
Prevalence and Correlates of Self-Medication Practices for Prevention and Treatment of COVID-19: A Systematic Review

 ,
,  , ,
, , 
Abstract
:1. Introduction
Objectives
2. Methods
2.1. Data Source
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Study Data Management and Extraction
2.6. Assessment of the Risk of Bias
2.7. Statistical Analysis
3. Results
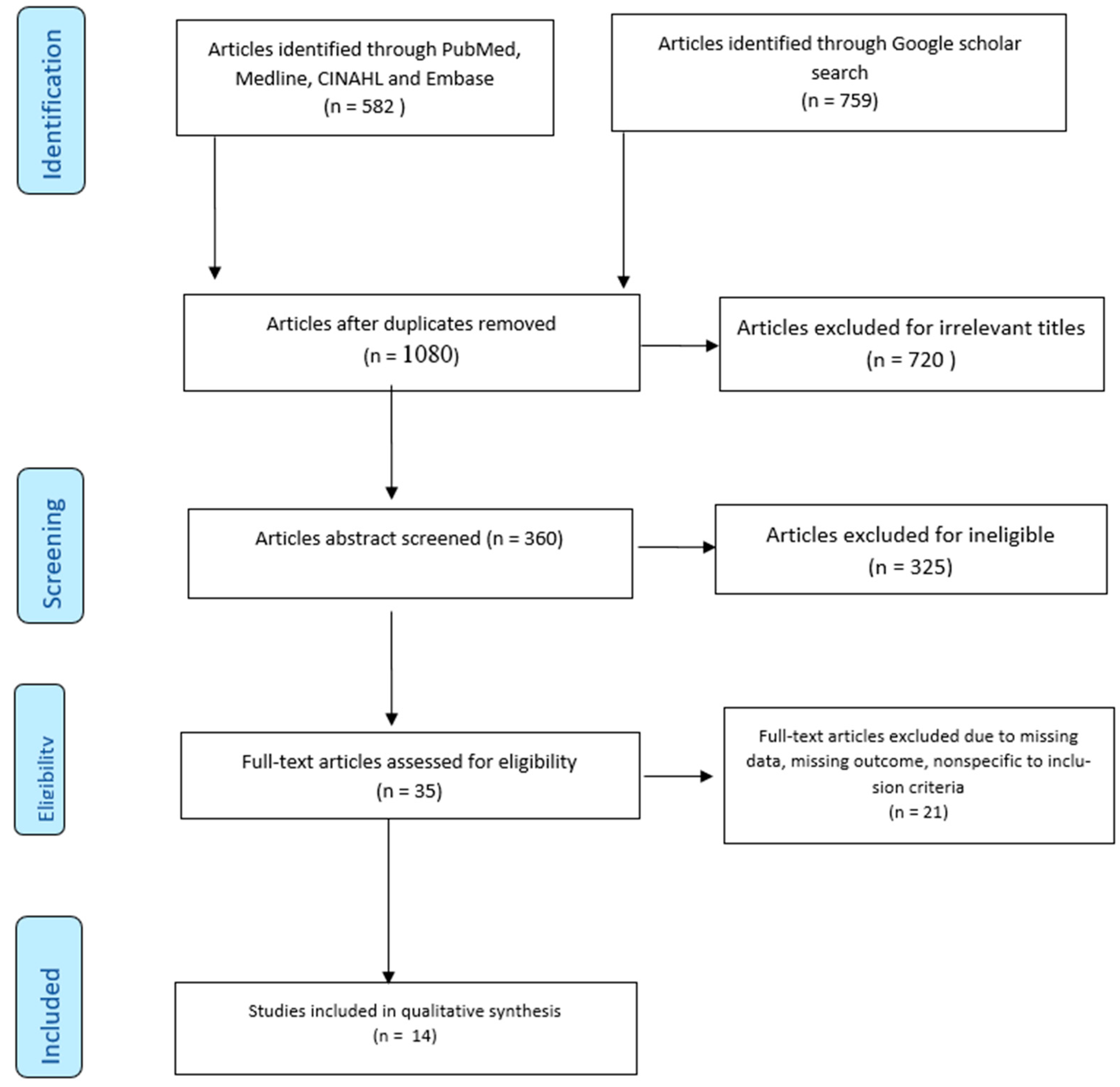
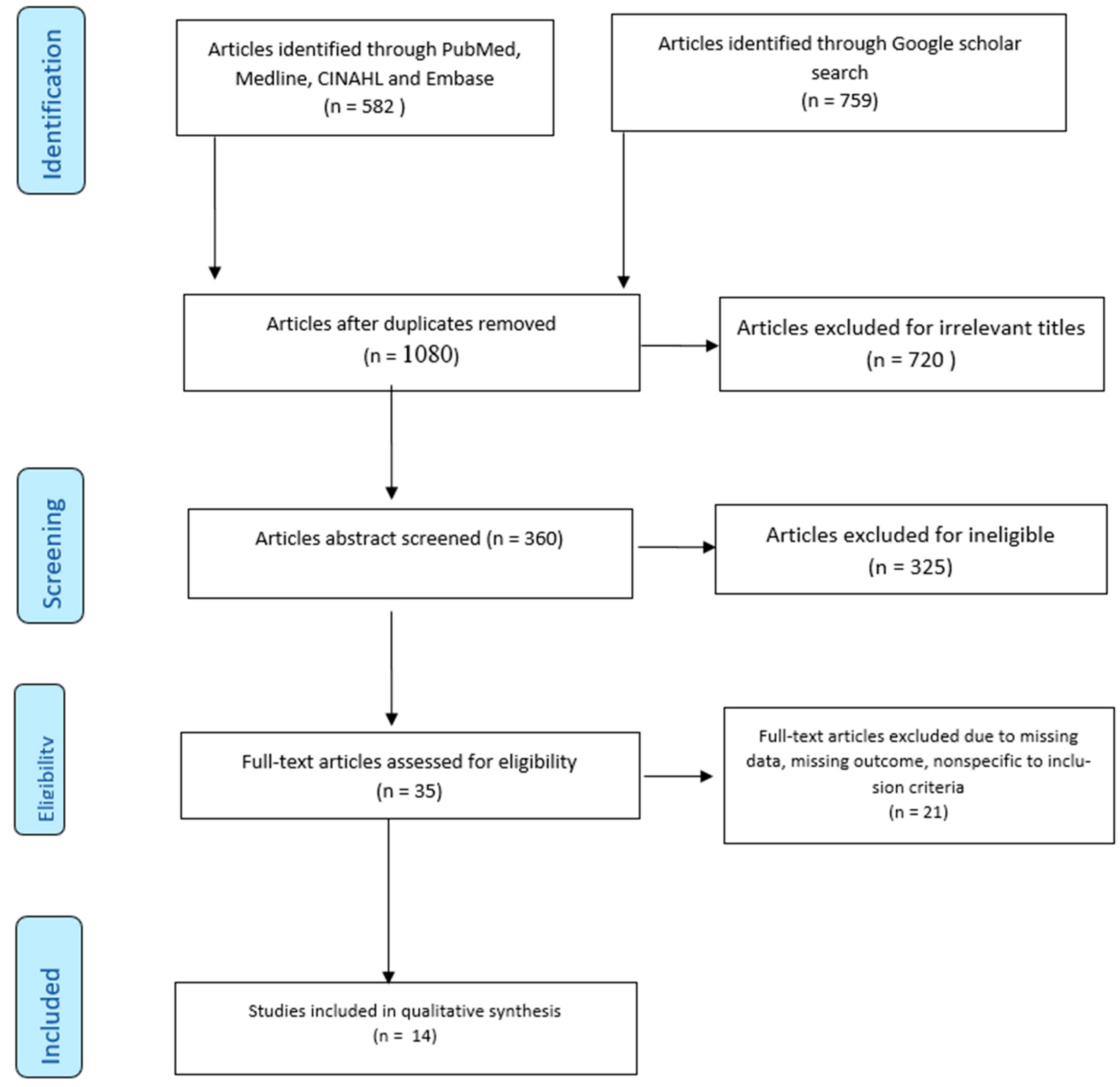
3.1. Study Selection
3.1.1. The Methodological Quality of the Included Studies
3.1.2. Studies’ Characteristics
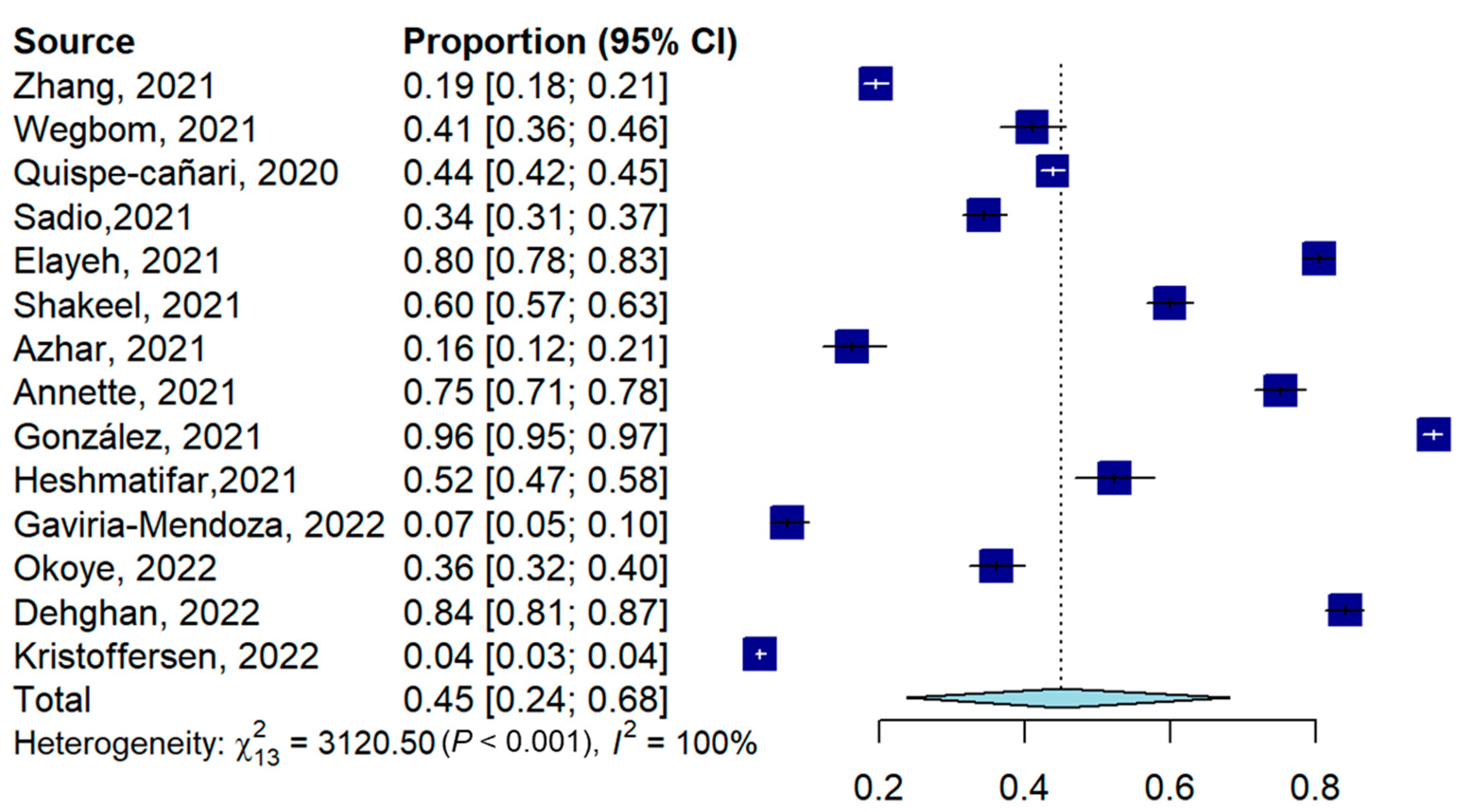
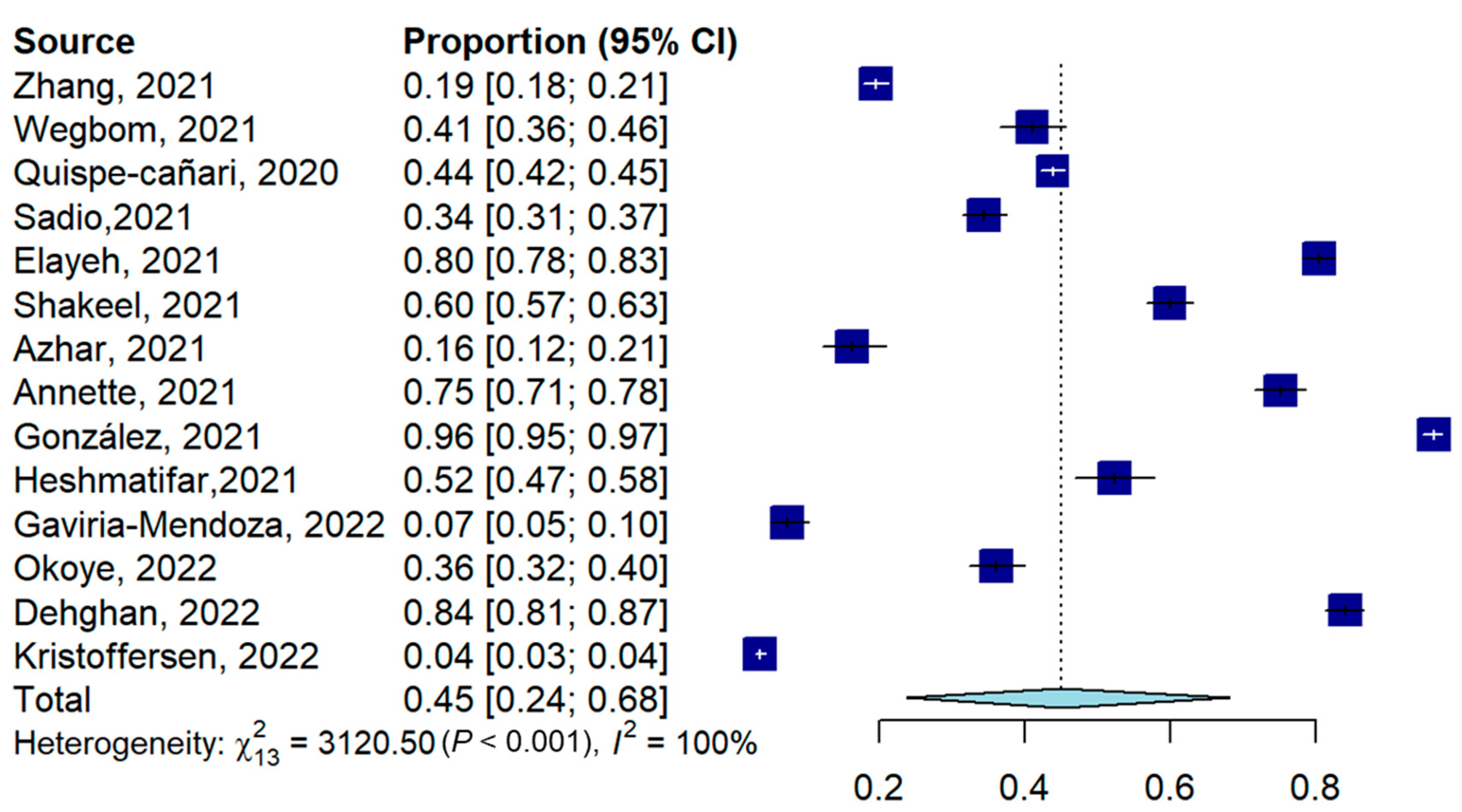
3.2. Prevalence of Self-Medication for Prevention and Treatment of COVID-19
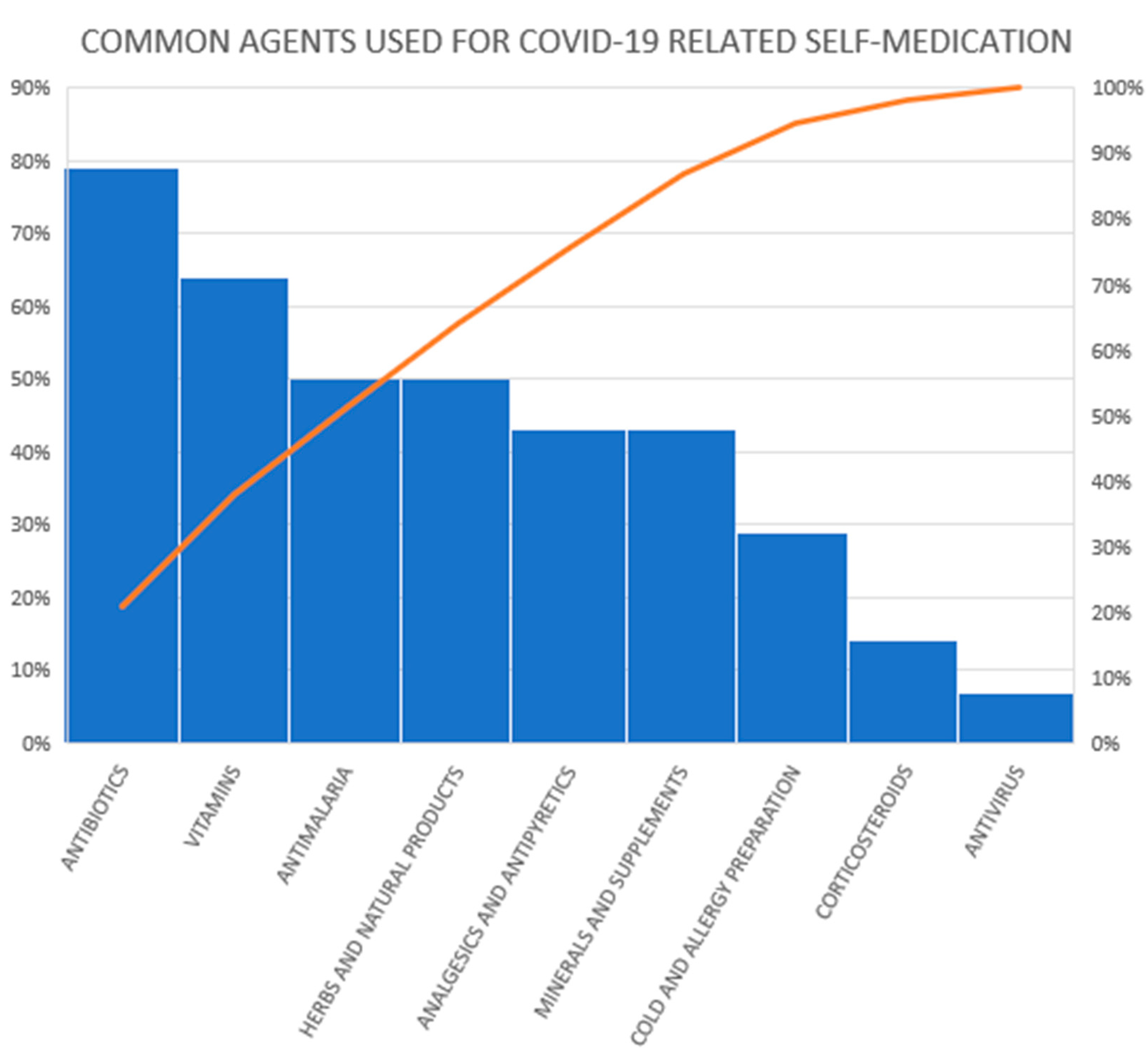
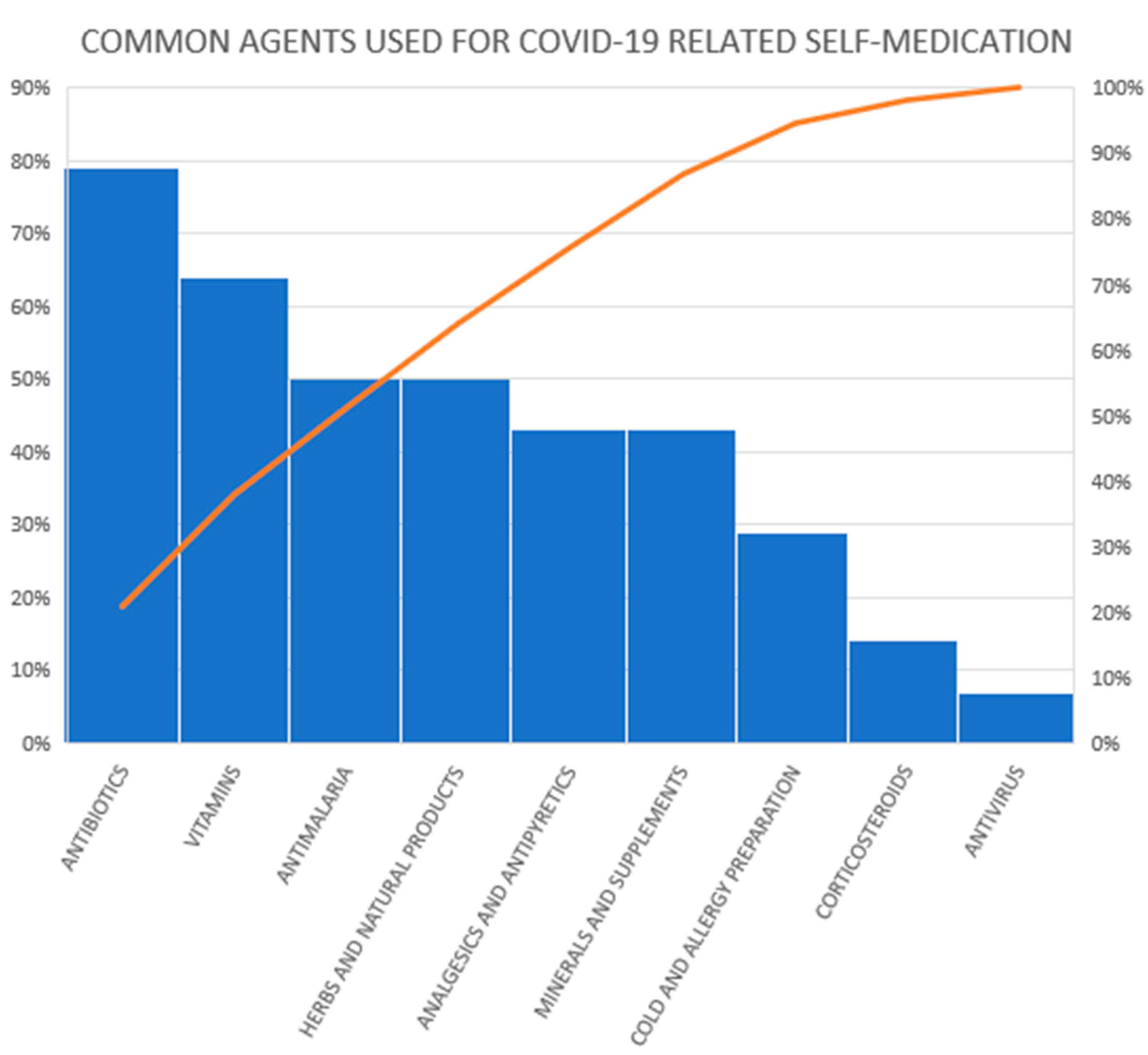
3.3. The Agents Used for Self-Medication
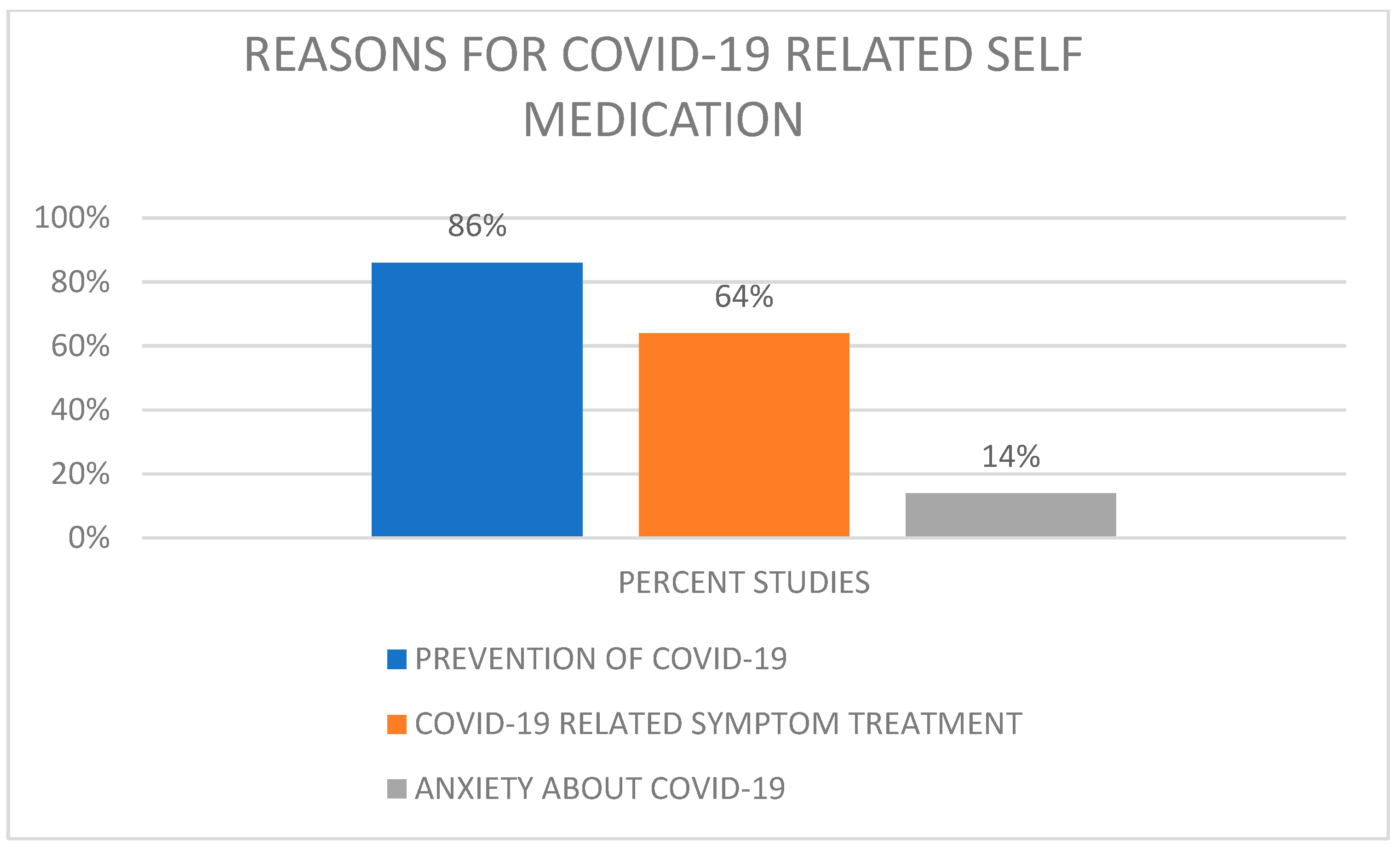
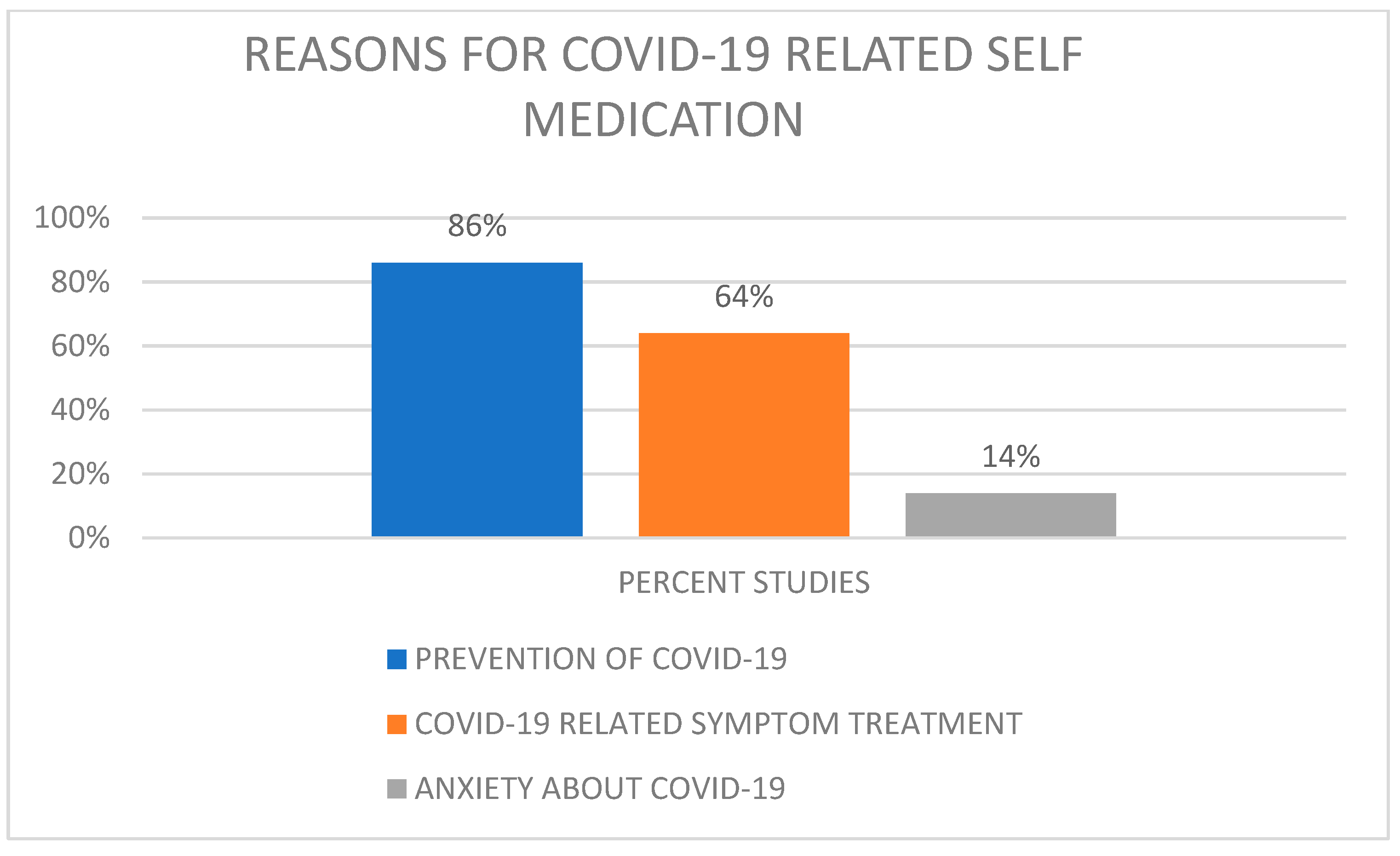
3.4. Reasons for Self-Medication and Correlates of Self-Medication
3.5. Sources of Information about Self-Medication
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Center for Disease Control and Prevention. Coronavirus Prevention-Social Distancing. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-distancing.html (accessed on 2 January 2022).
- Oliver, N.; Barber, X.; Roomp, K.; Roomp, K. Assessing the Impact of the COVID-19 Pandemic in Spain: Large-Scale, Online, Self-Reported Population Survey. J. Med. Internet Res. 2020, 22, e21319. [Google Scholar] [CrossRef] [PubMed]
- Bandara, N.A.; Mehrnoush, V.; Jhauj, R. Self-care during the pandemic. BC Med. J. 2020, 62, 194–195. [Google Scholar]
