
Causative Pathogens Do Not Differ between Early, Delayed or Late Fracture-Related Infections

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Demographics
2.2. Type of Infection in Early, Delayed and Late Infections
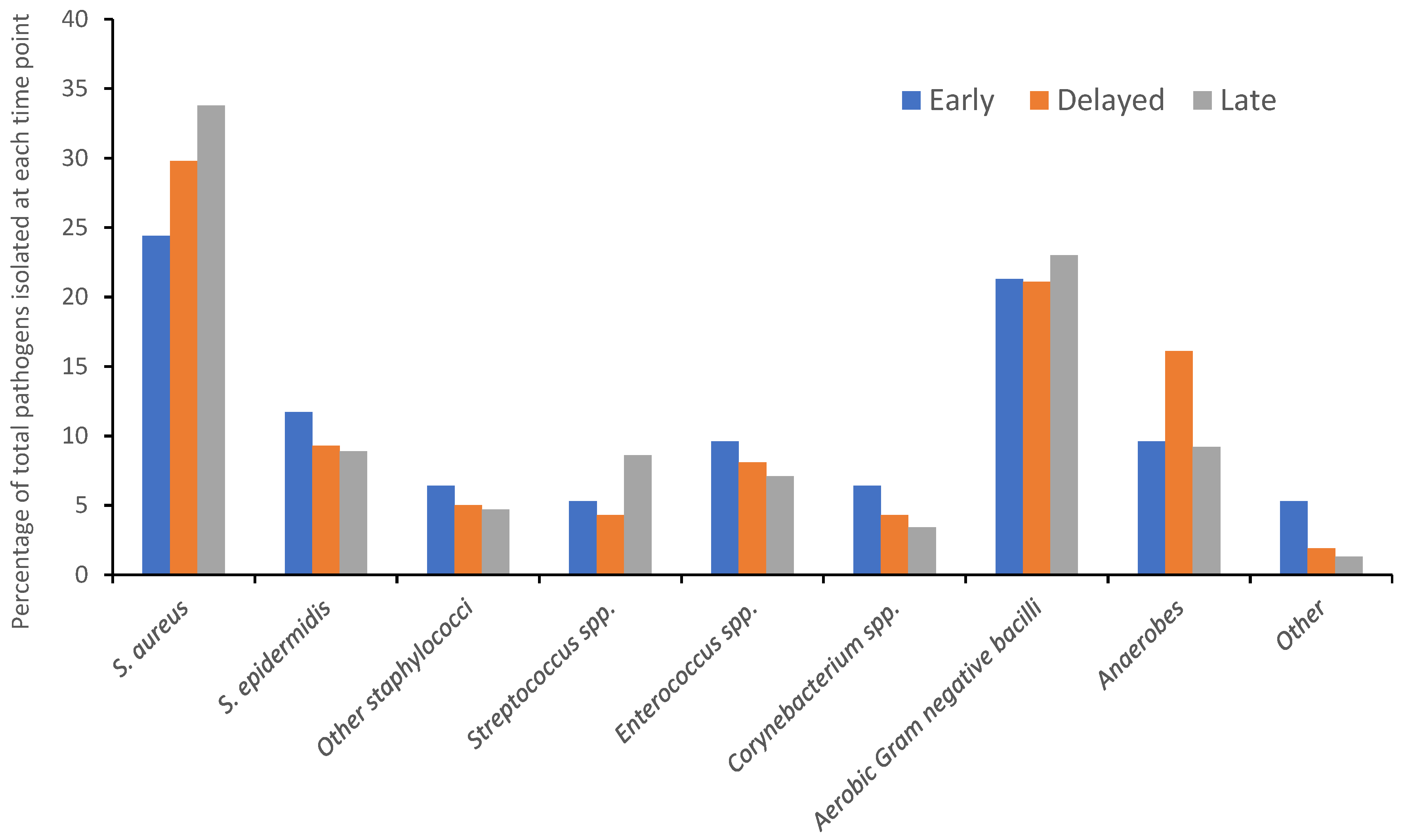
2.3. Pathogens Isolated in Early, Delayed and Late Infections
2.3.1. Staphylococcus aureus
2.3.2. Other Staphylococci
2.3.3. Gram-negative Aerobic Bacteria
2.4. Difficult to Treat’ Infections
2.5. Sub-Analysis of Patients Managed with DAIR
3. Discussion
3.1. Late FRI Are More Likely to Be Culture-Negative
3.2. Assumptions Regarding Different Pathogens in Early, Delayed and Late FRI Should Not Be Used to Guide Antimicrobial Therapy
3.3. The Role of Biofilm in Early, Late and Delayed FRI Remains Unclear
3.4. Biofilm-Active Antibiotics and FRI Managed with DAIR
3.5. Limitations and Future Work
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Metsemakers, W.-J.; Onsea, J.; Neutjens, E.; Steffens, E.; Schuermans, A.; McNally, M.; Nijs, S. Prevention of fracture-related infection: A multidisciplinary care package. Int. Orthop. 2017, 41, 2457–2469. [Google Scholar] [CrossRef] [Green Version]
- Olesen, U.K.; Pedersen, N.J.; Eckardt, H.; Lykke-Meyer, L.; Bonde, C.T.; Singh, U.M.; McNally, M. The cost of infection in severe open tibial fractures treated with a free flap. Int. Orthop. 2017, 41, 1049–1055. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Morgenstern, M.; McNally, M.A.; Moriarty, T.F.; McFadyen, I.; Scarborough, M.; Athanasou, N.A.; Ochsner, P.E.; Kuehl, R.; Raschke, M.; et al. Fracture-related infection: A consensus on definition from an international expert group. Injury 2018, 49, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Metsemakers, W.J.; Morgenstern, M.; Senneville, E.; Borens, O.; Govaert, G.A.M.; Onsea, J.; Depypere, M.; Richards, R.G.; Trampuz, A.; Verhofstad, M.H.J.; et al. General treatment principles for fracture-related infection: Recommendations from an international expert group. Arch. Orthop. Trauma Surg. 2020, 140, 1013–1027. [Google Scholar] [CrossRef] [Green Version]
- Depypere, M.; Kuehl, R.; Metsemakers, W.J.; Senneville, E.; McNally, M.A.; Obremskey, W.T.; Zimmerli, W.; Atkins, B.L.; Trampuz, A.; Fracture-Related Infection Consensus Group. Recommendations for Systemic Antimicrobial Therapy in Fracture-Related Infection: A Consensus From an International Expert Group. J. Orthop. Trauma 2020, 34, 30–41. [Google Scholar] [CrossRef]
- Baertl, S.; Walter, N.; Engelstaedter, U.; Ehrenschwender, M.; Hitzenbichler, F.; Alt, V.; Rupp, M. What Is the Most Effective Empirical Antibiotic Treatment for Early, Delayed, and Late Fracture-Related Infections? Antibiotics 2022, 11, 287. [Google Scholar] [CrossRef]
