
Comparison of Piperacillin and Tazobactam Pharmacokinetics in Critically Ill Patients with Trauma or with Burn


 ,
,
Abstract
1. Introduction
2. Results
2.1. Patient Demographics
2.2. Population Pharmacokinetic Models
- Base Model
- Covariate Model
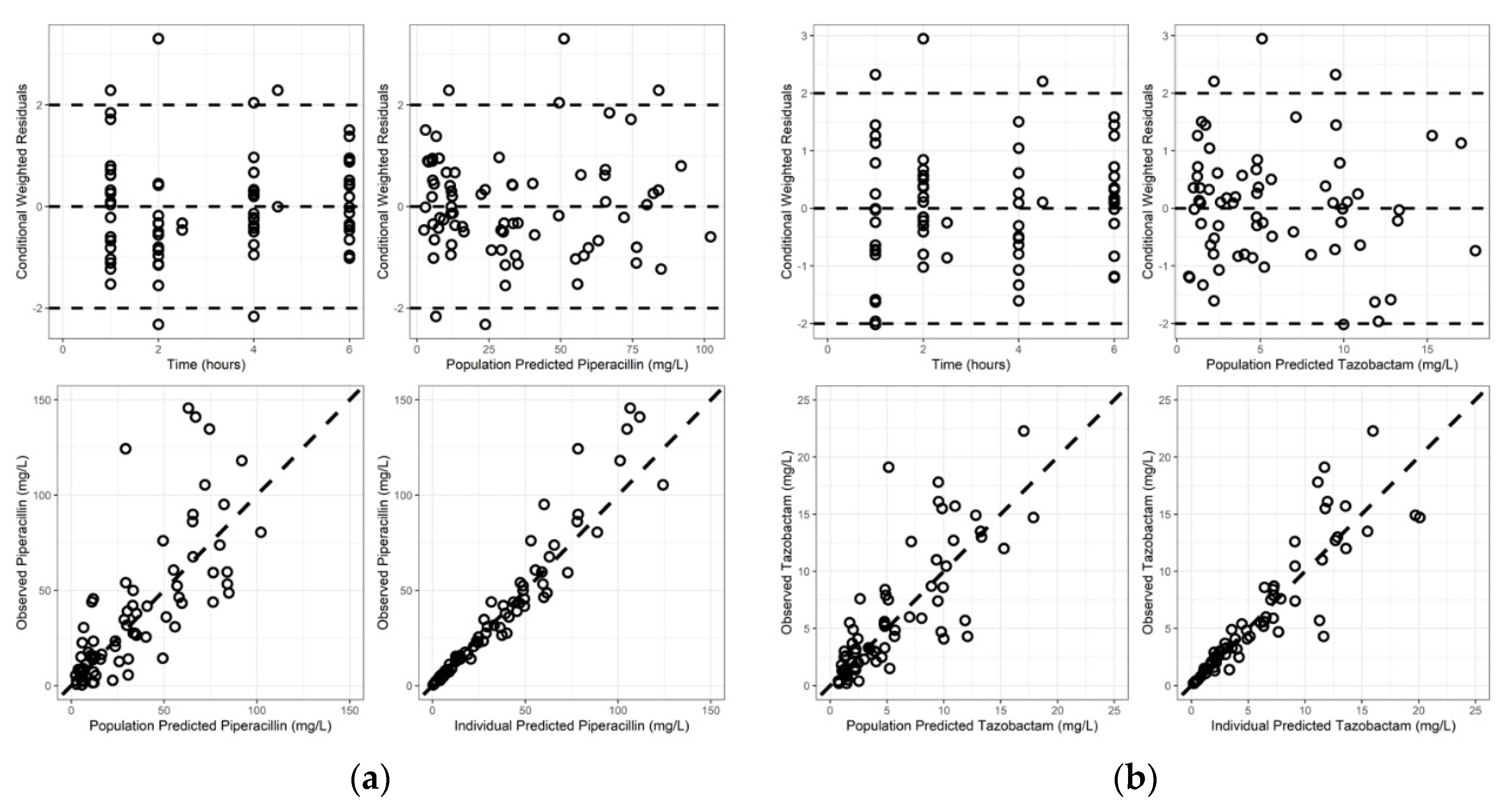
- Validation of Final Model
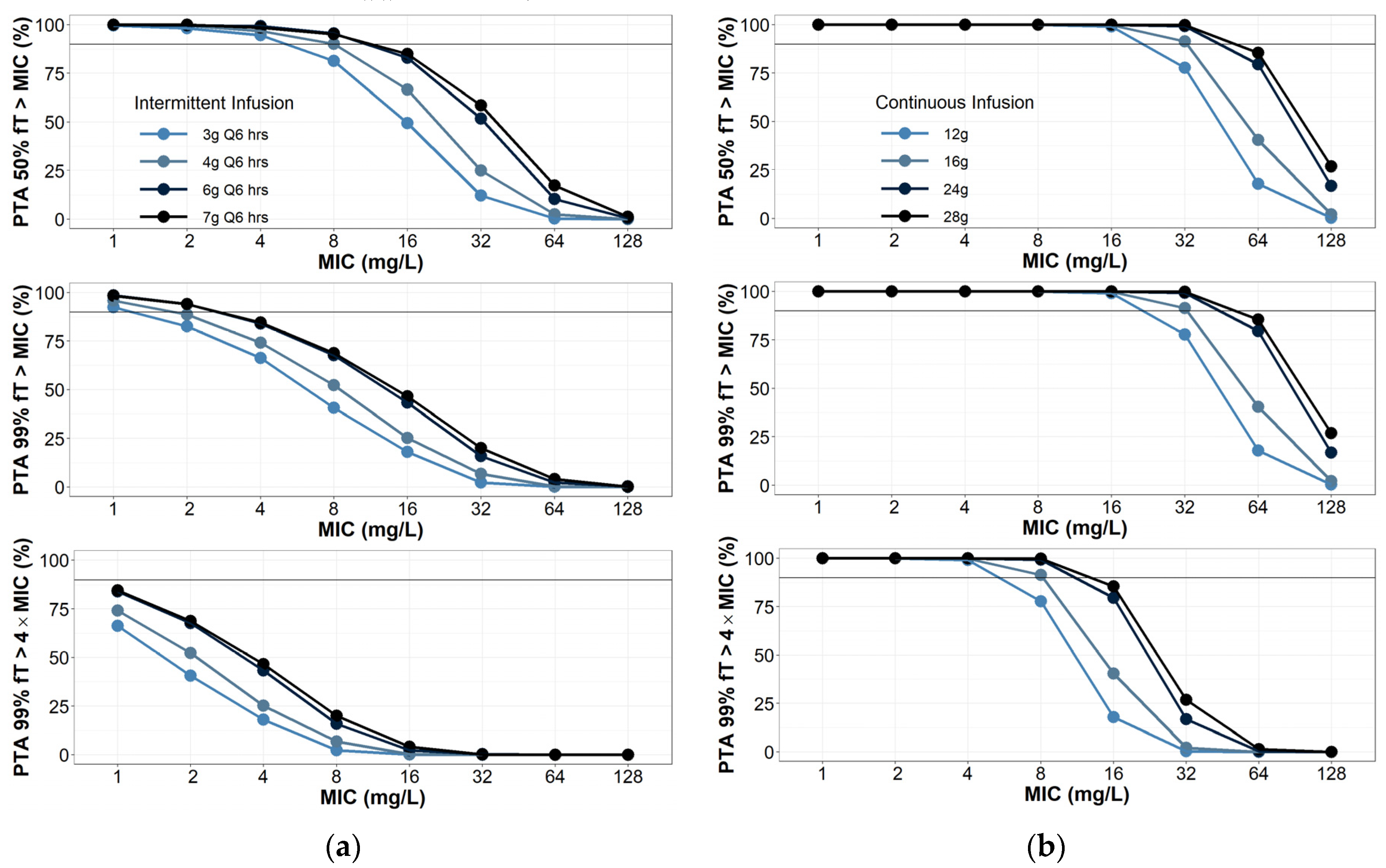
2.3. Probability of Target Attainment
3. Discussion
4. Materials and Methods
4.1. Data
4.2. High-Performance Liquid Chromatography (HPLC)
4.3. Population Pharmacokinetic Modelling and Simulations
- Base Model
- Covariate Model
- Final Model Qualification
- Monte Carlo Simulations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blot, S.I.; Pea, F.; Lipman, J. The effect of pathophysiology on pharmacokinetics in the critically ill patient—Concepts appraised by the example of antimicrobial agents. Adv. Drug Deliv. Rev. 2014, 77, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.M.; Roberts, J.A.; Lipman, J. Antimicrobial pharmacokinetic and pharmacodynamic issues in the critically ill with severe sepsis and septic shock. Crit. Care Clin. 2011, 27, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Bichon, A.; Bourenne, J.; Gainnier, M.; Carvelli, J. Capillary leak syndrome: State of the art in 2021. Rev. de Médecine Interne 2021, 42, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Wollborn, J.; Hassenzahl, L.O.; Reker, D.; Staehle, H.F.; Omlor, A.M.; Baar, W.; Kaufmann, K.B.; Ulbrich, F.; Wunder, C.; Utzolino, S.; et al. Diagnosing capillary leak in critically ill patients: Development of an innovative scoring instrument for non-invasive detection. Ann. Intensive Care 2021, 11, 175. [Google Scholar] [CrossRef]
- Pruskowski, K.A. Pharmacokinetics and Pharmacodynamics of Antimicrobial Agents in Burn Patients. Surg. Infect. 2021, 22, 77–82. [Google Scholar] [CrossRef]
- Luo, Y.; Wang, Y.; Ma, Y.; Wang, P.; Zhong, J.; Chu, Y. Augmented Renal Clearance: What Have We Known and What Will We Do? Front. Pharmacol. 2021, 12, 723731. [Google Scholar] [CrossRef]
