
Impact of Guideline Adherence on Outcomes in Patients Hospitalized with Community-Acquired Pneumonia (CAP) in Hungary: A Retrospective Observational Study


 ,
,
Abstract
1. Introduction
2. Results
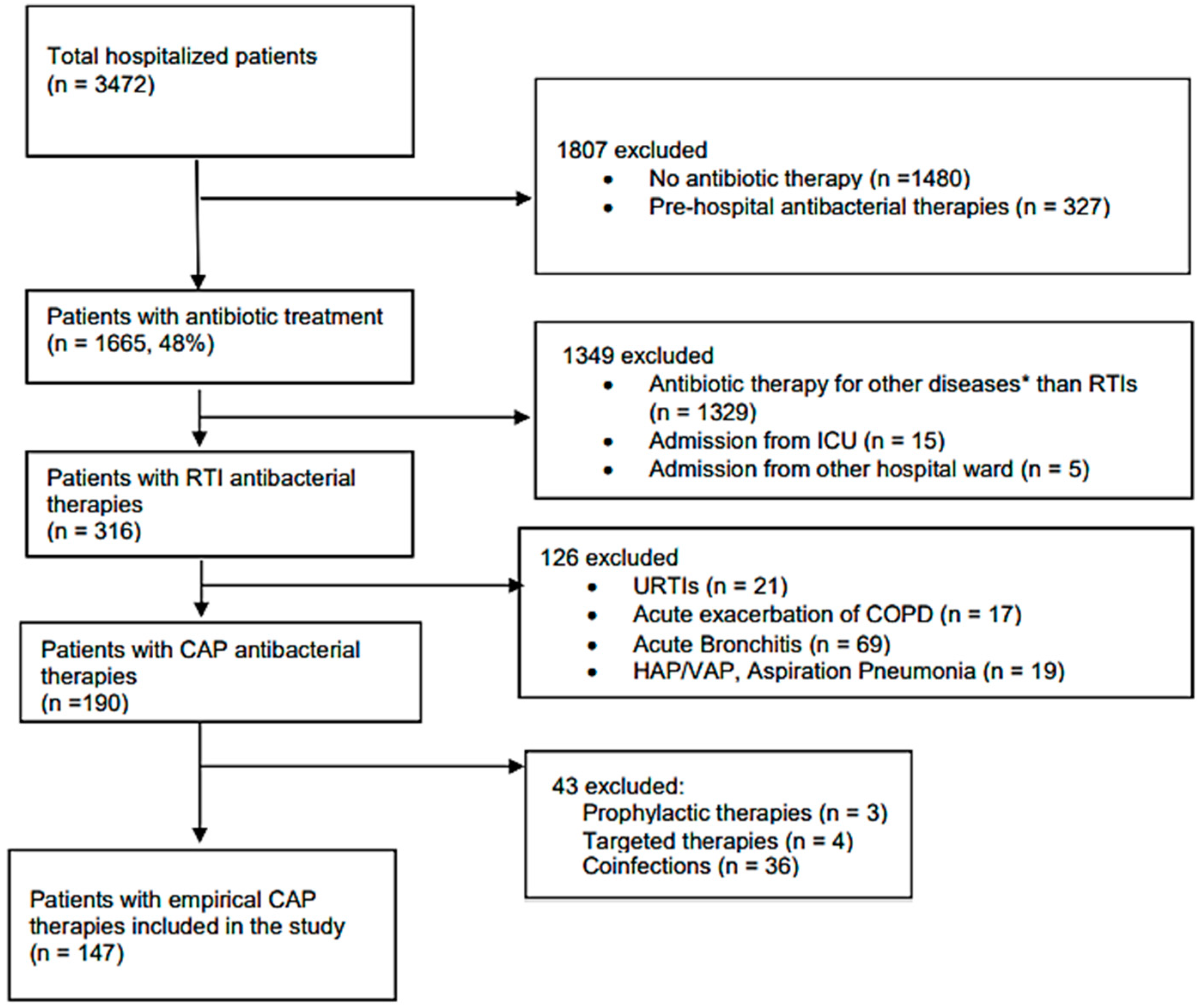
2.1. Patient Characteristics and Main Outcomes
2.2. Guideline Adherence
2.3. Antibiotic Therapy for CAP
2.4. Clinical Outcomes: LOS, 30-Day Mortality
2.5. Prognostic Factors for Mortality in CAP
3. Discussion
3.1. CAP Guidelines
3.1.1. Guideline Adherence: Agent Selection
3.1.2. Guideline Adherence: Dosing
3.2. Changes in the First Empirical Therapy
3.3. Duration of Antibiotic Therapy
3.4. Clinical Outcomes: 30-Day Mortality
3.5. Prognostic Factors for Mortality Due to CAP
3.6. Strengths and Limitations
4. Materials and Methods
4.1. Study Design and Setting
4.2. Data Collection
4.3. Main Outcome Measures
- -
- appropriate dose: dose recommended by guidelines, administration of loading dose when recommended, and dose adjustment in renal impairment.
