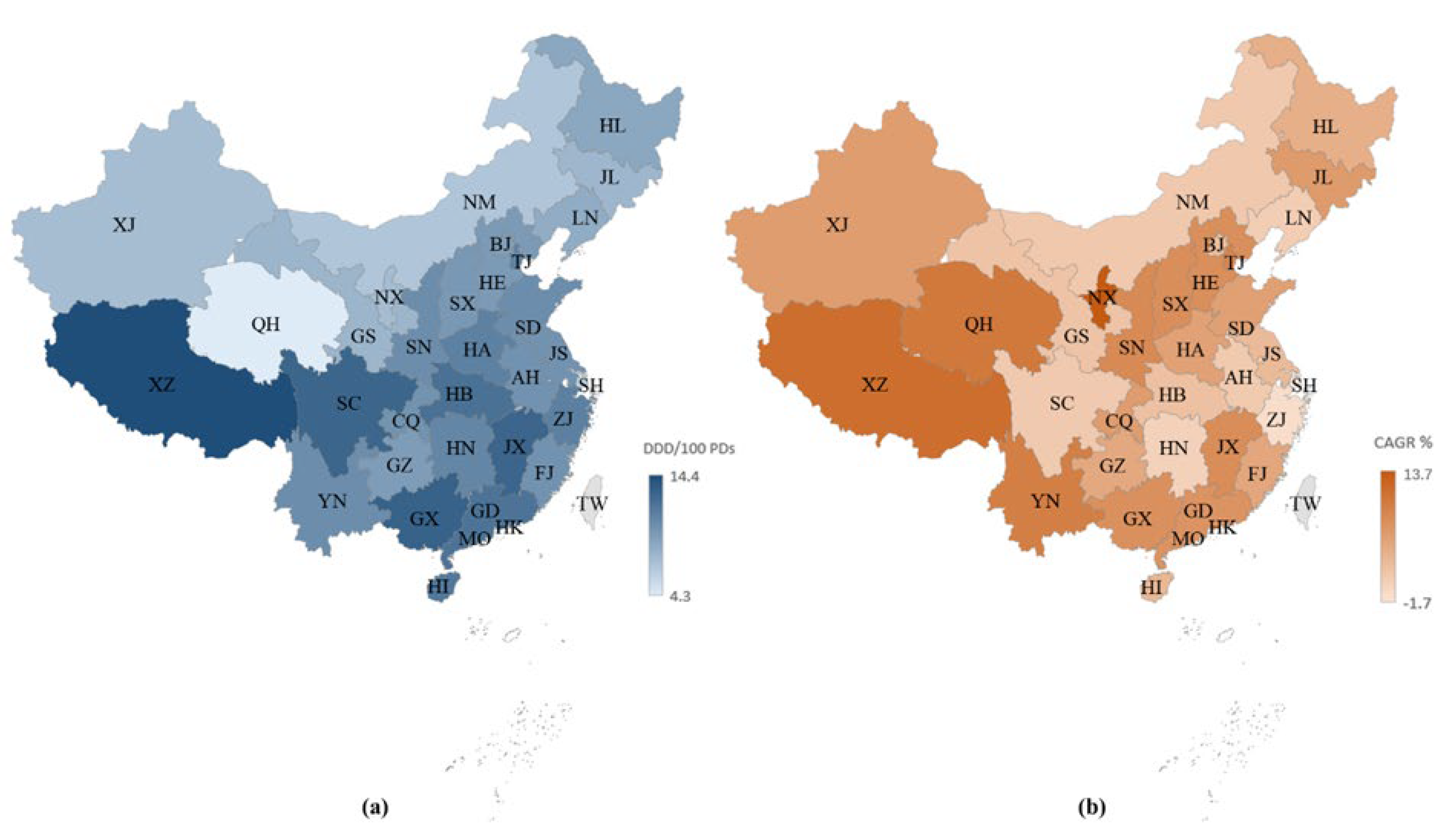
3.2. Regional Distribution of FDC Antibiotic Consumption
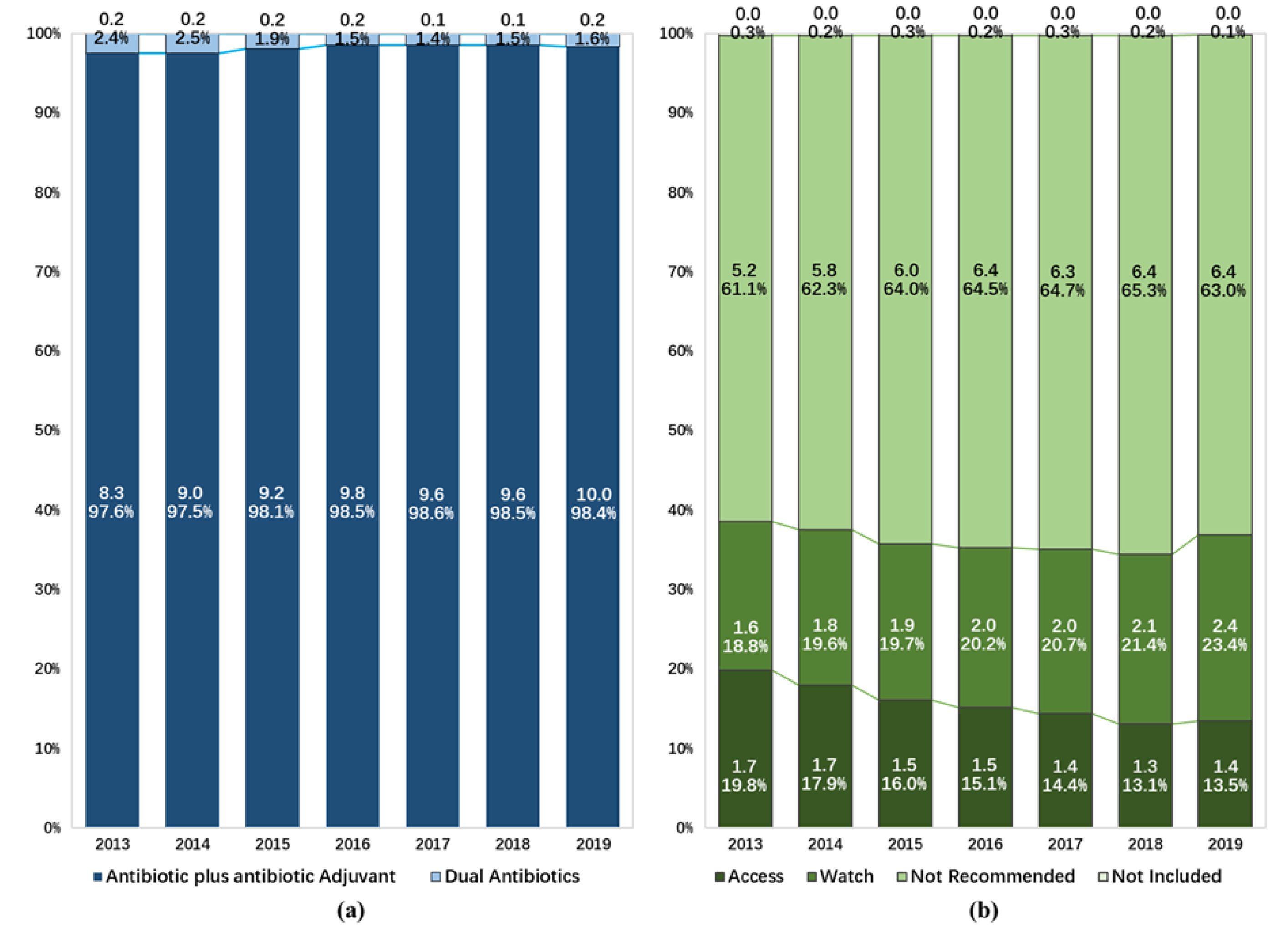
3.3. The Consumption of FDC Antibiotics in Different Compositions and AWaRe Classification
3.4. The Consumption of Most Frequently Used FDC Antibiotics
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Provinces | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | S | A | T | S | A | T | S | A | T | S | A | T | S | A | T | S | A | T | S | A | |
| C | 237 | 95 | 332 | 253 | 104 | 357 | 272 | 113 | 385 | 270 | 112 | 382 | 274 | 113 | 387 | 284 | 123 | 407 | 286 | 135 | 421 |
| AH | 40 | 7 | 47 | 42 | 9 | 51 | 43 | 11 | 54 | 44 | 11 | 55 | 48 | 14 | 62 | 52 | 18 | 70 | 56 | 22 | 78 |
| HA | 64 | 44 | 108 | 66 | 48 | 114 | 67 | 54 | 121 | 65 | 53 | 118 | 66 | 50 | 116 | 68 | 52 | 120 | 67 | 54 | 121 |
| HB | 40 | 4 | 44 | 43 | 4 | 47 | 49 | 3 | 52 | 50 | 5 | 55 | 48 | 5 | 53 | 49 | 3 | 52 | 48 | 4 | 52 |
| HN | 32 | 19 | 51 | 34 | 19 | 53 | 34 | 19 | 53 | 34 | 17 | 51 | 33 | 17 | 50 | 32 | 13 | 45 | 30 | 14 | 44 |
| JX | 25 | 7 | 32 | 33 | 10 | 43 | 42 | 12 | 54 | 40 | 11 | 51 | 41 | 13 | 54 | 48 | 22 | 70 | 49 | 25 | 74 |
| SX | 36 | 14 | 50 | 35 | 14 | 49 | 37 | 14 | 51 | 37 | 15 | 52 | 38 | 14 | 52 | 35 | 15 | 50 | 36 | 16 | 52 |
| E | 449 | 132 | 581 | 481 | 137 | 618 | 505 | 150 | 655 | 533 | 182 | 715 | 545 | 183 | 728 | 591 | 245 | 836 | 612 | 289 | 901 |
| BJ | 45 | 9 | 54 | 47 | 8 | 55 | 46 | 8 | 54 | 45 | 8 | 53 | 39 | 8 | 47 | 38 | 7 | 45 | 36 | 7 | 43 |
| FJ | 39 | 15 | 54 | 38 | 14 | 52 | 41 | 16 | 57 | 42 | 18 | 60 | 45 | 18 | 63 | 53 | 27 | 80 | 54 | 28 | 82 |
