
Periprosthetic Joint Infection (PJI)—Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone—A Retrospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Kaplan–Meier Analysis
2.3. Statistics
2.4. Allograft Bone as Antibiotic Carrier
2.5. Treatment Protocol
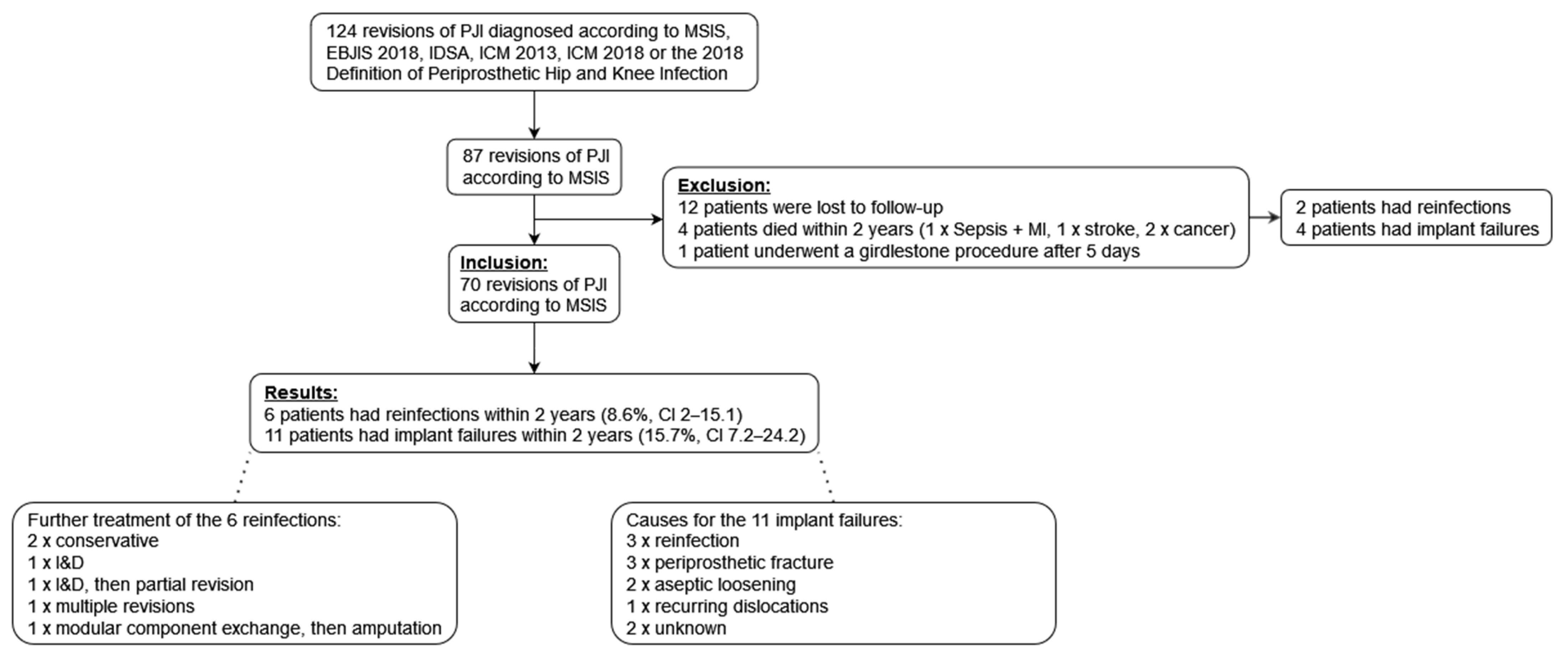
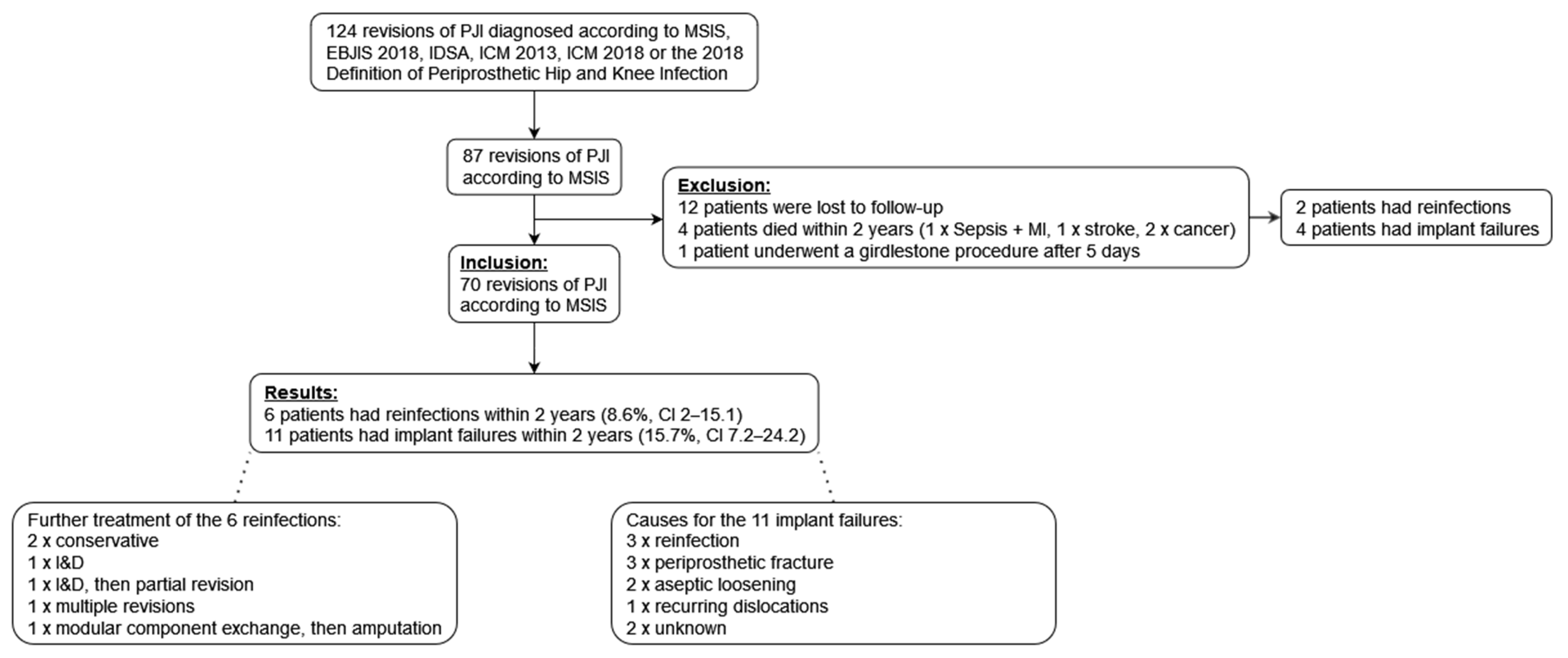
3. Results
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PJI Definition | MSIS 2011 | EBJIS 2018 | IDSA 2013 | ICM 2013 | ICM 2018 |
|---|---|---|---|---|---|
| Scoring System | 1 of the 2 Major Criteria OR ≥4 of 6 Minor Criteria | ≥1 Positive Criteria | ≥1 Positive Criteria | 1 of the 2 Major Criteria OR ≥3 of 5 Minor Criteria | 1 of the 2 Major Criteria OR Minor criteria scoring: ≥6 Infected 3–5 Possibly infected <3 Not infected |
| Criteria | Major: (1) Sinus tract communicating with the prosthesis (2) A pathogen is isolated by culture from at least two separate tissue or fluid samples obtained from the affected prosthetic joint a) Minor: (a) Elevated ESR (>30 mm/h) and CRP (>10 mg/L) concentration (b) Elevated synovial leukocyte count (c) Elevated PMN% (d) Purulence in the affected joint (e) Isolation of a microorganism in one culture of periprosthetic tissue or fluid (f) Greater than five neutrophils per high-power field in five high-power fields observed from histologic analysis of periprosthetic tissue at ×400 magnification | (1) Purulence around the prosthesis or sinus tract (2) Increase synovial fluid leukocyte count (>2000 cells/mL or >70% granulocytes) (3) Positive histopathology (type II or III according to Krenn et al. [92]) (4) ≥1 positive synovial fluid culture (5) ≥1 positive sonication culture (>50 colony-forming units/mL of sonication fluid.) (6) ≥2 positive periprosthetic tissue cultures (for highly virulent organisms b) one sample confirms infection) | (1) Sinus tract communicating with the prosthesis (2) Purulence without other etiology surrounding the prosthesis (3) Acute inflammation seen on histopathological examination of the periprosthetic tissue (4) ≥2 intraoperative cultures or combination of preoperative aspiration and intraoperative cultures yielding an indistinguishable organism c) [the growth of a virulent microorganism b) (e.g., Staphylococcus aureus) in a single specimen of a tissue biopsy or synovial fluid is also considered as indicative of a PJI] | Major: (1) A sinus tract communicating with the joint (2) Two positive periprosthetic cultures with phenotypically identical organisms c) Minor: (a) Elevated ESR (>30 mm/h) and CRP (>100 mg/L for acute infections; >10 mg/L for chronic infections) (b) Elevated synovial fluid WBC count (>10,000 cells/mL for acute infections; >3000 cells/mL for chronic infections) or ++ change on leukocyte esterase test strip (c) Elevated PMN% (>90% for acute infections; >80% for chronic infections) (d) Positive histological analysis of periprosthetic tissue (>5 neutrophils per high-power field in five high-power fields observed on periprosthetic tissue at ×400 magnification (e) A single positive culture | Major: (1) Sinus tract with evidence of communication to the joint or visualization of the prosthesis (2) Two positive growths of the same organism d) using standard culture methods Minor: (a) Elevated CRP (>100 mg/L for acute infections; >10 mg/L for chronic infections) or D-Dimer (unknown threshold for acute infection; >860 ug/L for chronic infection) (score 2) (b) Elevated ESR (no role for acute infections; >30 mm/h for chronic infections) (score 1) (c) Elevated synovial WBC count (>10,000 cells/mL for acute infections; >3000 cells/mL for chronic infections) OR Leukocyte Esterase (+ + for acute and chronic infections) OR Positive alpha-defensin (score 3) (d) Elevated synovial PMN% (>90% for acute infections; >70% for chronic infections) (score 2) (e) Single positive culture (score 2) (f) Positive histology (score 3) (g) Positive intraoperative purulence (score 3) |