- -
- debatable dose: under- or overdose by <50% compared to the dose recommended by guidelines, and/or absence of loading dose.
- -
- under-or overdose: under- or overdose by ≥50% compared to the dose recommended by guidelines, and/or no dose adjustment in renal impairment and in extremes for body weight.
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Agent | Appropriate (Recommended) Dose | Recommended Dose Adjustment by SPC | Debatable Dose | Underdose/ Overdose | |||
|---|---|---|---|---|---|---|---|
| National CAP Guideline 1 | BTS/NICE CAP Guideline 2 | ATS/IDSA CAP Guideline 2 | eGFR (mL/min) | Body Weight (kg) | |||
| amoxicillin | 500 mg orally q8hr or 1g iv3 q8hr | ˂10 | ˂50 kg | <50% deviation from the recommended dose and/or absence of loading dose | ≥50% deviation from the recommended dose and/or no dose adjustment in renal impairment and in extremes 4 for body weight | ||
| amoxicillin-clavulanic acid | 500/125 mg or 1/0.25 g q8hr 60/15 mg/kg of body weight/day | 500/125mg orally q8hr or 1/0.25g iv 3 q8hr | ˂10 | ˂50 kg | |||
| clarithromycin | 500 mg q12hr | 500 mg orally or iv 3 q12hr | 500 mg orally or iv3 q12hr | ˂30 | - | ||
| ceftriaxone | 1–2 g iv daily 50–80 mg/kg of body weight | 1–2 g iv daily | ˂30 | ˂40 kg | |||
| moxifloxacin | 400 mg daily | 400 mg orally or iv 3 daily | ˂30 | - | |||
| levofloxacin | 500 mg or 1 g daily | 500 mg orally or iv 3 q12hr | 750 mg orally or iv3 daily | ≤50 | - | ||
| doxycycline | 200 mg on first day, then 100 mg daily orally | ˂50 kg | |||||
References
- Rossolini, G.M.; Mantengoli, E. Antimicrobial resistance in Europe and its potential impact on empirical therapy. Clin. Microbiol. Infect. 2008, 14 (Suppl. 6), 2–8. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, D.; Veeraraghavan, B.; Elangovan, R.; Vivekanandan, P. Antibiotic Resistance and Epigenetics: More to It than Meets the Eye. Antimicrob. Agents Chemother. 2020, 64, e02225-19. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Use in European Hospitals. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-use-european-hospitals (accessed on 19 November 2021).
- Indication for Antimicrobial Use. Available online: https://www.ecdc.europa.eu/en/healthcare-associated-infections-acute-care-hospitals/database/indications-antimicrobial-use/use (accessed on 12 January 2022).
- Diagnosis Site of Antimicrobial Treatment. Available online: https://www.ecdc.europa.eu/en/healthcare-associated-infections-acute-care-hospitals/database/indications-antimicrobial-use/diagnosis-site (accessed on 12 January 2022).
- Respiratory Diseases Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Respiratory_diseases_statistics&oldid=497079#Deaths_from_diseases_of_the_respiratory_system (accessed on 21 January 2022).
