
Antibiotic Use and Stewardship Indicators in the First- and Second-Level Hospitals in Zambia: Findings and Implications for the Future

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Results
2.1. Frequency and Demographics of Patients Prescribed Antibiotics
2.2. Nature of Antibiotics Prescribed including Infections
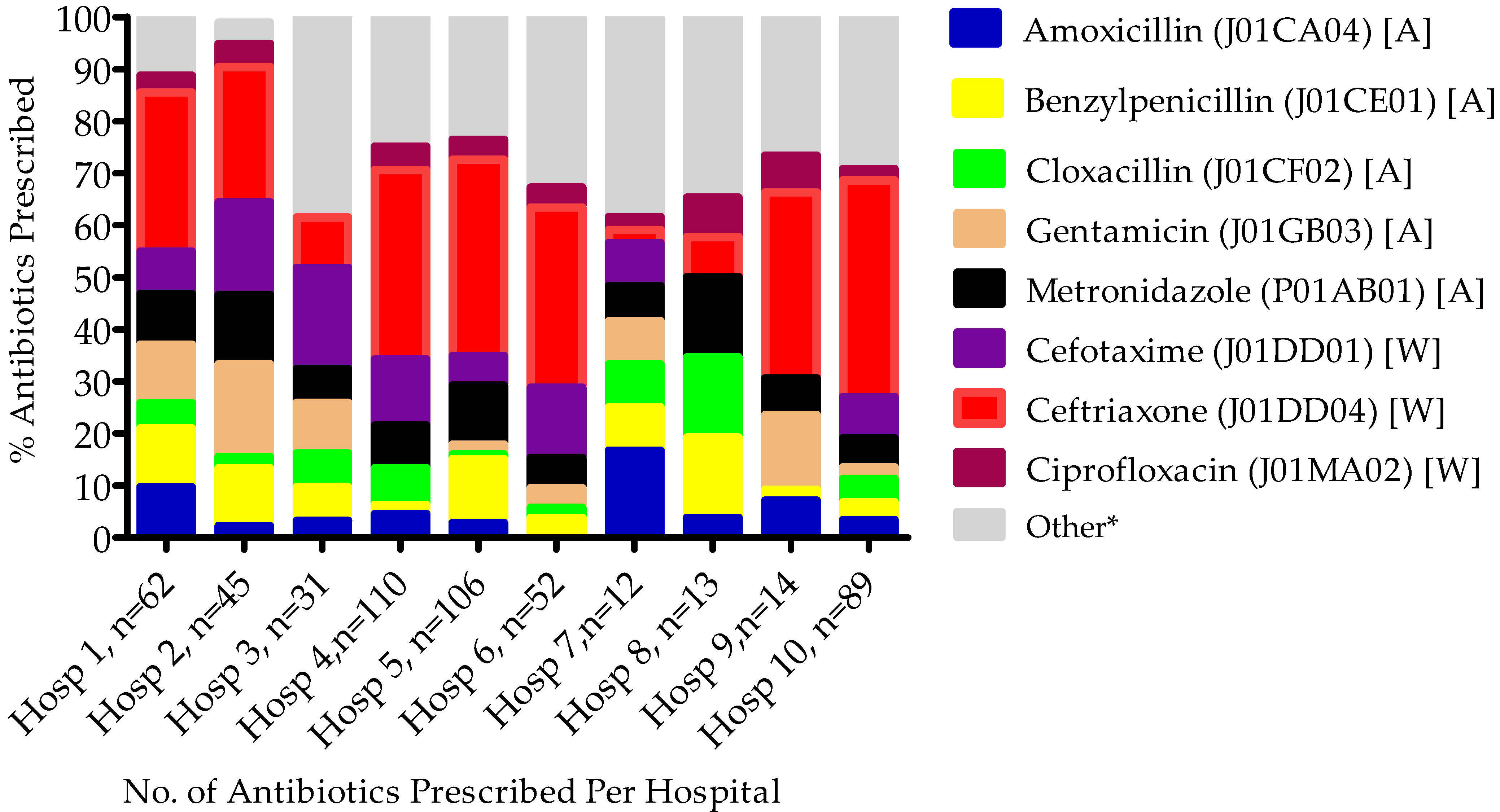
2.3. Commonly Prescribed Antibiotics among Surveyed Hospitals
2.4. Commonly Prescribed Antibiotics at the Ward Level among Surveyed Hospitals
2.5. Antibiotic Prescribing Broken down by Key Quality Indicators
3. Discussion
4. Materials and Methods
4.1. Study Design and Sites
4.2. Patient Inclusion and Exclusion Criteria
4.3. Data Collection and Analysis
4.4. Interpretation of Data Considering Antimicrobial Stewardship Programs
4.5. Ethical Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Stewart Williams, J.; Wall, S. The AMR emergency: Multi-sector collaboration and collective global policy action is needed now. Glob. Health Action 2019, 12, 1855831. [Google Scholar] [CrossRef]
- The World Bank. Final Report-Drug-Resistant Infections. A Threat to Our Economic Future March 2017. Available online: http://documents1.worldbank.org/curated/en/323311493396993758/pdf/final-report.pdf (accessed on 10 October 2022).
