
Antiseptic Agents for Chronic Wounds: A Systematic Review

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
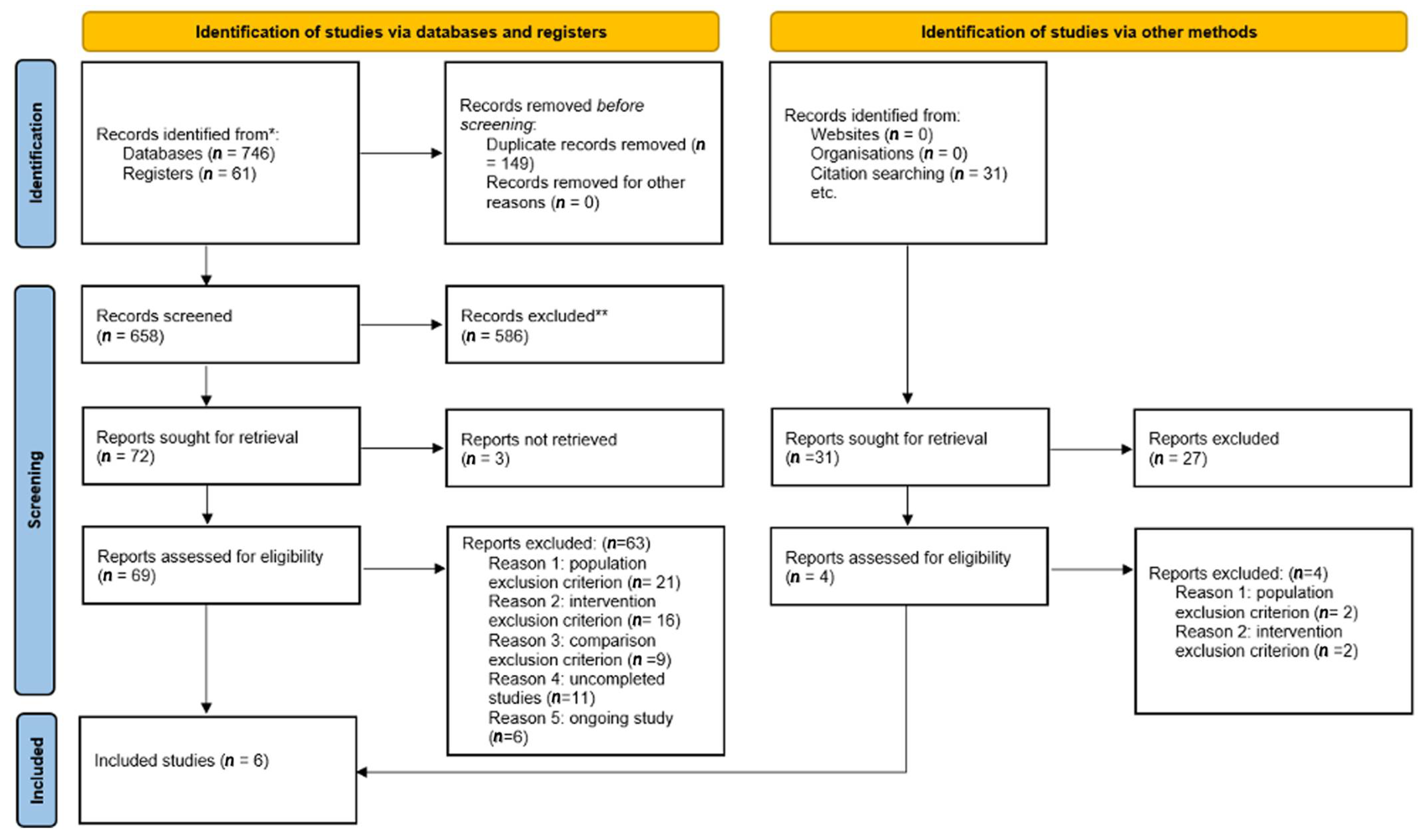
2.1. Characteristics of the Included Studies
2.2. Iodine vs. Saline (3 Randomised Controlled Trials (RCT), 260 Patients)
2.3. Polyhexanide Compared to Saline (2 RCT, 334 Patients)
2.4. Octenidine Compared to Saline (1 RCT, 126 Patients)
3. Discussion
4. Materials and Methods
4.1. Selection Criteria and Search Strategy
- Population: Our population was adult patients (≥18 years) with chronic wounds as previously defined [2]. We included studies from primary, secondary, and tertiary clinical settings. We included different types of chronic wounds (leg ulcer, DFU, PU, eschar). We excluded studies containing patients with wounds requiring specific care (acute wounds, burn wounds, systemic infected wound, postsurgical wounds).