- Brown, J.S. Community-acquired pneumonia. Clin. Med. 2012, 12, 538–543. [Google Scholar] [CrossRef]
- Rider, A.C.; Frazee, B.W. Community-Acquired Pneumonia. Emerg. Med. Clin. N. Am. 2018, 36, 665–683. [Google Scholar] [CrossRef]
- Kaysin, A.; Viera, A.J. Community-Acquired Pneumonia in Adults: Diagnosis and Management. Am. Fam. Physician 2016, 94, 698–706. [Google Scholar] [PubMed]
- OECD; European Union. Mortality from Respiratory Diseases, in Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: France, Paris; European Union: Brussels, Belgium, 2018; Available online: https://www.oecd-ilibrary.org/docserver/health_glance_eur-2018-12-en.pdf?expires=1642068861&id=id&accname=guest&checksum=486138DF9F452206CD45EE442FA8CAF1 (accessed on 12 January 2022).
- Kosar, F.; Alici, D.E.; Hacibedel, B.; Arpinar Yigitbas, B.; Golabi, P.; Cuhadaroglu, C. Burden of community-acquired pneumonia in adults over 18 y of age. Hum. Vaccin Immunother. 2017, 13, 1673–1680. [Google Scholar] [CrossRef]
- Sweeney, J. Panel Finds Widespread Inappropriate Use of Antibiotics in U.S. Hospitals. Pharm. Today 2021, 27, 52. [Google Scholar] [CrossRef]
- Arnold, F.W.; LaJoie, A.S.; Brock, G.N.; Peyrani, P.; Rello, J.; Menendez, R.; Lopardo, G.; Torres, A.; Rossi, P.; Ramirez, J.A.; et al. Improving outcomes in elderly patients with community-acquired pneumonia by adhering to national guidelines: Community-Acquired Pneumonia Organization International cohort study results. Arch. Intern. Med. 2009, 169, 1515–1524. [Google Scholar] [CrossRef]
- Dambrava, P.G.; Torres, A.; Valles, X.; Mensa, J.; Marcos, M.A.; Penarroja, G.; Camps, M.; Estruch, R.; Sanchez, M.; Menendez, R.; et al. Adherence to guidelines’ empirical antibiotic recommendations and community-acquired pneumonia outcome. Eur. Respir. J. 2008, 32, 892–901. [Google Scholar] [CrossRef]
- Wathne, J.S.; Harthug, S.; Kleppe, L.K.S.; Blix, H.S.; Nilsen, R.M.; Charani, E.; Smith, I. The association between adherence to national antibiotic guidelines and mortality, readmission and length of stay in hospital inpatients: Results from a Norwegian multicentre, observational cohort study. Antimicrob. Resist. Infect. Control. 2019, 8, 63. [Google Scholar] [CrossRef]
- McCabe, C.; Kirchner, C.; Zhang, H.; Daley, J.; Fisman, D.N. Guideline-concordant therapy and reduced mortality and length of stay in adults with community-acquired pneumonia: Playing by the rules. Arch. Intern. Med. 2009, 169, 1525–1531. [Google Scholar] [CrossRef] [PubMed]
- Frei, C.R.; Restrepo, M.I.; Mortensen, E.M.; Burgess, D.S. Impact of guideline-concordant empiric antibiotic therapy in community-acquired pneumonia. Am. J. Med. 2006, 119, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Matuz, M.; Bognar, J.; Hajdu, E.; Doro, P.; Bor, A.; Viola, R.; Soos, G.; Benko, R. Treatment of Community-Acquired Pneumonia in Adults: Analysis of the National Dispensing Database. Basic Clin. Pharmacol. Toxicol. 2015, 117, 330–334. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jackson, C.D.; Burroughs-Ray, D.C.; Summers, N.A. Clinical Guideline Highlights for the Hospitalist: 2019 American Thoracic Society/Infectious Diseases Society of America Update on Community-Acquired Pneumonia. J. Hosp. Med. 2020, 15, 743–745. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.S.; Smith, D.L.; Wise, M.P.; Welham, S.A. British Thoracic Society community acquired pneumonia guideline and the NICE pneumonia guideline: How they fit together. BMJ Open Respir. Res. 2015, 2, e000091. [Google Scholar] [CrossRef]
- Ministry of Health, National Guideline for Antimicrobial Treatment of Community Acquired Pneumonia in Adults with Healthy Immunity, Proffesional Society of Incetious Diseases and Pulmonology. Available online: http://www.tudogyogyasz.hu/upload/tudogyogyasz/document/infektologia_pneumoniak_antimikrobas_kezelese.pdf (accessed on 1 February 2022).