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef]
- Hofer, U. The cost of antimicrobial resistance. Nat. Rev. Microbiol. 2019, 17, 3. [Google Scholar] [PubMed]
- Interagency_Coordination_Group_on_Antimicrobial_Resistance. No Time to Wait: Securing the Future from Drug-Resistant Infections-Report to the Secretary-General of the United Nations 2019. Available online: https://cdn.who.int/media/docs/default-source/documents/no-time-to-wait-securing-the-future-from-drug-resistant-infections-en.pdf?sfvrsn=5b424d7_6&download=true (accessed on 14 November 2022).
- OECD_Health_Policy_Studies. Stemming the Superbug Tide 2018. Available online: https://www.oecd-ilibrary.org/sites/9789264307599-en/index.html?itemId=/content/publication/9789264307599-en&mimeType=text/html (accessed on 14 November 2022).
- World_Health_Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2021. Available online: https://www.who.int/publications/i/item/9789240027336 (accessed on 11 October 2022).
- World_Bank_Group. Pulling Together to Beat Superbugs Knowledge and Implementation Gaps in Addressing Antimicrobial Resistance 2019. Available online: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/430051570735014540/pulling-together-to-beat-superbugs-knowledge-and-implementation-gaps-in-addressing-antimicrobial-resistance (accessed on 14 November 2022).
- WHO. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 14 November 2022).
- Godman, B.; Egwuenu, A.; Wesangula, E.; Schellack, N.; Kalungia, A.C.; Tiroyakgosi, C.; Kgatlwane, J.; Mwita, J.C.; Patrick, O.; Niba, L.L.; et al. Tackling antimicrobial resistance across sub-Saharan Africa: Current challenges and implications for the future. Expert Opin. Drug Saf. 2022, 21, 1089–1111. [Google Scholar] [CrossRef] [PubMed]
- Government of the Republic of Zambia. Multi-Sectoral National Action Plan on Antimicrobial Resistance 2017–2027. Available online: https://www.afro.who.int/sites/default/files/2018-08/ZNPHI%20Document.pdf (accessed on 14 November 2022).
