
Mec-Positive Staphylococcus Healthcare-Associated Infections Presenting High Transmission Risks for Antimicrobial-Resistant Strains in an Equine Hospital


 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Mec-Positive Staphylococcus Strains Were Isolated from the Equine Hospital
2.2. Antimicrobial Resistance Profile of Mec-Positive Staphylococcus
2.3. mecA and mecC Were Found in MRSA and MRCoNS
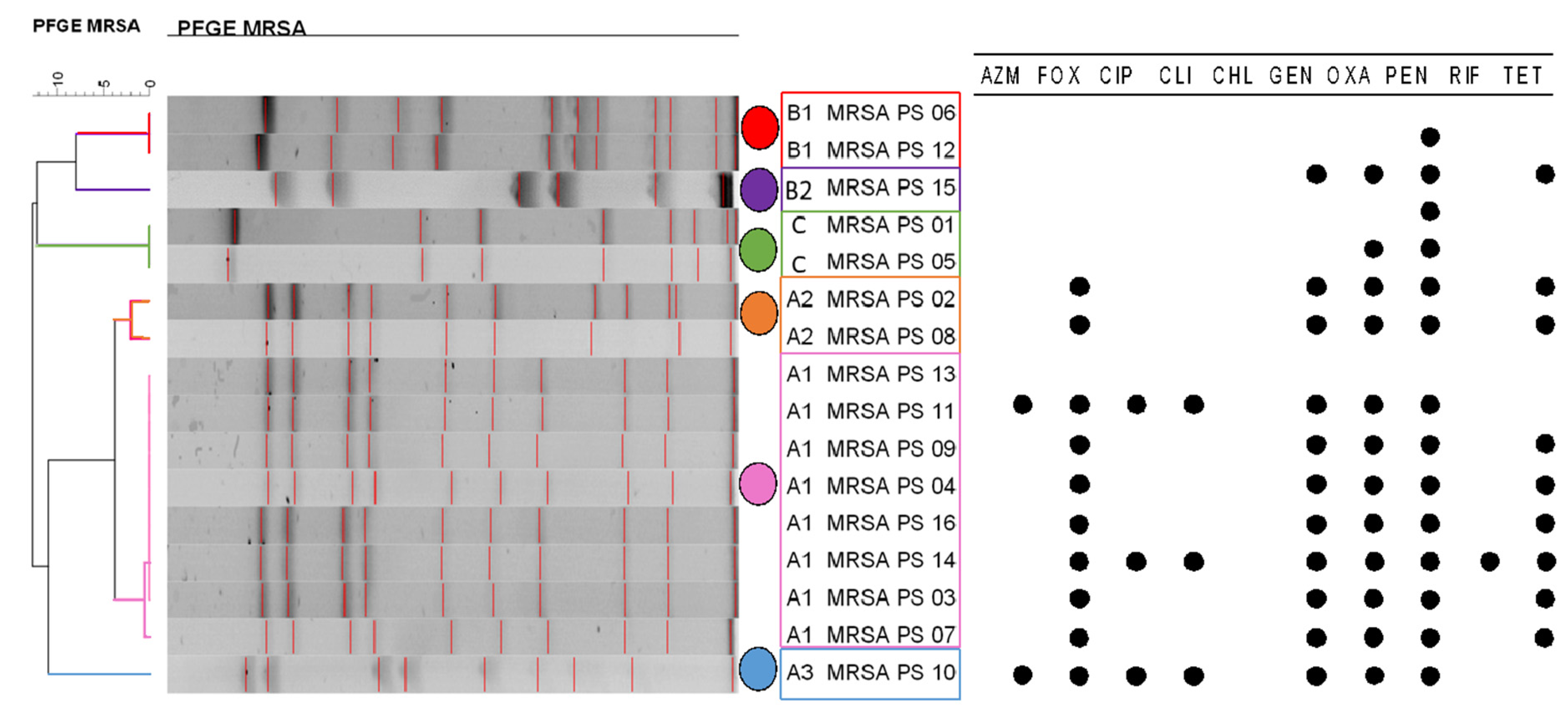
2.4. Diversity of PFGE Profiles in MRSA Strains
2.5. Risk Factors for the Acquisition of Resistance by MRCoNS or either MRSA Strains
3. Discussion
3.1. Hot Spots of Pathogens and Risks for Healthcare-Acquired Infections
3.2. Staphylococcus aureus Isolates Are Phenotypically MDR and Encode mecA and mecC Genes Suggesting an Unusual SCCmec
3.3. One Major Pulse-Type of MRSA Could Be Identified, Which Was Isolated from Different Sources and in Different Sampling Months
4. Materials and Methods
4.1. Study Design
4.2. Sample Procedure
4.3. Staphylococcus spp. Isolation and Identification
4.4. Antimicrobial Susceptibility
4.5. Detection and Confirmation of Methicillin-Resistance, mecA and mecC Genes
4.6. Subtyping by PFGE of Strains of S. aureus
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Milton, A.A.P.; Priya, G.B.; Aravind, M.; Parthasarathy, S.; Saminathan, M.; Jeeva, K.; Agarwal, R.K. Nosocomial Infections and their Surveillance in Veterinary Hospitals. Adv. Anim. Vet. Sci. 2015, 3, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Dalton, K.R.; Rock, C.; Carroll, K.C.; Davis, M.F. One Health in hospitals: How understanding the dynamics of people, animals, and the hospital built-environment can be used to better inform interventions for antimicrobial-resistant gram-positive infections. Antimicrob. Resist. Infect. Control 2020, 9, 78. [Google Scholar] [CrossRef] [PubMed]
- Stull, J.W.; Weese, J.S. Hospital-Associated Infections in Small Animal Practice. Vet. Clin. N. Am. Small Anim. Pract. 2015, 45, 217–233. [Google Scholar] [CrossRef] [PubMed]
- Shahida, S.M.; Islam, A.; Dey, B.R.; Islam, F.; Venkatesh, K.; Goodman, A. Hospital Acquired Infections in Low and Middle Income Countries: Root Cause Analysis and the Development of Infection Control Practices in Bangladesh. Open J. Obstet. Gynecol. 2016, 6, 28–39. [Google Scholar] [CrossRef] [Green Version]
- Vilar-Compte, D.; Camacho-Ortiz, A.; Ponce-de-León, S. Infection Control in Limited Resources Countries: Challenges and Priorities. Curr. Infect. Dis. Rep. 2017, 19, 20. [Google Scholar] [CrossRef] [PubMed]
- Walther, B.; Tedin, K.; Lübke-Becker, A. Multidrug-resistant opportunistic pathogens challenging veterinary infection control. Vet. Microbiol. 2016, 200, 71–78. [Google Scholar] [CrossRef]