- Willenegger, H.; Roth, B. Treatment tactics and late results in early infection following osteosynthesis. Unfallchirurgie 1986, 12, 241–246. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Kuehl, R.; Moriarty, T.F.; Richards, R.G.; Verhofstad, M.H.J.; Borens, O.; Kates, S.; Morgenstern, M. Infection after fracture fixation: Current surgical and microbiological concepts. Injury 2018, 49, 511–522. [Google Scholar] [CrossRef] [Green Version]
- Zimmerli, W.; Moser, C. Pathogenesis and treatment concepts of orthopaedic biofilm infections. FEMS Immunol. Med. Microbiol. 2012, 65, 158–168. [Google Scholar] [CrossRef] [Green Version]
- Depypere, M.; Morgenstern, M.; Kuehl, R.; Senneville, E.; Moriarty, T.F.; Obremskey, W.T.; Zimmerli, W.; Trampuz, A.; Lagrou, K.; Metsemakers, W.J. Pathogenesis and management of fracture-related infection. Clin. Microbiol. Infect. 2020, 26, 572–578. [Google Scholar] [CrossRef]
- Kuehl, R.; Tschudin-Sutter, S.; Morgenstern, M.; Dangel, M.; Egli, A.; Nowakowski, A.; Suhm, N.; Theilacker, C.; Widmer, A.F. Time-dependent differences in management and microbiology of orthopaedic internal fixation-associated infections: An observational prospective study with 229 patients. Clin. Microbiol. Infect. 2019, 25, 76–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkes, M.; Obremskey, W.T.; Scannell, B.; Ellington, J.K.; Hymes, R.A.; Bosse, M.; Southeast Fracture, C. Maintenance of hardware after early postoperative infection following fracture internal fixation. J. Bone Jt. Surg. 2010, 92, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Zimmerli, W. Diagnosis and treatment of infections associated with fracture-fixation devices. Injury 2006, 37, S59–S66. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, M.; Kuehl, R.; Zalavras, C.G.; McNally, M.; Zimmerli, W.; Burch, M.A.; Vandendriessche, T.; Obremskey, W.T.; Verhofstad, M.H.J.; Metsemakers, W.J. The influence of duration of infection on outcome of debridement and implant retention in fracture-related infection. Bone Jt. J. 2021, 103, 213–221. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.; Corrigan, R.; Sliepen, J.; Hietbrink, F.; IJpma, F.; Wouthuyzen-Bakker, M.; Rentenaar, R.; Atkins, B.; Govaert, G. What Affects Outcome After Treatment of Fracture-Realted Infection? Orthop. Proc. 2021, 103, 14. [Google Scholar]
- Akgun, D.; Perka, C.; Trampuz, A.; Renz, N. Outcome of hip and knee periprosthetic joint infections caused by pathogens resistant to biofilm-active antibiotics: Results from a prospective cohort study. Arch. Orthop. Trauma Surg. 2018, 138, 635–642. [Google Scholar] [CrossRef]
- WHO. Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 3 July 2022).