| GD | 70 | 14 | 84 | 77 | 15 | 92 | 80 | 16 | 96 | 92 | 16 | 108 | 97 | 23 | 120 | 126 | 70 | 196 | 148 | 114 | 262 |
| HI | 14 | 16 | 30 | 15 | 16 | 31 | 16 | 17 | 33 | 16 | 18 | 34 | 17 | 17 | 34 | 19 | 17 | 36 | 19 | 17 | 36 |
| HE | 22 | 4 | 26 | 30 | 7 | 37 | 31 | 8 | 39 | 36 | 9 | 45 | 37 | 7 | 44 | 39 | 8 | 47 | 41 | 9 | 50 |
| JS | 85 | 23 | 108 | 82 | 23 | 105 | 90 | 27 | 117 | 94 | 30 | 124 | 95 | 29 | 124 | 93 | 29 | 122 | 91 | 27 | 118 |
| SD | 61 | 9 | 70 | 75 | 11 | 86 | 76 | 10 | 86 | 78 | 15 | 93 | 79 | 15 | 94 | 81 | 16 | 97 | 80 | 15 | 95 |
| SH | 41 | 25 | 66 | 39 | 25 | 64 | 45 | 30 | 75 | 46 | 48 | 94 | 47 | 46 | 93 | 46 | 48 | 94 | 46 | 46 | 92 |
| TJ | 23 | 8 | 31 | 27 | 8 | 35 | 28 | 8 | 36 | 28 | 9 | 37 | 32 | 8 | 40 | 34 | 9 | 43 | 33 | 9 | 42 |
| ZJ | 49 | 9 | 58 | 51 | 10 | 61 | 52 | 10 | 62 | 56 | 11 | 67 | 57 | 12 | 69 | 62 | 14 | 76 | 64 | 17 | 81 |
| HL | 59 | 1 | 60 | 60 | 2 | 62 | 67 | 2 | 69 | 67 | 2 | 69 | 69 | 2 | 71 | 68 | 2 | 70 | 67 | 2 | 69 |
| JL | 22 | 4 | 26 | 23 | 4 | 27 | 22 | 5 | 27 | 23 | 4 | 27 | 22 | 5 | 27 | 21 | 4 | 25 | 20 | 4 | 24 |
| LN | 42 | 14 | 56 | 42 | 13 | 55 | 48 | 16 | 64 | 67 | 32 | 99 | 72 | 41 | 113 | 88 | 70 | 158 | 94 | 71 | 165 |
| W | 327 | 248 | 575 | 338 | 268 | 606 | 367 | 303 | 670 | 373 | 324 | 697 | 389 | 371 | 760 | 429 | 431 | 860 | 445 | 461 | 906 |
| CQ | 20 | 13 | 33 | 21 | 13 | 34 | 23 | 17 | 40 | 23 | 23 | 46 | 27 | 26 | 53 | 28 | 29 | 57 | 29 | 29 | 58 |
| GS | 30 | 28 | 58 | 30 | 34 | 64 | 31 | 35 | 66 | 29 | 35 | 64 | 32 | 41 | 73 | 35 | 43 | 78 | 36 | 50 | 86 |
| GX | 43 | 16 | 59 | 43 | 17 | 60 | 43 | 17 | 60 | 44 | 18 | 62 | 48 | 27 | 75 | 50 | 27 | 77 | 52 | 29 | 81 |
| GZ | 23 | 8 | 31 | 27 | 8 | 35 | 33 | 18 | 51 | 38 | 27 | 65 | 40 | 35 | 75 | 41 | 53 | 94 | 43 | 61 | 104 |
