
A Retrospective Study on the Effectiveness and Safety of Vancomycin versus Daptomycin in Hemodialysis Patients

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Results
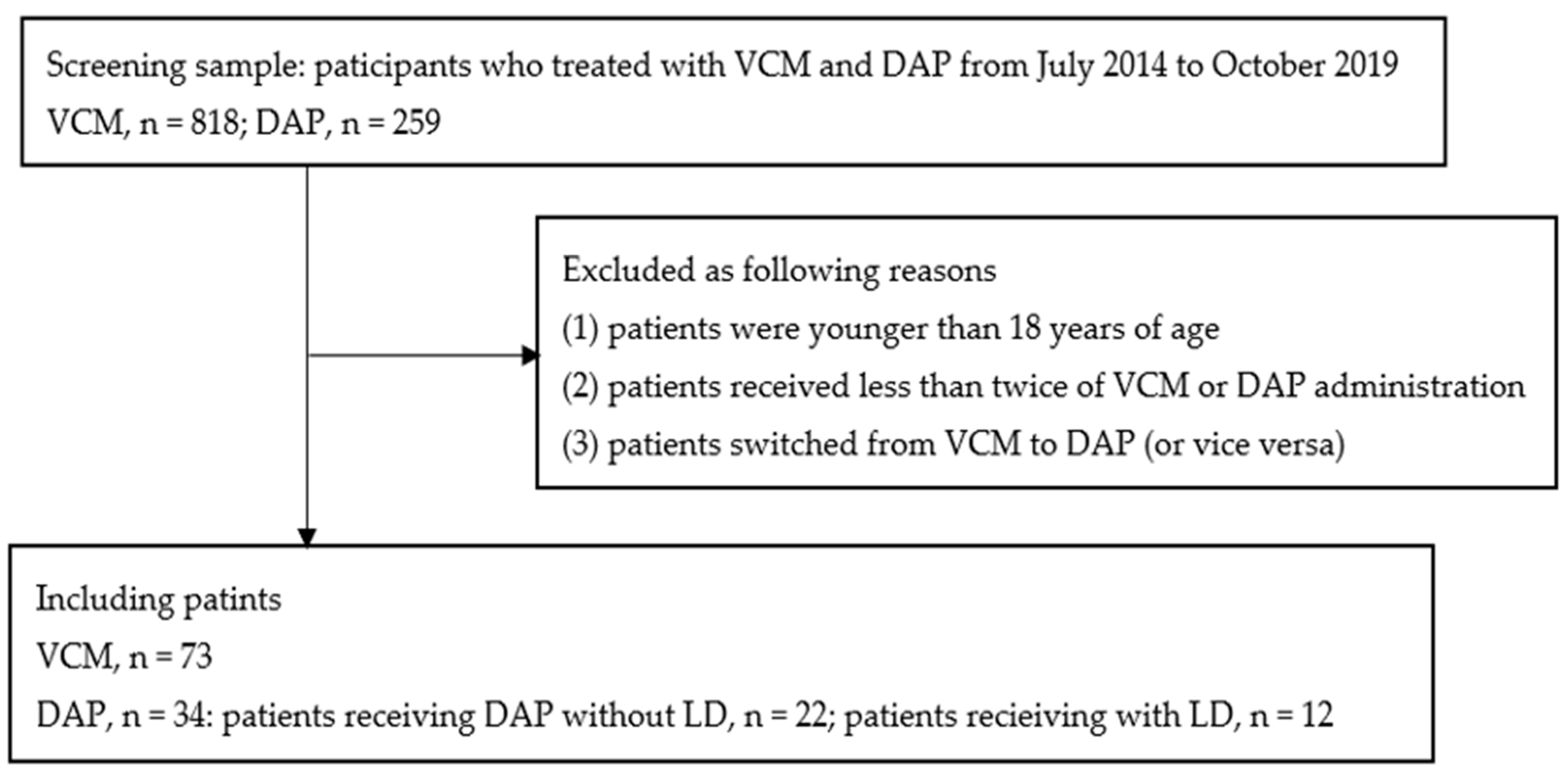
2.1. Patients
2.2. Microbiological Data
2.3. Clinical and Microbiological Effectiveness
2.4. Safety Evaluation
2.5. Comparison between the Survival and Non-Survival Groups
2.6. Clinical Effectiveness and Safety in Hemodialysis Patients Receiving Vancomycin and Daptomycin Treatments with or without a Loading Dose
3. Discussion
4. Patients and Methods
4.1. Patient Population
4.2. Treatment Regimen
4.3. Data Collection
4.4. Clinical and Microbiological Effectiveness
4.5. Safety Evaluation
4.6. Evaluation of Covariate Related to 30-Day Mortality
4.7. Evaluation of a Loading Dose of Daptomycin for Clinical Effectiveness and Safety
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vandecasteele, S.J.; Boelaert, J.R.; De Vriese, A.S. Staphylococcus aureus infections in hemodialysis: What a nephrologist should know. Clin. J. Am. Soc. Nephrol. 2009, 4, 1388–1400. [Google Scholar] [CrossRef]
- Ramanathan, V.; Riosa, S.; Al-Sharif, A.H.; Mansouri, M.D.; Tranchina, A.; Kayyal, T.; Abreo, A.P.; Aslam, S.; Nassar, G.; Darouiche, R.O. Characteristics of biofilm on tunneled cuffed hemodialysis catheters in the presence and absence of clinical infection. Am. J. Kidney Dis. 2012, 60, 976–982. [Google Scholar] [CrossRef]
- Bloembergen, W.E.; Prt, F.K. Epidemiological perspective on infections in chronic dialysis patients. Adv. Ren. Replace Ther. 1996, 3, 201–207. [Google Scholar] [CrossRef]
- Nassar, G.M.; Ayus, J.C. Infectious complications of the hemodialysis access. Kidney Int. 2001, 60, 1–13. [Google Scholar] [CrossRef]
- Iwabuchi, H.; Nakahara, T.; Okamoto, M.; Asano, M.; Oguchi, K.; Kurokawa, K.; Yamanishi, H.; Tateda, K.; Yamaguchi, K. Sepsis in hemodialysis patients. Jpn. Ass. Dial. Phys. 2011, 44, 617–622. [Google Scholar] [CrossRef][Green Version]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef]