| Annotations | “Metal-on-metal bearing implants can simulate pus (“pseudopus”).” | “The presence of PJI is possible even if the above criteria are not met; the clinician should use his/her clinical judgment to determine if this is the case after reviewing all the available preoperative and intraoperative information.” |
References
- Moore, A.J.; Blom, A.W.; Whitehouse, M.R.; Gooberman-Hill, R. Deep Prosthetic Joint Infection: A Qualitative Study of the Impact on Patients and Their Experiences of Revision Surgery. BMJ Open 2015, 5, e009495. [Google Scholar] [CrossRef] [Green Version]
- Cahill, J.; Shadbolt, B.; Scarvell, J.; Smith, P. Quality of Life after Infection in Total Joint Replacement. J. Orthop. Surg. 2008, 16, 58–65. [Google Scholar] [CrossRef]
- Cancienne, J.M.; Werner, B.C.; Bolarinwa, S.A.; Browne, J.A. Removal of an Infected Total Hip Arthroplasty: Risk Factors for Repeat Debridement, Long-Term Spacer Retention, and Mortality. J. Arthroplast. 2017, 32, 2519–2522. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.; Schmier, J.; Ong, K.L.; Zhao, K.; Parvizi, J. Infection Burden for Hip and Knee Arthroplasty in the United States. J. Arthroplast. 2008, 23, 984–991. [Google Scholar] [CrossRef]
- Klouche, S.; Sariali, E.; Mamoudy, P. Total Hip Arthroplasty Revision Due to Infection: A Cost Analysis Approach. Orthop. Traumatol. Surg. Res. 2010, 96, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Huotari, K.; Peltola, M.; Jämsen, E. The Incidence of Late Prosthetic Joint Infections: A Registry-Based Study of 112,708 Primary Hip and Knee Replacements. Acta Orthop. 2015, 86, 321–325. [Google Scholar] [CrossRef] [Green Version]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J.; Berry, D.; Parvizi, J. Prosthetic Joint Infection Risk after TKA in the Medicare Population. Clin. Orthop. 2010, 468, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Costerton, J.W. Biofilm Theory Can Guide the Treatment of Device-Related Orthopaedic Infections. Clin. Orthop. 2005, 437, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.L.; McLaren, A.C.; McLaren, S.G.; Johnson, J.W.; Smeltzer, M.S. Is Aseptic Loosening Truly Aseptic? Clin. Orthop. 2005, NA, 25–30. [Google Scholar] [CrossRef]
- Neut, D.; van Horn, J.R.; van Kooten, T.G.; van der Mei, H.C.; Busscher, H.J. Detection of Biomaterial-Associated Infections in Orthopaedic Joint Implants. Clin. Orthop. 2003, 413, 261–268. [Google Scholar] [CrossRef]
- Tunney, M.M.; Patrick, S.; Curran, M.D.; Ramage, G.; Hanna, D.; Nixon, J.R.; Gorman, S.P.; Davis, R.I.; Anderson, N. Detection of Prosthetic Hip Infection at Revision Arthroplasty by Immunofluorescence Microscopy and PCR Amplification of the Bacterial 16S RRNA Gene. J. Clin. Microbiol. 1999, 37, 3281–3290. [Google Scholar] [CrossRef] [Green Version]
- Claessens, J.; Roriz, M.; Merckx, R.; Baatsen, P.; Van Mellaert, L.; Van Eldere, J. Inefficacy of Vancomycin and Teicoplanin in Eradicating and Killing Staphylococcus epidermidis Biofilms in Vitro. Int. J. Antimicrob. Agents 2015, 45, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial Biofilms: A Common Cause of Persistent Infections. Sci. New Ser. 1999, 284, 1318–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fux, C.A.; Stoodley, P.; Hall-Stoodley, L.; Costerton, J.W. Bacterial Biofilms: A Diagnostic and Therapeutic Challenge. Expert Rev. Anti Infect. Ther. 2003, 1, 667–683. [Google Scholar] [CrossRef]