- Klastrup, V.; Thorsted, A.; Storgaard, M.; Christensen, S.; Friberg, L.E.; Obrink-Hansen, K. Population Pharmacokinetics of Piperacillin following Continuous Infusion in Critically Ill Patients and Impact of Renal Function on Target Attainment. Antimicrob. Agents Chemother. 2020, 64, e02556-19. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Roberts, J.A.; Carlier, M.; Verstraete, A.G.; Stove, V.; De Waele, J.J. Population pharmacokinetics of continuous infusion of piperacillin in critically ill patients. Int. J. Antimicrob. Agents 2018, 51, 594–600. [Google Scholar] [CrossRef]
- Kalaria, S.N.; Gopalakrishnan, M.; Heil, E.L. A Population Pharmacokinetics and Pharmacodynamic Approach To Optimize Tazobactam Activity in Critically Ill Patients. Antimicrob. Agents Chemother. 2020, 64, e02093-19. [Google Scholar] [CrossRef]
- Alobaid, A.S.; Wallis, S.C.; Jarrett, P.; Starr, T.; Stuart, J.; Lassig-Smith, M.; Mejia, J.L.; Roberts, M.S.; Roger, C.; Udy, A.A.; et al. Population Pharmacokinetics of Piperacillin in Nonobese, Obese, and Morbidly Obese Critically Ill Patients. Antimicrob. Agents Chemother. 2017, 61, e01276-16. [Google Scholar] [CrossRef]
- Jeon, S.; Han, S.; Lee, J.; Hong, T.; Paek, J.; Woo, H.; Yim, D.S. Population pharmacokinetic analysis of piperacillin in burn patients. Antimicrob. Agents Chemother. 2014, 58, 3744–3751. [Google Scholar] [CrossRef] [PubMed]
- Olbrisch, K.; Kisch, T.; Thern, J.; Kramme, E.; Rupp, J.; Graf, T.; Wicha, S.G.; Mailander, P.; Raasch, W. After standard dosage of piperacillin plasma concentrations of drug are subtherapeutic in burn patients. Naunyn Schmiedebergs Arch. Pharmacol. 2019, 392, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Baptista, J.P.; Martins, P.J.; Marques, M.; Pimentel, J.M. Prevalence and Risk Factors for Augmented Renal Clearance in a Population of Critically Ill Patients. J. Intensive Care Med. 2020, 35, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Loirat, P.; Rohan, J.; Baillet, A.; Beaufils, F.; David, R.; Chapman, A. Increased glomerular filtration rate in patients with major burns and its effect on the pharmacokinetics of tobramycin. N. Engl. J. Med. 1978, 299, 915–919. [Google Scholar] [CrossRef]