- D’Arcy, N.; Ashiru-Oredope, D.; Olaoye, O.; Afriyie, D.; Akello, Z.; Ankrah, D.; Asima, D.M.; Banda, D.C.; Barrett, S.; Brandish, C.; et al. Antibiotic Prescribing Patterns in Ghana, Uganda, Zambia and Tanzania Hospitals: Results from the Global Point Prevalence Survey (G-PPS) on Antimicrobial Use and Stewardship Interventions Implemented. Antibiotics 2021, 10, 1122. [Google Scholar] [CrossRef]
- Masich, A.M.; Vega, A.D.; Callahan, P.; Herbert, A.; Fwoloshi, S.; Zulu, P.M.; Chanda, D.; Chola, U.; Mulenga, L.; Hachaambwa, L.; et al. Antimicrobial usage at a large teaching hospital in Lusaka, Zambia. PLoS ONE 2020, 15, e0228555. [Google Scholar] [CrossRef] [PubMed]
- Kalungia, A.C.; Burger, J.; Godman, B.; Costa, J.O.; Simuwelu, C. Non-prescription sale and dispensing of antibiotics in community pharmacies in Zambia. Expert Rev. Anti-Infect. Ther. 2016, 14, 1215–1223. [Google Scholar] [CrossRef]
- Mudenda, S.; Mukosha, M.; Godman, B.; Fadare, J.; Malama, S.; Munyeme, M.; Hikaambo, C.N.A.; Kalungia, A.C.; Hamachila, A.; Kainga, H.; et al. Knowledge, Attitudes, and Practices of Community Pharmacy Professionals on Poultry Antibiotic Dispensing, Use, and Bacterial Antimicrobial Resistance in Zambia: Implications on Antibiotic Stewardship and WHO AWaRe Classification of Antibiotics. Antibiotics 2022, 11, 1210. [Google Scholar] [CrossRef]
- Ziko, L.M.; Hoffman, T.W.; Fwoloshi, S.; Chanda, D.; Nampungwe, Y.M.; Patel, D.; Bobat, H.; Moonga, A.; Chirwa, L.; Hachaambwa, L.; et al. Aetiology and prognosis of community-acquired pneumonia at the Adult University Teaching Hospital in Zambia. PLoS ONE 2022, 17, e0271449. [Google Scholar] [CrossRef]
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Koraqi, A.; et al. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: Results of an internet-based global point prevalence survey. Lancet Glob. Health 2018, 6, e619–e629. [Google Scholar] [CrossRef]
- Labi, A.K.; Obeng-Nkrumah, N.; Dayie, N.T.; Egyir, B.; Sampane-Donkor, E.; Newman, M.J.; Opintan, J.A. Antimicrobial use in hospitalized patients: A multicentre point prevalence survey across seven hospitals in Ghana. JAC-Antimicrob. Resist. 2021, 3, dlab087. [Google Scholar] [CrossRef]
- Saleem, Z.; Hassali, M.A.; Godman, B.; Versporten, A.; Hashmi, F.K.; Saeed, H.; Saleem, F.; Salman, M.; Rehman, I.U.; Khan, T.M. Point prevalence surveys of antimicrobial use: A systematic review and the implications. Expert Rev. Anti-Infect. Ther. 2020, 18, 897–910. [Google Scholar] [CrossRef] [PubMed]
- Kiggundu, R.; Wittenauer, R.; Waswa, J.P.; Nakambale, H.N.; Kitutu, F.E.; Murungi, M.; Okuna, N.; Morries, S.; Lawry, L.L.; Joshi, M.P.; et al. Point Prevalence Survey of Antibiotic Use across 13 Hospitals in Uganda. Antibiotics 2022, 11, 199. [Google Scholar] [CrossRef]