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Bio-Med. Atenei Parmensis. 2020, 91, 157–160. [Google Scholar]
- Balkhi, F.; Nasir, A.; Zehra, A.; Riaz, R. Psychological and Behavioral Response to the Coronavirus (COVID-19) Pandemic. Cureus 2020, 12, e7923. [Google Scholar] [CrossRef]
- Quispe-Cañari, J.F.; Fidel-Rosales, E.; Manrique, D.; Mascaró-Zan, J.; Huamán-Castillón, K.M.; Chamorro–Espinoza, S.E.; Garayar–Peceros, H.; Ponce–López, V.L.; Sifuentes-Rosales, J.; Alvarez-Risco, A.; et al. Self-medication practices during the COVID-19 pandemic among the adult population in Peru: A cross-sectional survey. Saudi Pharm. J. 2021, 29, 1–11. [Google Scholar] [CrossRef]
- Patel, S.R.; Pimpale, D.H.; Raje, S.S. Trends in the use of home-remedies and over-the-counter drugs during COVID-19 Pandemic: A Cross-Sectional Study. Indian J. Prev. Soc. Med. 2021, 52, 169–176. [Google Scholar]
- Palikhey, A.; Shrivastava, A.K.; Shrestha, L.; Gurung, S.; Yadav, C.K.; Pandit, M.; Shrestha, J. Self-medication Practices among Medical and Non-medical Students of Siddharthanagar, Nepal during COVID-19 Pandemic. J. Kist. Med. Col. 2021, 3, 40–48. [Google Scholar]
- Mutua, C.M.; Muthuka, J.K.; Muthoka, M.N.; Wambura, F.M. Pattern and Practices of Self Medication during COVID-19 Pandemic in Urban Settings, Kenya: “Does COVID-19 pandemic have a marginal Influence?”. IOSR J. Pharm. Biologic. Sci. (IOSR-JPBS) 2021, 16, 56–63. [Google Scholar]