- Gaudard, P.; Saour, M.; Morquin, D.; David, H.; Eliet, J.; Villiet, M.; Daures, J.P.; Colson, P. Acute kidney injury during daptomycin versus vancomycin treatment in cardiovascular critically ill patients: A propensity score matched analysis. BMC Infect. Dis. 2019, 19, 438. [Google Scholar] [CrossRef]
- Dvorchik, B.H.; Brazier, D.; DeBruin, M.F.; Arbeit, R.D. Daptomycin pharmacokinetics and safety following administration of escalating doses once daily to healthy subjects. Antimicrob. Agents Chemother. 2003, 47, 1318–1323. [Google Scholar] [CrossRef]
- Arbeit, R.D.; Maki, D.; Tally, F.P.; Camponaro, E.; Eisenstein, B.I.; Daptomycin 98-01 and 99-01 Investigators. The safety and efficacy of daptomycin for the treatment of complicated skin and skin-structure infections. Clin. Infect. Dis. 2004, 38, 1673–1681. [Google Scholar] [CrossRef]
- Maraolo, A.E.; Giaccone, A.; Saracino, A.; Bavaro, D.F. Daptomycin versus vancomycin for the treatment of methicillin-resistant Staphylococcus aureus bloodstream infection with or without endocarditis: A systematic review and meta-analysis. Antibiotics 2021, 10, 1014. [Google Scholar] [CrossRef] [PubMed]
- Hui, K.; Upjohn, M.; Buising, K.; Pedagogos, E.; Nelson, C.; Kirkpatrick, C.M.; Kong, D.C.M. Vancomycin dosing in chronic high-flux haemodialysis: A systematic review. Int. J. Antimicrob. Agents 2018, 51, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, M.; Nakatani, T.; Katori, H.; Hara, S.; Hayashi, M.; Takaichi, K.; Nakata, K.; Kasuya, Y. Vancomycin pharmacokinetics and dosing recommendations in patients undergoing hemodialysis. Jpn. J. Chemother. 2003, 51, 693–702. [Google Scholar]
- Cubicin (Daptomycin for Injection) [Prescribing Information]; Cubist Pharmaceuticals Inc.: Lexington, MA, USA, 2006.