- Jung, J.; Schmid, N.V.; Kelm, J.; Schmitt, E.; Anagnostakos, K. Complications after Spacer Implantation in the Treatment of Hip Joint Infections. Int. J. Med. Sci. 2009, 265–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Struelens, B.; Claes, S.; Bellemans, J. Spacer-Related Problems in Two-Stage Revision Knee Arthroplasty. Acta Orthop. Belg. 2013, 79, 422–426. [Google Scholar] [PubMed]
- Kunutsor, S.K.; Whitehouse, M.R.; Lenguerrand, E.; Blom, A.W.; Beswick, A.D. INFORM Team Re-Infection Outcomes Following One- And Two-Stage Surgical Revision of Infected Knee Prosthesis: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0151537. [Google Scholar] [CrossRef] [Green Version]
- The Global Infection Orthopaedic Management Collaboration; Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Board, T.; Kay, P.; Wroblewski, B.M.; Zeller, V.; Chen, S.-Y.; Hsieh, P.-H.; et al. One- and Two-Stage Surgical Revision of Peri-Prosthetic Joint Infection of the Hip: A Pooled Individual Participant Data Analysis of 44 Cohort Studies. Eur. J. Epidemiol. 2018, 33, 933–946. [Google Scholar] [CrossRef] [Green Version]
- Beswick, A.D.; Elvers, K.T.; Smith, A.J.; Gooberman-Hill, R.; Lovering, A.; Blom, A.W. What Is the Evidence Base to Guide Surgical Treatment of Infected Hip Prostheses? Systematic Review of Longitudinal Studies in Unselected Patients. BMC Med. 2012, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Lange, J.; Troelsen, A.; Thomsen, R.W.; Søballe, K. Soballe Chronic Infections in Hip Arthroplasties: Comparing Risk of Reinfection Following One-Stage and Two-Stage Revision: A Systematic Review and Meta-Analysis. Clin. Epidemiol. 2012, 57. [Google Scholar] [CrossRef] [Green Version]
- George, D.A.; Logoluso, N.; Castellini, G.; Gianola, S.; Scarponi, S.; Haddad, F.S.; Drago, L.; Romano, C.L. Does Cemented or Cementless Single-Stage Exchange Arthroplasty of Chronic Periprosthetic Hip Infections Provide Similar Infection Rates to a Two-Stage? A Systematic Review. BMC Infect. Dis. 2016, 16, 553. [Google Scholar] [CrossRef] [Green Version]
- Leonard, H.A.C.; Liddle, A.D.; Burke, Ó.; Murray, D.W.; Pandit, H. Single- or Two-Stage Revision for Infected Total Hip Arthroplasty? A Systematic Review of the Literature. Clin. Orthop. 2014, 472, 1036–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, M.; Sukeik, M.; Zahar, A.; Nizam, I.; Haddad, F.S. One-Stage Exchange Arthroplasty for Periprosthetic Hip and Knee Joint Infections. Open Orthop. J. 2016, 10, 646–653. [Google Scholar] [CrossRef] [Green Version]
- Winkler, H. Rationale for One Stage Exchange of Infected Hip Replacement Using Uncemented Implants and Antibiotic Impregnated Bone Graft. Int. J. Med. Sci. 2009, 247–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, H.; Stoiber, A.; Kaudela, K.; Winter, F.; Menschik, F. One Stage Uncemented Revision of Infected Total Hip Replacement Using Cancellous Allograft Bone Impregnated with Antibiotics. J. Bone Jt. Surg. Br. 2008, 90-B, 1580–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebied, A.M.; Elseedy, A.I.; Gamal, O. Single-Stage Revision for Periprosthetic Hip Infection Using Antibiotic Loaded Impaction Graft. HIP Int. 2016, 26, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New Definition for Periprosthetic Joint Infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [Green Version]
- Renz, N.; Yermak, K.; Perka, C.; Trampuz, A. Alpha Defensin Lateral Flow Test for Diagnosis of Periprosthetic Joint Infection: Not a Screening but a Confirmatory Test. JBJS 2018, 100, 742–750. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of Americaa. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Jt. J. 2013, 95-B, 1450–1452. [Google Scholar] [CrossRef]