- Mulder, M.B.; Eidelson, S.A.; Sussman, M.S.; Schulman, C.I.; Lineen, E.B.; Iyenger, R.S.; Namias, N.; Proctor, K.G. Risk Factors and Clinical Outcomes Associated With Augmented Renal Clearance in Trauma Patients. J. Surg. Res. 2019, 244, 477–483. [Google Scholar] [CrossRef]
- Legrand, M.; Payen, D. Understanding urine output in critically ill patients. Ann. Intensive Care 2011, 1, 13. [Google Scholar] [CrossRef]
- Merino-Bohorquez, V.; Docobo-Perez, F.; Valiente-Mendez, A.; Delgado-Valverde, M.; Camean, M.; Hope, W.W.; Pascual, A.; Rodriguez-Bano, J. Population Pharmacokinetics of Piperacillin in Non-Critically Ill Patients with Bacteremia Caused by Enterobacteriaceae. Antibiotics 2021, 10, 348. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Farkas, A.; Colin, P.; Lipman, J.; Stove, V.; Verstraete, A.G.; Roberts, J.A.; De Waele, J.J. Population pharmacokinetics and evaluation of the predictive performance of pharmacokinetic models in critically ill patients receiving continuous infusion meropenem: A comparison of eight pharmacokinetic models. J. Antimicrob. Chemother. 2019, 74, 432–441. [Google Scholar] [CrossRef]
- Udy, A.A.; Roberts, J.A.; Lipman, J.; Blot, S. The effects of major burn related pathophysiological changes on the pharmacokinetics and pharmacodynamics of drug use: An appraisal utilizing antibiotics. Adv. Drug Deliv. Rev. 2018, 123, 65–74. [Google Scholar] [CrossRef]
- Cota, J.M.; FakhriRavari, A.; Rowan, M.P.; Chung, K.K.; Murray, C.K.; Akers, K.S. Intravenous Antibiotic and Antifungal Agent Pharmacokinetic-Pharmacodynamic Dosing in Adults with Severe Burn Injury. Clin. Ther. 2016, 38, 2016–2031. [Google Scholar] [CrossRef]
- Cunio, C.B.; Uster, D.W.; Carland, J.E.; Buscher, H.; Liu, Z.; Brett, J.; Stefani, M.; Jones, G.R.D.; Day, R.O.; Wicha, S.G.; et al. Towards precision dosing of vancomycin in critically ill patients: An evaluation of the predictive performance of pharmacometric models in ICU patients. Clin. Microbiol. Infect. 2020, 27, 783.e7–783.e14. [Google Scholar] [CrossRef] [PubMed]