- Chirca, I. The hospital environment and its microbial burden: Challenges and solutions. Future Microbiol. 2019, 14, 1007–1010. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, S.; Stevenson, M.A.M.C.; Hudson, C.R.; Maier, M.; Buffington, T.; Dam, Q.; Maurer, J.J. Characterization of multidrug-resistant Escherichia coli isolates associated with nosocomial infections in dogs. J. Clin. Microbiol. 2002, 40, 3586–3595. [Google Scholar] [CrossRef] [Green Version]
- Morley, P.S.; Anderson, M.E.C.; Burgess, B.A.; Aceto, H.; Bender, J.B.; Clark, C.; Daniels, J.B.; Davis, M.A.; Hinchcliff, K.W.; Johnson, J.R.; et al. Report of the third Havemeyer workshop on infection control in equine populations. Equine Vet. J. 2013, 45, 131–136. [Google Scholar] [CrossRef]
- Khan, H.A.; Ahmad, A.; Mehboob, R. Nosocomial infections and their control strategies. Asian Pac. J. Trop. Biomed. 2015, 5, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Baptiste, K.E.; Williams, K.; Willams, N.J.; Wattret, A.; Clegg, P.D.; Dawson, S.; Corkill, J.E.; O’Neill, T.; Anthony Hart, C. Methicillin-resistant staphylococci in companion animals. Emerg. Infect. Dis. 2005, 11, 1942–1944. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.S.; Lee, A.R.; Kang, H.M.; Lee, E.S.; Kim, M.N.; Paik, Y.H.; Park, Y.H.; Joo, Y.S.; Koo, H.C. Phenotypic and genetic antibiogram of methicillin-resistant staphylococci isolated from bovine mastitis in Korea. J. Dairy Sci. 2007, 90, 1176–1185. [Google Scholar] [CrossRef]
- Hanselman, B.A.; Kruth, S.A.; Rousseau, J.; Low, D.E.; Willey, B.M.; McGeer, A.; Weese, J.S. Methicillin-resistant Staphylococcus aureus colonization in veterinary personnel. Emerg. Infect. Dis. 2006, 12, 1933–1938. [Google Scholar] [CrossRef] [PubMed]
- Van Duijkeren, E.; Hengeveld, P.D.; Albers, M.; Pluister, G.; Jacobs, P.; Heres, L.; Van De Giessen, A.W. Prevalence of methicillin-resistant Staphylococcus aureus carrying mecA or mecC in dairy cattle. Vet. Microbiol. 2014, 171, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Moodley, A.; Guardabassi, L. Clonal spread of methicillin-resistant coagulase-negative staphylococci among horses, personnel and environmental sites at equine facilities. Vet. Microbiol. 2009, 137, 397–401. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria : An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2011, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- García-Álvarez, L.; Holden, M.T.; Lindsay, H.; Webb, C.; Brown, D.F. Meticillin-resistant Staphylococcus aureus with a novel mecA homologue in human and bovine populations in the UK and Denmark: A descriptive study. Lancet Infect. Dis. 2011, 11, 595–603. [Google Scholar] [CrossRef] [Green Version]
- Martins, A.; Cunha, M.d.L.R.S. Methicillin resistance in Staphylococcus aureus and coagulase-negative staphylococci: Epidemiological and molecular aspects. Microbiol. Immunol. 2007, 51, 787–795. [Google Scholar] [CrossRef]