| NM | 28 | 5 | 33 | 26 | 7 | 33 | 31 | 9 | 40 | 32 | 10 | 42 | 33 | 10 | 43 | 33 | 9 | 42 | 33 | 9 | 42 |
| NX | 15 | 42 | 57 | 15 | 40 | 55 | 15 | 39 | 54 | 15 | 39 | 54 | 15 | 39 | 54 | 15 | 39 | 54 | 14 | 38 | 52 |
| QH | 17 | 12 | 29 | 19 | 17 | 36 | 20 | 23 | 43 | 20 | 24 | 44 | 19 | 25 | 44 | 19 | 29 | 48 | 19 | 26 | 45 |
| SN | 42 | 58 | 100 | 42 | 60 | 102 | 46 | 69 | 115 | 45 | 67 | 112 | 45 | 70 | 115 | 48 | 65 | 113 | 50 | 59 | 109 |
| SC | 47 | 3 | 50 | 50 | 3 | 53 | 54 | 3 | 57 | 54 | 4 | 58 | 54 | 3 | 57 | 82 | 31 | 113 | 92 | 43 | 135 |
| XJ | 32 | 26 | 58 | 33 | 30 | 63 | 34 | 32 | 66 | 35 | 37 | 72 | 35 | 48 | 83 | 35 | 50 | 85 | 35 | 55 | 90 |
| XZ | 1 | 1 | 1 | 1 | 1 | 1 | |||||||||||||||
| YN | 30 | 37 | 67 | 32 | 39 | 71 | 37 | 41 | 78 | 38 | 40 | 78 | 40 | 47 | 87 | 42 | 56 | 98 | 41 | 62 | 103 |
| Total | 1136 | 494 | 1630 | 1197 | 528 | 1725 | 1281 | 589 | 1870 | 1333 | 656 | 1989 | 1371 | 715 | 2086 | 1481 | 875 | 2356 | 1524 | 962 | 2486 |
| FDC | ATC Code | Composition | AWaRe | Ranking in 2013 | Ranking in 2019 | Cum. in 2019, % | Trend | CAGR, % | Trends in Antibiotic Use | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All FDC Antibiotics | - | - | - | - | - | - | ↑* | 3.0 |  | 8.521 | 9.246 | 9.428 | 9.926 | 9.785 | 9.729 | 10.201 |
| Cefoperazone/Sulbactam | J01DD62 | A and A | NR | 1 | 1 | 33.0 | ↑* | 3.9 |  | 2.672 | 2.959 | 2.876 | 3.089 | 3.249 | 3.278 | 3.367 |
| Piperacillin/Tazobactam | J01CR05 | A and A | W | 3 | 2 | 50.9 | ↑* | 7.7 |  | 1.172 | 1.337 | 1.295 | 1.393 | 1.446 | 1.543 | 1.824 |
| Amoxicillin/Clavulanic Acid | J01CR02 | A and A | A | 2 | 3 | 62.9 | ↓* | −3.2 |  | 1.491 | 1.441 | 1.357 | 1.342 | 1.239 | 1.146 | 1.227 |