- Hamada, Y.; Takahashi, S.; Hirayama, T.; Sunakawa, K.; Kuroyama, M. Population pharmacokinetics of tazobactam/piperacillin in Japanese patients with community-acquired pneumonia. Jpn. J. Antibiot. 2013, 66, 189–203. [Google Scholar] [PubMed]
- Landersdorfer, C.B.; Bulitta, J.B.; Kirkpatrick, C.M.; Kinzig, M.; Holzgrabe, U.; Drusano, G.L.; Stephan, U.; Sorgel, F. Population pharmacokinetics of piperacillin at two dose levels: Influence of nonlinear pharmacokinetics on the pharmacodynamic profile. Antimicrob. Agents Chemother. 2012, 56, 5715–5723. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Barreto, E.F.; Webb, A.J.; Pais, G.M.; Rule, A.D.; Jannetto, P.J.; Scheetz, M.H. Setting the Beta-Lactam Therapeutic Range for Critically Ill Patients: Is There a Floor or Even a Ceiling? Crit. Care Explor. 2021, 3, e0446. [Google Scholar] [CrossRef]
- Roger, C.; Louart, B. Beta-Lactams Toxicity in the Intensive Care Unit: An Underestimated Collateral Damage? Microorganisms 2021, 9, 1505. [Google Scholar] [CrossRef]
- Felton, T.W.; Ogungbenro, K.; Boselli, E.; Hope, W.W.; Rodvold, K.A. Comparison of piperacillin exposure in the lungs of critically ill patients and healthy volunteers. J. Antimicrob. Chemother. 2018, 73, 1340–1347. [Google Scholar] [CrossRef]
- Bulitta, J.B.; Kinzig, M.; Jakob, V.; Holzgrabe, U.; Sorgel, F.; Holford, N.H. Nonlinear pharmacokinetics of piperacillin in healthy volunteers--implications for optimal dosage regimens. Br. J. Clin. Pharmacol. 2010, 70, 682–693. [Google Scholar] [CrossRef]
- Bourget, P.; Lesne-Hulin, A.; Le Reveille, R.; Le Bever, H.; Carsin, H. Clinical pharmacokinetics of piperacillin-tazobactam combination in patients with major burns and signs of infection. Antimicrob. Agents Chemother. 1996, 40, 139–145. [Google Scholar] [CrossRef]