- Interventions of interest were those including antiseptics as cleansing method or within a dressing with at least weekly application.
- Comparative regimens included saline solution or another antiseptic. We anticipated that interventions would consist of povidone-iodine, hypochlorite or hypochlorous acid, iodine, polyhexanide, and octenidine in the form of creams, ointments, powders, sprays, or impregnated into dressings. We included intervention schedules applying concurrent therapies (e.g., negative pressure wound therapy) if the therapy was common across study arms. We excluded (i) interventions where the antiseptic agent was not the only systematic difference between treatment groups; (ii) physical and biological therapies with antimicrobial properties, such as heat or larval therapy; (iii) studies evaluating topical antiseptics in prevention of chronical wounds or those using antiseptics as preparation for surgical treatment of ulcers; (iv) studies evaluating non-recommended antiseptics in chronic wound care and those evaluating antiseptic agents alongside antibiotic agents.
- Outcome: The primary outcome was wound healing, evaluated as the proportion of patients with complete healing during follow-up and/or the time to complete wound healing (analysed using survival, time-to-event approaches). An adjustment for relevant covariates such as baseline wound area or duration were ideally used to evaluate the outcome. The secondary outcomes were healing rate (described as changes or rate of change in wound size, with adjustment for baseline size); mean pain scores; bacterial bioburden reduction; and AEs, including infection.
4.2. Data Collection and Analysis
4.3. Risk of Bias and Certainty of the Evidence
4.4. Role of the Funding Source
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix
Appendix A.1. Medline and Cochrane Library Search
- (((((chronic wound) OR diabetic foot) OR leg ulcer) OR pressure ulcer) OR eschar) AND (((iodine) OR povidone iodine OR betadine) OR cadexomer iodine).
- (((((chronic wound) OR diabetic foot) OR leg ulcer) OR pressure ulcer) OR eschar) AND ((((hypochlorite) OR hypochlorous) OR Dakin) OR Javel).
- (((((chronic wound) OR diabetic foot) OR leg ulcer) OR pressure ulcer) OR eschar) AND ((((PHMB) OR polyhexanide) OR Polyhexamethylene biguanide) OR Polyhexamethylene).
- (((((chronic wound) OR diabetic foot) OR leg ulcer) OR pressure ulcer) OR eschar) AND (Octenidine).