| Mezlocillin/Sulbactam | - | A and A | NR | 4 | 4 | 72.2 | ↑* | 5.7 |  | 0.682 | 0.781 | 0.886 | 1.052 | 0.993 | 1.014 | 0.951 |
| Piperacillin/Sulbactam | J01CR05 | A and A | NR | 5 | 5 | 78.7 | - | 2.5 |  | 0.565 | 0.648 | 0.729 | 0.693 | 0.644 | 0.640 | 0.654 |
| Cefoperazone/Tazobactam | J01DD62 | A and A | NR | 6 | 6 | 85.0 | - | 4.1 |  | 0.510 | 0.567 | 0.649 | 0.674 | 0.668 | 0.632 | 0.648 |
| Imipenem/Cilastatin | J01DH51 | A and A | W | 7 | 7 | 90.6 | - | 4.8 |  | 0.429 | 0.472 | 0.563 | 0.609 | 0.579 | 0.537 | 0.567 |
| Cefotaxime/Sulbactam | J01DD51 | A and A | NR | 11 | 8 | 93.8 | ↑* | 18.2 |  | 0.120 | 0.148 | 0.257 | 0.288 | 0.271 | 0.287 | 0.327 |
| Ceftriaxone/Tazobactam | J01DD63 | A and A | NR | 9 | 9 | 96.4 | - | 2.0 |  | 0.236 | 0.276 | 0.284 | 0.312 | 0.259 | 0.265 | 0.266 |
| Amoxicillin/Sulbactam | J01CR02 | A and A | NR | 8 | 10 | 97.8 | ↓** | −13.7 |  | 0.342 | 0.310 | 0.287 | 0.240 | 0.197 | 0.173 | 0.141 |
| Sulfamethoxazole/Trimethoprim | J01EE01 | DA | A | 10 | 11 | 98.9 | ↓* | −3.7 |  | 0.140 | 0.178 | 0.125 | 0.120 | 0.101 | 0.089 | 0.112 |
| Amoxicillin/Flucloxacillin | J01RA01 | DA | NR | 13 | 12 | 99.3 | - | 1.9 |  | 0.043 | 0.040 | 0.038 | 0.021 | 0.036 | 0.049 | 0.048 |
| Ampicillin/Sulbactam | J01CR01 | A and A | A | 12 | 13 | 99.7 | - | −8.5 |  | 0.057 | 0.039 | 0.029 | 0.040 | 0.065 | 0.037 | 0.033 |
| Ticarcillin/Clavulanic acid | J01CR03 | A and A | NI | 14 | 14 | 99.8 | ↓* | −9.3 |  | 0.023 | 0.021 | 0.021 | 0.021 | 0.022 | 0.018 | 0.013 |
| Ceftriaxone/Sulbactam | J01DD63 | A and A | NR | 15 | 15 | 99.9 | - | 2.1 |  | 0.010 | 0.012 | 0.013 | 0.023 | 0.007 | 0.013 | 0.012 |
