
Effect of Fluoroquinolone Use in Primary Care on the Development and Gradual Decay of Escherichia coli Resistance to Fluoroquinolones: A Matched Case-Control Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Summary of the Principal Findings
3.2. Findings of the Present Study in Light of Previous Observations
3.3. Strengths and Limitations of the Study
3.4. Meaning of the Study and Implication for Practice and Policy
3.5. Implications for Future Research
4. Methods
4.1. Study Design, Setting and Data Sources
- The database of hospital reference laboratories was used to define cases and controls.
- The database of outpatient pharmaceutical prescriptions was used to define the exposure.
- The hospital discharge record database was used to identify potential risk factors.
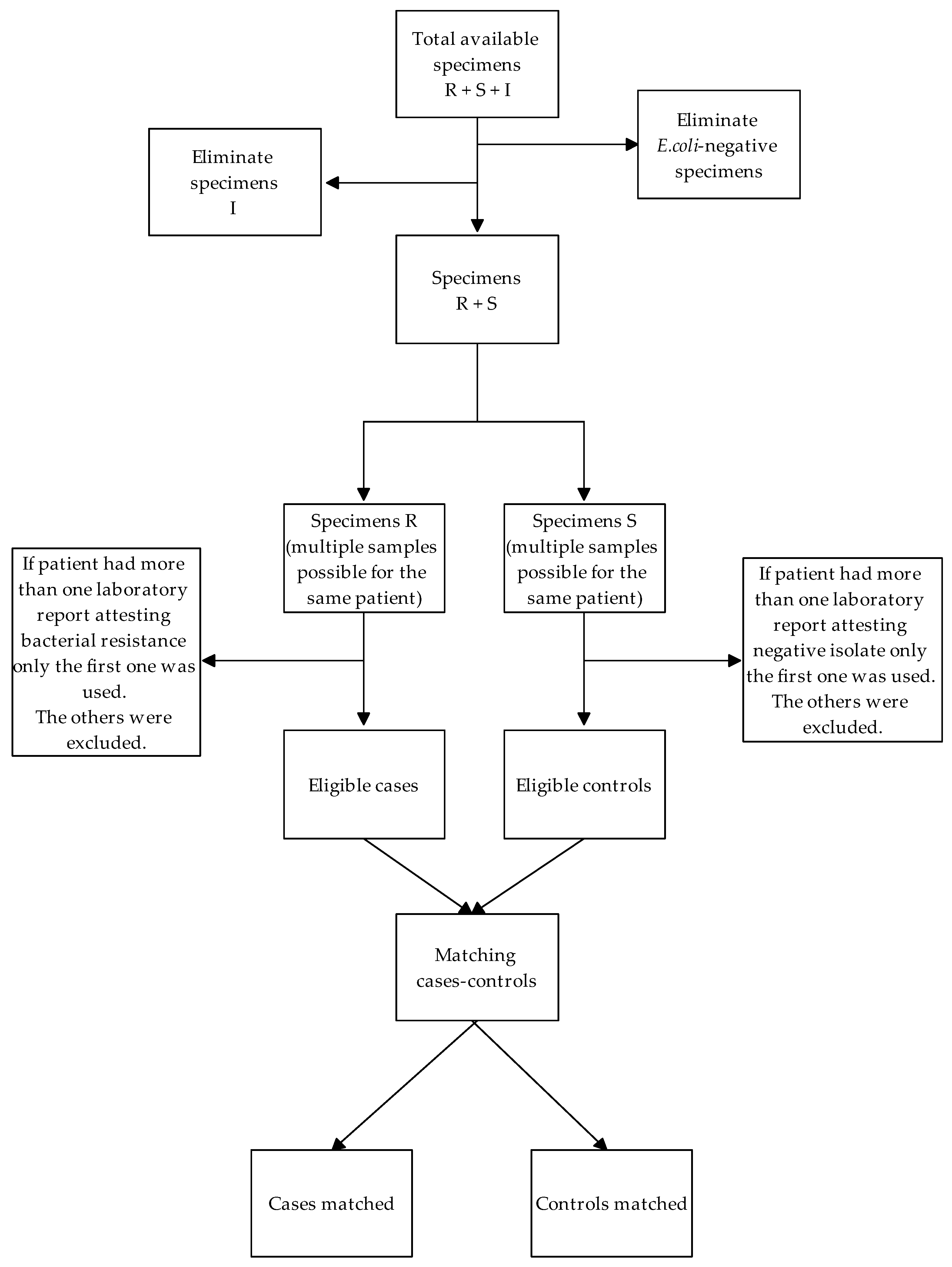
4.2. Definition of Cases and Controls
4.3. Definition of Exposure
4.4. Statistical Analysis
4.5. Sensitivity Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spellberg, B.; Bartlett, J.G.; Gilbert, D.N. The future of antibiotics and resistance. N. Engl. J. Med. 2013, 368, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.N. Antimicrobial resistance: Are we at the dawn of the post-antibiotic era? JR Coll. Physicians Edinb. 2016, 46, 150–156. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Review on Antimicrobial Resistance. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. 2014. Available online: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf (accessed on 4 April 2022).