- National Bacteriological Surveillance Management Team. NBS Annual Reports. National Center for Epidemiology. Available online: www.oek.hu (accessed on 11 December 2021).
- Silveira, C.D.; Ferreira, C.S.; Correa Rde, A. Adherence to guidelines and its impact on outcomes in patients hospitalized with community-acquired pneumonia at a university hospital. J. Bras. Pneumol. 2012, 38, 148–157. [Google Scholar] [CrossRef]
- Blasi, F.; Iori, I.; Bulfoni, A.; Corrao, S.; Costantino, S.; Legnani, D. Can CAP guideline adherence improve patient outcome in internal medicine departments? Eur. Respir. J. 2008, 32, 902–910. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef]
- Uranga, A.; Espana, P.P.; Bilbao, A.; Quintana, J.M.; Arriaga, I.; Intxausti, M.; Lobo, J.L.; Tomas, L.; Camino, J.; Nunez, J.; et al. Duration of Antibiotic Treatment in Community-Acquired Pneumonia: A Multicenter Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 1257–1265. [Google Scholar] [CrossRef]
- Robert, L.; Mark, V.; Moayed, A.; Nivashen, A.; Vinod, R.; Sophie, P.; Mohamed, E.W.; Rusheng, C. Antimicrobial prescribing and outcomes of community-acquired pneumonia in Australian hospitalized patients: A cross-sectional study. J. Int. Med. Res. 2021, 49, 3000605211058366. [Google Scholar] [CrossRef]
- van Heijl, I.; Schweitzer, V.A.; Boel, C.H.E.; Oosterheert, J.J.; Huijts, S.M.; Dorigo-Zetsma, W.; van der Linden, P.D.; Bonten, M.J.M.; van Werkhoven, C.H. Confounding by indication of the safety of de-escalation in community-acquired pneumonia: A simulation study embedded in a prospective cohort. PLoS ONE 2019, 14, e0218062. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.; Blasi, F.; Zanaboni, A.M.; Peyrani, P.; Tarsia, P.; Gaito, S.; Ramirez, J.A. Duration of antibiotic therapy in hospitalised patients with community-acquired pneumonia. Eur. Respir. J. 2010, 36, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, D.J.; McIntosh, K.A.; Pulver, L.K.; Easton, K.L. Empiric management of community-acquired pneumonia in Australian emergency departments. Med. J. Aust. 2005, 183, 520–524. [Google Scholar] [CrossRef]
- Cilli, A.; Sayiner, A.; Celenk, B.; Sakar Coskun, A.; Kilinc, O.; Hazar, A.; Aktas Samur, A.; Tasbakan, S.; Waterer, G.W.; Havlucu, Y.; et al. Antibiotic treatment outcomes in community-acquired pneumonia. Turk. J. Med. Sci. 2018, 48, 730–736. [Google Scholar] [CrossRef]
- Cowling, T.; Farrah, K. Fluoroquinolones for the Treatment of Respiratory Tract Infections: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2019.