- Buzaid, N.; Elzouki, A.N.; Taher, I.; Ghenghesh, K.S. Methicillin-resistant Staphylococcus aureus (MRSA) in a tertiary surgical and Trauma Hospital in Benghazi, Libya. J. Infect. Dev. Ctries. 2011, 5, 723–726. [Google Scholar] [CrossRef]
- Baragundi, M.C.; Solabannavar, S.S.; Gokale, S.K.; Sonth, S.B. Methicillin and multidrug resistant coagulase negative staphylococcal nasal carriage in medical students. J. Commun. Dis. 2012, 44, 231–237. [Google Scholar]
- Yasuda, R.; Kawano, J.; Onda, H.; Takagi, M.; Shimizu, A.; Anzai, T. Methicillin-resistant coagulase-negative staphylococci isolated from healthy horses in Japan. Am. J. Vet. Res. 2000, 61, 1451–1455. [Google Scholar] [CrossRef] [PubMed]
- Bergström, K.; Nyman, G.; Widgren, S.; Johnston, C.; Grönlund-Andersson, U.; Ransjö, U. Infection prevention and control interventions in the first outbreak of methicillin-resistant Staphylococcus aureus infections in an equine hospital in Sweden. Acta Vet. Scand. 2012, 54, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, C. MRSA More Common in Horse People. The Horse 2009, 3–5. [Google Scholar]
- Lowy, F.D. Staphylococcus aureus Infections. N. Engl. J. Med. 1998, 339, 520–532. [Google Scholar] [CrossRef] [PubMed]
- Enright, M.C.; Enright, M.C.; Robinson, D.A.; Robinson, D.A.; Randle, G.; Randle, G.; Feil, E.J.; Feil, E.J.; Grundmann, H.; Grundmann, H.; et al. The evolutionary history of methicillin-resistant Staphylococcus aureus (MRSA). Proc. Natl. Acad. Sci. USA 2002, 99, 7687–7692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deurenberg, R.H.; Vink, C.; Kalenic, S.; Friedrich, A.W.; Bruggeman, C.A.; Stobberingh, E.E. The molecular evolution of methicillin-resistant Staphylococcus aureus. Clin. Microbiol. Infect. 2007, 13, 222–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stegger, M.; Andersen, P.S.; Kearns, A.; Pichon, B.; Holmes, M.A.; Edwards, G.; Laurent, F.; Teale, C.; Skov, R.; Larsen, A.R. Rapid detection, differentiation and typing of methicillin-resistant Staphylococcus aureus harbouring either mecA or the new mecA. Eur. Soc. Clin. Infect. Dis. 2011, 18, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Hoet, A.E.; Johnson, A.; Nava-Hoet, R.C.; Bateman, S.; Hillier, A.; Dyce, J.; Gebreyes, W.A.; Wittum, T.E. Environmental methicillin-resistant Staphylococcus aureus in a veterinary teaching hospital during a nonoutbreak period. Vector Borne Zoonotic Dis. 2011, 11, 609–615. [Google Scholar] [CrossRef] [Green Version]
- Baquero, F. Gram-positive resistance: Challenge for the development of new antibiotics. J. Antimicrob. Chemother. 1997, 39 (Suppl. A), 1–6. [Google Scholar] [CrossRef]
- Stapleton, P.D.; Taylor, P.W. Methicillin reistance in Staphylococcus aureus. Sci. Prog. 2007, 85, 57–72. [Google Scholar] [CrossRef]
