
What Factors Affect Outcome in the Treatment of Fracture-Related Infection?

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Demographics
2.2. Treatment Strategies
2.3. Outcomes
2.3.1. Patient-Related Factors
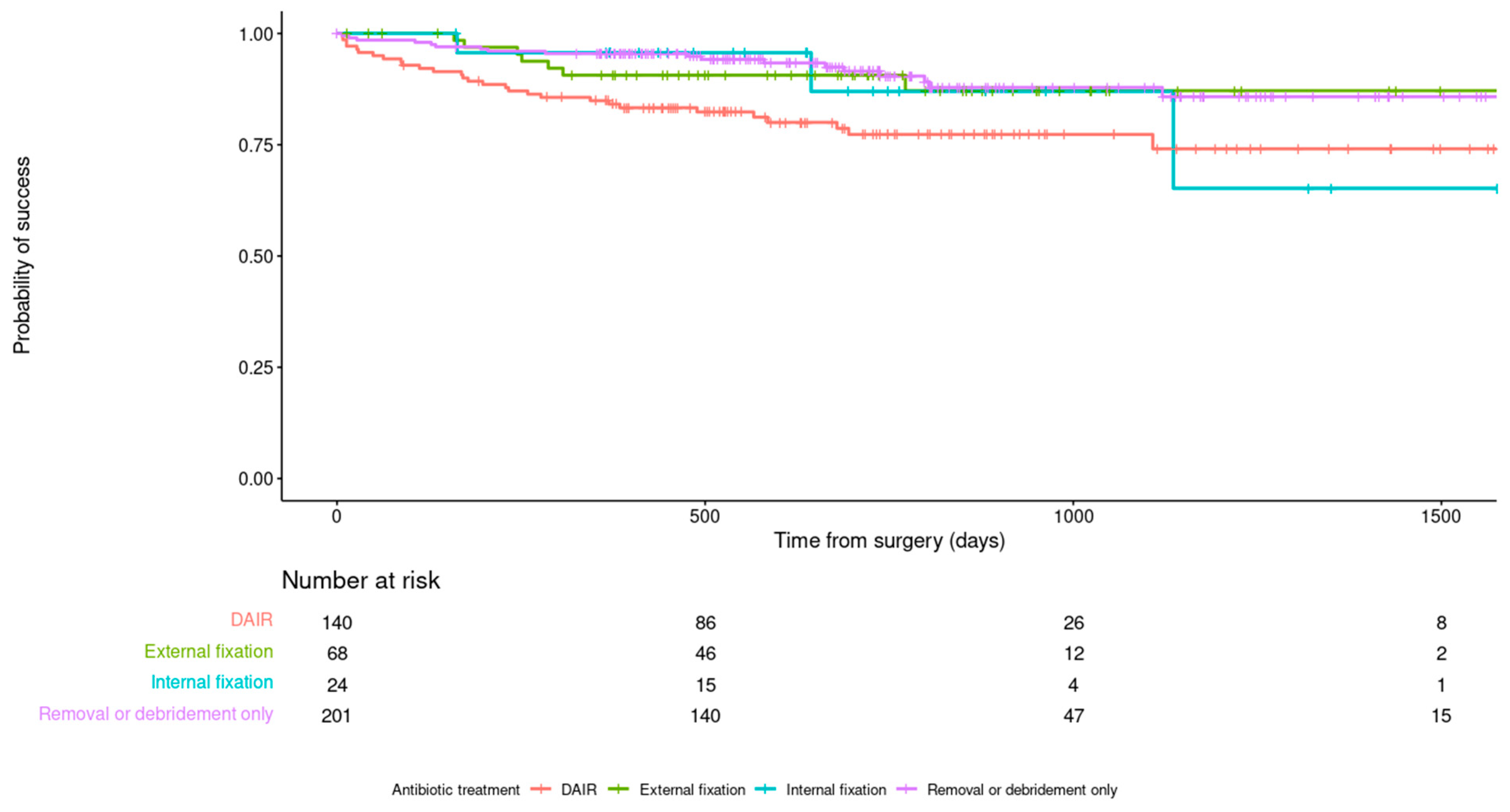
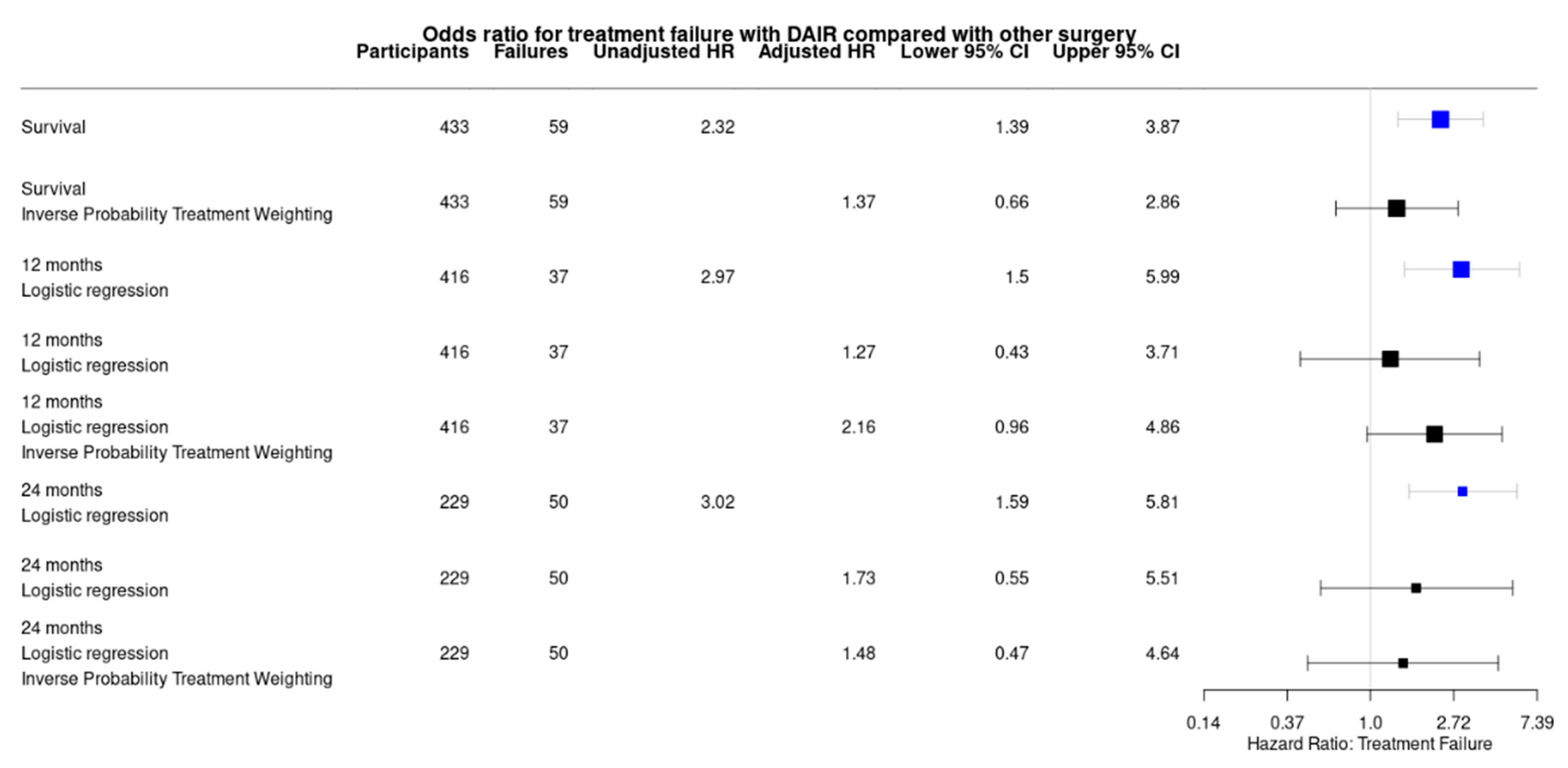
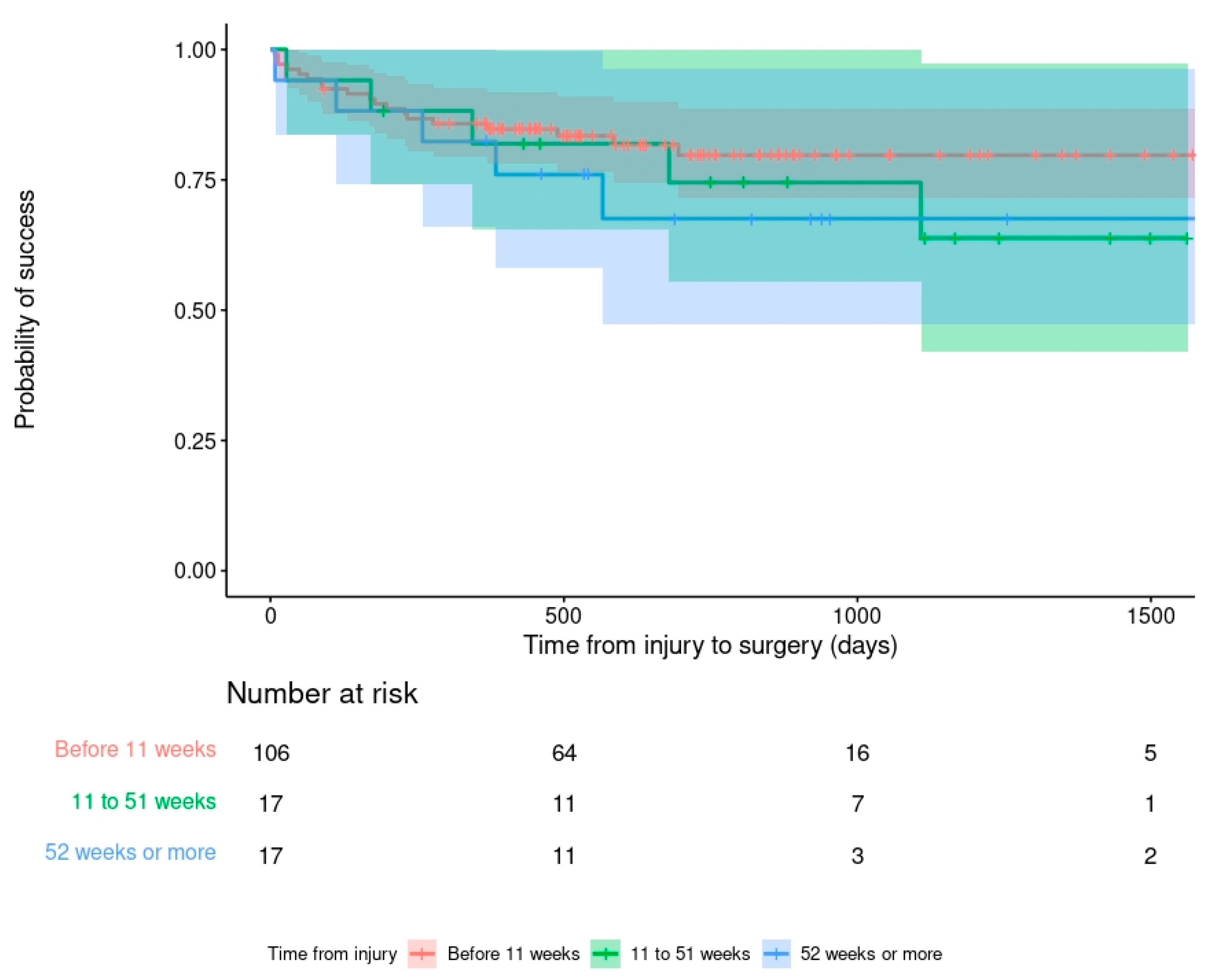
2.3.2. Surgery-Related Factors
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Baertl, S.; Metsemakers, W.J.; Morgenstern, M.; Alt, V.; Richards, R.G.; Moriarty, T.F.; Young, K. Fracture-related Infection. Bone Jt. Res. 2021, 10, 351–353. [Google Scholar] [CrossRef]
- Alt, V.; Giannoudis, P.V. Musculoskeletal infections– A global burden and a new subsection in Injury. Injury 2019, 50, 2152. [Google Scholar] [CrossRef]
- Iliaens, J.; Onsea, J.; Hoekstra, H.; Nijs, S.; Peetermans, W.E.; Metsemakers, W.-J. Fracture-related infection in long bone fractures: A comprehensive analysis of the economic impact and influence on quality of life. Injury 2021, 52, 3344–3349. [Google Scholar] [CrossRef]
- Olesen, U.K.; Pedersen, N.J.; Eckardt, H.; Lykke-Meyer, L.; Bonde, C.T.; Singh, U.M.; McNally, M. The cost of infection in severe open tibial fractures treated with a free flap. Int. Orthop. 2017, 41, 1049–1055. [Google Scholar] [CrossRef]
- Metsemakers, W.-J.; Onsea, J.; Neutjens, E.; Steffens, E.; Schuermans, A.; McNally, M.; Nijs, S. Prevention of fracture-related infection: A multidisciplinary care package. Int. Orthop. 2017, 41, 2457–2469. [Google Scholar] [CrossRef] [Green Version]
- Hak, D.J.; Fitzpatrick, D.; Bishop, J.A.; Marsh, J.L.; Tilp, S.; Schnettler, R.; Simpson, H.; Alt, V. Delayed union and nonunions: Epidemiology, clinical issues and financial aspects. Injury 2014, 45 (Suppl. S2), S3–S7. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Morgenstern, M.; McNally, M.A.; Moriarty, T.F.; McFadyen, I.; Scarborough, M.; Athanasou, N.A.; Ochsner, P.E.; Kuehl, R.; Raschke, M.; et al. Fracture-related infection: A consensus on definition from an international expert group. Injury 2018, 49, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Obremskey, W.T.; Metsemakers, W.-J.; Schlatterer, D.R.; Tetsworth, K.; Egol, K.; Kates, S.; McNally, M. Musculoskeletal Infection in Orthopaedic Trauma. Assessment of the 2018 International Consensus Meeting on Musculoskeletal Infection. J. Bone Jt. Surg. Am. 2020, 102, e44. [Google Scholar] [CrossRef]