| Ampicillin/Cloxacillin | J01CR50 | DA | NR | 16 | 16 | 99.9 | ↓* | −15.4 |  | 0.009 | 0.007 | 0.005 | 0.001 | 0.001 | 0.001 | 0.003 |
| Amoxicillin/Dicloxacillin | J01RA01 | DA | NR | 17 | 17 | 100.0 | - | −20.8 |  | 0.008 | 0.001 | 0.003 | 0.001 | 0.001 | 0.001 | 0.002 |
| Cefalexin/Trimethoprim | - | DA | NR | 20 | 18 | 100.0 | ↓* | −11.0 |  | 0.003 | 0.002 | 0.003 | 0.002 | 0.002 | 0.001 | 0.001 |
| Cefazolin/Sulbactam | - | A and A | NI | 23 | 19 | 100.0 | - | - |  | 0.000 | 0.000 | 0.000 | 0.000 | 0.002 | 0.003 | 0.001 |
| Ceftazidime/Sulbactam | J01DD52 | A and A | NR | 22 | 20 | 100.0 | - | - |  | 0.000 | 0.000 | 0.000 | 0.001 | 0.001 | 0.000 | 0.001 |
| Ampicillin/Probenecid | J01CA51 | A and A | NI | 19 | 21 | 100.0 | - | −23.7 |  | 0.003 | 0.001 | 0.004 | 0.002 | 0.001 | 0.002 | 0.001 |
| Fosfomycin/Trimethoprim | - | DA | NR | 21 | 22 | 100.0 | - | −6.7 |  | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Cefadroxil/Trimethoprim | - | DA | NR | 18 | 23 | 100.0 | ↓* | −47.5 |  | 0.005 | 0.003 | 0.002 | 0.001 | 0.001 | 0.001 | 0.000 |
| Ceftazidime/Avibactam | J01DD52 | A and A | R | 24 | 24 | 100.0 | - | - |  | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
References
- Roberts, S.C.; Zembower, T.R. Global Increases in Antibiotic Consumption: A Concerning Trend for WHO Targets. Lancet Infect. Dis. 2021, 21, 10–11. [Google Scholar] [CrossRef]
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K.; Sharland, M.; Gandra, S.; Pulcini, C.; Laxminarayan, R. Assessment of WHO Antibiotic Consumption and Access Targets in 76 Countries, 2000–2015: An Analysis of Pharmaceutical Sales Data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 30 March 2022).