- Li, L.; Chen, Z.; Guo, D.; Li, S.; Huang, J.; Wang, X.; Yao, Z.; Chen, S.; Ye, X. Nasal carriage of methicillin-resistant coagulase-negative staphylococci in healthy humans is associated with occupational pig contact in a dose-response manner. Vet. Microbiol. 2017, 208, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.M.; Paterson, G.K.; Holden, M.T.G.; Ba, X.; Rolo, J.; Morgan, F.J.E.; Pichon, B.; Kearns, A.; Zadoks, R.N.; Peacock, S.J.; et al. A novel hybrid SCCmec-mecC region in Staphylococcus sciuri. J. Antimicrob. Chemother. 2014, 69, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Otto, M. Coagulase-negative staphylococci as reservoirs of genes facilitating MRSA infection. BioEssays 2013, 35, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haque, M.; Sartelli, M.; Mckimm, J.; Bakar, M.A. Health care-associated infections–An overview. Infect. Drug Resist. 2018, 11, 2321–2333. [Google Scholar] [CrossRef] [Green Version]
- Cuny, C.; Abdelbary, M.M.H.; Köck, R.; Layer, F.; Scheidemann, W.; Werner, G.; Witte, W. Methicillin-resistant Staphylococcus aureus from infections in horses in Germany are frequent colonizers of veterinarians but rare among MRSA from infections in humans. Elsevier 2016, 2, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Van Balen, J.; Mowery, J.; Piraino-Sandoval, M.; Nava-Hoet, R.C.; Kohn, C.; Hoet, A.E. Molecular epidemiology of environmental MRSA at an equine teaching hospital: Introduction, circulation and maintenance. Vet. Res. 2014, 45, 31. [Google Scholar] [CrossRef] [Green Version]
- Lee Ventola, C. The antibiotic resistance crisis: Part 2: Management strategies and new agents. Pharm. Ther. 2015, 40, 344–352. [Google Scholar]
- Steneroden, K.K.; Van Metre, D.C.; Jackson, C.; Morley, P.S. Detection and control of a nosocomial outbreak caused by Salmonella Newport at a large animal hospital. J. Vet. Intern. Med. 2010, 24, 606–616. [Google Scholar] [CrossRef]
- Soza-Ossandón, P.; Rivera, D.; Tardone, R.; Riquelme-Neira, R.; García, P.; Hamilton-West, C.; Adell, A.D.; González-Rocha, G.; Moreno-Switt, A.I. Widespread Environmental Presence of Multidrug-Resistant Salmonella in an Equine Veterinary Hospital That Received Local and International Horses. Front. Vet. Sci. 2020, 7, 346. [Google Scholar] [CrossRef]
- Apfalter, P.; Assadian, O.; Kalczyk, A.; Lindenmann, V.; Makristathis, A.; Mustafa, S.; Rotter, M.; Hirschl, A.M. Performance of a new chromogenic oxacillin resistance screen medium (Oxoid) in the detection and presumptive identification of methicillin-resistant Staphylococcus aureus. Diagn. Microbiol. Infect. Dis. 2002, 44, 209–211. [Google Scholar] [CrossRef]
- Hudzicki, J.; University of K.M.C. Kirby Bauer Disk Diffusion Susceptibility Test Protocol. Available online: https://www.asmscience.org/content/education/protocol/protocol.3189 (accessed on 25 April 2022).