References
- Järbrink, K.; Ni, G.; Sönnergren, H.; Schmidtchen, A.; Pang, C.; Bajpai, R.; Car, J. Prevalence and incidence of chronic wounds and related complications: A protocol for a systematic review. Syst. Rev. 2016, 5, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirsner, R. The Wound Healing Society chronic wound ulcer healing guidelines update of the 2006 guidelines—Blending old with new. Wound Repair Regen. 2016, 24, 110–111. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Berendt, A.R.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; LeFrock, J.L.; Lew, D.P.; Mader, J.T.; Norden, C.; et al. Infectious Diseases Society of America. Diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2004, 39, 885–910. [Google Scholar] [CrossRef] [PubMed]
- Société de Pathologie Infectieuse de Langue Française. Management of diabetic foot infections. Long text. Société de Pathologie Infectieuse de Langue Française. Med. Mal. Infect. 2007, 37, 26–50. [Google Scholar]
- Bjarnsholt, T. The role of bacterial biofilms in chronic infections. APMIS 2013, 121(s136), 1–58. [Google Scholar] [CrossRef]
- Pouget, C.; Dunyach-Remy, C.; Pantel, A.; Schuldiner, S.; Sotto, A.; Lavigne, J.P. Biofilms in diabetic foot ulcers: Significance & clinical relevance. Microorganisms 2020, 8, 1580. [Google Scholar]
- Schultz, G.; Bjarnsholt, T.; James, G.A.; Leaper, D.J.; McBain, A.J.; Malone, M.; Stoodley, P.; Swanson, T.; Tachi, M.; Wolcott, R.D. Global Wound Biofilm Expert Panel. Consensus guidelines for the identification and treatment of biofilms in chronic nonhealing wounds. Wound Repair Regen. 2017, 25, 744–757. [Google Scholar] [CrossRef]
- Dissemond, J.; Assadian, O.; Gerber, V.; Kingsley, A.; Kramer, A.; Leaper, D.J.; Mosti, G.; Piatkowski de Grzymala, A.; Riepe, G.; Risse, A.; et al. Classification of wounds at risk and their antimicrobial treatment with polyhexanide: A practice-oriented expert recommendation. Skin Pharmacol. Physiol. 2011, 24, 245–255. [Google Scholar] [CrossRef]
- Bakker, K.; Apelqvist, J.; Lipsky, B.A.; Van Netten, J.J. International Working Group on the Diabetic Foot. The 2015 IWGDF guidance documents on prevention and management of foot problems in diabetes: Development of an evidence-based global consensus. Diabetes Metab. Res. Rev. 2016, 32, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Wolcott, R.D.; Kennedy, J.P.; Dowd, S.E. Regular debridement is the main tool for maintaining a healthy wound bed in most chronic wounds. J. Wound Care. 2009, 18, 54–56. [Google Scholar] [CrossRef] [Green Version]
- Sibbald, R.G.; Elliott, J.A.; Persaud-Jaimangal, R.; Goodman, L.; Armstrong, D.G.; Harley, C.; Coelho, S.; Xi, N.; Evans, R.; Mayer, D.O.; et al. Wound Bed Preparation 2021. Adv. Skin Wound Care. 2021, 34, 183–195. [Google Scholar] [CrossRef]
- Sun, X.; Chen, J.; Zhang, J.; Wang, W.; Sun, J.; Wang, A. Maggot debridement therapy promotes diabetic foot wound healing by up-regulating endothelial cell activity. J. Diabetes Complicat. 2016, 30, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Ayello, E.A.; Cuddigan, J.E. Debridement: Controlling the necrotic/cellular burden. Adv. Skin Wound Care 2004, 17, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, S.R.; McGuire, J.; Zinszer, K. Management of skin ulcers: Understanding the mechanism and selection of enzymatic debriding agents. Adv. Skin Wound Care 2008, 21, 72–74. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, F.; De Francesco, M.; Riccio, M. Hyaluronic Acid/Collagenase Ointment in the Treatment of Chronic Hard-to-Heal Wounds: An Observational and Retrospective Study. J. Clin. Med. 2022, 11, 537. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, P.; Kukrele, R.; Sharma, D. Vacuum assisted closure (VAC)/negative pressure wound therapy (NPWT) for difficult wounds: A review. J. Clin. Orthop. Trauma. 2019, 10, 845–848. [Google Scholar] [CrossRef]