- World Health Organization. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://apps.who.int/iris/handle/10665/193736 (accessed on 4 April 2022).
- Curtis, H.J.; Walker, A.J.; Mahtani, K.R.; Goldacre, B. Time trends and geographical variation in prescribing of antibiotics in England 1998–2017. J. Antimicrob. Chemother. 2019, 74, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Majeed, A.; Moser, K. Age- and sex-specific antibiotic prescribing patterns in general practice in England and Wales in 1996. Br. J. Gen. Pract. 1999, 49, 735–736. [Google Scholar]
- Bakhit, M.; Hoffmann, T.; Scott, A.M.; Beller, E.; Rathbone, J.; Del Mar, C. Resistance decay in individuals after antibiotic exposure in primary care: A systematic review and meta-analysis. BMC Med. 2018, 16, 126. [Google Scholar] [CrossRef]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [Green Version]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: Systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef] [Green Version]
- Fulgenzio, C.; Massari, M.; Traversa, G.; Da Cas, R.; Ferrante, G.; Aschbacher, R.; Moser, V.; Pagani, E.; Vestri, A.R.; Massidda, O.; et al. Impact of Prior Antibiotic Use in Primary Care on Escherichia coli Resistance to Third Generation Cephalosporins: A Case-Control Study. Antibiotics 2021, 10, 451. [Google Scholar] [CrossRef]
- Schmiemann, G.; Gágyor, I.; Hummers-Pradier, E.; Bleidorn, J. Resistance profiles of urinary tract infections in general practice—An observational study. BMC Urol. 2012, 12, 33. [Google Scholar] [CrossRef] [Green Version]
- Klingeberg, A.; Noll, I.; Willrich, N.; Feig, M.; Emrich, D.; Zill, E.; Krenz-Weinreich, A.; Kalka-Moll, W.; Oberdorfer, K.; Schmiemann, G.; et al. Antibiotic-Resistant E. coli in Uncomplicated Community-Acquired Urinary Tract Infection. Dtsch. Ärzteblatt Int. 2018, 115, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, A.E.; Wagenlehner, F.M.E.; Mulgirigama, A.; Twynholm, M. Escherichia coli Resistance to Fluoroquinolones in Community-Acquired Uncomplicated Urinary Tract Infection in Women: A Systematic Review. Antimicrob. Agents Chemother. 2020, 64, e00862-20. [Google Scholar] [CrossRef] [PubMed]
- Hammond, A.; Stuijfzand, B.; Avison, M.B.; Hay, A.D. Antimicrobial resistance associations with national primary care antibiotic stewardship policy: Primary care-based, multilevel analytic study. PLoS ONE 2020, 15, e0232903. [Google Scholar] [CrossRef]
- Cuevas, O.; Oteo, J.; Lázaro, E.; Aracil, B.; de Abajo, F.; García-Cobos, S.; Ortega, A.; Campos, J. Significant ecological impact on the progression of fluoroquinolone resistance in Escherichia coli with increased community use of moxifloxacin, levofloxacin and amoxicillin/clavulanic acid. J. Antimicrob. Chemother. 2011, 66, 664–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundqvist, M.; Geli, P.; Andersson, D.I.; Sjölund-Karlsson, M.; Runehagen, A.; Cars, H.; Abelson-Storby, K.; Cars, O.; Kahlmeter, G. Little evidence for reversibility of trimethoprim resistance after a drastic reduction in trimethoprim use. J. Antimicrob. Chemother. 2010, 65, 350–360. [Google Scholar] [CrossRef]
- Enne, V.I.; Livermore, D.M.; Stephens, P.; Hall, L.M. Persistence of sulphonamide resistance in Escherichia coli in the UK despite national prescribing restriction. Lancet 2001, 357, 1325–1328. [Google Scholar] [CrossRef]