- Mudassar, I.A.; Saira, S.; Ramesha, A.; Khurram, A. Assessment of Self-medication Practices During COVID-19 Pandemic in Hyderabad and Karachi, Pakistan. Sudan J. Med. Sci. 2021, 16, 347–354. [Google Scholar]
- Heshmatifar, N.; Davarinia, M.Q.A.; Mohammadzadeh, T.Z.; Moayed, L.; Moradi, S.; Rastagi, S.; Borzooei, F. Prevalence and Factors Related to Self-Medication for COVID-19 Prevention in the Elderly. Iranian J. Ageing 2021, 16, 112–127. [Google Scholar] [CrossRef]
- Azhar, H.; Tauseef, A.; Usman, T.; Azhar, Y.; Ahmed, M.; Umer, K.; Shoaib, M. Prevalence, Attitude and Knowledge of Self Medication during Covid-19 Disease Pandemic. Pakistan J. Med. Health Sci. 2021, 15, 902–905. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Worafi, Y.M. Self-medication. In Drug Safety in Developing Countries; Academic Press: Sana’a, Yemen, 2020; pp. 73–86. [Google Scholar]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balduzzi, S.; Rucker, G.; Schwarzer, G. How to perform a meta-analysis with 1. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzer, G.; Chemaitelly, H.; Abu-Raddad, L.J.; Rücker, G. Seriously misleading results using inverse of Freeman-Tukey double arcsine transformation in meta-analysis of single proportions. Res. Synth. Methods 2019, 10, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Wegbom, A.I.; Edet, C.K.; Raimi, O.; Fagbamigbe, A.F.; Kiri, V.A. Self-Medication Practices and Associated Factors in the Prevention and/or Treatment of COVID-19 Virus: A Population-Based Survey in Nigeria. Front. Public Health 2021, 9, 606801. [Google Scholar] [CrossRef]