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable Deaths and Disability-Adjusted Life-Years Caused by Infections with Antibiotic-Resistant Bacteria in the EU and the European Economic Area in 2015: A Population-Level Modelling Analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Laws, M.; Shaaban, A.; Rahman, K.M. Antibiotic Resistance Breakers: Current Approaches and Future Directions. FEMS Microbiol. Rev. 2019, 43, 490–516. [Google Scholar] [CrossRef]
- DiMasi, J.A.; Grabowski, H.G.; Hansen, R.W. Innovation in the Pharmaceutical Industry: New Estimates of R&D Costs. J. Health Econ. 2016, 47, 20–33. [Google Scholar] [CrossRef]
- Boyd, N.K.; Teng, C.; Frei, C.R. Brief Overview of Approaches and Challenges in New Antibiotic Development: A Focus on Drug Repurposing. Front. Cell. Infect. Microbiol. 2021, 11, 684515. [Google Scholar] [CrossRef]
- Micek, S.T.; Welch, E.C.; Khan, J.; Pervez, M.; Doherty, J.A.; Reichley, R.M.; Kollef, M.H. Empiric Combination Antibiotic Therapy Is Associated with Improved Outcome against Sepsis Due to Gram-Negative Bacteria: A Retrospective Analysis. Antimicrob. Agents Chemother. 2010, 54, 1742–1748. [Google Scholar] [CrossRef]
- European Medicines Agency. Guideline on Fixed Combination Medicinal Products. 2009. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-development-fixed-combination-medicinal-products-revision-1_en.pdf (accessed on 30 March 2022).
- Connor, J.; Rafter, N.; Rodgers, A. Do Fixed-Dose Combination Pills or Unit-of-Use Packaging Improve Adherence? A Systematic Review. Bull. World Health Organ. 2004, 82, 935–939. [Google Scholar] [CrossRef]
- Bortone, B.; Jackson, C.; Hsia, Y.; Bielicki, J.; Magrini, N.; Sharland, M. High Global Consumption of Potentially Inappropriate Fixed Dose Combination Antibiotics: Analysis of Data from 75 Countries. PLoS ONE 2021, 16, e0241899. [Google Scholar] [CrossRef]
- Harries, A.D.; Lawn, S.D.; Suthar, A.B.; Granich, R. Benefits of Combined Preventive Therapy with Co-Trimoxazole and Isoniazid in Adults Living with HIV: Time to Consider a Fixed-Dose, Single Tablet Coformulation. Lancet Infect. Dis. 2015, 15, 1492–1496. [Google Scholar] [CrossRef]
- Innovation, Nontraditional Antibacterial Drugs, and Clinical Utility—ACS Infectious Diseases. Available online: https://pubs.acs.org/doi/10.1021/acsinfecdis.1c00227 (accessed on 22 June 2022).
- Mauri, C.; Maraolo, A.E.; Di Bella, S.; Luzzaro, F.; Principe, L. The Revival of Aztreonam in Combination with Avibactam against Metallo-β-Lactamase-Producing Gram-Negatives: A Systematic Review of In Vitro Studies and Clinical Cases. Antibiotics 2021, 10, 1012. [Google Scholar] [CrossRef]
- Heo, Y.-A. Imipenem/Cilastatin/Relebactam: A Review in Gram-Negative Bacterial Infections. Drugs 2021, 81, 377–388. [Google Scholar] [CrossRef]
- McGettigan, P.; Roderick, P.; Kadam, A.; Pollock, A. Threats to Global Antimicrobial Resistance Control: Centrally Approved and Unapproved Antibiotic Formulations Sold in India. Br. J. Clin. Pharmacol. 2019, 85, 59–70. [Google Scholar] [CrossRef]
- Poudel, A.; Mohamed Ibrahim, M.I.; Mishra, P.; Palaian, S. Assessment of the Availability and Rationality of Unregistered Fixed Dose Drug Combinations in Nepal: A Multicenter Cross-Sectional Study. Glob. Health Res. Policy 2017, 2, 14. [Google Scholar] [CrossRef][Green Version]
- Wirtz, V.J.; Mol, P.G.M.; Verdijk, J.; Vander Stichele, R.H.; Taxis, K. Use of Antibacterial Fixed-Dose Combinations in the Private Sector in Eight Latin American Countries between 1999 and 2009. Trop. Med. Int. Health 2013, 18, 416–425. [Google Scholar] [CrossRef]
- Why Are Fixed Dose Combinations of Antibiotics Generally Not a Good Idea?—2018—ReAct. Available online: https://www.reactgroup.org/news-and-views/news-and-opinions/year-2018/why-are-fixed-dose-combinations-of-antibiotics-generally-not-a-good-idea/ (accessed on 30 March 2022).