- Aliabadi, S.; Anyanwu, P.; Beech, E.; Jauneikaite, E.; Wilson, P.; Hope, R.; Majeed, A.; Muller-Pebody, B.; Costelloe, C. Effect of antibiotic stewardship interventions in primary care on antimicrobial resistance of Escherichia coli bacteraemia in England 2013–18: A quasi-experimental, ecological, data linkage study. Lancet Infect. Dis. 2021, 21, 1689–1700. [Google Scholar] [CrossRef]
- Livermore, D.M.; Hope, R.; Reynolds, R.; Blackburn, R.; Johnson, A.P.; Woodford, N. Declining cephalosporin and fluoroquinolone non-susceptibility among bloodstream Enterobacteriaceae from the UK: Links to prescribing change? J. Antimicrob. Chemother. 2013, 68, 2667–2674. [Google Scholar] [CrossRef] [Green Version]
- Holmes, A.H.; Moore, L.S.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Vellinga, A.; Murphy, A.W.; Hanahoe, B.; Bennett, K.; Cormican, M. A multilevel analysis of trimethoprim and ciprofloxacin prescribing and resistance of uropathogenic Escherichia coli in general practice. J. Antimicrob. Chemother. 2010, 65, 1514–1520. [Google Scholar] [CrossRef] [Green Version]
- Zhu, D.-M.; Li, Q.-H.; Shen, Y.; Zhang, Q. Risk factors for quinolone-resistant Escherichia coli infection: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2020, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.; Roberts, Z.; Dunstan, F.; Butler, C.; Howard, A.; Palmer, S. Prior antibiotics and risk of antibiotic-resistant community-acquired urinary tract infection: A case-control study. J. Antimicrob. Chemother. 2007, 60, 92–99. [Google Scholar] [CrossRef]
- Alam, M.F.; Cohen, D.; Butler, C.; Dunstan, F.; Roberts, Z.; Hillier, S.; Palmer, S. The additional costs of antibiotics and re-consultations for antibiotic-resistant Escherichia coli urinary tract infections managed in general practice. Int. J. Antimicrob. Agents 2009, 33, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Kaußner, Y.; Röver, C.; Heinz, J.; Hummers, E.; Debray, T.; Hay, A.; Heytens, S.; Vik, I.; Little, P.; Moore, M.; et al. Reducing antibiotic use in uncomplicated urinary tract infections in adult women: A systematic review and individual participant data meta-analysis. Clin. Microbiol. Infect. 2022; in press. [Google Scholar]
- Fraile Navarro, D.; Sullivan, F.; Azcoaga-Lorenzo, A.; Hernandez Santiago, V. Point-of-care tests for urinary tract infections: Protocol for a systematic review and meta-analysis of diagnostic test accuracy. BMJ Open 2020, 10, e033424. [Google Scholar] [CrossRef]
- Osservatorio Nazionale sull’impiego dei Medicinali. L’uso degli antibiotici in Italia. Rapporto Nazionale 2019; Agenzia Italiana del Farmaco (AIFA): Roma, Italy, 2020. [Google Scholar]
- Popolazione residente—2016. ASTAT Istituto Provinciale di Statistica. Provincia Autonoma di Bolzano—Alto Adige. Available online: https://astat.provinz.bz.it/barometro/upload/statistikatlas/it/atlas.html#!bev/wohnbevbdv/wohnbev (accessed on 20 January 2021).
- EUCAST Expert rules in antimicrobial susceptibility testing, version 1. April 2008. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/4ESCMID_Library/3Publications/EUCAST_Documents/Other_Documents/EUCAST_Expert_rules_final_April_20080407.pdf (accessed on 12 May 2022).