- Abubakar, U. Antibiotic use among hospitalized patients in northern Nigeria: A multicenter point-prevalence survey. BMC Infect Dis 2020, 20, 86. [Google Scholar] [CrossRef]
- Cox, J.A.; Vlieghe, E.; Mendelson, M.; Wertheim, H.; Ndegwa, L.; Villegas, M.V.; Gould, I.; Hara, G.L. Antibiotic stewardship in low- and middle-income countries: The same but different? Clin. Microbiol. Infect. 2017, 23, 812–818. [Google Scholar] [CrossRef]
- Kalungia, A.C.; Mwambula, H.; Munkombwe, D.; Marshall, S.; Schellack, N.; May, C.; Jones, A.S.C.; Godman, B. Antimicrobial stewardship knowledge and perception among physicians and pharmacists at leading tertiary teaching hospitals in Zambia: Implications for future policy and practice. J. Chemother. 2019, 31, 378–387. [Google Scholar] [CrossRef]
- Hall, J.W.; Bouchard, J.; Bookstaver, P.B.; Haldeman, M.S.; Kishimbo, P.; Mbwanji, G.; Mwakyula, I.; Mwasomola, D.; Seddon, M.; Shaffer, M.; et al. The Mbeya Antimicrobial Stewardship Team: Implementing Antimicrobial Stewardship at a Zonal-Level Hospital in Southern Tanzania. Pharmacy 2020, 8, 107. [Google Scholar] [CrossRef] [PubMed]
- Akpan, M.R.; Isemin, N.U.; Udoh, A.E.; Ashiru-Oredope, D. Implementation of antimicrobial stewardship programmes in African countries: A systematic literature review. J. Glob. Antimicrob. Resist. 2020, 22, 317–324. [Google Scholar] [CrossRef]
- van den Bergh, D.; Messina, A.P.; Goff, D.A.; van Jaarsveld, A.; Coetzee, R.; de Wet, Y.; Bronkhorst, E.; Brink, A.; Mendelson, M.; Richards, G.A.; et al. A pharmacist-led prospective antibiotic stewardship intervention improves compliance to community-acquired pneumonia guidelines in 39 public and private hospitals across South Africa. Int. J. Antimicrob. Agents 2020, 56, 106189. [Google Scholar] [CrossRef]
- Brink, A.J.; Messina, A.P.; Feldman, C.; Richards, G.A.; Becker, P.J.; Goff, D.A.; Bauer, K.A.; Nathwani, D.; Van den Bergh, D.; Alliance, N.A.S.S. Antimicrobial stewardship across 47 South African hospitals: An implementation study. Lancet Infect. Dis. 2016, 16, 1017–1025. [Google Scholar] [CrossRef]
- Siachalinga, L.; Mufwambi, W.; Lee, I.H. Impact of antimicrobial stewardship interventions to improve antibiotic prescribing for hospital inpatients in Africa: A systematic review and meta-analysis. J Hosp. Infect. 2022. [Google Scholar] [CrossRef]
- Lester, R.; Haigh, K.; Wood, A.; MacPherson, E.E.; Maheswaran, H.; Bogue, P.; Hanger, S.; Kalizang’oma, A.; Srirathan, V.; Kulapani, D.; et al. Sustained Reduction in Third-generation Cephalosporin Usage in Adult Inpatients Following Introduction of an Antimicrobial Stewardship Program in a Large, Urban Hospital in Malawi. Clin. Infect. Dis. 2020, 71, e478–e486. [Google Scholar] [PubMed]