- Zhao, H.; Wei, L.; Li, H.; Zhang, M.; Cao, B.; Bian, J.; Zhan, S. Appropriateness of Antibiotic Prescriptions in Ambulatory Care in China: A Nationwide Descriptive Database Study. Lancet Infect. Dis. 2021, 21, 847–857. [Google Scholar] [CrossRef]
- Xiao, Y. Antimicrobial Stewardship in China: Systems, Actions and Future Strategies. Clin. Infect. Dis. 2018, 67, S135–S141. [Google Scholar] [CrossRef]
- Li, H.; Yan, S.; Li, D.; Gong, Y.; Lu, Z.; Yin, X. Trends and Patterns of Outpatient and Inpatient Antibiotic Use in China’s Hospitals: Data from the Center for Antibacterial Surveillance, 2012–2016. J. Antimicrob. Chemother. 2019, 74, 1731–1740. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for ATC Classification and DDD Assignment. 2020. Available online: https://www.whocc.no/filearchive/publications/2020_guidelines_web.pdf (accessed on 30 December 2021).
- World Health Organization. Introduction to DDD Indicators. Available online: https://www.who.int/tools/atc-ddd-toolkit/indicators (accessed on 24 June 2022).
- WHOCC-ATC/DDD Index. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 30 March 2022).
- Wushouer, H.; Zhou, Y.; Zhang, X.; Fu, M.; Fan, D.; Shi, L.; Guan, X. Secular Trend Analysis of Antibiotic Utilisation in China’s Hospitals 2011-2018, a Retrospective Analysis of Procurement Data. Antimicrob. Resist. Infect. Control 2020, 9, 53. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global Antibiotic Consumption 2000 to 2010: An Analysis of National Pharmaceutical Sales Data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- World Health Organization. 2021 AWaRe Classification. 2021. Available online: https://www.who.int/publications/i/item/2021-aware-classification (accessed on 22 June 2022).
- Bush, K.; Bradford, P.A. Epidemiology of β-Lactamase-Producing Pathogens. Clin. Microbiol. Rev. 2020, 33, e00047-19. [Google Scholar] [CrossRef]
- Expert group of “Expert Consensus on clinical Application of β -lactam antibiotic β -lactam inhibitor Compound Preparation”. Expert Consensus on clinical Application of β -lactam antibiotic β -lactam inhibitor Compound Preparation (2020 Edition). Natl. Med. J. China 2020, 100, 738–747. (In Chinese) [Google Scholar] [CrossRef]
- CARSS-2020 China Antimicrobial Resistance Surveillance Report. Available online: http://www.carss.cn/Report/Details?aId=808 (accessed on 31 March 2022). (In Chinese).
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31, e00079-17. [Google Scholar] [CrossRef]
- Chinese expert consensus group on emergency diagnosis and treatment of extended-spectrum β-lactamase-producing Enterobacter infection. Chinese expert consensus on emergency diagnosis and treatment of extended-spectrum β-lactamase-producing Enterobacter infection. Chin. J. Emerg. Med. 2020, 29, 1520–1526. (In Chinese) [CrossRef]
- Palwe, S.; Veeraraghavan, B.; Periasamy, H.; Khobragade, K.; Kharat, A.S. Unorthodox Parenteral β-Lactam and β-Lactamase Inhibitor Combinations: Flouting Antimicrobial Stewardship and Compromising Patient Care. Antimicrob. Agents Chemother. 2020, 64, e00168-20. [Google Scholar] [CrossRef]
- Anand, P.; Kaur, N.; Verma, V.; Shafiq, N.; Malhotra, S. Assessment of Rationality of Available Fixed Dose Combinations of Antibiotics in India. Expert Rev. Anti Infect. Ther. 2022, 20, 797–808. [Google Scholar] [CrossRef]
- Sayer, B.; Bortone, B.; Sharland, M.; Hsia, Y. Fixed-Dose Combination Antibiotics: The Search for Evidence Using the Example of Ampicillin-Cloxacillin. Br. J. Clin. Pharmacol. 2021, 87, 2996–2999. [Google Scholar] [CrossRef]
