
Incidence of Vancomycin-Resistant Staphylococcus aureus Strains among Patients with Urinary Tract Infections

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Bacterial Isolates
2.2. Antibiotic Susceptibility Testing
2.3. β-Lactamase Detection
2.4. Plasmid Studies
3. Results
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nicolle, L.E. Urinary Tract Infection. In Nephrology Secrets; Elsevier: Amsterdam, The Netherlands, 2012; pp. 340–345. ISBN 978-1-4160-3362-2. [Google Scholar]
- Liu, N.H.; Daumit, G.L.; Dua, T.; Aquila, R.; Charlson, F.; Cuijpers, P.; Druss, B.; Dudek, K.; Freeman, M.; Fujii, C.; et al. Excess Mortality in Persons with Severe Mental Disorders: A Multilevel Intervention Framework and Priorities for Clinical Practice, Policy and Research Agendas. World Psychiatry 2017, 16, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary Tract Infections: Epidemiology, Mechanisms of Infection and Treatment Options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Shrank, W.H.; Rogstad, T.L.; Parekh, N. Waste in the US Health Care System: Estimated Costs and Potential for Savings. JAMA 2019, 322, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Baron, S. (Ed.) Medical Microbiology, 4th ed.; University of Texas Medical Branch at Galveston: Galveston, TX, USA, 1996; ISBN 978-0-9631172-1-2. [Google Scholar]
- Despotovic, A.; Milosevic, B.; Milosevic, I.; Mitrovic, N.; Cirkovic, A.; Jovanovic, S.; Stevanovic, G. Hospital-Acquired Infections in the Adult Intensive Care Unit—Epidemiology, Antimicrobial Resistance Patterns, and Risk Factors for Acquisition and Mortality. Am. J. Infect. Control 2020, 48, 1211–1215. [Google Scholar] [CrossRef]
- Seifu, W.D.; Gebissa, A.D. Prevalence and Antibiotic Susceptibility of Uropathogens from Cases of Urinary Tract Infections (UTI) in Shashemene Referral Hospital, Ethiopia. BMC Infect. Dis. 2018, 18, 30. [Google Scholar] [CrossRef]
- Kaper, J.B.; Nataro, J.P.; Mobley, H.L.T. Pathogenic Escherichia Coli. Nat. Rev. Microbiol. 2004, 2, 123–140. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Lee, S.-J.; Choe, H.-S. Community-Acquired Urinary Tract Infection by Escherichia Coli in the Era of Antibiotic Resistance. BioMed Res. Int. 2018, 2018, 7656752. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D.; Kaye, D. Urinary Tract Infections. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2015; pp. 886–913.e3. ISBN 978-1-4557-4801-3. [Google Scholar]
- Nauclér, P.; Huttner, A.; van Werkhoven, C.H.; Singer, M.; Tattevin, P.; Einav, S.; Tängdén, T. Impact of Time to Antibiotic Therapy on Clinical Outcome in Patients with Bacterial Infections in the Emergency Department: Implications for Antimicrobial Stewardship. Clin. Microbiol. Infect. 2021, 27, 175–181. [Google Scholar] [CrossRef]