- Vijayakumar, A.B.; Reddy, Y.P.; Suphala, B.; Gopalakrishnan, A.; Vinod Kumar, C.S. Microbiological and antibiotic profile of osteomyelitis in tertiary care hospital. Int. Surg. J. 2021, 8, 910–914. [Google Scholar] [CrossRef]
- Walter, N.; Baertl, S.; Engelstaedter, U.; Ehrenschwender, M.; Hitzenbichler, F.; Alt, V.; Rupp, M. Letter in response to article in journal of infection: “The microbiology of chronic osteomyelitis: Changes over ten years”. J. Infect. 2021, 83, 709–737. [Google Scholar] [CrossRef]
- Kortram, K.; Bezstarosti, H.; Metsemakers, W.J.; Raschke, M.J.; Van Lieshout, E.M.M.; Verhofstad, M.H.J. Risk factors for infectious complications after open fractures; a systematic review and meta-analysis. Int. Orthop. 2017, 41, 1965–1982. [Google Scholar] [CrossRef] [Green Version]
- Gitajn, I.L.; Heng, M.; Weaver, M.J.; Ehrlichman, L.K.; Harris, M.B. Culture-Negative Infection After Operative Fixation of Fractures. J. Orthop. Trauma 2016, 30, 538–544. [Google Scholar] [CrossRef]
- van Sloten, M.; Gómez-Junyent, J.; Ferry, T.; Rossi, N.; Petersdorf, S.; Lange, J.; Corona, P.; Araújo Abreu, M.; Borens, O.; Zlatian, O.; et al. Should all patients with a culture-negative periprosthetic joint infection be treated with antibiotics? A multicentre observational study. Bone Jt. J. 2022, 104, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Atkins, B.L.; Athanasou, N.; Deeks, J.J.; Crook, D.W.; Simpson, H.; Peto, T.E.; McLardy-Smith, P.; Berendt, A.R. Prospective evaluation of criteria for microbiological diagnosis of prosthetic-joint infection at revision arthroplasty. The OSIRIS Collaborative Study Group. J. Clin. Microbiol. 1998, 36, 2932–2939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudareva, M.; Barrett, L.; Figtree, M.; Scarborough, M.; Watanabe, M.; Newnham, R.; Wallis, R.; Oakley, S.; Kendrick, B.; Stubbs, D.; et al. Sonication versus Tissue Sampling for Diagnosis of Prosthetic Joint and Other Orthopedic Device-Related Infections. J. Clin. Microbiol. 2018, 56, e00688-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Eiff, C.; Peters, G.; Becker, K. The small colony variant (SCV) concept—The role of staphylococcal SCVs in persistent infections. Injury 2006, 37 (Suppl. 2), S26–S33. [Google Scholar] [CrossRef]
- Proctor, R.A.; von Eiff, C.; Kahl, B.C.; Becker, K.; McNamara, P.; Herrmann, M.; Peters, G. Small colony variants: A pathogenic form of bacteria that facilitates persistent and recurrent infections. Nat. Rev. Microbiol. 2006, 4, 295–305. [Google Scholar] [CrossRef]
- Yang, D.; Wijenayaka, A.R.; Solomon, L.B.; Pederson, S.M.; Findlay, D.M.; Kidd, S.P.; Atkins, G.J. Novel Insights into Staphylococcus aureus Deep Bone Infections: The Involvement of Osteocytes. MBio 2018, 9, e00415-18. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Yu, A.; Doern, G.V. Diagnostic Value of a PCR-Based Technique for Prosthetic Joint Infection. J. Clin. Microbiol. 2014, 52, 2281–2282. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Lu, Q.; Liu, T.; Li, Z.; Cai, W. Bacterial resistance trends among intraoperative bone culture of chronic osteomyelitis in an affiliated hospital of South China for twelve years. BMC Infect. Dis. 2019, 19, 823. [Google Scholar] [CrossRef]