- O’Meara, S.; Cullum, N.; Nelson, E.A.; Dumville, J.C. Compression for venous leg ulcers. Cochrane Database Syst. Rev. 2012, 11, CD000265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vouillarmet, J.; Bourron, O.; Gaudric, J.; Lermusiaux, P.; Millon, A.; Hartemann, A. Lower-extremity arterial revascularization: Is there any evidence for diabetic foot ulcer-healing? Diabetes Metab. 2016, 42, 4–15. [Google Scholar] [CrossRef]
- Schaper, N.C.; van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Hinchliffe, R.J.; Lipsky, B.A. IWGDF Editorial Board. Practical guidelines on the prevention and management of diabetic foot diseases (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36, e3266. [Google Scholar] [CrossRef] [Green Version]
- Bowers, S.; Franco, E. Chronic wounds: Evaluation and management. Am. Fam. Physician. 2020, 101, 159–166. [Google Scholar]
- Kramer, A.; Dissemond, J.; Kim, S.; Willy, C.; Mayer, D.; Papke, R.; Tuchmann, F.; Assadian, O. Consensus on wound antisepsis: Update 2018. Skin Pharmacol. Physiol. 2018, 31, 28–58. [Google Scholar] [CrossRef] [PubMed]
- Babalska, Z.Ł.; Korbecka-Paczkowska, M.; Karpiński, T.M. Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment. Pharmaceuticals 2021, 14, 1253. [Google Scholar] [CrossRef] [PubMed]
- Pouget, C.; Dunyach-Remy, C.; Pantel, A.; Boutet-Dubois, A.; Schuldiner, S.; Sotto, A.; Lavigne, J.P.; Loubet, P. Alternative approaches for the management of diabetic foot ulcers. Front. Microbiol. 2021, 12, 747618. [Google Scholar] [CrossRef] [PubMed]
- Rayman, G.; Vas, P.; Dhatariya, K.; Driver, V.; Hartemann, A.; Londahl, M.; Piagessi, A.; Apelqvist, J.; Attinger, C.; Game, F. International Working Group on the Diabetic Foot (IWGDF). Guidelines on use of interventions to enhance healing of chronic foot ulcers in diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36, e3283. [Google Scholar] [CrossRef] [Green Version]
- Norman, G.; Dumville, J.C.; Moore, Z.E.H.; Tanner, J.; Christie, J.; Goto, S. Antibiotics and antiseptics for pressure ulcers. Cochrane Database Syst. Rev. 2016, 4, CD011586. [Google Scholar] [CrossRef]
- Dogra, S.; Sarangal, R. Summary of recommendations for leg ulcers. Indian Dermatol. Online J. 2014, 5, 400–407. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Senneville, E.; Abbas, Z.G.; Aragón-Sánchez, J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; van Asten, S.A.; et al. International Working Group on the Diabetic Foot (IWGDF). Guidelines on the diagnostic and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36, e3280. [Google Scholar] [CrossRef] [Green Version]
- Gwak, H.C.; Han, S.H.; Lee, J.; Park, S.; Sung, K.S.; Kim, H.J.; Chun, D.; Lee, K.; Ahn, J.H.; Kwak, K.; et al. Efficacy of a povidone-iodine foam dressing (Betafoam) on diabetic foot ulcer. Int. Wound J. 2020, 17, 91–99. [Google Scholar] [CrossRef]
