

Use of a Novel Anti-Infective Noble Metal Alloy-Coated Titanium Orthopedic Nail in Patients with Open Fractures: A Case Series from Malaysia
 ,
,
Abstract
1. Introduction
2. Results
2.1. Infections
2.2. Bony Union Assessment by the Treating Orthopedic Surgeons
2.3. Bony Union Assessment by the Independent Expert Panel
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hannigan, G.D.; Pulos, N.; Grice, E.A.; Mehta, S. Current concepts and ongoing research in the prevention and treatment of open fracture infections. Adv. Wound Care 2015, 4, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Lie, S.A.; Hallan, G.; Zirkle, L.G.; Engesæter, L.B.; Havelin, L.I. Risk factors for infection after 46,113 intramedullary nail operations in low- and middle-income countries. World J. Surg. 2013, 37, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M.; Cook, G.; Costerton, B.; Hanson, S.R.; Hensten-Pettersen, A.; Jacobsen, N.; Johnson, R.J.; Mitchell, R.N.; Pasmore, M.; Schoen, F.J.; et al. Host reactions to biomaterials and their evaluation. In Biomaterials Science, 2nd ed.; Ratner, B., Hoffman, A., Schoen, F., Lemons, J., Eds.; Academic Press: Cambridge, MA, USA, 2004; pp. 293–295. [Google Scholar]
- Tissingh, E.K.; Marais, L.; Loro, A.; Bose, D.; Ferguson, J.; Morgensten, M.; McNally, M. Management of fracture-related infection in low resource settings: How applicable are the current consensus guidelines? EFORT Open Rev. 2022, 7, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.S.; Galat, D.D.; Zirkle, L.G.; Shaw, M.K.; Galat, J.D. Risk factors for infection after intramedullary nailing of open tibial shaft fractures in low- and middle-income countries. J. Orthop. Trauma 2019, 33, e234–e239. [Google Scholar] [CrossRef]
- Haonga, B.T.; Liu, M.; Albright, P.; Challa, S.T.; Ali, S.H.; Lazar, A.A.; Eliezer, E.N.; Shearer, D.W.; Morshed, S. Intramedullary nailing versus external fixation in the treatment of open tibial fractures in Tanzania: Results of a randomized clinical trial. J. Bone Jt. Surg. Am. Vol. 2020, 102, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Osmon, D.R.; Hanssen, A.D.; Steckelberg, J.M.; Patel, R. Molecular and antibiofilm approaches to prosthetic joint infection. Clin. Orthop. Relat. Res. 2003, 414, 69–88. [Google Scholar] [CrossRef]
- Goodman, S.B.; Yao, Z.; Keeney, M.; Yang, F. The future of biologic coatings for orthopaedic implants. Biomaterials 2013, 34, 3174–3183. [Google Scholar] [CrossRef]
- Alexander, J.W. History of the medical use of silver. Surg. Infect. 2009, 10, 289–292. [Google Scholar] [CrossRef]
- Karchmer, T.B.; Giannetta, E.T.; Muto, C.A.; Strain, B.A.; Farr, B.M. A randomized crossover study of silver-coated urinary catheters in hospitalized patients. Arch. Intern. Med. 2000, 160, 3294–3298. [Google Scholar] [CrossRef]
- Stenzelius, K.; Persson, S.; Olsson, U.B.; Stjarneblad, M. Noble metal alloy-coated latex versus silicone Foley catheter in short-term catheterization: A randomized controlled study. Scand. J. Urol. Nephrol. 2011, 45, 258–264. [Google Scholar] [CrossRef]
- Lederer, J.W.; Jarvis, W.R.; Thomas, L.; Ritter, J. Multicenter cohort study to assess the impact of a silver-alloy and hydrogel-coated urinary catheter on symptomatic catheter-associated urinary tract infections. J. Wound Ostomy Cont. Nurs. 2014, 41, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo Fabrellas, I.; Rebollo Pavon, M.; Planas Canals, M.; Barbero Cabezas, M. Incidence of urinary tract infections after cardiac surgery: Comparative study accordind to catheterization device. Enferm. Intensiv. 2015, 26, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Aljohi, A.A.; Hassan, H.E.; Gupta, R.K. The efficacy of noble metal alloy urinary catheters in reducing catheter-associated urinary tract infection. Urol. Ann. 2016, 8, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.H.; Wong, C.W.; Lai, C.K.; Siu, H.K.; Tsang, D.N.; Yeung, K.Y.; Ip, D.K.; Tam, P.K. A prospective interventional study to examine the effect of a silver alloy and hydrogel-coated catheter on the incidence of catheter-associated urinary tract infection. Hong Kong Med. J. 2017, 23, 239–245. [Google Scholar] [CrossRef][Green Version]