- McNally, M.A. Infection after Fracture. In Principles of Orthopedic Infection Management; Kates, S.L., Borens, O., Eds.; AO Trauma Thieme Verlag: New York, NY, USA, 2016; pp. 139–165. [Google Scholar]
- Willenegger, H.; Roth, B. Treatment tactics and late results in early infection following osteosynthesis. Unfallchirurgie 1986, 12, 241–246. [Google Scholar] [CrossRef]
- Sendi, P.; Morgenstern, M.; Metsemakers, W.-J.; McNally, M.A. Fracture-related Infection of long bones. In Bone and Joint Infections: From Microbiology to Diagnostics and Treatment, 2nd ed.; Zimmerli, W., Ed.; John Wiley & Sons: Hoboken, NJ, USA, 2021; Chapter 23; pp. 367–386. [Google Scholar] [CrossRef]
- Gristina, A.G.; Costerton, J.W. Bacterial adherence and the glycocalyx and their role in musculoskeletal infection. Orthop. Clin. N. Am. 1984, 15, 517–535. [Google Scholar] [CrossRef]
- Stewart, P.S.; Costerton, J.W. Antibiotic resistance of bacteria in biofilms. Lancet 2001, 358, 135–138. [Google Scholar] [CrossRef]
- Masters, E.A.; Trombetta, R.P.; de Mesy Bentley, K.L.; Boyce, B.F.; Gill, A.L.; Gill, S.R.; Nishitani, K.; Ishikawa, M.; Morita, Y.; Ito, H.; et al. Evolving concepts in bone infection: Redefining “biofilm”, “acute vs. chronic osteomyelitis”, “the immune proteome” and “local antibiotic therapy”. Bone Res. 2019, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Aytaç, S.; Schnetzke, M.; Swartman, B.; Herrmann, P.; Woelfl, C.; Heppert, V.; Gruetzner, P.A.; Guehring, T. Posttraumatic and postoperative osteomyelitis: Surgical revision strategy with persisting fistula. Arch. Orthop. Trauma. Surg. 2014, 134, 159–165. [Google Scholar] [CrossRef]