- Liu, S.; Tong, X.; Ma, Y.; Wang, D.; Huang, J.; Zhang, L.; Wu, M.; Wang, L.; Liu, T.; Fan, H. Respiratory Fluoroquinolones Monotherapy vs. beta-Lactams With or Without Macrolides for Hospitalized Community-Acquired Pneumonia Patients: A Meta-Analysis. Front. Pharmacol. 2019, 10, 489. [Google Scholar] [CrossRef]
- Dimopoulos, G.; Matthaiou, D.K.; Karageorgopoulos, D.E.; Grammatikos, A.P.; Athanassa, Z.; Falagas, M.E. Short- versus long-course antibacterial therapy for community-acquired pneumonia: A meta-analysis. Drugs 2008, 68, 1841–1854. [Google Scholar] [CrossRef]
- Zhang, Z.X.; Yong, Y.; Tan, W.C.; Shen, L.; Ng, H.S.; Fong, K.Y. Prognostic factors for mortality due to pneumonia among adults from different age groups in Singapore and mortality predictions based on PSI and CURB-65. Singap. Med. J. 2018, 59, 190–198. [Google Scholar] [CrossRef]
- Conte, H.A.; Chen, Y.T.; Mehal, W.; Scinto, J.D.; Quagliarello, V.J. A prognostic rule for elderly patients admitted with community-acquired pneumonia. Am. J. Med. 1999, 106, 20–28. [Google Scholar] [CrossRef]
- Torres, A.; Peetermans, W.E.; Viegi, G.; Blasi, F. Risk factors for community-acquired pneumonia in adults in Europe: A literature review. Thorax 2013, 68, 1057–1065. [Google Scholar] [CrossRef]
- Torner, N.; Izquierdo, C.; Soldevila, N.; Toledo, D.; Chamorro, J.; Espejo, E.; Fernandez-Sierra, A.; Dominguez, A.; Project, P.I.W.G. Factors associated with 30-day mortality in elderly inpatients with community acquired pneumonia during 2 influenza seasons. Hum. Vaccin Immunother. 2017, 13, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Luna, C.M.; Palma, I.; Niederman, M.S.; Membriani, E.; Giovini, V.; Wiemken, T.L.; Peyrani, P.; Ramirez, J. The Impact of Age and Comorbidities on the Mortality of Patients of Different Age Groups Admitted with Community-acquired Pneumonia. Ann. Am. Thorac. Soc. 2016, 13, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Marshall, D.C.; Goodson, R.J.; Xu, Y.; Komorowski, M.; Shalhoub, J.; Maruthappu, M.; Salciccioli, J.D. Trends in mortality from pneumonia in the Europe union: A temporal analysis of the European detailed mortality database between 2001 and 2014. Respir. Res. 2018, 19, 81. [Google Scholar] [CrossRef] [PubMed]
- Summah, H.; Qu, J.M. Biomarkers: A definite plus in pneumonia. Mediat. Inflamm. 2009, 2009, 675753. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.L.; Liu, C.H.; Xu, J.; Cui, Z.Y.; Guo, W.C.; Li, H.L.; Fu, A.S.; Wang, H.Y.; Zhang, H.F.; Zhu, X.Y. Serum High-Sensitivity C Reactive Protein Improves Sensitivity of CURB-65 in Predicting ICU Admission and Mortality in Community-Acquired Pneumonia Patients. Clin. Lab. 2018, 64, 1749–1754. [Google Scholar] [CrossRef]
- Almirall, J.; Bolibar, I.; Toran, P.; Pera, G.; Boquet, X.; Balanzo, X.; Sauca, G. Contribution of C-reactive protein to the diagnosis and assessment of severity of community-acquired pneumonia. Chest 2004, 125, 1335–1342. [Google Scholar] [CrossRef]
- Menendez, R.; Martinez, R.; Reyes, S.; Mensa, J.; Polverino, E.; Filella, X.; Esquinas, C.; Martinez, A.; Ramirez, P.; Torres, A. Stability in community-acquired pneumonia: One step forward with markers? Thorax 2009, 64, 987–992. [Google Scholar] [CrossRef]
- Colak, A.; Yilmaz, C.; Toprak, B.; Aktogu, S. Procalcitonin and CRP as Biomarkers in Discrimination of Community-acquired Pneumonia and Exacerbation of COPD. J. Med. Biochem. 2017, 36, 122–126. [Google Scholar] [CrossRef]
- Smith, R.P.; Lipworth, B.J. C-reactive protein in simple community-acquired pneumonia. Chest 1995, 107, 1028–1031. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Singanayagam, A.; Hill, A.T. C-reactive protein is an independent predictor of severity in community-acquired pneumonia. Am. J. Med. 2008, 121, 219–225. [Google Scholar] [CrossRef]
- Andersen, S.; Baunbæk-Knudsen, G.L.; Jensen, A.V.; Petersen, P.T.; Ravn, P. The prognostic value of consecutive C-reactive protein measurements in community acquired pneumonia. Eur. Respir. J. 2015, 46, 2577. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- WHO Collaborating Centre for Drug Statistics Methodology, Definition and General Considerations. Available online: https://www.whocc.no/ddd/definition_and_general_considera/ (accessed on 27 January 2022).