- Ahmad, A.; Khan, M.U.; Balkrishnan, R. Fixed-Dose Combination Antibiotics in India: Global Perspectives. Lancet Glob. Health 2016, 4, e521. [Google Scholar] [CrossRef]
- Wang, L.; Chen, Y.; Han, R.; Huang, Z.; Zhang, X.; Hu, F.; Yang, F. Sulbactam Enhances In Vitro Activity of β-Lactam Antibiotics Against Acinetobacter Baumannii. Infect. Drug Resist. 2021, 14, 3971–3977. [Google Scholar] [CrossRef]
- Xiao, S.; Zhuo, C.; Zhuo, C. In Vitro Activity of Various Sulbactam Compounds and Piperacillin/Tazobactam against Clinical Isolates of Different Gram-Negative Bacteria. Comput. Math Methods Med. 2021, 2021, 1175379. [Google Scholar] [CrossRef]
- Wareham, D.W.; Momin, M.H.F.A.; Phee, L.M.; Hornsey, M.; Standing, J.F. Cefepime/Sulbactam as an Enhanced Antimicrobial Combination Therapy for the Treatment of MDR Gram-Negative Infections. J. Antimicrob. Chemother. 2020, 75, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, P.G.; Lomovskaya, O.; Griffith, D.C.; Dudley, M.N.; VanScoy, B. β-Lactamase Inhibitors: What You Really Need to Know. Curr. Opin. Pharmacol. 2017, 36, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Crass, R.L.; Pai, M.P. Pharmacokinetics and Pharmacodynamics of β-Lactamase Inhibitors. Pharmacotherapy 2019, 39, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.B. Kinetics of Sulbactam Hydrolysis by β-Lactamases, and Kinetics of β-Lactamase Inhibition by Sulbactam. Antimicrob. Agents Chemother. 2017, 61, e01612-17. [Google Scholar] [CrossRef]
- He, P.; Sun, Q.; Shi, L.; Meng, Q. Rational Use of Antibiotics in the Context of China’s Health System Reform. BMJ 2019, 365, l4016. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of China. Questions and Answers for Administrative Measures for the Clinical Application of Antibacterial Drugs. 2012. Available online: http://www.nhc.gov.cn/wjw/zcjd/201304/43c21ad2846d4cd58785310fc1fc775a.shtml (accessed on 30 March 2022). (In Chinese)
- National Health and Family Planning Commission of China. Administrative Measures for the Clinical Application of Antibacterial Drugs. 2012. Available online: http://www.nhc.gov.cn/cms-search/xxgk/getManuscriptXxgk.htm?id=347e8d20a6d442ddab626312378311b4 (accessed on 30 March 2022). (In Chinese)



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wushouer, H.; Hu, L.; Zhou, Y.; Yang, Y.; Du, K.; Deng, Y.; Yan, Q.; Yang, X.; Chen, Z.; Zheng, B.; et al. Trends of Fixed-Dose Combination Antibiotic Consumption in Hospitals in China: Analysis of Data from the Center for Antibacterial Surveillance, 2013–2019. Antibiotics 2022, 11, 957. https://doi.org/10.3390/antibiotics11070957
Wushouer H, Hu L, Zhou Y, Yang Y, Du K, Deng Y, Yan Q, Yang X, Chen Z, Zheng B, et al. Trends of Fixed-Dose Combination Antibiotic Consumption in Hospitals in China: Analysis of Data from the Center for Antibacterial Surveillance, 2013–2019. Antibiotics. 2022; 11(7):957. https://doi.org/10.3390/antibiotics11070957
Chicago/Turabian StyleWushouer, Haishaerjiang, Lin Hu, Yue Zhou, Yaoyao Yang, Kexin Du, Yanping Deng, Qing Yan, Xiaoqiang Yang, Zhidong Chen, Bo Zheng, and et al. 2022. "Trends of Fixed-Dose Combination Antibiotic Consumption in Hospitals in China: Analysis of Data from the Center for Antibacterial Surveillance, 2013–2019" Antibiotics 11, no. 7: 957. https://doi.org/10.3390/antibiotics11070957
APA StyleWushouer, H., Hu, L., Zhou, Y., Yang, Y., Du, K., Deng, Y., Yan, Q., Yang, X., Chen, Z., Zheng, B., Guan, X., & Shi, L. (2022). Trends of Fixed-Dose Combination Antibiotic Consumption in Hospitals in China: Analysis of Data from the Center for Antibacterial Surveillance, 2013–2019. Antibiotics, 11(7), 957. https://doi.org/10.3390/antibiotics11070957