- Morgenstern, M.; Kuehl, R.; Zalavras, C.G.; McNally, M.; Zimmerli, W.; Burch, M.A.; Vandendriessche, T.; Obremskey, W.T.; Verhofstad, M.H.J.; Metsemakers, W.J. The influence of duration of infection on outcome of Debridement and Implant Retention (DAIR) in Fracture-related Infection; A systematic review and critical appraisal. Bone Jt. J. 2021, 103-B, 213–221. [Google Scholar] [CrossRef]
- Metsemakers, W.-J.; On behalf of the Fracture-Related Infection (FRI) group; Morgenstern, M.; Senneville, E.; Borens, O.; Govaert, G.A.M.; Onsea, J.; Depypere, M.; Richards, R.G.; Trampuz, A.; et al. General treatment principles for fracture-related infection: Recommendations from an international expert group. Arch. Orthop. Trauma. Surg. 2020, 140, 1013–1027. [Google Scholar] [CrossRef] [Green Version]
- Bezstarosti, H.; Van Lieshout, E.M.M.; Voskamp, L.W.; Kortram, K.; Obremskey, W.; McNally, M.A.; Metsemakers, W.J.; Verhofstad, M.H.J. Insights into treatment and outcome of fracture-related infection: A systematic literature review. Arch. Orthop. Trauma. Surg. 2019, 139, 61–72. [Google Scholar] [CrossRef] [Green Version]
- Foster, A.L.; Moriarty, T.F.; Zalavras, C.; Morgenstern, M.; Jaiprakash, A.; Crawford, R.; Burch, M.-A.; Boot, W.; Tetsworth, K.; Miclau, T.; et al. The influence of biomechanical stability on bone healing and fracture-related infection: The legacy of Stephan Perren. Injury 2020, 52, 43–52. [Google Scholar] [CrossRef]
- Chan, J.; Ferguson, J.; Scarborough, M.; McNally, M.A.; Ramsden, A. Management of Post-traumatic Osteomyelitis in the Lower Limb: Current State of the Art. Indian J. Plast. Surg. 2019, 52, 62–72. [Google Scholar] [CrossRef] [Green Version]
- Müller, S.L.; Morgenstern, M.; Kuehl, R.; Muri, T.; Kalbermatten, D.F.; Clauss, M.; Schaefer, D.J.; Sendi, P.; Osinga, R. Soft tissue reconstruction in lower leg fracture-related infections: An orthoplastic outcome and risk factor analysis. Injury 2021, 52, 3489–3497. [Google Scholar] [CrossRef]
- Depypere, M.; Kuehl, R.; Metsemakers, W.J.; Senneville, E.; McNally, M.A.; Obremskey, W.T.; Zimmerli, W.; Atkins, B.L.; Trampuz, A. Recommendations for systemic antimicrobial therapy in fracture-related infection: A consensus from an international expert group. J. Orthop. Trauma 2020, 34, 30–41. [Google Scholar] [CrossRef]