| Parameter | N | % |
|---|---|---|
| 147 | 100 | |
| Gender (Male) | 64 | 43.54 |
| Age | ||
| 20–64 years | 29 | 19.73 |
| 65–84 years | 72 | 48.98 |
| ≥85 years | 46 | 31.29 |
| Penicillin allergy | 2 | 1.36 |
| CCI—Charlson comorbidity index | ||
| 0 | 3 | 2.04 |
| 1 | 2 | 1.36 |
| 2 | 10 | 6.80 |
| 3 | 12 | 8.16 |
| 4 | 32 | 21.77 |
| >4 | 88 | 59.86 |
| Comorbidities | ||
| Cardiovascular disease | 52 | 35.37 |
| Diabetes mellitus | 33 | 22.45 |
| Chronic obstructive pulmonary disease | 13 | 8.84 |
| Chronic liver/kidney disease (moderate to severe) | 11 | 7.48 |
| Hematologic malignant diseases | 8 | 5.44 |
| Solid tumor | ||
| Localized | 2 | 1.36 |
| Metastatic | 6 | 4.08 |
| Peripheral vascular disease | 5 | 3.40 |
| Dementia | 3 | 2.04 |
| Peptic ulcer disease | 2 | 1.36 |
| Cerebrovascular accident or transient ischemic attack | 1 | 0.68 |
| Discharge types | ||
| Discharged home | 119 | 80.95 |
| Moved to another hospital ward | 2 | 1.36 |
| Intensive care unit (ICU) | 11 | 7.48 |
| Outcome | ||
| In-hospital mortality | 15 | 10.20 |
| 30-day mortality | 24 | 16.33 |
| Length of stay (LOS) (mean ± SD)-days | 8.26 ± 5.64 (1–33) * | |
| Antibiotics | Frequency (N) | % | Guideline Adherence | |||
|---|---|---|---|---|---|---|
| National | BTS/NICE/NICE | ATS/IDSA | ||||
| Monotherapies (N = 86; 100%) | ||||||
| Amoxicillin-clavulanic acid | 25 | 29.07 | ||||
| Ceftriaxone | 25 | 29.07 | ||||
| Moxifloxacin | 17 | 19.77 | ✓ | ✓ | ||
| Levofloxacin | 6 | 6.98 | ✓ | ✓ | ✓ | |
| Clarithromycin | 5 | 5.81 | ✓ | |||
| Meropenem | 4 | 4.65 | ||||
| Amoxicillin | 1 | 1.16 | ✓ | |||
| Doxycycline | 1 | 1.16 | ✓ | |||
| Metronidazole | 1 | 1.16 | ||||
| Norfloxacin | 1 | 1.16 | ||||
| Combination therapies (N = 61; 100%) | ||||||
| amoxicillin-clavulanic acid + clarithromycin | 23 | 37.70 | ✓ | ✓ | ||
| moxifloxacin + metronidazole | 7 | 11.48 | ||||
| ceftriaxone + metronidazole | 6 | 9.84 | ||||
| amoxicillin-clavulanic acid + metronidazole | 5 | 8.20 | ||||
| amoxicillin-clavulanic acid + clarithromycin + metronidazole | 3 | 4.92 | ||||
| ceftriaxone + clarithromycin | 2 | 3.28 | ✓ | ✓ | ||
| ceftriaxone + metronidazole + clarithromycin | 2 | 3.28 | ||||
| ceftriaxone + sulphamethoxazole and trimethoprim | 2 | 3.28 | ||||
| amoxicillin-clavulanic acid + clarithromycin + amikacin | 1 | 1.64 | ||||
| amoxicillin-clavulanic acid + flucloxacillin | 1 | 1.64 | ||||
| ceftriaxone + metronidazole + sulphamethoxazole and trimethoprim | 1 | 1.64 | ||||
| ceftriaxone + moxifloxacin | 1 | 1.64 | ✓ | |||
| levofloxacin + metronidazole | 1 | 1.64 | ||||
| meropenem + metronidazole | 1 | 1.64 | ||||
| moxifloxacin + flucloxacillin | 1 | 1.64 | ||||