- Fowler, V.G., Jr.; Boucher, H.W.; Corey, G.R.; Abrutyn, E.; Karchmer, A.W.; Rupp, M.E.; Levine, D.P.; Chambers, H.F.; Tally, F.P.; Vigliani, G.A.; et al. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N. Engl. J. Med. 2006, 355, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Kalimuddin, S.; Chan, Y.F.Z.; Philips, R.; Ong, S.P.; Archuleta, S.; Lye, D.C.; Tan, T.T.; Low, J.G.H. A randomized phase 2B trial of vancomycin versus daptomycin for the treatment of methicillin-resistant Staphylococcus aureus bacteremia due to isolates with high vancomycin minimum inhibitory concentrations—Results of a prematurely terminated study. Trials 2018, 19, 305. [Google Scholar] [CrossRef] [PubMed]
- Moise, P.A.; Culshaw, D.L.; Wong-Beringer, A.; Bensman, J.; Lamp, K.C.; Smith, W.J.; Bauer, K.; Goff, D.A.; Adamson, R.; Leuthner, K.; et al. Comparative Effectiveness of Vancomycin versus Daptomycin for MRSA Bacteremia with Vancomycin MIC >1 mg/L: A Multicenter Evaluation. Clin. Ther. 2016, 38, 16–30. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Hagihara, M.; Nishiyama, N.; Koizumi, Y.; Yamagishi, Y.; Matsuura, K.; Mikamo, H. Clinical effectiveness of daptomycin loading dose in patients infected with Gram-positive pathogens. J. Infect. Chmother. 2017, 23, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.J.; Lomaestro, B.M.; Rotschafer, J.C.; Moellering, R.C.; Craig, W.A.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Vancomycin therapeutic guidelines: A summary of consensus recommendations from the infectious diseases Society of America, the American Society of Health-System Pharmacists, and the Society of Infectious Diseases Pharmacists. Clin. Infect. Dis. 2009, 49, 325–327. [Google Scholar] [CrossRef]
- Canut, A.; Isla, A.; Betriu, C.; Gascon, A.R. Pharmacokinetic-pharmacodynamic evaluation of daptomycin, tigecycline, and linezolid versus vancomycin for the treatment of MRSA infections in four western European countries. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 2227–2235. [Google Scholar] [CrossRef]
- Diolez, J.; Venisse, N.; Belmouaz, S.; Bauwens, M.A.; Bridoux, F.; Beraud, G. Pilot Pharmacokinetic Study of High-Dose Daptomycin in Hemodialysis Patients with Infected Medical Devices. Am. J. Kidney Dis. 2017, 70, 732–734. [Google Scholar] [CrossRef]
- Mei, H.; Wang, J.; Che, H.; Wang, R.; Cai, Y. The clinical efficacy and safety of vancomycin loading dose: A systematic review and meta-analysis. Medicine 2019, 98, e17639. [Google Scholar] [CrossRef]
- Kato, H.; Hagihara, M.; Murakami, E.; Suematsu, H.; Nishiyama, N.; Koizumi, Y.; Yamagishi, Y.; Uno, B.; Mikamo, H. Considerations about the use of a loading dose of daptomycin in neutropenic murine thigh model with methicillin-resistant Staphylococcus aureus infection. Chemotherapy 2017, 63, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Hagihara, M.; Shibata, Y.; Asai, N.; Koizumi, Y.; Watarai, M.; Yamagishi, Y.; Mikamo, H. Retrospective study on clinical efficacy and safety for daptomycin intermittent doses with or without loading dose in renal failure patients. J. Infect. Chemother. 