- Pesch, S.; Hanschen, M.; Greve, F.; Zyskowski, M.; Seidl, F.; Kirchhoff, C.; Biberthaler, P.; Huber-Wagner, S. Treatment of fracture-related infection of the lower extremity with antibiotic-eluting ceramic bone substitutes: Case series of 35 patients and literature review. Infection 2020, 48, 333–344. [Google Scholar] [CrossRef]
- Metsemakers, W.-J.; Fragomen, A.T.; Moriarty, T.F.; Morgenstern, M.; Egol, K.; Zalavras, C.; Obremskey, W.T.; Raschke, M.; McNally, M.A. Evidence-based recommendations for local antimicrobial strategies and dead space management in Fracture-related Infection. J. Orthop. Trauma 2019, 34, 18–29. [Google Scholar] [CrossRef]
- McNally, M.; Govaert, G.; Dudareva, M.; Morgenstern, M.; Metsemakers, W.-J. Definition and diagnosis of fracture-related infection. EFORT Open Rev. 2020, 5, 614–619. [Google Scholar] [CrossRef]
- Kuehl, R.; Sutter, S.T.; Morgenstern, M.; Dangel, M.; Egli, A.; Nowakowski, A.; Suhm, N.; Theilacker, C.; Widmer, A.F. Time-dependent differences in management and microbiology of orthopaedic internal fixation-associated infections: An observational prospective study with 229 patients. Clin. Microbiol. Infect. 2019, 25, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Conway, J.; Mansour, J.; Kotze, K.; Specht, S.; Shabtai, L. Antibiotic cement-coated rods: An effective treatment for infected long bones and prosthetic joint nonunions. Bone Jt. J. 2014, 96-B, 1349–1354. [Google Scholar] [CrossRef]
- Makhdom, A.M.; Buksbaum, J.; Rozbruch, S.R.; Da Cunha, R.; Fragomen, A.T. Antibiotic Cement-Coated interlocking Intramedullary Nails in the Treatment of Septic Complex Lower Extremity Reconstruction; A Retrospective Analysis with Two year Minimum Follow Up. J. Bone Jt. Infect. 2020, 5, 176–183. [Google Scholar] [CrossRef]