- Annette, D.A.; Brihastami, S.; Zamal, N.; Riko, L. “Anti-COVID-19” Medications, Supplements, and Mental Health Status in Indonesian Mothers with School-Age Children. Int. J. Women’s Health 2021, 13, 699–709. [Google Scholar]
- Zhang, A.; Hobman, E.V.; De Barro, P.; Young, A.; Carter, D.J.; Byrne, M. Self-medication with antibiotics for protection against COVID-19, The role of psychological distress, knowledge of, and experiences with antibiotics. Antibiotics 2021, 10, 232. [Google Scholar] [CrossRef]
- Elayeh, E.; Akour, A.; Haddadin, R.N. Prevalence and predictors of self-medication drugs to prevent or treat COVID-19, Experience from a Middle Eastern country. Int. J. Clin. Pract. 2021, 75, 1–12. [Google Scholar] [CrossRef]
- Mir, S.A.; Shakeel, D.; Qadri, Z.L. Self-medication practices during covid-19 pandemic: A cross-sectional survey. Asian J. Pharm. Clin. Res. 2021, 14, 80–82. [Google Scholar]
- Sadio, A.J.; Gbeasor-Komlanvi, F.A.; Konu, R.Y.; Bakoubayi, A.W.; Tchankoni, M.K.; Bitty-Anderson, A.M.; Gomez, I.M.; Denadou, C.P.; Anani, J.; Kouanfack, H.R.; et al. Assessment of self-medication practices in the context of the COVID-19 outbreak in Togo. BMC Public Health 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gaviria-Mendoza, A.; Mejía-Mazo, D.A.; Duarte-Blandón, C.; Castrillón-Spitia, J.D.; Machado-Duque, M.E.; Valladales-Restrepo, L.F.; Machado-Alba, J.E. Self-medication and the ‘infodemic’during mandatory preventive isolation due to the COVID-19 pandemic. Ther. Adv. Drug. Saf. 2022, 13, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Okoye, O.C.; Adejumo, O.A.; Opadeyi, A.O.; Madubuko, C.R.; Ntaji, M.; Okonkwo, K.C.; Edeki, I.R.; Agboje, U.O.; Alli, O.E.; Ohaju-Obodo, J.O. Self medication practices and its determinants in health care professionals during the coronavirus disease-2019 pandemic: Cross-sectional study. Int. J. Clin. Pharm. 