- Mwita, J.C.; Ogunleye, O.O.; Olalekan, A.; Kalungia, A.C.; Kurdi, A.; Saleem, Z.; Sneddon, J.; Godman, B. Key Issues Surrounding Appropriate Antibiotic Use for Prevention of Surgical Site Infections in Low- and Middle-Income Countries: A Narrative Review and the Implications. Int. J. Gen. Med. 2021, 14, 515–530. [Google Scholar] [CrossRef]
- Boyles, T.H.; Naicker, V.; Rawoot, N.; Raubenheimer, P.J.; Eick, B.; Mendelson, M. Sustained reduction in antibiotic consumption in a South African public sector hospital; Four year outcomes from the Groote Schuur Hospital antibiotic stewardship program. S. Afr. Med. J. 2017, 107, 115–118. [Google Scholar] [CrossRef]
- Allegranzi, B.; Aiken, A.M.; Kubilay, N.Z.; Nthumba, P.; Barasa, J.; Okumu, G.; Mugarura, R.; Elobu, A.; Jombwe, J.; Maimbo, M.; et al. A multimodal infection control and patient safety intervention to reduce surgical site infections in Africa: A multicentre, before-after, cohort study. Lancet Infect. Dis. 2018, 18, 507–515. [Google Scholar] [CrossRef]
- Sharland, M.; Gandra, S.; Huttner, B.; Moja, L.; Pulcini, C.; Zeng, M.; Mendelson, M.; Cappello, B.; Cooke, G.; Magrini, N.; et al. Encouraging AWaRe-ness and discouraging inappropriate antibiotic use-the new 2019 Essential Medicines List becomes a global antibiotic stewardship tool. Lancet Infect. Dis. 2019, 19, 1278–1280. [Google Scholar] [CrossRef]
- Hsia, Y.; Lee, B.R.; Versporten, A.; Yang, Y.; Bielicki, J.; Jackson, C.; Newland, J.; Goossens, H.; Magrini, N.; Sharland, M.; et al. Use of the WHO Access, Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): An analysis of paediatric survey data from 56 countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [CrossRef]
- Pauwels, I.; Versporten, A.; Drapier, N.; Vlieghe, E.; Goossens, H. Hospital antibiotic prescribing patterns in adult patients according to the WHO Access, Watch and Reserve classification (AWaRe): Results from a worldwide point prevalence survey in 69 countries. J. Antimicrob. Chemother. 2021, 76, 1614–1624. [Google Scholar]
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K.; Sharland, M.; Gandra, S.; Pulcini, C.; Laxminarayan, R. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–2015: An analysis of pharmaceutical sales data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Ramzan, K.; Shafiq, S.; Raees, I.; Mustafa, Z.U.; Salman, M.; Khan, A.H.; Meyer, J.C.; Godman, B. Co-Infections, Secondary Infections, and Antimicrobial Use in Patients Hospitalized with COVID-19 during the First Five Waves of the Pandemic in Pakistan; Findings and Implications. Antibiotics 2022, 11, 789. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Methodology for Point Prevalence Survey on Antibiotic Use in Hospitals. Version 1.1. 2018. Available online: https://www.who.int/publications/i/item/WHO-EMP-IAU-2018.01 (accessed on 10 October 2022).