- Gharbi, M.; Drysdale, J.H.; Lishman, H.; Goudie, R.; Molokhia, M.; Johnson, A.P.; Holmes, A.H.; Aylin, P. Antibiotic Management of Urinary Tract Infection in Elderly Patients in Primary Care and Its Association with Bloodstream Infections and All Cause Mortality: Population Based Cohort Study. BMJ 2019, 364, l525. [Google Scholar] [CrossRef]
- Sakr, A.; Brégeon, F.; Mège, J.-L.; Rolain, J.-M.; Blin, O. Staphylococcus Aureus Nasal Colonization: An Update on Mechanisms, Epidemiology, Risk Factors, and Subsequent Infections. Front. Microbiol. 2018, 9, 2419. [Google Scholar] [CrossRef]
- Parker, D.; Prince, A. Immunopathogenesis of Staphylococcus Aureus Pulmonary Infection. Semin. Immunopathol. 2012, 34, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Fukunaga, B.T.; Sumida, W.K.; Taira, D.A.; Davis, J.W.; Seto, T.B. Hospital-Acquired Methicillin-Resistant Staphylococcus Aureus Bacteremia Related to Medicare Antibiotic Prescriptions: A State-Level Analysis. Hawaii J. Med. Public Health 2016, 75, 303–309. [Google Scholar] [PubMed]
- Neyaz, L.; Rajagopal, N.; Wells, H.; Fakhr, M.K. Molecular Characterization of Staphylococcus Aureus Plasmids Associated With Strains Isolated From Various Retail Meats. Front. Microbiol. 2020, 11, 223. [Google Scholar] [CrossRef]
- Chambers, H.F.; Deleo, F.R. Waves of Resistance: Staphylococcus Aureus in the Antibiotic Era. Nat. Rev. Microbiol. 2009, 7, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Song, G.; Sun, M.; Wang, J.; Wang, Y. Prevalence and Therapies of Antibiotic-Resistance in Staphylococcus Aureus. Front. Cell. Infect. Microbiol. 2020, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, W.A.; Malachowa, N.; DeLeo, F.R. Vancomycin Resistance in Staphylococcus Aureus. Yale J. Biol. Med. 2017, 90, 269–281. [Google Scholar] [PubMed]
- Kang, H.-K.; Park, Y. Glycopeptide Antibiotics: Structure and Mechanisms of Action. J. Bacteriol. Virol. 2015, 45, 67. [Google Scholar] [CrossRef]
- Gardete, S.; Tomasz, A. Mechanisms of Vancomycin Resistance in Staphylococcus Aureus. J. Clin. Investig. 2014, 124, 2836–2840. [Google Scholar] [CrossRef]
- Fisher, J.F.; Mobashery, S. Enzymology of Bacterial Resistance. In Comprehensive Natural Products II; Elsevier: Amsterdam, The Netherlands, 2010; pp. 443–487. ISBN 978-0-08-045382-8. [Google Scholar]
- Périchon, B.; Courvalin, P. VanA-Type Vancomycin-Resistant Staphylococcus Aureus. Antimicrob. Agents Chemother. 2009, 53, 4580–4587. [Google Scholar] [CrossRef]