- Chadayammuri, V.; Herbert, B.; Hao, J.; Mavrogenis, A.; Quispe, J.C.; Kim, J.W.; Young, H.; Hake, M.; Mauffrey, C. Factors associated with adverse postoperative outcomes in patients with long bone post-traumatic osteomyelitis. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 877–882. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Kortram, K.; Morgenstern, M.; Moriarty, T.F.; Meex, I.; Kuehl, R.; Nijs, S.; Richards, R.G.; Raschke, M.; Borens, O.; et al. Definition of infection after fracture fixation: A systematic review of randomized controlled trials to evaluate current practice. Injury 2018, 49, 497–504. [Google Scholar] [CrossRef] [Green Version]
- Metsemakers, W.J.; Kuehl, R.; Moriarty, T.F.; Richards, R.G.; Verhofstad, M.H.; Borens, O.; Kates, S.; Morgenstern, M. Infection after fracture fixation: Current surgical and microbiological concepts. Injury 2018, 49, 511–522. [Google Scholar] [CrossRef] [Green Version]
- Hotchen, A.J.; Dudareva, M.; Corrigan, R.A.; Ferguson, J.Y.; McNally, M.A. Can we predict outcome after treatment of long bone osteomyelitis? A study of patient-reported quality of life, stratified with the BACH Classification. Bone Jt. J. 2020, 102-B, 1587–1596. [Google Scholar] [CrossRef]
- Dudareva, M.; Hotchen, A.; McNally, M.A.; Hartmann-Boyce, J.; Scarborough, M.; Collins, G. Systematic review of risk prediction studies in bone and joint infection: Are modifiable prognostic factors useful in predicting recurrence? J. Bone Jt. Infect. 2021, 6, 257–271. [Google Scholar] [CrossRef]
- Walter, N.; Baertl, S.; Engelstaedter, U.; Ehrenschwender, M.; Hitzenbichler, F.; Alt, V.; Rupp, M. Letter in response to article in journal of infection: “The microbiology of chronic osteomyeleitis: Changes over ten years”. J. Infect. 2021, 83, 709–737. [Google Scholar] [CrossRef]
- British orthopaedic Association Trauma Committee. BOA Standard for Trauma: Open frature management. Injury 2020, 51, 174–177. [Google Scholar] [CrossRef]
- The FLOW Investigators. A trial of wound irrigation in the initial management of open fracture wounds. N. Engl. J. Med. 2015, 373, 2629–2641. [Google Scholar] [CrossRef] [Green Version]
- Sendi, P.; McNally, M.A. Wound irrigation in initial management of open fractures. N. Engl. J. Med. 2016, 374, 1788–1790. [Google Scholar]