- Skosana, P.P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J.C. A national, multicentre, web-based point prevalence survey of antimicrobial use and quality indices among hospitalised paediatric patients across South Africa. J. Glob. Antimicrob. Resist. 2022, 29, 542–550. [Google Scholar] [CrossRef]
- Dlamini, N.N.; Meyer, J.C.; Kruger, D.; Kurdi, A.; Godman, B.; Schellack, N. Feasibility of using point prevalence surveys to assess antimicrobial utilisation in public hospitals in South Africa: A pilot study and implications. Hosp. Pract. 2019, 47, 88–95. [Google Scholar] [CrossRef]
- Afriyie, D.K.; Sefah, I.A.; Sneddon, J.; Malcolm, W.; McKinney, R.; Cooper, L.; Kurdi, A.; Godman, B.; Seaton, R.A. Antimicrobial point prevalence surveys in two Ghanaian hospitals: Opportunities for antimicrobial stewardship. JAC-Antimicrob. Resist. 2020, 2, dlaa001. [Google Scholar] [CrossRef] [PubMed]
- Amponsah, O.K.O.; Buabeng, K.O.; Owusu-Ofori, A.; Ayisi-Boateng, N.K.; Hämeen-Anttila, K.; Enlund, H. Point prevalence survey of antibiotic consumption across three hospitals in Ghana. JAC-Antimicrob. Resist. 2021, 3, dlab008. [Google Scholar] [CrossRef]
- Dodoo, C.C.; Orman, E.; Alalbila, T.; Mensah, A.; Jato, J.; Mfoafo, K.A.; Folitse, I.; Hutton-Nyameaye, A.; Okon Ben, I.; Mensah-Kane, P.; et al. Antimicrobial Prescription Pattern in Ho Teaching Hospital, Ghana: Seasonal Determination Using a Point Prevalence Survey. Antibiotics 2021, 10, 199. [Google Scholar] [CrossRef]
- Okoth, C.; Opanga, S.; Okalebo, F.; Oluka, M.; Baker Kurdi, A.; Godman, B. Point prevalence survey of antibiotic use and resistance at a referral hospital in Kenya: Findings and implications. Hosp. Pract. 2018, 46, 128–136. [Google Scholar] [CrossRef]
- Momanyi, L.; Opanga, S.; Nyamu, D.; Oluka, M.; Kurdi, A.; Godman, B. Antibiotic Prescribing Patterns at a Leading Referral Hospital in Kenya: A Point Prevalence Survey. J. Res. Pharm. Pract. 2019, 8, 149–154. [Google Scholar] [PubMed]
- Omulo, S.; Oluka, M.; Ombajo, L.; Osoro, E.; Kinuthia, R.; Guantai, A.; Ndegwa, L.; Verani, J.; Opanga, S.; Wesangula, E.; et al. Point-Prevalence Surveys of Antibiotic Use at Three Large Public Hospitals in Kenya. Infect. Control. Hosp. Epidemiol. 2020, 41, s353–s354. [Google Scholar] [CrossRef]
- Seni, J.; Mapunjo, S.G.; Wittenauer, R.; Valimba, R.; Stergachis, A.; Werth, B.J.; Saitoti, S.; Mhadu, N.H.; Lusaya, E.; Konduri, N. Antimicrobial use across six referral hospitals in Tanzania: A point prevalence survey. BMJ Open 2020, 10, e042819. [Google Scholar] [CrossRef]
- Anand Paramadhas, B.D.; Tiroyakgosi, C.; Mpinda-Joseph, P.; Morokotso, M.; Matome, M.; Sinkala, F.; Gaolebe, M.; Malone, B.; Molosiwa, E.; Shanmugam, M.G.; et al. Point prevalence study of antimicrobial use among hospitals across Botswana; findings and implications. Expert Rev. Anti-Infect. Ther. 2019, 17, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Gwebu, P.C.; Meyer, J.C.; Schellack, N.; Matsebula-Myeni, Z.C.; Godman, B. A web-based point prevalence survey of antimicrobial use and quality indicators at Raleigh Fitkin Memorial Hospital in the Kingdom of Eswatini and the implications. Hosp. Pract. 2022, 50, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Ogunleye, O.O.; Oyawole, M.R.; Odunuga, P.T.; Kalejaye, F.; Yinka-Ogunleye, A.F.; Olalekan, A.; Ogundele, S.O.; Ebruke, B.E.; Kalada Richard, A.; Anand Paramadhas, B.D.; et al. A multicentre point prevalence study of antibiotics utilization in hospitalized patients in an urban secondary and a tertiary healthcare facilities in Nigeria: Findings and implications. Expert Rev. Anti-Infect. Ther. 2022, 20, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Aboderin, A.O.; Adeyemo, A.T.; Olayinka, A.A.; Oginni, A.S.; Adeyemo, A.T.; Oni, A.A.; Olabisi, O.F.; Fayomi, O.D.; Anuforo, A.C.; Egwuenu, A.; et al. Antimicrobial use among hospitalized patients: A multi-center, point prevalence survey across public healthcare facilities, Osun State, Nigeria. Germs 2021, 11, 523–535. [Google Scholar] [CrossRef] [PubMed]
- Moolla, M.S.; Whitelaw, A.; Decloedt, E.H.; Koegelenberg, C.F.N.; Parker, A. Opportunities to enhance antibiotic stewardship: Colistin use and outcomes in a low-resource setting. JAC-Antimicrob. Resist. 2021, 3, dlab169. [Google Scholar] [CrossRef]
- Skosana, P.P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J.C. A point prevalence survey of antimicrobial utilisation patterns and quality indices amongst hospitals in South Africa; findings and implications. Expert Rev. Anti-Infect. Ther. 2021, 19, 1353–1366. [Google Scholar] [CrossRef]
- Antimicrobial Resistance (AMR)—A Growing Global Health Threat [Press Release]. Zambia National Public Health Institute: The Health Press. January 2017. Available online: http://znphi.co.zm/thehealthpress/antimicrobial-resistance-amr-a-growing-global-health-threat (accessed on 10 October 2022).