2022, 44, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.; Ghanbari, A.; Heidari, F.G.; Shahrbabaki, P.M.; Zakeri, M.A. Use of complementary and alternative medicine in general population during COVID-19 outbreak: A survey in Iran. J. Int. Med. 2022, 20, 45–51. [Google Scholar] [CrossRef]
- Kristoffersen, A.E.; van der Werf, E.T.; Stub, T.; Musial, F.; Wider, B.; Jong, M.C.; Wode, K.; Danell, J.A.; Busch, M.; Hoenders, H.R.; et al. Consultations with health care providers and use of self-management strategies for prevention and treatment of COVID-19 related symptoms. A population-based cross-sectional study in Norway, Sweden and the Netherlands. Complem. Ther. Med. 2022, 64, 102792. [Google Scholar] [CrossRef]
- de los Ángeles, M.; Minchala-Urgilés, R.E.; Ramírez-Coronel, A.A.; Aguayza-Perguachi, M.A.; Torres-Criollo, L.M.; Romero-Sacoto, L.A.; Luzmia, G.; Magdal, M.; Mercedes, F.; Isabel, N.; et al. Herbal medicine as prevention and treatment against COVID-19. Arch. Venez. De Farmacol. Y Ter. 2020, 5, 948–953. [Google Scholar]
- Limaye, D.; Limaye, V.; Krause, G.; Fortwengel, G. A systematic review of the literature to assess self-medication practices. Int. J. Commun. Med. Public Health 2017, 4, 2620–2631. [Google Scholar] [CrossRef] [Green Version]