- US Food and Drug Administration. The National Antimicrobial Resistance Monitoring System Manual of Laboratory Methods; 2020; pp. 1–24. Available online: https://www.fda.gov/media/101423/download (accessed on 25 April 2022).
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 27th ed.; M100; Clinical and Laboratory Standars Institute: Wayne, PA, USA, 2017; ISBN 1562388045. [Google Scholar]
- Altschul, S.F.; Gish, W.; Miller, W.; Myers, E.W.; Lipman, D.J. Basic local alignment search tool. J. Mol. Biol. 1990, 215, 403–410. [Google Scholar] [CrossRef]
- Sievers, F.; Wilm, A.; Dineen, D.; Gibson, T.J.; Karplus, K.; Li, W.; Lopez, R.; Thompson, J.D.; Higgins, D.G.; Mcwilliam, H.; et al. Fast, scalable generation of high-quality protein multiple sequence alignments using Clustal Omega. Mol. Syst. Biol. 2011, 7, 539. [Google Scholar] [CrossRef] [PubMed]
- McDougal, L.K.; Steward, C.D.; Killgore, G.E.; Chaitram, J.M.; McAllister, S.K.; Tenover, F.C. Pulsed-Field Gel Electrophoresis Typing of Oxacillin-Resistant Staphylococcus aureus Isolates from the United States: Establishing a National Database. J. Clin. Microbiol. 2003, 41, 5113–5120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenover, F.C.; Arbeit, R.D.; Goering, R.V.; Mickelsen, P.A.; Murray, B.E.; Persing, D.H.; Swaminathan, B. Interpreting chromosomal DNA restriction patterns produced by pulsed- field gel electrophoresis: Criteria for bacterial strain typing. J. Clin. Microbiol. 1995, 33, 2233–2239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Souece Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperandei, S. Lessons in biostatistics: Understanding logistic regression analysis. Biochem. Med. 2014, 24, 12–18. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Sampling Number | Month/Season | Number of Samples | Number of Samples from Equines (Number of Equines (1)) | Number of Environmental Samples (2) | Nº of MRSA | Nº of MRCoNS | |
|---|---|---|---|---|---|---|---|
| 1 | July | Winter 2015 | 82 | 21 (5) | 61 | 2 | 13 |
| 2 | August | 82 | 21 (5) | 61 | |||
| 3 | September | Spring 2015 | 90 | 29 (7) | 61 | ||
| 4 | October | 75 | 14 (3) | 61 | 6 | 7 | |
| 5 | November | 86 | 25 (6) | 61 | |||
| 6 | December | Summer 2015–2016 | 92 | 31 (7) | 61 | ||
| 7 | January | 99 | 38 (9) | 61 | 3 | 8 | |
| 8 | February | 71 | 10 (2) | 61 | |||
| 9 | March | Autumn 2016 | 81 | 20 (5) | 61 | ||
| 10 | April | 71 | 10 (1) | 61 | 5 | 8 | |
| 11 | May | 78 | 17 (4) | 61 | |||
| 12 | June | Winter 2016 | 71 | 10 (1) | 61 | ||
| Total | 978 | 246 (55) | 732 | 16 | 36 | ||
| Isolation Date | Source (a) | Area (a) | mecA | mecC | PFGE | Antibiotic Resistance Profiles (f) |
|---|---|---|---|---|---|---|
| July-15 | Patient (b) | Surgery | Yes | No | B2 | PEN |
| Augest-15 | Patient (b) | Hospitalization | Yes | Yes | A2 | FOX - GEN - OXA - PEN - TET |
| September-15 | Patient (b) | Surgery | Yes | Yes | A1 | FOX - GEN - OXA - PEN- TET |
| September-15 | Patient (c) | Surgery | Yes | Yes | A1 | FOX - GEN - OXA - PEN - TET |