- Corrigan, R.A.; Dudareva, M.; McNally, M. Increasing antimicrobial resistance is not inevitable in reply to microbiological and antibiotic profile of osteomyelitis in tertiary care hospital. Int. Surg. J. 2021, 8, 1967–1968. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Marotta, C.; Amicone, M.; Bavaro, D.F.; Bernaudo, F.; Frisicale, E.M.; Kurotschka, P.K.; Mazzari, A.; Veronese, N.; Murri, R.; et al. Italian young doctors’ knowledge, attitudes and practices on antibiotic use and resistance: A national cross-sectional survey. J. Glob. Antimicrob. Resist. 2020, 23, 167–173. [Google Scholar] [CrossRef]
- Zimmerli, W.; Sendi, P. Orthopaedic biofilm infections. APMIS 2017, 125, 353–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, P.S. Antimicrobial Tolerance in Biofilms. Microbiol. Spectr. 2015, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tre-Hardy, M.; Mace, C.; El Manssouri, N.; Vanderbist, F.; Traore, H.; Devleeschouwer, M.J. Effect of antibiotic co-administration on young and mature biofilms of cystic fibrosis clinical isolates: The importance of the biofilm model. Int. J. Antimicrob. Agents 2009, 33, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Tomizawa, T.; Nishitani, K.; Ito, H.; Okae, Y.; Morita, Y.; Doi, K.; Saito, M.; Ishie, S.; Yoshida, S.; Murata, K.; et al. The limitations of mono- and combination antibiotic therapies on immature biofilms in a murine model of implant-associated osteomyelitis. J. Orthop. Res. 2021, 39, 449–457. [Google Scholar] [CrossRef]
- Saginur, R.; Stdenis, M.; Ferris, W.; Aaron, S.D.; Chan, F.; Lee, C.; Ramotar, K. Multiple combination bactericidal testing of staphylococcal biofilms from implant-associated infections. Antimicrob. Agents Chemother. 2006, 50, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Zimmerli, W.; Widmer, A.F.; Blatter, M.; Frei, R.; Ochsner, P.E. Role of rifampin for treatment of orthopedic implant-related staphylococcal infections: A randomized controlled trial. Foreign-Body Infection (FBI) Study Group. JAMA 1998, 279, 1537–1541. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, O.E.; Borgen, P.; Bragnes, B.; Figved, W.; Grogaard, B.; Rydinge, J.; Sandberg, L.; Snorrason, F.; Wangen, H.; Witsoe, E.; et al. Rifampin combination therapy in staphylococcal prosthetic joint infections: A randomized controlled trial. J. Orthop. Surg. Res. 2020, 15, 365. [Google Scholar] [CrossRef]
- Scheper, H.; Gerritsen, L.M.; Pijls, B.G.; Van Asten, S.A.; Visser, L.G.; De Boer, M.G.J. Outcome of Debridement, Antibiotics, and Implant Retention for Staphylococcal Hip and Knee Prosthetic Joint Infections, Focused on Rifampicin Use: A Systematic Review and Meta-Analysis. Open Forum Infect. Dis. 2021, 8, ofab298. [Google Scholar] [CrossRef]