- Gualano, M.R.; Bert, F.; Passi, S.; Stillo, M.; Galis, V.; Manzoli, L.; Siliquini, R. Use of self-medication among adolescents: A systematic review and meta-analysis. Eur. J. Pub. Health 2015, 25, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Shaghaghi, A.; Asadi, M.; Allahverdipour, H. Predictors of self-medication behavior: A systematic review. Iranian J. Pub. Health 2014, 43, 136–146. [Google Scholar]
- Kim, H.K.; Ahn, J.; Atkinson, L.; Kahlor, L.A. Effects of COVID-19 Misinformation on Information Seeking, Avoidance, and Processing: A Multicountry Comparative Study. Sci. Commun. 2020, 42, 586–615. [Google Scholar] [CrossRef]
- Ebrahim, A.; Saif, Z.; Buheji, M.; AlBasri, N.; Al-Husaini, F.; Jahrami, H. COVID-19 information-seeking behavior and anxiety symptoms among parents. OSP J. Health Care Med. 2020, 1, 1–9. [Google Scholar]
- Bento, A.I.; Nguyen, T.; Wing, C.; Lozano-Rojas, F.; Ahn, Y.-Y.; Simon, K. Evidence from internet search data shows information-seeking responses to news of local COVID-19 cases. Proc. Natl. Acad. Sci. USA 2020, 117, 11220–11222. [Google Scholar] [CrossRef] [PubMed]
- Alhomoud, F.; Aljamea, Z.; Almahasnah, R.; Alkhalifah, K.; Basalelah, L.; Alhomoud, F.K. Self-medication and self-prescription with antibiotics in the Middle East—do they really happen? A systematic review of the prevalence, possible reasons, and outcomes. Int. J. Infect. Dis. 2017, 57, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nepal, G.; Bhatta, S. Self-medication with antibiotics in WHO Southeast Asian Region: A systematic review. Cureus 2018, 10, e2428. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 2 January 2022).