- Shohat, N.; Bauer, T.; Buttaro, M.; Budhiparama, N.; Cashman, J.; Della Valle, C.J.; Drago, L.; Gehrke, T.; Marcelino Gomes, L.S.; Goswami, K.; et al. Hip and Knee Section, What Is the Definition of a Periprosthetic Joint Infection (PJI) of the Knee and the Hip? Can the Same Criteria Be Used for Both Joints? Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S325–S327. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef] [PubMed]
- Little, J.P. Consistency of ASA Grading. Anaesthesia 1995, 50, 658–659. [Google Scholar] [PubMed]
- Winkler, H.; Haiden, P. Allograft Bone as Antibiotic Carrier. J. Bone Jt. Infect. 2017, 2, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Fages, J.; Marty, A.; Delga, C.; Condoret, J.S.; Combes, D.; Frayssinet, P. Use of Supercritical CO2 for Bone Delipidation. Biomaterials 1994, 15, 650–656. [Google Scholar] [CrossRef]
- Fages, J.; Poirier, B.; Barbier, Y.; Frayssinet, P.; Joffret, M.L.; Majewski, W.; Bonel, G.; Larzul, D. Viral Inactivation of Human Bone Tissue Using Supercritical Fluid Extraction. ASAIO J. Am. Soc. Artif. Intern. Organs 1992 1998, 44, 289–293. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Raja, S.; Haddad, F.S. Acetabular Impaction Bone Grafting in Total Hip Replacement. Bone Jt. J. 2013, 95-B, 98–102. [Google Scholar] [CrossRef] [Green Version]
- Winkler, H.; Janata, O.; Berger, C.; Wein, W.; Georgopoulos, A. In Vitro Release of Vancomycin and Tobramycin from Impregnated Human and Bovine Bone Grafts. J. Antimicrob. Chemother. 2000, 46, 423–428. [Google Scholar] [CrossRef]
- Cypher, T.J.; Grossman, J.P. Biological Principles of Bone Graft Healing. J. Foot Ankle Surg. 1996, 35, 413–417. [Google Scholar] [CrossRef]
- Dempsey, K.E.; Riggio, M.P.; Lennon, A.; Hannah, V.E.; Ramage, G.; Allan, D.; Bagg, J. Identification of Bacteria on the Surface of Clinically Infected and Non-Infected Prosthetic Hip Joints Removed during Revision Arthroplasties by 16S RRNA Gene Sequencing and by Microbiological Culture. Arthritis Res. Ther. 2007, 9, R46. [Google Scholar] [CrossRef] [Green Version]
- Castaneda, P.; McLaren, A.; Tavaziva, G.; Overstreet, D. Biofilm Antimicrobial Susceptibility Increases with Antimicrobial Exposure Time. Clin. Orthop. 2016, 474, 1659–1664. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Thomsen, T.R.; Winkler, H.; Xu, Y. Influence of Biofilm Growth Age, Media, Antibiotic Concentration and Exposure Time on Staphylococcus aureus and Pseudomonas aeruginosa Biofilm Removal in Vitro. BMC Microbiol. 2020, 20, 264. [Google Scholar] [CrossRef] [PubMed]
- Post, V.; Wahl, P.; Richards, R.G.; Moriarty, T.F. Vancomycin Displays Time-Dependent Eradication of Mature Staphylococcus aureus Biofilms: VANCOMYCIN-MEDIATED BIOFILM ERADICATION. J. Orthop. Res. 2017, 35, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Garazzino, S.; Aprato, A.; Baietto, L.; D’Avolio, A.; Maiello, A.; De Rosa, F.G.; Aloj, D.; Siccardi, M.; Biasibetti, A.; Massè, A.; et al. Glycopeptide Bone Penetration in Patients with Septic Pseudoarthrosis of the Tibia. Clin. Pharmacokinet. 2008, 47, 793–805. [Google Scholar] [CrossRef]
- Ampe, E.; Delaere, B.; Hecq, J.-D.; Tulkens, P.M.; Glupczynski, Y. Implementation of a Protocol for Administration of Vancomycin by Continuous Infusion: Pharmacokinetic, Pharmacodynamic and Toxicological Aspects. Int. J. Antimicrob. Agents 2013, 41, 439–446. [Google Scholar] [CrossRef]
- James, C.W.; Gurk-Turner, C. Recommendations for Monitoring Serum Vancomycin Concentrations. Bayl. Univ. Med. Cent. Proc. 2001, 14, 189–190. [Google Scholar] [CrossRef]
- Nelson, C.L.; Griffin, F.M.; Harrison, B.H.; Cooper, R.E. In Vitro Elution Characteristics of Commercially and Noncommercially Prepared Antibiotic PMMA Beads. Clin. Orthop. 1992, 284, 303–309. [Google Scholar] [CrossRef]