- WHO Collaborating Centre for Drug Statistics Methodology. Anatomical Therapeutic Chemical (ATC) classification system: Guidelines for ATC classification and DDD assignment. Oslo: Norwegian Institute of Public Health. 2020. Available online: https://www.whocc.no/filearchive/publications/2020_guidelines_web.pdf (accessed on 6 September 2020).
- International Classification of Diseases, 9th revision. Clinical Modification, 5th ed.; Medicode: Salt Lake City, UT, USA, 1995. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 17; StataCorp LLC.: College Station, TX, USA, 2021. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing [Internet], Vienna, Austria. 2016. Available online: https://www.R-project.org/ (accessed on 29 April 2022).


{kind=link}
| Variable | Cases a N = 403 | Controls a N = 933 | Crude OR (95% CI) | p |
|---|---|---|---|---|
| Age, Median (IQ) | 78 (68–85) | 74 (59–84) | 1.17 b (1.10–1.25) | <0.0001 |
| Gender, Male (%) | 176 (43.03) | 291 (31.19) | 1.66 (1.30–2.11) | <0.0001 |
| Drug’s DDD taken in previous 5 years, Median (IQ) | 4760 (1741–8074) | 2869 (256–6190) | 1.07 c (1.04–1.10) | <0.0001 |
| Number of active ingredients taken in previous 5 years, Median (IQ) | 17 (9–24) | 10 (4–18) | 1.05 (1.04–1.06) | <0.0001 |
| At least one FQ in previous 1st year (%) | 161 (39.36) | 148 (15.86) | 3.87 (2.88–5.18) | <0.0001 |
| At least one FQ taken in previous 2nd year (%) | 129 (31.54) | 142 (15.22) | 2.72 (2.04–3.64) | <0.0001 |
| At least one FQ taken in previous 3rd, 4th or 5th year (%) | 173 (42.30) | 261 (27.97) | 1.90 (1.49–2.44) | <0.0001 |
| FQ prescriptions in previous year (%) 0 | 248 (60.64) | 785 (84.14) | Ref. | |
| 1 | 72 (17.60) | 83 (8.90) | 3.14 (2.17–4.53) | <0.0001 |
| 2 | 40 (9.78) | 35 (3.75) | 3.80 (2.33–6.19) | <0.0001 |
| 3+ | 49 (11.98) | 30 (3.22) | 6.00 (3.55–10.17) | <0.0001 |
| Number of hospitalizations in previous 5 years, Median (IQ) | 4 (2–8) | 2 (0–4) | 3.67 (2.76–4.88) | <0.0001 |
| Hospitalization days, Median (IQ) | 48 (12–116) | 10 (0–41) | 1.07 d (1.05–1.09) | <0.0001 |
| Hospitalization with surgery (%) | 206 (50.37) | 370 (39.66) | 1.54 (1.23–1.95) | <0.0001 |
| Hospitalization with device implantation (%) | 44 (10.76) | 65 (6.97) | 1.57 (1.05–2.36) | 0.029 |
| Hospitalization with organ transplant (%) | 9 (2.20) | 18 (1.93) | 1.19 (0.53–2.66) | 0.673 |
| Diagnosis of chronic diseases (%) Cancer | 92 (22.49) | 156 (16.72) | 1.48 (1.11–1.98) | 0.008 |
| Diabetes | 108 (26.41) | 146 (15.65) | 1.90 (1.44–2.51) | <0.0001 |
| COPD | 166 (40.59) | 244 (26.15) | 2.01 (1.56–2.59) | <0.0001 |
| End-stage renal disease | 10 (2.44) | 15 (1.61) | 1.67 (0.75–3.72) | 0.213 |
| Variable | Adjusted OR (95% CI) | p |
|---|---|---|
| At least one FQ prescription in 1st previous year | 2.67 (1.92–3.70) | <0.0001 |
| At least one FQ prescription taken in previous 2nd year | 1.54 (1.09–2.17) | 0.015 |
| At least one FQ prescription taken in previous 3rd, 4th or 5th year | 1.09 (0.80–1.48) | 0.997 |
| Age | 1.09 a (1.01–1.18) | 0.026 |
| Gender, male | 1.42 (1.07–1.88) | 0.016 |
| Hospitalization days | 1.03 b (1.01–1.06) | 0.022 |
| Diagnosis of chronic diseasesDiabetes | 1.41 (0.96–1.80) | 0.037 |
| COPD | 1.43 (1.05–1.87) | 0.019 |
| Variables | Adjusted OR (95%CI) | p |
|---|---|---|