- Vanscheidt, W.; Harding, K.; Téot, L.; Siebert, J. Effectiveness and tissue compatibility of a 12-week treatment of chronic venous leg ulcers with an octenidine based antiseptic—A randomized, double-blind controlled study. Int. Wound J. 2012, 9, 316–323. [Google Scholar] [CrossRef]
- Bellingeri, A.; Falciani, F.; Traspedini, P.; Moscatelli, A.; Russo, A.; Tino, G.; Chiari, P.; Peghetti, A. Effect of a wound cleansing solution on wound bed preparation and inflammation in chronic wounds: A single-blind RCT. J. Wound Care 2016, 25, 160–168. [Google Scholar] [CrossRef] [Green Version]
- Holloway, G.A.; Johansen, K.H.; Barnes, R.W.; Pierce, G.E. Multicenter trial of cadexomer iodine to treat venous stasis ulcer. West J. Med. 1989, 151, 35–38. [Google Scholar] [PubMed]
- Raju, R.; Kethavath, S.N.; Sangavarapu, S.M.; Kanjarla, P. Efficacy of cadexomer iodine in the treatment of chronic ulcers: A randomized, multicenter, controlled trial. Wounds 2019, 31, 85–90. [Google Scholar] [PubMed]
- Sibbald, R.G.; Coutts, P.; Woo, K.Y. Reduction of bacterial burden and pain in chronic wounds using a new polyhexamethylene biguanide antimicrobial foam dressing-clinical trial results. Adv. Skin Wound Care 2011, 24, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savonic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- O’Meara, S.M.; Cullum, N.A.; Majid, M.; Sheldon, T.A. Systematic review of antimicrobial agents used for chronic wounds. Br. J. Surg. 2001, 88, 4–21. [Google Scholar] [CrossRef]
- Hämmerle, G.; Strohal, R. Efficacy and cost-effectiveness of octenidine wound gel in the treatment of chronic venous leg ulcers in comparison to modern wound dressings. Int. Wound J. 2016, 13, 182–188. [Google Scholar] [CrossRef]
- To, E.; Dyck, R.; Gerber, S.; Kadavil, S.; Woo, K.Y. The effectiveness of topical polyhexamethylene biguanide (PHMB) agents for the treatment of chronic wounds: A systematic review. Surg. Technol. Int. 2016, 29, 45–51. [Google Scholar]
- Dwan, K.; Altman, D.G.; Arnaiz, J.A.; Bloom, J.; Chan, A.W.; Cronin, E.; Decullier, E.; Easterbrook, P.J.; Von Elm, E.; Gamble, C.; et al. Systematic review of the empirical evidence of study publication bias and outcome reporting bias. PLoS One 2008, 3, e3081. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.W.; Hróbjartsson, A.; Haahr, M.T.; Gøtzsche, P.C.; Altman, D.G. Empirical evidence for selective reporting of outcomes in randomized trials: Comparison of protocols to published articles. JAMA 2004, 291, 2457–2465. [Google Scholar] [CrossRef] [Green Version]
- Bahamondez-Canas, T.F.; Heersema, L.A.; Smyth, H.D.C. Current status of in vitro models and assays for susceptibility testing for wound biofilm infections. Biomedicines 2019, 7, 34. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, W.P. Randomised and non-randomised studies to estimate the effect of community-level public health interventions: Definitions and methodological considerations. Emerg. Themes Epidemiol. 2017, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Higgings, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, W.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Cochrane. 2021. Available online: www.training.cochrane.org/handbook (accessed on 17 January 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of interventions v6.0; Higgins, J.P.T., Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2019; Available online: www.training.cochrane.org/handbook/current/chapter-08 (accessed on 17 January 2022).