- Anagnostakos, K.; Kelm, J.; Regitz, T.; Schmitt, E.; Jung, W. In Vitro Evaluation of Antibiotic Release from and Bacteria Growth Inhibition by Antibiotic-Loaded Acrylic Bone Cement Spacers. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 72B, 373–378. [Google Scholar] [CrossRef]
- Holtom, P.D.; Warren, C.A.; Greene, N.W.; Bravos, P.D.; Ressler, R.L.; Shepherd, L.; McPherson, E.J.; Patzakis, M.J. Relation of Surface Area to in Vitro Elution Characteristics of Vancomycin-Impregnated Polymethylmethacrylate Spacers. Am. J. Orthop. 1998, 27, 207–210. [Google Scholar]
- Törholm, C.; Lidgren, L.; Lindberg, L.; Kahlmeter, G. Total Hip Joint Arthroplasty with Gentamicin-Impregnated Cement. A Clinical Study of Gentamicin Excretion Kinetics. Clin. Orthop. 1983, 181, 99–106. [Google Scholar] [CrossRef]
- Bunetel, L.; Segui, A.; Cormier, M.; Percheron, E.; Langlais, F. Release of Gentamicin from Acrylic Bone Cement. Clin. Pharmacokinet. 1989, 17, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Klekamp, J.; Dawson, J.M.; Haas, D.W.; DeBoer, D.; Christie, M. The Use of Vancomycin and Tobramycin in Acrylic Bone Cement. J. Arthroplast. 1999, 14, 339–346. [Google Scholar] [CrossRef]
- Neut, D.; van de Belt, H.; van Horn, J.; van der Mei, H.; Busscher, H. The Effect of Mixing on Gentamicin Release from Polymethylmethacrylate Bone Cements. Acta Orthop. Scand. 2003, 74, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Schurman, D.J.; Trindade, C.; Hirshman, H.P.; Moser, K.; Kajiyama, G.; Stevens, P. Antibiotic-Acrylic Bone Cement Composites. Studies of Gentamicin and Palacos. J. Bone Jt. Surg. Am. 1978, 60, 978–984. [Google Scholar] [CrossRef]
- Hsieh, P.-H.; Chang, Y.-H.; Chen, S.-H.; Ueng, S.W.N.; Shih, C.-H. High Concentration and Bioactivity of Vancomycin and Aztreonam Eluted from SimplexTM Cement Spacers in Two-Stage Revision of Infected Hip Implants: A Study of 46 Patients at an Average Follow-up of 107 Days. J. Orthop. Res. 2006, 24, 1615–1621. [Google Scholar] [CrossRef]
- Hsieh, P.-H.; Huang, K.-C.; Tai, C.-L. Liquid Gentamicin in Bone Cement Spacers: In Vivo Antibiotic Release and Systemic Safety in Two-Stage Revision of Infected Hip Arthroplasty. J. Trauma Inj. Infect. Crit. Care 2009, 66, 804–808. [Google Scholar] [CrossRef]
- Dunne, N.J.; Hill, J.; McAfee, P.; Kirkpatrick, R.; Patrick, S.; Tunney, M. Incorporation of Large Amounts of Gentamicin Sulphate into Acrylic Bone Cement: Effect on Handling and Mechanical Properties, Antibiotic Release, and Biofilm Formation. Proc. Inst. Mech. Eng. [H] 2008, 222, 355–365. [Google Scholar] [CrossRef]
- Dunne, N.; Hill, J.; Mcafee, P.; Todd, K.; Kirkpatrick, R.; Tunney, M.; Patrick, S. In Vitro Study of the Efficacy of Acrylic Bone Cement Loaded with Supplementary Amounts of Gentamicin: Effect on Mechanical Properties, Antibiotic Release, and Biofilm Formation. Acta Orthop. 2007, 78, 774–785. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-H.; Tai, C.-L.; Chen, S.-Y.; Chang, C.-H.; Chang, Y.-H.; Hsieh, P.-H. Elution and Mechanical Strength of Vancomycin-Loaded Bone Cement: In Vitro Study of the Influence of Brand Combination. PLoS ONE 2016, 11, e0166545. [Google Scholar] [CrossRef] [Green Version]
- Moran, J.M.; Seth, A.; Matejczyk, M.-B. Effect of Gentamicin on Shear and Interface Strengths of Bone Cement. Clin. Orthop. 1979, 141, 96–101. [Google Scholar] [CrossRef]
- Seldes, R.M.; Winiarsky, R.; Jordan, L.C.; Baldini, T.; Brause, B.; Zodda, F.; Sculco, T.P. Liquid Gentamicin in Bone Cement: A Laboratory Study of a Potentially More Cost-Effective Cement Spacer. J. Bone Jt. Surg. 2005, 87, 268–272. [Google Scholar] [CrossRef]