| moxifloxacin + metronidazole + ceftriaxone | 1 | 1.64 | ||||
| piperacillin/tazobactame + amikacin | 1 | 1.64 | ||||
| piperacillin/tazobactame + metronidazole | 1 | 1.64 | ||||
| meropenem + vancomycin | 1 | 1.64 | ||||
| Parameters | N | % |
|---|---|---|
| 147 | 100 | |
| Adherence to the national guideline (agent choice) | 45 | 30.61 |
| Adherence to BTS/NICE guideline (agent choice) | 33 | 22.45 |
| Adherence to ATS/IDSA guideline (agent choice) | 23 | 15.65 |
| Adherence to at least one guideline (agent choice) | 51 | 34.69 |
| Type of the first antibiotic therapy | ||
| Combination therapies | 61 | 41.50 |
| Monotherapies | 86 | 58.50 |
| Most common therapies | ||
| beta-lactams and macrolide | 25 | 17.01 |
| beta-lactams | 51 | 34.69 |
| respiratory fluoroquinolones | 23 | 15.65 |
| Route of administration of the first antibiotic therapy | ||
| iv | 93 | 63.27 |
| oral | 54 | 36.73 |
| Duration of total antibiotic therapies | ||
| short therapy (1–6 days) | 120 | 81.63 |
| long therapy (≥ 7 days) | 27 | 18.37 |
| Number of consecutive antibiotic therapies | ||
| 1 | 85 | 57.8 |
| >1 (2–4) | 62 | 42.2 |
| Changes in the first empirical therapy | ||
| Sequential antibiotic therapy* | 14 | 9.52 |
| De-escalation | 6 | 4.08 |
| Escalation | 42 | 28.57 |
| No change | 85 | 57.8 |
| Adherence Frequency | % | |
|---|---|---|
| AB1-National CAP guideline adherence | 45 | 100 |
| appropriate use | 40 | 88.89 |
| overdose (compared to SPC, due to lack of guideline recommended dose) | 4 | 8.89 |
| underdose (due to body weight) | 1 | 2.22 |
| AB1-BTS/NICE CAP guideline adherence | 33 | 100 |
| appropriate use | 24 | 72.73 |
| underdose (compared to guideline) | 4 | 12.12 |
| overdose (in case of low levels of eGFR) | 4 | 12.12 |
| debatable use (absence of loading dose) | 1 | 3.03 |
| AB1-ATS/IDSA CAP guideline adherence | 23 | 100 |
| appropriate use | 18 | 78.26 |
| underdose (compared to guideline) | 3 | 13.04 |
| overdose (in case of low levels of eGFR) | 2 | 8.70 |
| 30-Day Survival | ||||
|---|---|---|---|---|
| Non-Survivors | Survivors | p-Value | ||
| Total | 24 (16.33%) | 123 (83.67%) | - | |
| Gender | male | 9 (14.06%) | 55 (85.94%) | 0.654 |
| female | 15 (18.07%) | 68 (81.93%) | ||
| Age (years) | mean ± SD | 81.57 ± 10.77 | 75.12 ± 13.43 | 0.028 |
| 20–64 | 2 (6.90%) | 27 (93.1%) | - | |
| 65–84 | 8 (11.11%) | 64 (88.89%) | ||
| 85+ | 14 (30.43%) | 32 (69.57%) | ||
| CCI score | mean ± SD | 5.71 ± 1.85 | 4.67 ± 1.83 | 0.012 |
| Diabetes mellitus | yes | 7 (21.21%) | 26 (78.79%) | 0.425 |
| no | 17 (14.91%) | 97 (85.09%) | ||
| Leukemia | yes | 5 (13.89%) | 31 (86.11%) | 0.798 |
| no | 19 (17.12%) | 92 (82.88%) | ||