- Bennadi, D. Self-medication: A current challenge. J. Basic Clin. Pharm. 2013, 5, 19–23. [Google Scholar] [CrossRef]
- Stosic, R.; Dunagan, F.; Palmer, H.; Fowler, T.; Adams, I. Responsible self-medication: Perceived risks and benefits of over-the-counter analgesic use. Int. J. Pharm. Pract. 2011, 19, 236–245. [Google Scholar] [CrossRef]
- Galato, D.; Galafassi, L.d.M.; Alano, G.M.; Trauthman, S.C. Responsible self-medication: Review of the process of pharmaceutical attendance. Brazil J. Pharm. Sci. 2009, 45, 625–633. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assessment Parameters | Zhang, 2021 | Wegbom, 2021 | Quispe-Cañari, 2020 | Sadio, 2021 | Elayeh, 2021 | Shakeel, 2021 | Azhar, 2021 | Annette d’arqom, 2021 | de los Ángeles, 2020 | Heshmatifar, 2021 | Gaviria-Mendoza, 2022 | Okoye et al., 2022 | Dehghan, 2022 | Kristoffersen, 2022 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Introduction | ||||||||||||||
| 1. Were the aims/objectives of the study clear? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Methods | ||||||||||||||
| 2. Was the study design appropriate for the stated aim(s)? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 3. Was the sample size justified? | No | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4. Was the target/reference population clearly defined? (Is it clear who the research was about?) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 5. Was the sample frame taken from an appropriate population base so that it closely represented the target/reference population under investigation? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| 6. Was the selection process likely to select subjects/participants that were representative of the target/reference population under investigation? | Yes | No | No | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | Yes | Yes |
| 7. Were measures undertaken to address and categorize non-responders? | No | No | No | No | No | No | No | No | No | No | No | No | No | No |
| 8. Were the risk factor and outcome variables measured appropriate to the aims of the study? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 9. Were the risk factor and outcome variables measured correctly using instruments/measurements that had been trialled, piloted or published previously? | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 10. Is it clear what was used to determine statistical significance and/or precision estimates? (e.g., p values, CIs) | Yes | Yes | Yes | Yes | Yes | ND | Yes | Yes | Yes | ND | Yes | Yes | Yes | Yes |
| 11. Were the methods (including statistical methods) sufficiently described to enable them to be repeated? | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Result | ||||||||||||||
| 12. Were the basic data adequately described? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 13. Did the response rate not raise concerns about non-response bias? | Yes | Yes | Yes | Yes | ND | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 14. If appropriate, was information about non-responders described? | No | No | No | No | No | No | No | No | No | No | No | No | No | No |
| 15. Were the results internally consistent? | ND | Yes | Yes | ND | ND | ND | ND | Yes | ND | ND | ND | ND | ND | ND |
| 16. Were the results for the analyses, as described in the methods, presented? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Discussion | ||||||||||||||
| 17. Were the authors’ discussions and conclusions justified by the results? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 18. Were the limitations of the study discussed? | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Others | ||||||||||||||
| 19. Was there information about any funding sources or conflicts of interest that may affect the authors’ interpretation of the results? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 20. Was ethical approval or consent of participants attained? | Yes | Yes | Yes | Yes | Yes | Yes | ND | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Aggregate risk of bias rating | 16/20 (80%) | 17/20 (85%) | 17/20 (85%) | 16/20 (80%) | 17/20 (85%) | 13/20 (65%) | 12/20 (60%) | 17/20 (85%) | 17/20 (85%) | 13/20 (65%) | 17/20 (85%) | 17/20 (85%) | 17/20 (85%) | 17/20 (85%) |
| Author (Year) | Location | Study Period | Study Design | Population | Sample size | SD | Prev | Self-Medication Agent | Reasons for Self-Medication | Correlates of Self-Medication | Sources of Information |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Zhang 2021 | Australia | March–April 2020 | Online survey | Adults 18+ | 2217 | 49.8% female | 19.5% | Antibiotics | Prevention of COVID-19; self-treatment of COVID-19 | Younger age; higher education; male gender; healthcare worker; poor knowledge about antibiotics; psychological distress due to the pandemic | Not reported |
| Wegbom 2021 | Nigeria | June–July 2020 | Online survey | Adults (age not specified) | 461 | 57.1% female | 41.0% | Vitamin C; multivitamins; antimalarials; amoxicillin; ciprofloxacin; herbal products; erythromycin; metronidazole; hydroxychloroquine and chloroquine | Anxiety about COVID-19; prevention of COVID-19; self-treatment of COVID-19 | Female gender; Higher education; Poor knowledge about self-medication | Medical personnel; friend |
| Quispe-cañari 2020 | Peru | 25 May to 3 June 2020 | Online survey | Adults 18+ | 3792 | 54.5% female | 43.8% | Acetaminophen; azithromycin; ibuprofen; antiretrovirals; hydroxychloroquine; penicillin | Prevention of COVID-19; self-treatment of COVID-19 | Older age; employed; living in the rainforest region | Not reported |
| Sadio 2021 | Togo | 23 April to 8 May 2020 | Survey | Adults 18+; healthcare, air transport, police, road transport, informal sectors | 955 | 28.3% female | 34.2% | Vitamin C; traditional medicines; chloroquine/hydroxychloroquine | Prevention of COVID-19; self-treatment of COVID-19 | Female gender; healthcare worker; higher education | Not reported |
| Elayeh 2021 | Jordan | 26 March to 16 April 2021 | Online survey | Adults | 1179 | 46.4% female | 80.4% | Antibiotics (azithromycin and doxycycline); analgesics and antipyretics (paracetamol, ibuprofen and diclofenac); minerals (zinc, magnesium and iron salts); vitamins (vitamins C, D and B and multivitamins); herbals and supplements (propolis, omega-3 fatty acids and immune-boosting supplements); antithrombotics (aspirin and enoxaparin); cold and cough preparations; antihistamines; antiseptics; lozenges; nasal solutions (normal saline or sea water); clove oil; menthol rub | Prevention of COVID-19; self-treatment of COVID-19 | Female gender; healthcare worker | Newspapers; pharmacist; friends; internet search |