| October-15 | Environmental | Hospitalization (e) | Yes | No | B2 | PEN-OXA |
| October-15 | Patient (c) | Surgery | Yes | Yes | B1 | Pan-susceptible |
| October-15 | Patient (c) | Surgery | Yes | Yes | A1 | FOX - GEN - OXA - PEN - TET |
| October-15 | Environmental | Surgery (e) | Yes | Yes | A2 | FOX - GEN - OXA - PEN - TET |
| January-16 | Patient (c) | Surgery | Yes | Yes | A1 | FOX - GEN - OXA - PEN - TET |
| February-16 | Environmental | Equipment (e) | Yes | Yes | A3 | AZM - FOX - CIP - CLI - OXA - PEN |
| February-16 | Environmental | Equipment (e) | Yes | Yes | A1 | AZM - FOX - CIP - CLI - GEN - OXA - PEN - TET |
| April-16 | Patient (c) | Hospitalization | Yes | Yes | B1 | FOX - GEN - OXA - PEN - TET |
| May-16 | Environmental | Hospitalization (e) | Yes | No | A1 | Pan-susceptible |
| June-16 | Environmental | Hospitalization (e) | Yes | Yes | A1 | FOX - GEN - OXA - PEN - TET |
| June-16 | Environmental | Proceeding (d) | Yes | Yes | C | FOX - CLI - GEN - OXA - PEN -TET |
| June-16 | Environmental | Equipment (f) | Yes | Yes | A1 | FOX - GEN - OXA - PEN - TET |
| 16/16 (100) | 14/16 (87.5) |
| Isolation Date | Specie (a) | Source (b,c) | Area (d, e) | mecA | mecC | Antibiotic Resistance Profiles (f) |
|---|---|---|---|---|---|---|
| July-15 | S. vitulinus | Patient (b) | Surgery | Yes | Yes | Pan-susceptible |
| July-15 | S. sciuri | Patient (b) | Hospitalization | Yes | Yes | OXA - PEN |
| July-15 | S. sciuri | Patient (b) | Hospitalization | Yes | Yes | AZM - FOX - CIP - OXA - PEN - TET |
| July-15 | S. sciuri | Environmental | Surgery (e) | Yes | Yes | FOX - GEN - OXA - PEN |
| July-15 | S. vitulinus | Environmental | Proceeding (e) | Yes | Yes | CLI - OXA |
| July-15 | S. sciuri | Environmental | Proceeding (e) | Yes | Yes | FOX - GEN - OXA - PEN |
| July-15 | S. vitulinus | Environmental | Surgery (e) | Yes | Yes | OXA |
| July-15 | S. sciuri | Environmental | Surgery (e) | Yes | Yes | FOX - CLI - OXA - PEN |
| July-15 | CoNS | Environmental | Exterior (e) | Yes | No | FOX - CLI - OXA - PEN |
| July-15 | S. sciuri | Patient (b) | Hospitalization | Yes | No | FOX - GEN - OXA - PEN |
| Ago-15 | S. sciuri | Patient (b) | Hospitalization | Yes | No | FOX - CLI - GEN - OXA - PEN |
| Ago-15 | S. lentus | Patient (b) | Surgery | Yes | Yes | FOX - CIP - CLI - CHL - GEN - OXA - PEN - SXT |
| Ago-15 | S. sciuri | Patient (b) | Surgery | Yes | Yes | FOX - GEN - OXA - PEN |
| October-15 | CoNS | Environmental | Proceeding (e) | Yes | Yes | FOX - CLI - OXA - PEN |
| October-15 | CoNS | Patient (b) | Surgery | Yes | Yes | FOX - CIP - CLI - OXA - PEN |
| October-15 | S. sciuri | Environmental | Exterior (e) | No | Yes | FOX - CLI - OXA - PEN |
| October-15 | CoNS | Environmental | Exterior (e) | Yes | Yes | Pan-susceptible |
| October-15 | S. sciuri | Environmental | Equipment (e) | Yes | No | CLI - OXA |
| October-15 | S. vitulinus | Environmental | Equipment (e) | No | Yes | OXA - PEN |
| October-15 | CoNS | Environmental | Hospitalization (d) | Yes | Yes | FOX - GEN - OXA - PEN |