2020, 26, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Tai, C.H.; Shao, C.H.; Chen, C.Y.; Lin, S.W.; Wu, C.C. Safety of high-dose daptomycin in patients with severe renal impairment. Ther. Clin. Risk Manag. 2018, 14, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Takesue, Y.; Ohmagari, N.; Mochizuki, T.; Mikamo, H.; Seki, M.; Takakura, S.; Tokimatsu, I.; Takahashi, Y.; Kasahara, K.; et al. Practice guidelines for therapeutic drug monitoring of vancomycin: A consensus review of the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring. J. Infect. Chemother. 2013, 19, 365–380. [Google Scholar] [CrossRef]
- Clinical Laboratory Standards Institute. Clinical Laboratory Standards Institute. In Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard; CLSI Publication M07-A10.10th Edition; Clinical Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]


{kind=link}
| VCM | DAP | p Value | |
|---|---|---|---|
| Gender (male/female) | 64/9 | 23/11 | 0.01 |
| Age (years) | 71 (46–85) | 73 (46–91) | 0.23 |
| Body weight (kg) | 56.7 (32.4–115.5) | 50.7 (35.0–100.0) | 0.29 |
| Duration of therapy (days) | 13 (3–74) | 13 (5–52) | 0.09 |
| Dosage on day 1 (mg/kg) | 18.9 (5.4–30.9) | 6.4 (3.7–14.0) | - |
| Receiving a loading dose (%) | 82.2 (60/72) | 35.3 (12/34) | <0.01 |
| WBC (×103/μL) | 8.2 (2.1–26.6) | 8.2 (1.0–27.8) | 0.44 |
| Eosinophil granulocytes (%) | 2.0 (0.2–15.0) | 2.0 (0.1–21.2) | 0.49 |
| Serum creatinine (mg/dL) | 6.15 (1.70–13.45) | 5.08 (1.34–12.29) | 0.08 |
| eGFR (mL/min/1.73 m2) | 8 (3–30) | 9 (3–37) | 0.06 |
| AST (U/L) | 18 (8–5537) | 21 (7–85) | 0.51 |
| ALT (U/L) | 9 (1–2905) | 10 (3–40) | 0.52 |
| CK (U/L) | 40 (2–2794) | 52 (3–591) | 0.45 |
| CRP (mg/dL) | 7.38 (0.03–33.13) | 7.56 (0.52–34.94) | 0.43 |
| Body temperature (°C) | 37.1 (36.3–40.3) | 37.3 (36.5–40.2) | 0.27 |
| Detected isolates | |||
| MRSA (%) | 60.3 (44/73) | 67.7 (23/34) | 0.46 |
| MRCNS (%) | 31.5 (23/73) | 29.4 (10/34) | 0.83 |
| E. faecium (%) | 8.2 (6/73) | 2.9 (1/34) | 0.30 |
| Resistant pathogen (%) | 1.4 (1/73) | 5.9 (2/34) | 0.19 |
| Comrmodity | |||
| Cancer | 11.0 (8/73) | 14.7 (5/34) | 0.58 |
| Diabates | 31.5 (23/73) | 32.4 (11/34) | 0.85 |
| Types of infection | |||
| Bacteremia (%) | 41.1 (30/73) | 52.9 (18/34) | 0.25 |
| SSTIs (%) | 45.2 (33/73) | 47.1 (16/34) | 0.86 |
| Pneumonia (%) | 9.6 (7/73) | 0 (0/34) | 0.07 |
| UTI (%) | 4.1 (3/73) | 0 (0/34) | 0.23 |
| VCM | DAP | p-Value | |
|---|---|---|---|
| BT of <37.0 °C (%) | 55.9 (38/68) | 44.1 (15/34) | 0.26 |
| CRP of <60% (%) | 55.4 (36/65) | 44.1 (15/34) | 0.29 |
| 14-day mortality (%) | 2.7 (2/73) | 11.8 (4/34) | 0.06 |
| 30-day mortality (%) | 4.1 (3/73) | 26.5 (9/34) | <0.01 |
| Microbiological effectiveness (%) | 78.6 (44/56) | 77.7 (21/37) | 0.94 |
| VCM | DAP | p-Value | |
|---|---|---|---|
| Increased AST level (%) | 9.1 (6/66) | 11.8 (4/34) | 0.67 |
| Increased ALT levels (%) | 9.1 (6/66) | 8.8 (3/34) | 0.97 |
| Increased blood CK level (%) | 2.3 (1/43) | 3.3 (1/30) | 0.80 |
| Increased eosinophil count (%) | 11.4 (4/35) | 11.5 (3/26) | 0.99 |
| Onset of eosinophilic pneumonia (%) | 0 (0/73) | 0 (0/34) | - |
| Rash (%) | 4.1 (3/73) | 2.9 (1/34) | 0.77 |