- Howden, B.P.; Davies, J.K.; Johnson, P.D.R.; Stinear, T.P.; Grayson, M.L. Reduced Vancomycin Susceptibility in Staphylococcus Aureus, Including Vancomycin-Intermediate and Heterogeneous Vancomycin-Intermediate Strains: Resistance Mechanisms, Laboratory Detection, and Clinical Implications. Clin. Microbiol. Rev. 2010, 23, 99–139. [Google Scholar] [CrossRef]
- Ahmed, M.O.; Baptiste, K.E. Vancomycin-Resistant Enterococci: A Review of Antimicrobial Resistance Mechanisms and Perspectives of Human and Animal Health. Microbial. Drug Resist. 2018, 24, 590–606. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.D.; Temkin, E.; Carmeli, Y. The Negative Impact of Antibiotic Resistance. Clin. Microbiol. Infect. 2016, 22, 416–422. [Google Scholar] [CrossRef]
- Faron, M.L.; Ledeboer, N.A.; Buchan, B.W. Resistance Mechanisms, Epidemiology, and Approaches to Screening for Vancomycin-Resistant Enterococcus in the Health Care Setting. J. Clin. Microbiol. 2016, 54, 2436–2447. [Google Scholar] [CrossRef] [PubMed]
- Shariati, A.; Dadashi, M.; Moghadam, M.T.; van Belkum, A.; Yaslianifard, S.; Darban-Sarokhalil, D. Global Prevalence and Distribution of Vancomycin Resistant, Vancomycin Intermediate and Heterogeneously Vancomycin Intermediate Staphylococcus Aureus Clinical Isolates: A Systematic Review and Meta-Analysis. Sci. Rep. 2020, 10, 12689. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Heilmann, C.; Peters, G. Coagulase-Negative S. aureus. Clin. Microbiol. Rev. 2014, 27, 870–926. [Google Scholar] [CrossRef]
- Tacconelli, E.; Tumbarello, M.; de Donati, K.G.; Bettio, M.; Spanu, T.; Leone, F.; Sechi, L.A.; Zanetti, S.; Fadda, G.; Cauda, R. Glycopeptide Resistance among Coagulase-Negative S. aureus That Cause Bacteremia: Epidemiological and Clinical Findings from a Case-Control Study. Clin. Infect. Dis. 2001, 33, 1628–1635. [Google Scholar] [CrossRef]
- Vergis, E.N.; Hayden, M.K.; Chow, J.W.; Snydman, D.R.; Zervos, M.J.; Linden, P.K.; Wagener, M.M.; Schmitt, B.; Muder, R.R. Determinants of Vancomycin Resistance and Mortality Rates in Enterococcal Bacteremia: A Prospective Multicenter Study. Ann. Intern. Med. 2001, 135, 484. [Google Scholar] [CrossRef]
- Benamu, E.; Deresinski, S. Vancomycin-Resistant Enterococcus Infection in the Hematopoietic Stem Cell Transplant Recipient: An Overview of Epidemiology, Management, and Prevention. F1000Research 2018, 7, 3. [Google Scholar] [CrossRef]
- Cetinkaya, Y.; Falk, P.; Mayhall, C.G. Vancomycin-Resistant Enterococci. Clin. Microbiol. Rev. 2000, 13, 686–707. [Google Scholar] [CrossRef]
- Tiwari, H.K.; Sen, M.R. Emergence of Vancomycin Resistant Staphylococcus Aureus(VRSA) from a Tertiary Care Hospital from Northern Part of India. BMC Infect. Dis. 2006, 6, 156. [Google Scholar] [CrossRef]
- Cong, Y.; Yang, S.; Rao, X. Vancomycin Resistant Staphylococcus Aureus Infections: A Review of Case Updating and Clinical Features. J. Adv. Res. 2020, 21, 169–176. [Google Scholar] [CrossRef]