- Mifsud, M.; McNally, M.A. Local delivery of antimicrobials in the treatment of bone infections. Orthop. Trauma 2019, 33, 160–165. [Google Scholar] [CrossRef]
- Ferguson, J.; Diefenbeck, M.; McNally, M. Ceramic biocomposites as biodegradable antibiotic carriers in the treatment of bone infections. J. Bone Jt. Infect. 2017, 2, 41–54. [Google Scholar] [CrossRef] [Green Version]
- Morgenstern, M.; Vallejo, A.; McNally, M.; Moriarty, F.; Ferguson, J.; Nijs, S.; Metsemakers, W. The effect of local antibiotic prophylaxis in open limb fractures: A systematic review and meta-analysis. Bone Jt. Res. 2018, 7, 447–456. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Treatment Success | Treatment Failure | |
|---|---|---|---|
| (n = 374) | (n = 59) | ||
| Age (mean, range) | 49.8 (18 to 84) | 48.2 (20 to 74) | |
| Gender | Male | 270 | 48 |
| Female | 104 | 11 | |
| BMI | 27.5 (12.5 to 47.0) | 27.5 (18.5 to 40.8) | |
| Current smoking | Yes | 84 (22.5%) | 28 (47.5%) |
| No | 290 | 31 | |
| Diabetes mellitus | 39 (10.4%) | 8 (13.6%) | |
| Immunosuppressant use | 14 (3.7%) | 3 (5.4%) | |
| Time from injury to surgery in weeks | 33.8 (0 to 3432) | 23.3 (1 to 1820) | |
| Mean (range) median | 48 | 35 | |
| Diagnostic criteria | Sinus or fistula | 199 (53.2%) | 25 (42.4%) |
| Purulence in fracture site | 138 (37.0%) | 25 (42.4%) | |
| Microbiology ≥2 specimens culture-positive | 282 (75.4%) | 51 (86.4%) | |
| Microbiology 1 specimen positive | 36 (9.6%) | 3 (5.1%) | |
| Histopathology positive | 157 (42.0%) | 14 (23.7%) | |
| Histopathology negative | 68 (18.2%) | 3 (5.4%) | |
| Pre-operative CRP (mean, range) | 53.6 (0 to 480) | 57.4 (1 to 274) | |
| Bone | Tibia | 189 | 37 |
| Fibula | 12 | 1 | |
| Foot | 13 | 6 | |
| Femur | 81 | 13 | |
| Pelvis | 26 | 0 | |
| Clavicle | 6 | 0 | |
| Humerus | 20 | 0 | |
| Radius/ulna | 24 | 2 | |
| Other | 3 | 0 | |
| Fracture healed? | Yes | 172 (46.0%) | 18 (30.5%) |
| No | 202 (54.0%) | 41 (69.5%) | |
| Pre-operative fixation? | None | 122 (32.6%) | 13 (22.0%) |
| Internal | 249 (66.6%) | 42 (71.1%) | |
| External | 3 (0.8%) | 4 (6.8%) | |
| Followed-up (survivors *) | At least 12 months | 363/368 (98.6%) | 58/58 (100%) |