| Survival | Non-Survival | p-Value a | p-Value b, OR, 95%CI | |
|---|---|---|---|---|
| Receiving a loading dose (%) | 72.6 (69/95) | 25.0 (3/12) | <0.01 | <0.01, 7.96, 2.00–31.72 |
| Receiving a loading dose of daptomycin (%) | 44.0 (11/25) | 11.1 (1/9) | 0.08 | 0.10, 6.29, 0.68–58.11 |
| Receiving a loading dose of vancomycin (%) | 82.9 (58/70) | 66.7 (2/3) | 0.47 | 0.49 |
| Initial VCM trough concentrations (mg/L) | 16.3 ± 4.4 | 15.3 ± 6.6 | 0.69 | 0.69 |
| Microbiological effectiveness (%) | 81.1 (60/74) | 55.6 (5/9) | 0.08 | 0.09, 3.43, 0.81–14.44 |
| Bacteremia (%) | 43.2 (41/95) | 58.3 (7/12) | 0.32 | 0.32 |
| Detected isolates | ||||
| Resistant pathogen (%) | 2.1 (2/95) | 8.3 (1/12) | 0.22 | 0.25 |
| MRSA (%) | 62.1 (59/95) | 66.7 (8/12) | 0.76 | 0.76 |
| MRCNS (%) | 30.5 (29/95) | 33.3 (4/12) | 0.84 | 0.84 |
| E. faecium (%) | 7.4 (7/95) | 0 (0/12) | 0.33 | 0.97 |
| VCM | DAP without LD | DAP with LD | p-Value | |
|---|---|---|---|---|
| BT of <37.0 °C (%) | 55.9 (38/68) | 40.9 (9/22) | 50.0 (6/12) | 0.47 |
| CRP of <60% (%) | 55.4 (36/65) | 40.9 (9/22) | 50.0 (6/12) | 0.50 |
| 14-day mortality (%) | 2.7 (2/73) | 13.6 (3/22) | 8.3 (1/12) | 0.14 |
| 30-day mortality (%) | 4.1 (3/73) | 36.4 (8/22) | 8.3 (1/12) | <0.01 |
| Microbiological effectiveness (%) | 78.6 (44/56) | 76.5 (13/17) | 80.0 (8/10) | 0.97 |
| VCM | DAP without LD | DAP with LD | p-Value | |
|---|---|---|---|---|
| Increased AST level (%) | 9.1 (6/66) | 4.5 (1/22) | 25.0 (3/12) | 0.15 |
| Increased ALT level (%) | 9.1 (6/66) | 4.5 (1/22) | 16.7 (2/12) | 0.50 |
| Increased blood CK levels (%) | 2.3 (1/43) | 0 (0/19) | 9.1 (1/11) | 0.33 |
| Increased eosinophil granulocyte count (%) | 11.4 (4/35) | 12.5 (2/16) | 10.0 (1/10) | 0.98 |
| Onset of eosinophilic pneumonia (%) | 0 (0/73) | 0 (0/22) | 0 (0/12) | - |
| Rash (%) | 4.1 (3/73) | 5.6 (1/22) | 0 (0/12) | 0.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, H.; Hagihara, M.; Kato, M.; Yamagishi, Y.; Umemura, T.; Asai, N.; Hirai, J.; Iwamoto, T.; Mikamo, H. A Retrospective Study on the Effectiveness and Safety of Vancomycin versus Daptomycin in Hemodialysis Patients. Antibiotics 2022, 11, 710. https://doi.org/10.3390/antibiotics11060710
Kato H, Hagihara M, Kato M, Yamagishi Y, Umemura T, Asai N, Hirai J, Iwamoto T, Mikamo H. A Retrospective Study on the Effectiveness and Safety of Vancomycin versus Daptomycin in Hemodialysis Patients. Antibiotics. 2022; 11(6):710. https://doi.org/10.3390/antibiotics11060710
Chicago/Turabian StyleKato, Hideo, Mao Hagihara, Mariko Kato, Yuka Yamagishi, Takumi Umemura, Nobuhiro Asai, Jun Hirai, Takuya Iwamoto, and Hiroshige Mikamo. 2022. "A Retrospective Study on the Effectiveness and Safety of Vancomycin versus Daptomycin in Hemodialysis Patients" Antibiotics 11, no. 6: 710. https://doi.org/10.3390/antibiotics11060710
APA StyleKato, H., Hagihara, M., Kato, M., Yamagishi, Y., Umemura, T., Asai, N., Hirai, J., Iwamoto, T., & Mikamo, H. (2022). A Retrospective Study on the Effectiveness and Safety of Vancomycin versus Daptomycin in Hemodialysis Patients. Antibiotics, 11(6), 710. https://doi.org/10.3390/antibiotics11060710