- Nelson, C.L.; Jones, R.B.; Wingert, N.C.; Foltzer, M.; Bowen, T.R. Sonication of Antibiotic Spacers Predicts Failure during Two-Stage Revision for Prosthetic Knee and Hip Infections. Clin. Orthop. 2014, 472, 2208–2214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neut, D. Biomaterial-Associated Infection of Gentamicin-Loaded PMMA Beads in Orthopaedic Revision Surgery. J. Antimicrob. Chemother. 2001, 47, 885–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bereza, P.; Ekiel, A.; Auguściak-Duma, A.; Aptekorz, M.; Wilk, I.; Kusz, D.; Wojciechowski, P.; Sieroń, A.L.; Martirosian, G. Comparison of Cultures and 16S RRNA Sequencing for Identification of Bacteria in Two-Stage Revision Arthroplasties: Preliminary Report. BMC Musculoskelet. Disord. 2016, 17, 138. [Google Scholar] [CrossRef] [Green Version]
- Buttaro, M.A.; Gimenez, M.I.; Greco, G.; Barcan, L.; Piccaluga, F. High Active Local Levels of Vancomycin without Nephrotoxicity Released from Impacted Bone Allografts in 20 Revision Hip Arthroplasties. Acta Orthop. 2005, 76, 336–340. [Google Scholar] [CrossRef]
- Edin, M.L.; Miclau, T.; Lester, G.E.; Lindsey, R.W.; Dahners, L.E. Effect of Cefazolin and Vancomycin on Osteoblasts in Vitro. Clin. Orthop. 1996, 245–251. [Google Scholar] [CrossRef]
- Winkler, H. Treatment of Chronic Orthopaedic Infection. EFORT Open Rev. 2017, 2, 110–116. [Google Scholar] [CrossRef]
- Pelt, C.E.; Grijalva, R.; Anderson, L.; Anderson, M.B.; Erickson, J.; Peters, C.L. Two-Stage Revision TKA Is Associated with High Complication and Failure Rates. Adv. Orthop. 2014, 2014, 659047. [Google Scholar] [CrossRef] [Green Version]
- Gomez, M.M.; Tan, T.L.; Manrique, J.; Deirmengian, G.K.; Parvizi, J. The Fate of Spacers in the Treatment of Periprosthetic Joint Infection. J. Bone Jt. Surg. 2015, 97, 1495–1502. [Google Scholar] [CrossRef] [Green Version]
- Blumenfeld, T.J. Does the Infection or the Treatment Kill the Patient?: Commentary on an Article by Benjamin Zmistowski, BS, et al.: “Periprosthetic Joint Infection Increases the Risk of One-Year Mortality”. J. Bone Jt. Surg. 2013, 95, e200. [Google Scholar] [CrossRef]
- Cierny, G.; Mader, J.T.; Penninck, J.J. The Classic: A Clinical Staging System for Adult Osteomyelitis. Clin. Orthop. 2003, 414, 7–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirakawa, K.; Stulberg, B.N.; Wilde, A.H.; Bauer, T.W.; Secic, M. Results of 2-Stage Reimplantation for Infected Total Knee Arthroplasty. J. Arthroplast. 1998, 13, 22–28. [Google Scholar] [CrossRef]
- Sabry, F.Y.; Buller, L.; Ahmed, S.; Klika, A.K.; Barsoum, W.K. Preoperative Prediction of Failure Following Two-Stage Revision for Knee Prosthetic Joint Infections. J. Arthroplast. 2014, 29, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Lange, J.; Troelsen, A.; Solgaard, S.; Otte, K.S.; Jensen, N.K.; Søballe, K.; Troelsen, A.; Zawadski, A.; Kjersgaard, A.G.; Heine, C.; et al. Cementless One-Stage Revision in Chronic Periprosthetic Hip Joint Infection. Ninety-One Percent Infection Free Survival in 56 Patients at Minimum 2-Year Follow-Up. J. Arthroplast. 2018, 33, 1160–1165.e1. [Google Scholar] [CrossRef] [PubMed]
- Haleem, A.A.; Berry, D.J.; Hanssen, A.D. The Chitranjan Ranawat Award: Mid-Term to Long-Term Followup of Two-Stage Reimplantation for Infected Total Knee Arthroplasty. Clin. Orthop. 2004, 428, 35–39. [Google Scholar] [CrossRef]
- Volin, S.J.; Hinrichs, S.H.; Garvin, K.L. Two-Stage Reimplantation of Total Joint Infections: A Comparison of Resistant and Non-Resistant Organisms. Clin. Orthop. 2004, 427, 94–100. [Google Scholar] [CrossRef]