- McNally, M.; Govaert, G.; Dudareva, M.; Morgenstern, M.; Metsemakers, W.J. Definition and diagnosis of fracture-related infection. EFORT Open Rev. 2020, 5, 614–619. [Google Scholar] [CrossRef]
- Hellebrekers, P.; Rentenaar, R.J.; McNally, M.A.; Hietbrink, F.; Houwert, R.M.; Leenen, L.P.H.; Govaert, G.A.M. Getting it right first time: The importance of a structured tissue sampling protocol for diagnosing fracture-related infections. Injury 2019, 50, 1649–1655. [Google Scholar] [CrossRef] [Green Version]
- Minassian, A.M.; Newnham, R.; Kalimeris, E.; Bejon, P.; Atkins, B.L.; Bowler, I.C. Use of an automated blood culture system (BD BACTEC) for diagnosis of prosthetic joint infections: Easy and fast. BMC Infect. Dis. 2014, 14, 233. [Google Scholar] [CrossRef] [PubMed]
- Talsma, D.T.; Ploegmakers, J.J.W.; Jutte, P.C.; Kampinga, G.; Wouthuyzen-Bakker, M. Time to positivity of acute and chronic periprosthetic joint infection cultures. Diagn. Microbiol. Infect. Dis. 2021, 99, 115178. [Google Scholar] [CrossRef] [PubMed]
- Hughes, H.C.; Newnham, R.; Athanasou, N.; Atkins, B.L.; Bejon, P.; Bowler, I.C. Microbiological diagnosis of prosthetic joint infections: A prospective evaluation of four bacterial culture media in the routine laboratory. Clin. Microbiol. Infect. 2011, 17, 1528–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| 0–2 Weeks | 3–10 Weeks | >10 Weeks | Whole Group | Significance | |
|---|---|---|---|---|---|
| Patient Demographics | |||||
| Number of cases | 51 | 82 | 300 | 433 | |
| Age (median, years; IQR) | 50; 32–60 | 52; 36–63 | 50; 37–62 | 51; 36–62 | p = 0.85 |
| Sex (% male) | 67 | 67 | 76 | 70 | p = 0.12 |
| BMI (median; IQR) | 23.6 *; 22.8–24.9 | 25.4; 23.0–29.6 | 27.8 *; 23.6–31.6 | 27.3; 23.4–31.0 | * p = 0.004 |
| Time since injury (median, weeks; IQR) | 2; 1–2 | 5; 4–8 | 112; 40–737 | 44; 6–342 | |
| Bone Involved | |||||
| Tibia/fibula | 24 (47%) | 47 (57%) | 166 (55%) | 237 | p < 0.001 |
| Femur | 10 (20%) | 8 (10%) | 76 (25%) | 94 | |
| Upper limb | 5 (10%) | 8 (10%) | 39 (13%) | 52 | |
| Pelvis | 8 (16%) | 11 (13%) | 7 (2%) | 26 | p = 0.17 (tibia/fibula, femur, upper limb only) |
| Foot | 4 (8%) | 7 (9%) | 8 (3%) | 19 | |
| Other | 0 | 1 (1%) | 4 (1%) | 5 | |
| Culture Type | |||||
| Culture-negative | 2 (4%) *** | 6 (7%) | 72 (24%) *** | 80 (19%) | *** p < 0.0001 |
| Monomicrobial | 19 (37%) | 30 (37%) | 150 (50%) | 199 (46%) | |
| Polymicrobial | 30 (59%) ** | 46 (56%) *** | 78 (26%) **,*** | 154 (36%) | ** p = 0.0004, *** p < 0.0001 |
| Species Isolated | |||||
| S. aureus | 23 (24%) | 48 (30%) | 129 (34%) | 200 (31%) | p = 0.20 |
| S. epidermidis | 11 (12%) | 15 (9%) | 34 (9%) | 60 (9%) | |
| Other staphylococci | 6 (6%) | 8 (5%) | 18 (5%) | 32 (5%) | |
| Streptococcus spp. | 5 (5%) | 7 (4%) | 33 (9%) | 45 (7%) | |
| Enterococcus spp. | 9 (10%) | 13 (8%) | 27 (7%) | 49 (8%) | |
| Corynebacterium spp. | 6 (6%) | 7 (4%) | 13 (3%) | 26 (4%) | |
| Aerobic Gram-neg. bacilli | 20 (21%) | 34 (21%) | 88 (23%) | 142 (22%) | |
| Anaerobes | 9 (10%) | 26 (16%) | 35 (9%) | 70 (11%) | |
| Other | 5 (5%) | 3 (2%) | 5 (1%) | 13 (2%) | |