- Magnusson, B.; Kai-Larsen, Y.; Granlund, P.; Seiger, A.; Lindbo, L.; Sanchez, J.; Johansson, D. Long-term use of noble metal alloy coated urinary catheters reduces recurrent CAUTI and decreases proinflammatory markers. Ther. Adv. Urol. 2019, 11, 1756287219854915. [Google Scholar] [CrossRef]
- Singh, R.; Hokenstad, E.D.; Wiest, S.R.; Kim-Fine, S.; Weaver, A.L.; McGree, M.E.; Klingele, C.J.; Trabuco, E.C.; Gebhart, J.B. Randomized controlled trial of silver-alloy-impregnated suprapubic catheters versus standard suprapubic catheters in assessing urinary tract infection rates in urogynecology patients. Int. Urogynecol. J. 2019, 30, 779–787. [Google Scholar] [CrossRef]
- Bjorling, G.; Johansson, D.; Bergstrom, L.; Jalal, S.; Kohn, I.; Frostell, C.; Kalman, S. Tolerability and performance of BIP endotracheal tubes with noble metal alloy coating—A randomized clinical evaluation study. BMC Anesthesiol. 2015, 15, 174. [Google Scholar] [CrossRef]
- Thorarinsdottir, H.R.; Kander, T.; Holmberg, A.; Petronis, S.; Klarin, B. Biofilm formation on three different endotracheal tubes: A prospective clinical trial. Crit. Care 2020, 24, 382. [Google Scholar] [CrossRef]
- Goldschmidt, H.; Hahn, U.; Salwender, H.J.; Haas, R.; Jansen, B.; Wolbring, P.; Rinck, M.; Hunstein, W. Prevention of catheter-related infections by silver coated central venous catheters in oncological patients. Zentralbl. Bakteriol. 1995, 283, 215–223. [Google Scholar] [CrossRef]
- Svensson, S.; Suska, F.; Emanuelsson, L.; Palmquist, A.; Norlindh, B.; Trobos, M.; Backros, H.; Persson, L.; Rydja, G.; Ohrlander, M.; et al. Osseointegration of titanium with an antimicrobial nanostructured noble metal coating. Nanomedicine 2013, 9, 1048–1056. [Google Scholar] [CrossRef]
- Suska, F.; Svensson, S.; Johansson, A.; Emanuelsson, L.; Karlholm, H.; Ohrlander, M.; Thomsen, P. In vivo evaluation of noble metal coatings. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 92, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Perisano, C.; Greco, T.; Polichetti, C.; Inverso, M.; Maccauro, G. Antibiotic-coated nail in open tibial fracture: A retrospective case series. J. Funct. Morphol. Kinesiol. 2021, 6, 97. [Google Scholar] [CrossRef]
- Li, B.; Webster, T.J. Bacteria antibiotic resistance: New challenges and opportunities for implant-associated orthopedic infections. J. Orthop. Res. 2018, 36, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Miclau, T.; Schmidt, A.H.; Wenke, J.C.; Webb, L.X.; Harro, J.M.; Prabhakara, R.; Shirtliff, M.E. Infection. J. Orthop. Trauma 2010, 24, 583–586. [Google Scholar] [CrossRef]
- Badia, J.M.; Casey, A.L.; Petrosillo, N.; Hudson, P.M.; Mitchell, S.A.; Crosby, C. Impact of surgical site infection on healthcare costs and patient outcomes: A systematic review in six European countries. J. Hosp. Infect. 2017, 96, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Mock, C.; Cherian, M.N. The global burden of musculoskeletal injuries: Challenges and solutions. Clin. Orthop. Relat. Res. 2008, 466, 2306–2316. [Google Scholar] [CrossRef]
- Hussmann, B.; Johann, I.; Kauther, M.D.; Landgraeber, S.; Jager, M.; Lendemans, S. Measurement of the silver ion concentration in wound fluids after implantation of silver-coated megaprostheses: Correlation with the clinical outcome. BioMed Res. Int. 2013, 2013, 763096. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.; Grimer, R.J.; Reddy, K.; Jeys, L.; Abudu, A.; Carter, S.R.; Tillman, R.M. Retrospective evaluation of the incidence of early periprosthetic infection with silver-treated endoprostheses in high-risk patients: Case-control study. Bone Jt. J. 2015, 97, 252–257. [Google Scholar] [CrossRef]
- Hardes, J.; Henrichs, M.P.; Hauschild, G.; Nottrott, M.; Guder, W.; Streitbuerger, A. Silver-coated megaprosthesis of the proximal tibia in patients with sarcoma. J. Arthroplast. 2017, 32, 2208–2213. [Google Scholar] [CrossRef]
- Bactigard. The Bactiguard Technology. Available online: https://www.bactiguard.com/about-bactiguard/the-bactiguard-technology/ (accessed on 27 April 2022).