- Por, E.D.; Akers, K.S.; Chung, K.K.; Livezey, J.R.; Selig, D.J. Population Pharmacokinetic Modeling and Simulations of Imipenem in Burn Patients With and Without Continuous Venovenous Hemofiltration in the Military Health System. J. Clin. Pharmacol. 2021, 61, 1182–1194. [Google Scholar] [CrossRef]
- Selig, D.J.; Akers, K.S.; Chung, K.K.; Pruskowski, K.A.; Livezey, J.R.; Por, E.D. Meropenem pharmacokinetics in critically ill patients with or without burn treated with or without continuous veno-venous haemofiltration. Br. J. Clin. Pharmacol. 2021, 88, 2156–2168. [Google Scholar] [CrossRef]
- Hallare, J.; Gerriets, V. Half Life; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Lee, C.; Walker, S.A.N.; Walker, S.E.; Seto, W.; Simor, A.; Jeschke, M. A prospective study evaluating tobramycin pharmacokinetics and optimal once daily dosing in burn patients. Burns 2017, 43, 1766–1774. [Google Scholar] [CrossRef] [PubMed]
- Sime, F.B.; Lassig-Smith, M.; Starr, T.; Stuart, J.; Pandey, S.; Parker, S.L.; Wallis, S.C.; Lipman, J.; Roberts, J.A. Population Pharmacokinetics of Unbound Ceftolozane and Tazobactam in Critically Ill Patients without Renal Dysfunction. Antimicrob. Agents Chemother. 2019, 63, e01265-19. [Google Scholar] [CrossRef] [PubMed]
- Tsai, D.; Stewart, P.; Goud, R.; Gourley, S.; Hewagama, S.; Krishnaswamy, S.; Wallis, S.C.; Lipman, J.; Roberts, J.A. Pharmacokinetics of Piperacillin in Critically Ill Australian Indigenous Patients with Severe Sepsis. Antimicrob. Agents Chemother. 2016, 60, 7402–7406. [Google Scholar] [CrossRef] [PubMed]
- Rackauckas, C.; Ma, Y.; Noack, A.; Dixit, V.; Mogensen, P.K.; Bryne, S.; Maddhashiya, S.; Santiago Calderon, J.B.; Nyberg, J.; Gobburu, J.V.S.; et al. Accelerated Predictive Healthcare Analytics with Pumas, a High Performance Pharmaceutical Modeling and Simulation Platform. bioRxiv 2020. [Google Scholar] [CrossRef]
- FDA. Guidance for Industry Pharmacokinetics in Patients with Impaired Renal Function—Study Design, Data Analysis, and Impact on Dosing. 2020. Available online: https://www.fda.gov/media/78573/download (accessed on 27 April 2022).