| Total | 94 | 161 | 382 | 637 |
| 0–2 Weeks | 3–10 Weeks | >10 Weeks | Whole Group | Significance | |
|---|---|---|---|---|---|
| Patient Demographics | |||||
| Number of cases | 45 | 62 | 33 | 140 | |
| Age (median, years; IQR) | 50; 32–60 | 53; 37–63 | 55; 36–64 | 53; 35–63 | p = 0.63 |
| Sex (% male) | 64 | 63 | 73 | 66 | p = 0.62 |
| BMI (median; IQR) | 23.5 *; 22.8–24.3 | 25.5; 23.4–29.9 | 30.7 *; 26.2–35.5 | 25.7; 23.1–31.2 | * p = 0.027 |
| Time since injury (median, weeks; IQR) | 2; 1–2 | 5; 4–6 | 45; 28–97 | 4; 2–8 | |
| Bone Involved | |||||
| Tibia/fibula | 21 (47%) | 34 (55%) | 15 (45%) | 70 | p = 0.26 |
| Femur | 9 (20%) | 7 (11%) | 10 (30%) | 26 | |
| Upper limb | 5 (11%) | 5 (8%) | 4 (12%) | 14 | |
| Pelvis | 8 (18%) | 10 (16%) | 2 (6%) | 20 | |
| Foot | 2 (4%) | 6 (10%) | 1 (3%) | 9 | |
| Other | 0 (0%) | 0 (0%) | 1 (3%) | 1 | |
| Culture Type | |||||
| Culture-negative | 2 (4%) | 3 (5%) | 2 (6%) | 7 (5%) | p = 0.52 |
| Monomicrobial | 18 (40%) | 23 (37%) | 18 (55%) | 59 (42%) | |
| Polymicrobial | 25 (56%) | 36 (58%) | 13 (39%) | 74 (53%) | |
| Species Isolated | |||||
| S. aureus | 20 (24%) | 40 (33%) | 21 (35%) | 81 (30%) | p = 0.56 |
| S. epidermidis | 8 (10%) | 12 (10%) | 8 (13%) | 28 (11%) | |
| Other staphylococci | 5 (6%) | 6 (5%) | 4 (7%) | 15 (6%) | |
| Streptococcus spp. | 4 (5%) | 6 (5%) | 6 (10%) | 16 (6%) | |
| Enterococcus spp. | 8 (10%) | 8 (7%) | 3 (5%) | 19 (7%) | |
| Corynebacterium spp. | 6 (7%) | 5 (4%) | 3 (5%) | 14 (5%) | |
| Aerobic Gram-neg. bacilli | 17 (21%) | 19 (16%) | 5 (8%) | 41 (16%) | |
| Anaerobes | 10 (12%) | 23 (19%) | 10 (17%) | 43 (16%) | |
| Other | 4 (5%) | 3 (3%) | 0 | 7 (3%) | |
| Total | 82 | 122 | 60 | 264 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corrigan, R.A.; Sliepen, J.; Dudareva, M.; IJpma, F.F.A.; Govaert, G.; Atkins, B.L.; Rentenaar, R.; Wouthuyzen-Bakker, M.; McNally, M. Causative Pathogens Do Not Differ between Early, Delayed or Late Fracture-Related Infections. Antibiotics 2022, 11, 943. https://doi.org/10.3390/antibiotics11070943
Corrigan RA, Sliepen J, Dudareva M, IJpma FFA, Govaert G, Atkins BL, Rentenaar R, Wouthuyzen-Bakker M, McNally M. Causative Pathogens Do Not Differ between Early, Delayed or Late Fracture-Related Infections. Antibiotics. 2022; 11(7):943. https://doi.org/10.3390/antibiotics11070943
Chicago/Turabian StyleCorrigan, Ruth A., Jonathan Sliepen, Maria Dudareva, Frank F. A. IJpma, Geertje Govaert, Bridget L. Atkins, Rob Rentenaar, Marjan Wouthuyzen-Bakker, and Martin McNally. 2022. "Causative Pathogens Do Not Differ between Early, Delayed or Late Fracture-Related Infections" Antibiotics 11, no. 7: 943. https://doi.org/10.3390/antibiotics11070943
APA StyleCorrigan, R. A., Sliepen, J., Dudareva, M., IJpma, F. F. A., Govaert, G., Atkins, B. L., Rentenaar, R., Wouthuyzen-Bakker, M., & McNally, M. (2022). Causative Pathogens Do Not Differ between Early, Delayed or Late Fracture-Related Infections. Antibiotics, 11(7), 943. https://doi.org/10.3390/antibiotics11070943