- Mahmud, T.; Lyons, M.C.; Naudie, D.D.; MacDonald, S.J.; McCalden, R.W. Assessing the Gold Standard: A Review of 253 Two-Stage Revisions for Infected TKA. Clin. Orthop. 2012, 470, 2730–2736. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Sotelo, J.; Berry, D.J.; Hanssen, A.D.; Cabanela, M.E. Midterm to Long-Term Followup of Staged Reimplantation for Infected Hip Arthroplasty. Clin. Orthop. 2009, 467, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Kurd, M.F.; Ghanem, E.; Steinbrecher, J.; Parvizi, J. Two-Stage Exchange Knee Arthroplasty: Does Resistance of the Infecting Organism Influence the Outcome? Clin. Orthop. 2010, 468, 2060–2066. [Google Scholar] [CrossRef] [Green Version]
- Javad Mortazavi, S.M.; Vegari, D.; Ho, A.; Zmistowski, B.; Parvizi, J. Two-Stage Exchange Arthroplasty for Infected Total Knee Arthroplasty: Predictors of Failure. Clin. Orthop. 2011, 469, 3049–3054. [Google Scholar] [CrossRef] [Green Version]
- Berend, K.R.; Lombardi, A.V.; Morris, M.J.; Bergeson, A.G.; Adams, J.B.; Sneller, M.A. Two-Stage Treatment of Hip Periprosthetic Joint Infection Is Associated with a High Rate of Infection Control but High Mortality. Clin. Orthop. 2013, 471, 510–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, Y.; Fehring, T.K.; Hanssen, A.; Marculescu, C.; Odum, S.M.; Osmon, D. Two-Stage Reimplantation for Periprosthetic Knee Infection Involving Resistant Organisms. J. Bone Jt. Surg. 2007, 89, 1227–1231. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Hu, C.-C.; Chen, C.-C.; Chang, Y.-H.; Hsieh, P.-H. Two-Stage Revision Arthroplasty for Periprosthetic Hip Infection: Mean Follow-Up of Ten Years. BioMed Res. Int. 2015, 2015, 345475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoad-Reddick, D.A.; Evans, C.R.; Norman, P.; Stockley, I. Is There a Role for Extended Antibiotic Therapy in a Two-Stage Revision of the Infected Knee Arthroplasty? J. Bone Jt. Surg. Br. 2005, 87-B, 171–174. [Google Scholar] [CrossRef]
- Gooding, C.R.; Masri, B.A.; Duncan, C.P.; Greidanus, N.V.; Garbuz, D.S. Durable Infection Control and Function with the PROSTALAC Spacer in Two-Stage Revision for Infected Knee Arthroplasty. Clin. Orthop. 2011, 469, 985–993. [Google Scholar] [CrossRef] [Green Version]
- Kalore, N.V.; Maheshwari, A.; Sharma, A.; Cheng, E.; Gioe, T.J. Is There a Preferred Articulating Spacer Technique for Infected Knee Arthroplasty?: A Preliminary Study. Clin. Orthop. 2012, 470, 228–235. [Google Scholar] [CrossRef] [Green Version]
- Tan, T.L.; Goswami, K.; Fillingham, Y.A.; Shohat, N.; Rondon, A.J.; Parvizi, J. Defining Treatment Success after 2-Stage Exchange Arthroplasty for Periprosthetic Joint Infection. J. Arthroplast. 2018, 33, 3541–3546. [Google Scholar] [CrossRef]
- Huard, M.; Detrembleur, C.; Poilvache, H.; Pastor y Geels, I.; Van Cauter, M.; Driesen, R.; Yombi, J.-C.; Neyt, J.; Cornu, O. Alpha Defensin: A Diagnostic Accuracy Depending on the Infection Definition Used. J. Arthroplast. 2020, 35, 1355–1360. [Google Scholar] [CrossRef]
- Melendez, D.; Osmon, D.; Quaintance, K.E.G.; Hanssen, A.D.; Patel, R. 693Comparison of the 2011 Musculoskeletal Infection Society (MSIS), the 2013 International Consensus Meeting (ICM) and the Infectious Diseases Society of America (IDSA) Diagnostic Criteria for Prosthetic Joint Infection (PJI). Open Forum Infect. Dis. 2014, 1, S196. [Google Scholar] [CrossRef]
- Guan, H.; Fu, J.; Li, X.; Chai, W.; Hao, L.; Li, R.; Zhao, J.; Chen, J. The 2018 New Definition of Periprosthetic Joint Infection Improves the Diagnostic Efficiency in the Chinese Population. J. Orthop. Surg. 2019, 14, 151. [Google Scholar] [CrossRef]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success after Treatment of Periprosthetic Joint Infection: A Delphi-Based International Multidisciplinary Consensus. Clin. Orthop. 2013, 471, 2374–2382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krenn, V.; Morawietz, L.; Perino, G.; Kienapfel, H.; Ascherl, R.; Hassenpflug, G.J.; Thomsen, M.; Thomas, P.; Huber, M.; Kendoff, D.; et al. Revised Histopathological Consensus Classification of Joint Implant Related Pathology. Pathol.-Res. Pract. 2014, 210, 779–786. [Google Scholar] [CrossRef] [PubMed]