- Hughes, R.G. (Ed.) Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Advances in Patient Safety; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. [Google Scholar]
- Leiros, H.-K.S.; Thomassen, A.M.; Samuelsen, Ø.; Flach, C.-F.; Kotsakis, S.D.; Larsson, D.G.J. Structural Insights into the Enhanced Carbapenemase Efficiency of OXA-655 Compared to OXA-10. FEBS Open Bio 2020, 10, 1821–1832. [Google Scholar] [CrossRef] [PubMed]
- Stojanoski, V.; Hu, L.; Sankaran, B.; Wang, F.; Tao, P.; Prasad, B.V.V.; Palzkill, T. Mechanistic Basis of OXA-48-like β-Lactamases’ Hydrolysis of Carbapenems. ACS Infect. Dis. 2021, 7, 445–460. [Google Scholar] [CrossRef] [PubMed]
- Skov, R.; Larsen, A.R.; Frimodt-Møller, N.; Espersen, F. Evaluation of Different Disk Diffusion/Media Combinations for Detection of Methicillin Resistance in Staphylococcus Aureus and Coagulase-Negative S. aureus. APMIS 2003, 111, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Odugbemi, T.O.; Hafiz, S.; McEntegart, M.G. Penicillinase-Producing Neisseria Gonorrhoeae: Detection by Starch Paper Technique. BMJ 1977, 2, 500. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sambrook, J. Molecular Cloning: A Laboratory Manual.; Cold Spring Harbor: New York, NY, USA, 1991; ISBN 978-0-87969-373-2. [Google Scholar]
- Rawat, D.; Nair, D. Extended-Spectrum β-Lactamases in Gram Negative Bacteria. J. Glob. Infect. Dis. 2010, 2, 263–274. [Google Scholar] [CrossRef]
- Tooke, C.L.; Hinchliffe, P.; Bragginton, E.C.; Colenso, C.K.; Hirvonen, V.H.A.; Takebayashi, Y.; Spencer, J. β-Lactamases and β-Lactamase Inhibitors in the 21st Century. J. Mol. Biol. 2019, 431, 3472–3500. [Google Scholar] [CrossRef]
- Foxman, B. Epidemiology of Urinary Tract Infections: Incidence, Morbidity, and Economic Costs. Am. J. Med. 2002, 113 (Suppl. 1A), 5S–13S. [Google Scholar] [CrossRef]
- Patterson, J.E.; Andriole, V.T. Bacterial Urinary Tract Infections in Diabetes. Infect. Dis. Clin. N. Am. 1997, 11, 735–750. [Google Scholar] [CrossRef]
- Ronald, A.R.; Harding, G.K. Complicated Urinary Tract Infections. Infect. Dis. Clin. N. Am. 1997, 11, 583–592. [Google Scholar] [CrossRef]
- Llor, C.; Bjerrum, L. Antimicrobial Resistance: Risk Associated with Antibiotic Overuse and Initiatives to Reduce the Problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef]
- Mores, C.R.; Montelongo, C.; Putonti, C.; Wolfe, A.J.; Abouelfetouh, A. Investigation of Plasmids Among Clinical Staphylococcus Aureus and Staphylococcus haemolyticus Isolates From Egypt. Front. Microbiol. 2021, 12, 659116. [Google Scholar] [CrossRef] [PubMed]