| Shakeel 2021 | India | May 2021 | Online survey | Adults | 920 | 28.6% female | 59.9% | Paracetamol; azithromycin; expectorants; ivermectin; doxycycline; corticosteroids; hydroxychloroquine | Prevention of COVID-19; self-treatment of COVID-19 | Male gender; older age; higher education; government employees | Family; friends; pharmacists/health professionals; newspapers; books/magazines/journals; radio; television; internet |
| Azhar 2021 | Pakistan | 2020 (month unspecified) | Online survey | Adults 16–60 years | 290 | 66.3% female | 59.5% | Herbal medicines, sana makhi; azithromycin; hydroxychloroquine; ivermectin; Disprin; softener; dexamethasone; cough syrup; Panadol; ibuprofen; levofloxacin; cephalosporins; vitamin C; vitamin D | Prevention of COVID-19; self-treatment of COVID-19 | Not reported | Not assessed |
| Annette 2021 | Indonesia | July–December 2020 | Online survey | Adults; mothers 18–49 with school-age children | 610 | 100% female | 75.0% | Antibiotics; antipyretics; cold medications; antihypertension; blood glucose-lowering agents; supplements, antioxidants (vitamins and minerals); herbs or natural products (ginger and honey) | Prevention of COVID-19; self-treatment of COVID-19 | Not reported | Family; friends; social media; news; product brochures |
| de los Ángeles 2020 | Ecuador | 2020 (date unspecified) | In-person and online survey | Adults | 829 | 57.8% female | 96.2% | Eucalyptus; ginger | Prevention of COVID-19; self-treatment of COVID-19 | Not reported | |
| Heshmatifar 2021 | Iran | 2020 (date unspecified) | Online survey | Adults; > 60 years | 342 | 55.5% female | 56.4% | Analgesics; vitamins and supplements; anticold; sedative; antibiotics; gastrointestinal drugs; cardiac drugs | Prevention of COVID-19; self-treatment of COVID-19 | Not reported | Not reported |
| Gaviria-Mendoza 2022 | Columbia | June–September 2020 | Survey | Adults | 397 | 58.20% female | 7.40% | Chloroquine; hydroxychloroquine;ivermectin;azithromycin | To prevent COVID-19 | Distrust in health personnel or institutions;fear of being sanctioned or fined for leaving the home | Social network |
| Okoye et al. 2022 | Nigeria | March–April 2021 | Survey | Adults | 638 | 58.60% female | 36% | Ivermectin;azithromycin;vitamin C;chloroquine;zinc | To prevent COVID-19 and treat symptoms | Older age;married;pharmacist;higher annual income | Not assessed |
| Dehghan 2022 | Iran | April–August | Survey | Adults | 782 | 66.60% female | 84% | Nutritional supplements such as vitamin D, vitamin C, multivitamin, and others, including vitamin B6, vitamin B complex, vitamin E, zinc, calcium, iron, omega-3, and folic acid, or a combination of supplements | To prevent the transmission of COVID-19 or to reduce anxiety caused by the COVID-19 pandemic or both | Female gender; place of residence; COVID-19 Screening | Friends |
| Kristoffersen 2022 | Norway, (n = 990), Sweden, (n = 500), and the Netherlands, (n = 1004) | April–June 2020 | Telephone interview and online survey | Adults | 2494 | 49.7% female | Prevention, 3.4% and treatment, 0.2% | Vitamin C (n = 3); prayer for own health (n = 3); vitamin D (n = 2); omega-3, -6 and -9 fatty acids (n = 2); relaxation exercise (n = 2); unspecified vitamins and minerals (n = 2); ginger (n = 1); garlic (n = 1); ginkgo biloba (n = 1); magnesium (n = 1); zinc (n = 1); breathing exercise (n = 1); unspecified herb (n = 1) | To prevent and treat COVID-19 | Not assessed | Not assessed |
| Drug Class | Names of Specified Medications in the Studies | |||||||
|---|---|---|---|---|---|---|---|---|
| Antibiotics | Azithromycin | Penicillin | Doxycycline | Ciprofloxacin | Erythromycin | Metronidazole | Levofloxacin | Cephalosporins |
| Antimalarials | Chloroquine/hydroxychloroquine | Quinine | Unspecified antimalarials | |||||
| Analgesics and antipyretics | Ibuprofen | Diclofenac | Acetaminophen | Aspirin | ||||
| Minerals supplements | Calcium | Zinc | Magnesium | Aluminium | Omega-3 fatty acids | Immune boosters | ||
| Cold and allergy preparations | Cough syrups | Lozenges | Nasal solutions | Clove oil | Menthol rub | Expectorants | Unspecified cold and allergy preparations | |
| Corticosteroids | Dexamethasone | Unspecified corticosteroids | ||||||
| Antithrombotics | Aspirin | Enoxaparin | ||||||
| Anthelmintics | Ivermectin | |||||||
| Antihistamines | Famotidine | Unspecified antihistamine | ||||||
| Herbs and natural agents | Ginger | Eucalyptus | Unspecified traditional medicine | Unspecified herbal products | Honey | Sana | Makhi | Propolis |
| Vitamins | Vitamin C | Multivitamins | Vitamin C | Vitamin D | ||||
| Antivirals | Antiretrovirals | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayosanmi, O.S.; Alli, B.Y.; Akingbule, O.A.; Alaga, A.H.; Perepelkin, J.; Marjorie, D.; Sansgiry, S.S.; Taylor, J. Prevalence and Correlates of Self-Medication Practices for Prevention and Treatment of COVID-19: A Systematic Review. Antibiotics 2022, 11, 808. https://doi.org/10.3390/antibiotics11060808
Ayosanmi OS, Alli BY, Akingbule OA, Alaga AH, Perepelkin J, Marjorie D, Sansgiry SS, Taylor J. Prevalence and Correlates of Self-Medication Practices for Prevention and Treatment of COVID-19: A Systematic Review. Antibiotics. 2022; 11(6):808. https://doi.org/10.3390/antibiotics11060808
Chicago/Turabian StyleAyosanmi, Oluwasola Stephen, Babatunde Yusuf Alli, Oluwatosin Adetolani Akingbule, Adeyemi Hakeem Alaga, Jason Perepelkin, Delbaere Marjorie, Sujit S. Sansgiry, and Jeffrey Taylor. 2022. "Prevalence and Correlates of Self-Medication Practices for Prevention and Treatment of COVID-19: A Systematic Review" Antibiotics 11, no. 6: 808. https://doi.org/10.3390/antibiotics11060808
APA StyleAyosanmi, O. S., Alli, B. Y., Akingbule, O. A., Alaga, A. H., Perepelkin, J., Marjorie, D., Sansgiry, S. S., & Taylor, J. (2022). Prevalence and Correlates of Self-Medication Practices for Prevention and Treatment of COVID-19: A Systematic Review. Antibiotics, 11(6), 808. https://doi.org/10.3390/antibiotics11060808