| Characteristics | Values |
|---|---|
| Preoperative | |
| Age (years) | 68.2 ± 12.3 (31.5–86.9) |
| Sex | |
| Male | 34 (48.6%) |
| Female | 36 (51.4%) |
| BMI (kg/m2) a) | 29.3 ± 6 (19.5–46.1) |
| ASA score ≥ 3 a) | 20 (52.6%) |
| History of surgery for PJI on respective joint | 35 (50%) |
| Previous surgeries on respective joint | 3.2 ± 2.8 (1–13) |
| ≥8 previous surgeries on respective joint | 7 (10%) |
| Sepsis as surgery indication | 4 (5.7%) |
| Sinus tract | 21 (30%) |
| Purulence | 37 (52.9%) |
| Intraoperative | |
| Surgery duration (minutes) a) | 187.8 ± 47.8 (114–305) |
| Surgery site | |
| Knee joint | 32 (45.7%) |
| Hip Joint | 38 (54.3%) |
| Spacer explantation | 3 (4.3%) |
| Osteosynthesis plate removal | 3 (4.3%) |
| Volume antibiotic-impregnated allograft bone (cm3) | 92.2 ± 27.8 (40–202) |
| Arthrodesis Implantation | 1 (1.4%) |
| Cementless prosthesis implantation | 49 (70%) |
| Application of intramedullary cement | 0 (0%) |
| Postoperative | |
| Hospital stay after surgery (days) | 16.8 days ± 8.7 (7–47) |
| Microorganisms | Monomicrobial Infections (n = 32), No. of Infected Patients | Polymicrobial Infections (n = 38), No. of Infected Patients |
|---|---|---|
| Fungus: | ||
| Candida albicans | 1 | |
| Gram-negative bacteria: | ||
| Pseudomonas aeruginosa | 2 | |
| Escherichia coli | 1 | |
| Klebsiella pneumoniae | 1 | |
| Proteus vulgaris | 1 | |
| Fusobacterium sp. | 1 | |
| Ralstonia picketti | 1 | |
| Gram-positive bacteria: | ||
| Micrococcus sp. | 4 | |
| Brevibacterium casei | 1 | |
| Propionibacterium sp. | 3 | 9 |
| Corynebacterium sp. | 5 | |
| Bacillus sp. | 2 | |
| Staphylococcus aureus | 1 | 6 |
| Staphylococcus epidermidis | 16 | 24 |
| Staphylococcus warneri | 3 | |
| Staphylococcus capitis | 1 | 3 |
| Staphylococcus hominis | 3 | |
| Staphylococcus lugdunensis | 1 | 1 |
| Staphylococcus caprae | 1 | |
| Staphylococcus haemolyticus | 1 | |
| “Mixed growth of Staphylococcus spp.” | 2 | |
| Coagulase-negative Staphylococcus sp., unspecified | 2 | 7 |
| Gemella morbillorum | 1 | |
| Streptococcus sp. | 3 | 6 |
| Enterococcus sp. | 1 | 5 |
| Aerococcus viridans | 1 | |
| Finegoldia magna | 2 | |
| Peptostreptococcus sp. | 2 | |
| Peptococcus sp. | 1 | |
| Anaerococcus prevotii | 1 | |
| unspecified Species | 2 | |
| Culture-negative | none | none |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dersch, G.; Winkler, H. Periprosthetic Joint Infection (PJI)—Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone—A Retrospective Cohort Study. Antibiotics 2022, 11, 310. https://doi.org/10.3390/antibiotics11030310
Dersch G, Winkler H. Periprosthetic Joint Infection (PJI)—Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone—A Retrospective Cohort Study. Antibiotics. 2022; 11(3):310. https://doi.org/10.3390/antibiotics11030310
Chicago/Turabian StyleDersch, Gregor, and Heinz Winkler. 2022. "Periprosthetic Joint Infection (PJI)—Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone—A Retrospective Cohort Study" Antibiotics 11, no. 3: 310. https://doi.org/10.3390/antibiotics11030310
APA StyleDersch, G., & Winkler, H. (2022). Periprosthetic Joint Infection (PJI)—Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone—A Retrospective Cohort Study. Antibiotics, 11(3), 310. https://doi.org/10.3390/antibiotics11030310