| At least 24 months | 170/363 (46.8%) | 38/58 (65.5%) | |
| Amputation or mortality during follow-up | 4 amputations 7 deaths | 5 amputations 1 death |
| Variable | Treatment Success | Treatment Failure | |
|---|---|---|---|
| (n = 374) | (n = 59) | ||
| Surgical approach | Debridement +/− implant removal | 182 (48.7%) | 19 (32.2%) |
| External fixation | 61 (16.3%) | 7 (11.9%) | |
| Internal fixation | 21 (5.6%) | 3 (5.1%) | |
| DAIR | 110 (29.4%) | 30 (50.8%) | |
| Closure and plastic surgical approach | Direct closure | 259 (69.2%) | 41 (69.5%) |
| Split skin graft only | 5 (1.3%) | 4 (6.8%) | |
| Local flap | 39 (10.4%) | 8 (13.6%) | |
| Free flap | 71 (19.0%) | 6 (10.2%) | |
| NPWT used prior to skin closure | Yes | 45 (12%) | 19 (32.2%) |
| No | 329 (88%) | 40 (67.8%) | |
| Local anti-microbial therapy | Yes | 227 (60.7%) | 25 (42.4%) |
| No | 147 (39.3%) | 34 (57.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McNally, M.; Corrigan, R.; Sliepen, J.; Dudareva, M.; Rentenaar, R.; IJpma, F.; Atkins, B.L.; Wouthuyzen-Bakker, M.; Govaert, G. What Factors Affect Outcome in the Treatment of Fracture-Related Infection? Antibiotics 2022, 11, 946. https://doi.org/10.3390/antibiotics11070946
McNally M, Corrigan R, Sliepen J, Dudareva M, Rentenaar R, IJpma F, Atkins BL, Wouthuyzen-Bakker M, Govaert G. What Factors Affect Outcome in the Treatment of Fracture-Related Infection? Antibiotics. 2022; 11(7):946. https://doi.org/10.3390/antibiotics11070946
Chicago/Turabian StyleMcNally, Martin, Ruth Corrigan, Jonathan Sliepen, Maria Dudareva, Rob Rentenaar, Frank IJpma, Bridget L. Atkins, Marjan Wouthuyzen-Bakker, and Geertje Govaert. 2022. "What Factors Affect Outcome in the Treatment of Fracture-Related Infection?" Antibiotics 11, no. 7: 946. https://doi.org/10.3390/antibiotics11070946
APA StyleMcNally, M., Corrigan, R., Sliepen, J., Dudareva, M., Rentenaar, R., IJpma, F., Atkins, B. L., Wouthuyzen-Bakker, M., & Govaert, G. (2022). What Factors Affect Outcome in the Treatment of Fracture-Related Infection? Antibiotics, 11(7), 946. https://doi.org/10.3390/antibiotics11070946