| Chronic kidney disease | yes | 4 (57.14%) | 3 (42.86%) | 0.014 |
| no | 20 (14.29%) | 120 (85.71%) | ||
| Congestive heart failure | yes | 6 (12.77%) | 41 (87.23%) | 0.482 |
| no | 18 (18%) | 82 (82%) | ||
| Type of therapy | combination | 6 (9.84%) | 55 (90.16%) | 0.112 |
| monotherapy | 18 (20.93%) | 68 (79.07%) | ||
| National CAP guideline adherence | adherent | 7 (15.56%) | 38 (84.44%) | 1.000 |
| non-adherent | 17 (16.67%) | 85 (83.33%) | ||
| BTS/NICE CAP guideline adherence | adherent | 7 (21.21%) | 26 (78.79%) | 0.425 |
| non-adherent | 17 (14.91%) | 97 (85.09%) | ||
| ATS/IDSA CAP guideline adherence | adherent | 5 (21.74%) | 18 (78.26%) | 0.538 |
| non-adherent | 19 (15.32%) | 105 (84.68%) | ||
| CRP (mg/L) at admission | mean ± SD | 177.28 ± 118.94 | 112.88 ± 93.47 | 0.006 |
| high levels (8˂) | 20 (16.67%) | 101 (83.47%) | 0.449 | |
| normal levels (0–8) | 1 (8.33%) | 10 (90.91%) | ||
| NA | 3 (20%) | 12 (80%) | - | |
| B | S.E. | p-Value | OR | 95% CI for OR | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Age (years) | 0.058 | 0.032 | 0.072 | 1.059 | 0.995 | 1.128 |
| CCI score | 0.203 | 0.155 | 0.191 | 1.2259 | 0.904 | 1.659 |
| CRP 9 category * | 0.289 | 0.125 | 0.020 | 1.3362 | 1.046 | 1.705 |
| Constant | −8.562 | 2.675 | 0.001 | 0.000 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fésüs, A.; Benkő, R.; Matuz, M.; Engi, Z.; Ruzsa, R.; Hambalek, H.; Illés, Á.; Kardos, G. Impact of Guideline Adherence on Outcomes in Patients Hospitalized with Community-Acquired Pneumonia (CAP) in Hungary: A Retrospective Observational Study. Antibiotics 2022, 11, 468. https://doi.org/10.3390/antibiotics11040468
Fésüs A, Benkő R, Matuz M, Engi Z, Ruzsa R, Hambalek H, Illés Á, Kardos G. Impact of Guideline Adherence on Outcomes in Patients Hospitalized with Community-Acquired Pneumonia (CAP) in Hungary: A Retrospective Observational Study. Antibiotics. 2022; 11(4):468. https://doi.org/10.3390/antibiotics11040468
Chicago/Turabian StyleFésüs, Adina, Ria Benkő, Mária Matuz, Zsófia Engi, Roxána Ruzsa, Helga Hambalek, Árpád Illés, and Gábor Kardos. 2022. "Impact of Guideline Adherence on Outcomes in Patients Hospitalized with Community-Acquired Pneumonia (CAP) in Hungary: A Retrospective Observational Study" Antibiotics 11, no. 4: 468. https://doi.org/10.3390/antibiotics11040468
APA StyleFésüs, A., Benkő, R., Matuz, M., Engi, Z., Ruzsa, R., Hambalek, H., Illés, Á., & Kardos, G. (2022). Impact of Guideline Adherence on Outcomes in Patients Hospitalized with Community-Acquired Pneumonia (CAP) in Hungary: A Retrospective Observational Study. Antibiotics, 11(4), 468. https://doi.org/10.3390/antibiotics11040468