- Janmahasatian, S.; Duffull, S.B.; Ash, S.; Ward, L.C.; Byrne, N.M.; Green, B. Quantification of lean bodyweight. Clin. Pharmacokinet. 2005, 44, 1051–1065. [Google Scholar] [CrossRef] [PubMed]
- Testing TECoAS. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 11.0. 2021. Available online: http://www.eucast.org (accessed on 27 April 2022).
- Institute CaLS. CLSI Supplement M100. 2021. Available online: http://em100.edaptivedocs.net/GetDoc.aspx?doc=CLSI%20M100%20ED31:2021&scope=user (accessed on 27 April 2022).
- Pfizer. Piperacillin and Tazobactam Package Insert. 1993. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/050684s88s89s90_050750s37s38s39lbl.pdf (accessed on 27 April 2022).




{kind=link}
{kind=link}
{kind=link}
| Category | All (N = 19) 1 | No Burn Trauma (N = 14) | Burn (N = 5) |
|---|---|---|---|
| Age (years) | 38.3 ± 16.34 | 42.86 ± 16.7 | 25.6 ± 4.62 |
| Sex | 16 male, 3 female | 11 male, 3 female | 5 male, 0 female |
| Weight (kg) | 88 ± 26.43 | 82.44 ± 20.66 | 103.56 ± 36.68 |
| Lean Body Mass (kg) | 61.03 ± 13.12 | 58.27 ± 12.05 | 68.76 ± 14.18 |
| Serum Creatinine (mg/dL) | 0.74 ± 0.25 | 0.73 ± 0.29 | 0.77 ± 0.15 |
| Creatinine Clearance (mL/min) | 176.56 ± 63.58 | 164.46 ± 63.46 | 210.41 ± 56.2 |
| Urine Output (mL) | 2802.4 ± 1443.5 | 3035.7 ± 1542.7 | 2149.2 ± 846.1 |
| Blood Urea Nitrogen | 19.07 ± 8.48 | 18 ± 7.6 | 22.04 ± 10.1 |
| Albumin (g/dL) | 2.43 ± 0.63 | 2.58 ± 0.6 | 2.02 ± 0.58 |
| Total Burn Surface Area (%) | – | – | 38.2 ± 28.53 |
| Piperacillin Fraction Unbound | 0.64 ± 0.33 | 0.6 ± 0.33 | 0.75 ± 0.3 |
| Tazobactam Fraction Unbound | 0.51 ± 0.4 | 0.48 ± 0.3 | 0.6 ± 0.61 |
| Parameter | FOCEI Estimate (%RSE) | FOCEI 95% CI | Bootstrap Estimate (95% CI) |
|---|---|---|---|
| CL (L/hr) | 17.56 (9.24) | 14.38–20.73 | 17.56 (13.66–21.61) |
| Vc (L) | 33.59 (16.21) | 22.92–44.27 | 33.59 (23.4–45.02) |
| Q (L/hr) | 6.8 (29.97) | 2.81–10.8 | 6.8 (3.1–11.15) |
| Vp (L) | 10.5 (20.44) | 6.29–14.7 | 10.5 (7.91–23.97) |
| Covariates on CL | |||
| CrCl (power) | 0.65 (20.63) | 0.38–0.91 | 0.65 (0.27–1.11) |
| Random Effects | |||
| ω2 CL | 0.17 (27.35) | 0.08–0.27 | 0.17 (0.068–0.26) |
| ω2 Vc | 0.34 (44.14) | 0.046–0.63 | 0.34 (0.013–0.65) |
| η-shrinkage CL: 1.39%, η-shrinkage Vc: 14.9% Pearson’s correlation coefficients: η-Vc & η-CL: 0.065 | |||