- Igumbor, E.; Gwanzura, L.; Chirara, M.; Obi, C.; Muza, D.; Chihara, M. Antibiotic Sensitivity and Plasmid Profiles of Pseudomonas Aeruginosa. Cent. Afr. J. Med. 2000, 46, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Lyon, B.R.; Skurray, R. Antimicrobial Resistance of Staphylococcus Aureus: Genetic Basis. Microbiol. Rev. 1987, 51, 88–134. [Google Scholar] [CrossRef] [PubMed]
- Munita, J.M.; Arias, C.A. Mechanisms of Antibiotic Resistance. Microbiol. Spectr. 2016, 4, 1–37. [Google Scholar] [CrossRef]
- Manyi-Loh, C.; Mamphweli, S.; Meyer, E.; Okoh, A. Antibiotic Use in Agriculture and Its Consequential Resistance in Environmental Sources: Potential Public Health Implications. Molecules 2018, 23, 795. [Google Scholar] [CrossRef]
- Brook, I.; Wexler, H.M.; Goldstein, E.J.C. Antianaerobic Antimicrobials: Spectrum and Susceptibility Testing. Clin. Microbiol. Rev. 2013, 26, 526–546. [Google Scholar] [CrossRef]
- Ventola, C.L. The Antibiotic Resistance Crisis: Part 1: Causes and Threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Doron, S.; Davidson, L.E. Antimicrobial Stewardship. Mayo Clin. Proc. 2011, 86, 1113–1123. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
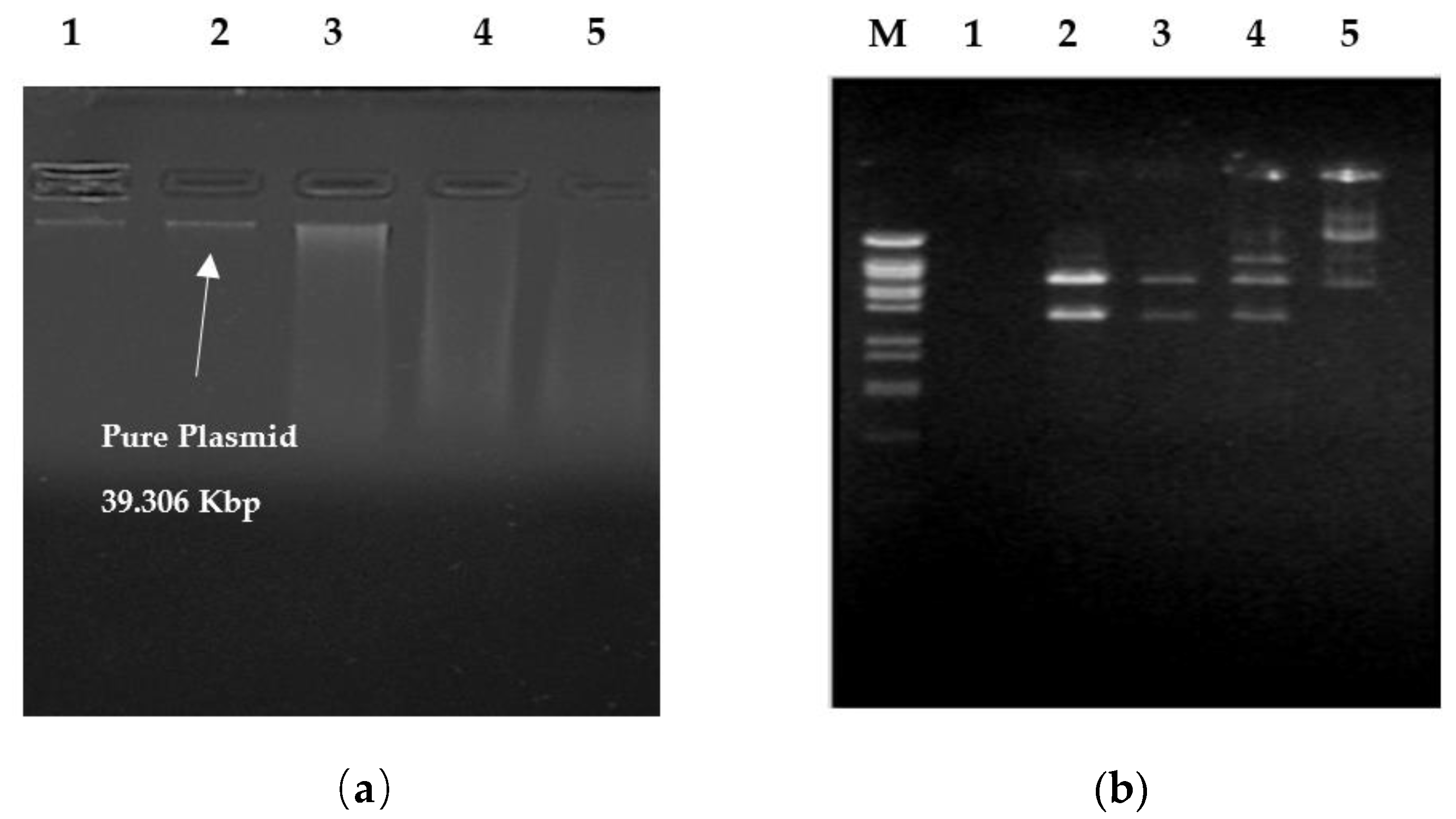
| Endonuclease Enzymes | Hind III | EcoR I | BamH I |
|---|---|---|---|
| No. of Recognition Sites | 6 | 6 | 8 |
| No. of Fragments | 5 | 5 | 7 |
| Size of Fragments (Kbp) | 23.00–6.557–5.148–4.973–3.530 | 22.000–5.804–49.73–3.530–2.037 | 9.416–7.421–5.148–5.100–3.430–3.530–2.322 |
| Plasmid Size (Kbp) | 39.306 Kbp | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selim, S.; Faried, O.A.; Almuhayawi, M.S.; Saleh, F.M.; Sharaf, M.; El Nahhas, N.; Warrad, M. Incidence of Vancomycin-Resistant Staphylococcus aureus Strains among Patients with Urinary Tract Infections. Antibiotics 2022, 11, 408. https://doi.org/10.3390/antibiotics11030408
Selim S, Faried OA, Almuhayawi MS, Saleh FM, Sharaf M, El Nahhas N, Warrad M. Incidence of Vancomycin-Resistant Staphylococcus aureus Strains among Patients with Urinary Tract Infections. Antibiotics. 2022; 11(3):408. https://doi.org/10.3390/antibiotics11030408
Chicago/Turabian StyleSelim, Samy, Osama Ahmed Faried, Mohammed S. Almuhayawi, Fayez M. Saleh, Mohamed Sharaf, Nihal El Nahhas, and Mona Warrad. 2022. "Incidence of Vancomycin-Resistant Staphylococcus aureus Strains among Patients with Urinary Tract Infections" Antibiotics 11, no. 3: 408. https://doi.org/10.3390/antibiotics11030408
APA StyleSelim, S., Faried, O. A., Almuhayawi, M. S., Saleh, F. M., Sharaf, M., El Nahhas, N., & Warrad, M. (2022). Incidence of Vancomycin-Resistant Staphylococcus aureus Strains among Patients with Urinary Tract Infections. Antibiotics, 11(3), 408. https://doi.org/10.3390/antibiotics11030408