- Huei, T.J.; Lip, H.T.C.; Hong, L.C.; Fang, C.Z.; Ann, C.S.; Rou, L.H.; Ganesen, G.; Jie, O.Y.; Sing, T.C.; Azlin, N.; et al. Predictors of mortality and outcomes of ventilated patients managed in a resource-limited acute surgical ward. World J. Surg. 2022, 46, 497–503. [Google Scholar] [CrossRef]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.E.; Koch, P.; Nazarian, S.; Schatzker, J. The Comprehensive Classification of Fractures of Long Bones, 1st ed.; Springer: Berlin/Heidelberg, Germany, 1990. [Google Scholar]



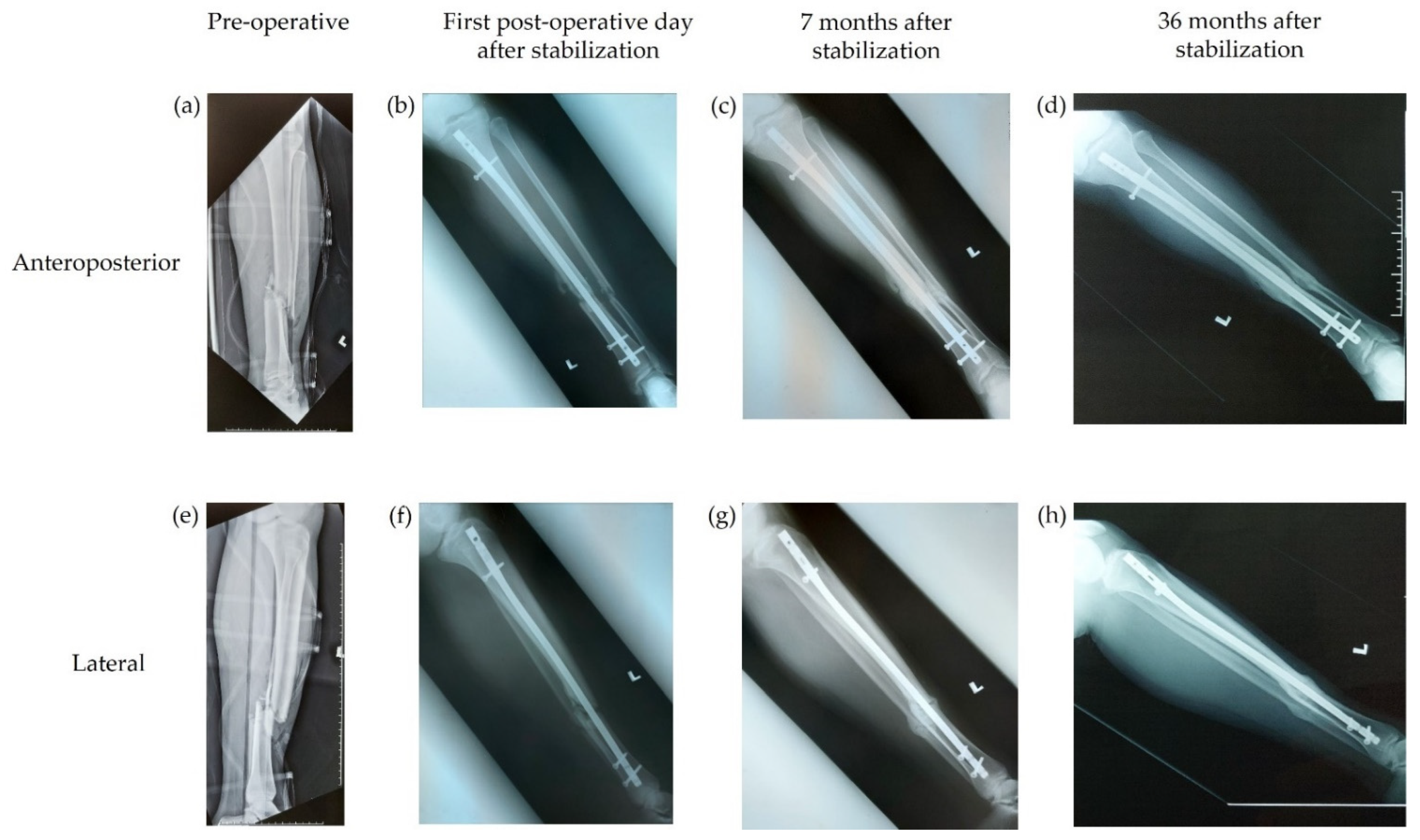{kind=link}
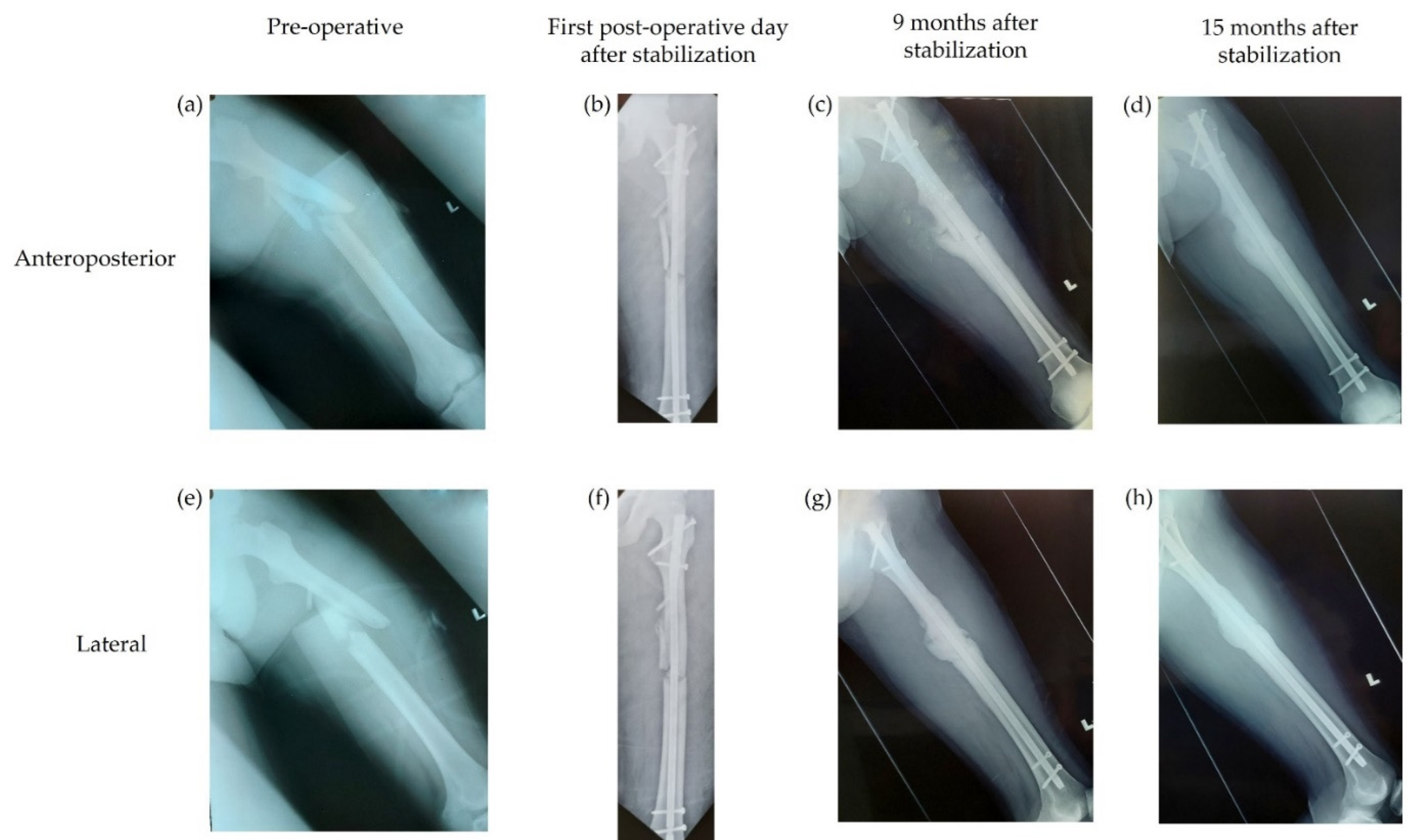{kind=link}
| Patients (N = 35) | |
|---|---|
| Sex, n (%) | |
| Male | 27 (77.1) |
| Female | 8 (22.9) |
| Age, mean (SD) | 33 (15) |
| Comorbidities, n (%) | |
| Diabetes mellitus | 1 (2.9) |
| Smoking | 1 (2.9) |
| Gustilo type of open fracture, n (%) | |
| Type IIIa | 29 (82.9) |
| Type IIIb | 6 (17.1) |
| AO fracture classification, n (%) | |
| 32 A3 | 1 (2.9) |
| 32 B2 | 3 (8.6) |
| 32 B3 | 3 (8.6) |
| 32 C2 | 2 (5.7) |
| 42 A1 | 2 (5.7) |