{kind=link}
| Study | Country | Date | Setting | Number of Participants | Diagnosis | Main Outcome (Scale Details) | Duration of the Study | Intervention | Comparator |
|---|---|---|---|---|---|---|---|---|---|
| Gwak et al., 2020 [28] | Korea | March 2016–September 2017 | Multicentre 10 sites | 71 | DFU ≥ 1 cm2 post debridement and no clinical signs of infection | Proportion of patients with complete wound healing | 8 weeks | PVP-I 44.4% (16/36) | Saline 44.1% (15/35) |
| Raju et al., 2019 [32] | India | March 2016–March 2017 | Multicentre 15 sites | 124 | Chronic ulcers (single VLU, DFU, PU with adequate arterial blood supply) | Proportion of patients with complete wound healing | 12 weeks | Cadexomer iodine ointment: 65.9% (27/41) Cadexomer iodine powder: 58.1% (25/43) | Saline 20% (8/40) |
| Bellingeri et al., 2016 [30] | Italy | June 2010–December 2013 | Multicentre 6 sites | 289 | PU less than 80 cm2 | Wound improvement measured by BWAT scale tool | 4 weeks | PHMB | Saline |
| Vanscheidt et al., 2011 [29] | Germany, France, Hungary, UK | November 2007–December 2009 | Multicentre 15 sites | 126 | Chronic venous ulcer locally infected | Time to complete wound healing Proportion of patients with complete wound healing | 12 weeks | Octenidine 92 days 30.6% (15/49) | Saline 87 days 32.0% (16/50) |
| Sibbald et al., 2011 [33] | Canada | February 2008–April 2009 | Multicentre 2 sites | 40 | Chronic wounds > 1 cm2 | Healing rate | 4 weeks | PHMB 35% reduction in wound surface | Saline 28% reduction in wound surface |
| Holloway et al., 1989 [31] | USA | NG | Multicentre 3 sites | 75 | At least a venous stasis ulcer present for a minimum of 3 months | Healing rate | 24 weeks | Cadexomer iodine 0.95 cm2 per week | Saline 0.41 cm2 per week |
| Comparison One: Iodine Compared to Normal Saline for Chronic Wound Care | |||||
|---|---|---|---|---|---|
| Patient or Population: Chronic Wound Care Intervention: Iodine Comparison: Normal Saline | |||||
| Outcomes | Anticipated Absolute Effects * (95% CI) | Relative Effect (95% CI) | № of Participants (Studies) | Certainty of the Evidence (GRADE) | |
| Risk with Normal Saline | Risk with Iodine | ||||
| Proportion of patients with complete wound healing assessed with: visual assessment follow up: range 8 weeks to 12 weeks | 307 per 1000 | 567 per 1000 (390 to 824) | RR 1.8478 (1.2706 to 2.6874) | 195 (2 RCTs) | ⨁⨁⨁◯ MODERATE a |
| Adverse events assessed with: report follow-up: range 8 weeks to 24 weeks | 115 per 1000 | 166 per 1000 (89 to 308) | RR 1.440 (0.774 to 2.676) | 270 (3 RCTs) | ⨁⨁⨁◯ MODERATE a |
| Ulcer healing rate (healing rate) assessed with: planimetry follow-up: range 8 weeks to 24 weeks | Raju et al. [32] found a significantly (p < 0.001) higher percentage of reduction for both formulations of iodine (94.3% and 90.4%) compared to saline (67.8%). Holloway et al. [31] found a rate reported to baseline of 0.04 ± 0.01 cm2/week/cm2 for cadexomer iodine and 0.03 ± 0.01 cm2/week/cm2 for saline. There was no significant difference (p = 0.079). Gwak et al. [28] presented the healing rate with three different visual displays showing the percentage change rate for the length, the width, and the area. They found no difference. | 270 (3 RCTs) | ⨁◯◯◯ VERY LOW b,c,d | ||
| Pain evaluation (Pain) assessed with: mean rate of change follow up: mean 24 weeks | The mean rate of change in pain scores were −2.44 ± 0.4 for cadexomer iodine and −2.47 ± 0.3 with saline with a p = 0.96. | (1 RCT) | ⨁⨁◯◯ LOW d,e | ||
| GRADE Working Group grades of evidence ⨁⨁⨁⨁ High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. ⨁⨁⨁ Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. ⨁⨁ Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. ⨁ Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. | |||||
| Comparison Two: Polyhexanide Compared to Saline for Chronic Wound Care | |||||
|---|---|---|---|---|---|