| FQ prescription in previous year 0 | Ref. | Ref. |
| 1 | 2.40 (1.62–3.56) | <0.0001 |
| 2 | 2.76 (1.63–4.66) | <0.0001 |
| 3+ | 4.21 (2.38–7.50) | <0.0001 |
| At least one other J01 prescription in previous year | 1.10 (0.83–1.45) | 0.516 |
| Age | 1.11 a (1.03–1.20) | 0.008 |
| Gender | 1.39 (1.05–1.84) | 0.010 |
| Hospitalization days | 1.03 b (1.01–1.06) | 0.020 |
| Diagnosis of chronic diseases Diabetes | 1.40 (1.02–1.93) | 0.037 |
| COPD | 1.46 (1.09–1.96) | 0.004 |
| Potential Confounding Factor | Data Source |
|---|---|
| Age | hospital discharge records database |
| Gender | hospital discharge records database |
| Drug’s DDD taken in previous 5 years | database of drug prescription records |
| Number of active ingredients taken in previous 5 years | database of drug prescription records |
| Number of antibiotics taken in previous 5 years | database of drug prescription records |
| One or more J01 prescription taken in previous 5, 4 and 3 years | database of drug prescription records |
| One or more J01 prescription taken in previous 2 years | database of drug prescription records |
| Hospitalization days | hospital discharge records database |
| Hospitalizations | hospital discharge records database |
| Hospitalizations with surgery | hospital discharge records database |
| Hospitalizations with device implantation | hospital discharge records database |
| Hospitalizations with organ transplant | hospital discharge records database |
| Diagnosis of chronic diseases | hospital discharge records database |
| Cancer | |
| Diabetes Mellitus | |
| COPD | |
| Hemodialysis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurotschka, P.K.; Fulgenzio, C.; Da Cas, R.; Traversa, G.; Ferrante, G.; Massidda, O.; Gágyor, I.; Aschbacher, R.; Moser, V.; Pagani, E.; et al. Effect of Fluoroquinolone Use in Primary Care on the Development and Gradual Decay of Escherichia coli Resistance to Fluoroquinolones: A Matched Case-Control Study. Antibiotics 2022, 11, 822. https://doi.org/10.3390/antibiotics11060822
Kurotschka PK, Fulgenzio C, Da Cas R, Traversa G, Ferrante G, Massidda O, Gágyor I, Aschbacher R, Moser V, Pagani E, et al. Effect of Fluoroquinolone Use in Primary Care on the Development and Gradual Decay of Escherichia coli Resistance to Fluoroquinolones: A Matched Case-Control Study. Antibiotics. 2022; 11(6):822. https://doi.org/10.3390/antibiotics11060822
Chicago/Turabian StyleKurotschka, Peter Konstantin, Chiara Fulgenzio, Roberto Da Cas, Giuseppe Traversa, Gianluigi Ferrante, Orietta Massidda, Ildikó Gágyor, Richard Aschbacher, Verena Moser, Elisabetta Pagani, and et al. 2022. "Effect of Fluoroquinolone Use in Primary Care on the Development and Gradual Decay of Escherichia coli Resistance to Fluoroquinolones: A Matched Case-Control Study" Antibiotics 11, no. 6: 822. https://doi.org/10.3390/antibiotics11060822
APA StyleKurotschka, P. K., Fulgenzio, C., Da Cas, R., Traversa, G., Ferrante, G., Massidda, O., Gágyor, I., Aschbacher, R., Moser, V., Pagani, E., Spila Alegiani, S., & Massari, M. (2022). Effect of Fluoroquinolone Use in Primary Care on the Development and Gradual Decay of Escherichia coli Resistance to Fluoroquinolones: A Matched Case-Control Study. Antibiotics, 11(6), 822. https://doi.org/10.3390/antibiotics11060822