| 42 A3 | 4 (11.4) |
| 42 B2 | 11 (31.4) |
| 42 B3 | 3 (8.6) |
| 42 C2 | 3 (8.6) |
| Unavailable | 3 (8.6) |
| Site of fracture, n (%) | |
| Tibia | 26 (74.3) |
| Femur | 9 (25.7) |
| Patient | AO Fracture Classification | Gustilo Type | Underlying Medical Issues | Timing of Infection from Index Surgery | Timing of Union from Index Surgery | Fever | Sinus Location | Wound Dehiscence | Warm | Erythema | Isolated Microorganism | CRP, mg/L |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 42 B2 | IIIa | Nil | 4 months | 4 months | No | Distal screw | No | Yes | Yes | Staphylococcus aureus | 5.50 |
| 2 | 42 B3 | IIIa | Diabetes mellitus | 2 months | 8 months | No | Fracture site | No | Yes | Yes | Escherichia coli | 6.20 |
| 3 | 42 C2 | IIIb | Nil | 2 weeks | 1 year 4 months | No | No | Yes | Yes | Yes | S. aureus & Pseudomonas aeruginosa | 8.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karupiah, T.; Yong, A.P.; Ong, Z.W.; Tan, H.K.; Tang, W.C.; Salam, H.B. Use of a Novel Anti-Infective Noble Metal Alloy-Coated Titanium Orthopedic Nail in Patients with Open Fractures: A Case Series from Malaysia. Antibiotics 2022, 11, 1763. https://doi.org/10.3390/antibiotics11121763
Karupiah T, Yong AP, Ong ZW, Tan HK, Tang WC, Salam HB. Use of a Novel Anti-Infective Noble Metal Alloy-Coated Titanium Orthopedic Nail in Patients with Open Fractures: A Case Series from Malaysia. Antibiotics. 2022; 11(12):1763. https://doi.org/10.3390/antibiotics11121763
Chicago/Turabian StyleKarupiah, Thevarajan, Aik Peng Yong, Ze Wee Ong, Heng Keat Tan, Wei Chern Tang, and Hishamuddin Bin Salam. 2022. "Use of a Novel Anti-Infective Noble Metal Alloy-Coated Titanium Orthopedic Nail in Patients with Open Fractures: A Case Series from Malaysia" Antibiotics 11, no. 12: 1763. https://doi.org/10.3390/antibiotics11121763
APA StyleKarupiah, T., Yong, A. P., Ong, Z. W., Tan, H. K., Tang, W. C., & Salam, H. B. (2022). Use of a Novel Anti-Infective Noble Metal Alloy-Coated Titanium Orthopedic Nail in Patients with Open Fractures: A Case Series from Malaysia. Antibiotics, 11(12), 1763. https://doi.org/10.3390/antibiotics11121763