| Residual Unexplained Variability | |||
| Proportional Error | 0.24 (10) | 0.19–0.28 | 0.24 (0.18–0.28) |
| ϵ-shrinkage: 20.27% 19 subjects, 76 total concentration observations, OFV = 552.3, condition number = 83569.8 | |||
| Parameter | FOCEI Estimate (%RSE) | FOCEI 95% CI | Bootstrap Estimate (95% CI) |
|---|---|---|---|
| CL (L/hr) | 11.54 (12.75) | 8.65–14.42 | 11.54 (5.22–14.28) |
| Vc (L) | 20.12 (36.69) | 5.65–34.49 | 20.21 (1.51–31.44) |
| Q (L/hr) | 9.84 (51.93) | 0–19.86 | 9.84 (3.72–15.74) |
| Vp (L) | 15.93 (14.64) | 11.36–20.49 | 15.93 (7.6–23.52) |
| Covariates on CL | |||
| CrCL (power)—fixed | 0.67 | – | 0.67 |
| Random Effects | |||
| ω2 CL | 0.13 (44.03) | 0.02–0.23 | 0.13 (0.037–0.24) |
| η-shrinkage CL: 0.28% | |||
| Residual Unexplained Variability | |||
| Proportional Error | 0.29 (12.18) | 0.21–0.35 | 0.29 (0.21–0.34) |
| ϵ-shrinkage: 10.86% 17 subjects, 66 total concentration observations, OFV = 255.22, condition number = 83,243 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selig, D.J.; Akers, K.S.; Chung, K.K.; Kress, A.T.; Livezey, J.R.; Por, E.D.; Pruskowski, K.A.; DeLuca, J.P. Comparison of Piperacillin and Tazobactam Pharmacokinetics in Critically Ill Patients with Trauma or with Burn. Antibiotics 2022, 11, 618. https://doi.org/10.3390/antibiotics11050618
Selig DJ, Akers KS, Chung KK, Kress AT, Livezey JR, Por ED, Pruskowski KA, DeLuca JP. Comparison of Piperacillin and Tazobactam Pharmacokinetics in Critically Ill Patients with Trauma or with Burn. Antibiotics. 2022; 11(5):618. https://doi.org/10.3390/antibiotics11050618
Chicago/Turabian StyleSelig, Daniel J., Kevin S. Akers, Kevin K. Chung, Adrian T. Kress, Jeffrey R. Livezey, Elaine D. Por, Kaitlin A. Pruskowski, and Jesse P. DeLuca. 2022. "Comparison of Piperacillin and Tazobactam Pharmacokinetics in Critically Ill Patients with Trauma or with Burn" Antibiotics 11, no. 5: 618. https://doi.org/10.3390/antibiotics11050618
APA StyleSelig, D. J., Akers, K. S., Chung, K. K., Kress, A. T., Livezey, J. R., Por, E. D., Pruskowski, K. A., & DeLuca, J. P. (2022). Comparison of Piperacillin and Tazobactam Pharmacokinetics in Critically Ill Patients with Trauma or with Burn. Antibiotics, 11(5), 618. https://doi.org/10.3390/antibiotics11050618