| January-16 | S. sciuri | Patient (b) | Surgery | Yes | Yes | FOX - CLI - GEN - OXA - PEN |
| January-16 | S. sciuri | Patient (b) | Surgery | Yes | Yes | AZM - FOX - CIP - CLI - CHL - GEN - OXA - PEN - RIF - TET |
| January-16 | S. sciuri | Patient (b) | Hospitalization | Yes | Yes | FOX - GEN - OXA - PEN |
| January-16 | CoNS | Environmental | Proceeding (e) | Yes | Yes | OXA |
| January-16 | S. sciuri | Environmental | Exterior (e) | Yes | Yes | FOX - OXA - PEN |
| February-16 | S. sciuri | Environmental | Equipment (e) | Yes | Yes | AZM - FOX - CIP - CLI - OXA - PEN |
| February-16 | S. sciuri | Environmental | Equipment (e) | Yes | Yes | FOX - CHL - OXA - PEN |
| February-16 | CoNS | Environmental | Equipment (e) | Yes | Yes | AZM - FOX - CIP - CLI - GEN - OXA - PEN |
| March-16 | S. sciuri | Environmental | Equipment (e) | Yes | Yes | FOX - CHL - GEN - OXA - PEN |
| March-16 | S. sciuri | Environmental | Surgery (e) | Yes | Yes | AZM - FOX - CIP - CLI - CHL - OXA - PEN - SXT |
| March-16 | S. sciuri | Patient (b) | Surgery | Yes | No | AZM - FOX - CIP - CLI - GEN - OXA - PEN - TET |
| March-16 | CoNS | Patient (b) | Hospitalization | Yes | Yes | RIF - TET |
| May-16 | CoNS | Environmental | Hospitalization (d) | Yes | Yes | Pan-susceptible |
| June-16 | S. sciuri | Environmental | Hospitalization (d) | Yes | Yes | FOX - CLI - OXA - PEN |
| June-16 | CoNS | Environmental | Proceeding (e) | Yes | Yes | FOX - CLI - GEN - OXA -PEN - RIF |
| June-16 | CoNS | Patient (b) | Surgery | Yes | Yes | FOX |
| 34/36 (94%) | 31/36 (86%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soza-Ossandón, P.; Rivera, D.; Allel, K.; González-Rocha, G.; Quezada-Aguiluz, M.; San Martin, I.; García, P.; Moreno-Switt, A.I. Mec-Positive Staphylococcus Healthcare-Associated Infections Presenting High Transmission Risks for Antimicrobial-Resistant Strains in an Equine Hospital. Antibiotics 2022, 11, 621. https://doi.org/10.3390/antibiotics11050621
Soza-Ossandón P, Rivera D, Allel K, González-Rocha G, Quezada-Aguiluz M, San Martin I, García P, Moreno-Switt AI. Mec-Positive Staphylococcus Healthcare-Associated Infections Presenting High Transmission Risks for Antimicrobial-Resistant Strains in an Equine Hospital. Antibiotics. 2022; 11(5):621. https://doi.org/10.3390/antibiotics11050621
Chicago/Turabian StyleSoza-Ossandón, Paula, Dácil Rivera, Kasim Allel, Gerardo González-Rocha, Mario Quezada-Aguiluz, Ivan San Martin, Patricia García, and Andrea I. Moreno-Switt. 2022. "Mec-Positive Staphylococcus Healthcare-Associated Infections Presenting High Transmission Risks for Antimicrobial-Resistant Strains in an Equine Hospital" Antibiotics 11, no. 5: 621. https://doi.org/10.3390/antibiotics11050621
APA StyleSoza-Ossandón, P., Rivera, D., Allel, K., González-Rocha, G., Quezada-Aguiluz, M., San Martin, I., García, P., & Moreno-Switt, A. I. (2022). Mec-Positive Staphylococcus Healthcare-Associated Infections Presenting High Transmission Risks for Antimicrobial-Resistant Strains in an Equine Hospital. Antibiotics, 11(5), 621. https://doi.org/10.3390/antibiotics11050621