| Patient or Population: Chronic Wound Care Intervention: Polyhexanide Comparison: Saline | |||||
| Outcomes | Anticipated Absolute Effects * (95% CI) | Relative Effect (95% CI) | № of Participants (Studies) | Certainty of the Evidence (GRADE) | |
| Risk with Saline | Risk with Polyhexanide | ||||
| Wound healing follow-up: mean 4 weeks Not measured | Not reported | (0 studies) | - | ||
| Adverse events assessed with: report follow-up: mean 4 days | 12 per 1000 | 2 per 1000 (0 to 50) | RR 0.2024 (0.0098 to 4.1813) | 334 (2 RCTs) | ⨁⨁◯◯ LOW a,b |
| Healing rate assessed with: planimetry follow-up: median 4 weeks | Bellingeri et al. [30] found a significantly better progression of wounds in the polyhexanide group (p = 0.0025) using the BWAT wound assessment scale. Sibbald et al. [33] found no significant difference (p = 0.85) between the two groups by comparing wound surface reduction (35% vs. 28%). | 334 (2 RCTs) | ⨁⨁◯◯ LOW a,b | ||
| Pain assessment assessed with: Pain scales follow-up: mean 4 weeks | Bellingeri et al. [30] found similar pain scores with no significant difference in the two groups (average score = 3 with minimal or no change during follow up). Sibbald et al. [33] reported significant pain reduction in the polyhexanide group compared to the saline control group (73.1% vs. 38.1%; p = 0.02). | (2 RCTs) | ⨁⨁◯◯ LOW a,b | ||
| GRADE Working Group grades of evidence ⨁⨁⨁⨁ High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. ⨁⨁⨁ Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. ⨁⨁ Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. ⨁ Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. | |||||
| Comparison Three: Octenidine Compared to Saline for Chronic Wound Care | |||||
|---|---|---|---|---|---|
| Patient or Population: Chronic Wound Care Intervention: Octenidine Comparison: Saline | |||||
| Outcomes | Anticipated Absolute Effects * (95% CI) | Relative Effect (95% CI) | № of Participants (Studies) | Certainty of the Evidence (GRADE) | |
| Risk with Saline | Risk with Octenidine | ||||
| Wound healing assessed with: Proportion of patients with complete wound healing follow-up: mean 12 weeks | 242 per 1000 | 250 per 1000 (136 to 461) | RR 1.0313 (0.5595 to 1.9009) | 126 (1 RCT) | ⨁⨁⨁⨁ HIGH |
| Adverse events assessed with: AE report follow-up: mean 12 weeks | 317 per 1000 | 178 per 1000 (90 to 351) | RR 0.5614 (0.2844 to 1.1081) | 120 (1 RCT) | ⨁⨁⨁⨁ HIGH |
| Healing rate assessed with: planimetry follow-up: mean 12 weeks | No difference in the healing rate of the patients in the octenidine group, compared to patients in the saline group (37.9% vs. 40.3%; p = 0.769) [29]. | (1 RCT) | ⨁⨁⨁⨁ HIGH | ||
| Pain assessment—not measured | Not reported | - | - | ||
| GRADE Working Group grades of evidence ⨁⨁⨁⨁ High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. ⨁⨁⨁ Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. ⨁⨁ Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. ⨁ Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrigah-Benissan, K.; Ory, J.; Sotto, A.; Salipante, F.; Lavigne, J.-P.; Loubet, P. Antiseptic Agents for Chronic Wounds: A Systematic Review. Antibiotics 2022, 11, 350. https://doi.org/10.3390/antibiotics11030350
Barrigah-Benissan K, Ory J, Sotto A, Salipante F, Lavigne J-P, Loubet P. Antiseptic Agents for Chronic Wounds: A Systematic Review. Antibiotics. 2022; 11(3):350. https://doi.org/10.3390/antibiotics11030350
Chicago/Turabian StyleBarrigah-Benissan, Koko, Jérôme Ory, Albert Sotto, Florian Salipante, Jean-Philippe Lavigne, and Paul Loubet. 2022. "Antiseptic Agents for Chronic Wounds: A Systematic Review" Antibiotics 11, no. 3: 350. https://doi.org/10.3390/antibiotics11030350
APA StyleBarrigah-Benissan, K., Ory, J., Sotto, A., Salipante, F., Lavigne, J.-P., & Loubet, P. (2022). Antiseptic Agents for Chronic Wounds: A Systematic Review. Antibiotics, 11(3), 350. https://doi.org/10.3390/antibiotics11030350