- Skosana, P.P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J.C. A national, multicentre web-based point prevalence survey of antimicrobial use in community healthcare centres across South Africa and the implications. Hosp. Pract. 2022, 50, 306–317. [Google Scholar] [CrossRef]
- Engler, D.; Meyer, J.C.; Schellack, N.; Kurdi, A.; Godman, B. Antimicrobial Stewardship Activities in Public Healthcare Facilities in South Africa: A Baseline for Future Direction. Antibiotics 2021, 10, 996. [Google Scholar] [CrossRef]
- Ankrah, D.; Owusu, H.; Aggor, A.; Osei, A.; Ampomah, A.; Harrison, M.; Nelson, F.; Aboagye, G.O.; Ekpale, P.; Laryea, J.; et al. Point Prevalence Survey of Antimicrobial Utilization in Ghana’s Premier Hospital: Implications for Antimicrobial Stewardship. Antibiotics 2021, 10, 1528. [Google Scholar] [CrossRef]
- Haldeman, M.S.; Kishimbo, P.; Seddon, M.; Sangare, A.; Mwasomola, D.; Hall, J.; Shaffer, M.; Leclair, R.; Caulder, C.; Bookstaver, P.B.; et al. Evaluation of Antimicrobial Utilization and Concordance with National Guidelines at a Tertiary Hospital in the Southern Highlands Zone of Tanzania. Am. J. Trop. Med. Hyg. 2020, 102, 370–376. [Google Scholar] [CrossRef]
- Olaru, I.D.; Meierkord, A.; Godman, B.; Ngwenya, C.; Fitzgerald, F.; Dondo, V.; Ferrand, R.A.; Kranzer, K. Assessment of antimicrobial use and prescribing practices among pediatric inpatients in Zimbabwe. J. Chemother. 2020, 32, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Niaz, Q.; Godman, B.; Campbell, S.; Kibuule, D. Compliance to prescribing guidelines among public health care facilities in Namibia; findings and implications. Int. J. Clin. Pharm. 2020, 42, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.M.; Meyer, J.; Godman, B. Why Compliance to National Prescribing Guidelines is Important Especially across Sub-Saharan Africa and Suggestions for the Future. J. Biomed. Pharm. Sci. 2021, 4, 1–7. [Google Scholar]
- Md Rezal, R.S.; Hassali, M.A.; Alrasheedy, A.A.; Saleem, F.; Md Yusof, F.A.; Godman, B. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: A systematic review of the literature. Expert Rev. Anti-Infect. Ther. 2015, 13, 665–680. [Google Scholar] [CrossRef] [PubMed]
- Saleem, Z.; Hassali, M.A.; Godman, B.; Hashmi, F.K.; Saleem, F. A multicenter point prevalence survey of healthcare-associated infections in Pakistan: Findings and implications. Am. J. Infect. Control 2019, 47, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Jeon, K.; Jeong, S.; Lee, N.; Park, M.J.; Song, W.; Kim, H.S.; Kim, H.S.; Kim, J.S. Impact of COVID-19 on Antimicrobial Consumption and Spread of Multidrug-Resistance in Bacterial Infections. Antibiotics 2022, 11, 535. [Google Scholar]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.P.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef]
- Alshaikh, F.S.; Godman, B.; Sindi, O.N.; Seaton, R.A.; Kurdi, A. Prevalence of bacterial coinfection and patterns of antibiotics prescribing in patients with COVID-19: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0272375. [Google Scholar]
- Republic of Zambia Ministry of Health. Zambia Standard Treatment Guideline. Available online: https://www.moh.gov.zm/wp-content/uploads/filebase/guidelines/Standard-Treatment-Guidelines-2020_2.pdf (accessed on 8 October 2022).
- Matsitse, T.B.; Helberg, E.; Meyer, J.C.; Godman, B.; Massele, A.; Schellack, N. Compliance with the primary health care treatment guidelines and the essential medicines list in the management of sexually transmitted infections in correctional centres in South Africa: Findings and implications. Expert Rev. Anti-Infect. Ther. 2017, 15, 963–972. [Google Scholar] [CrossRef]
- Sefah, I.A.; Essah, D.O.; Kurdi, A.; Sneddon, J.; Alalbila, T.M.; Kordorwu, H.; Godman, B. Assessment of adherence to pneumonia guidelines and its determinants in an ambulatory care clinic in Ghana: Findings and implications for the future. JAC-Antimicrob. Resist. 2021, 3, dlab080. [Google Scholar]
- Ntumba, P.; Mwangi, C.; Barasa, J.; Aiken, A.; Kubilay, Z.; Allegranzi, B. Multimodal approach for surgical site infection prevention–results from a pilot site in Kenya. Antimicrob. Resist. Infect. Control. 2015, 4, P87. [Google Scholar] [CrossRef]
- Abubakar, U.; Syed Sulaiman, S.A.; Adesiyun, A.G. Impact of pharmacist-led antibiotic stewardship interventions on compliance with surgical antibiotic prophylaxis in obstetric and gynecologic surgeries in Nigeria. PLoS ONE 2019, 14, e0213395. [Google Scholar] [CrossRef] [PubMed]
- Ofori-Asenso, R.; Brhlikova, P.; Pollock, A.M. Prescribing indicators at primary health care centers within the WHO African region: A systematic analysis (1995–2015). BMC Public Health 2016, 16, 724. [Google Scholar] [CrossRef] [PubMed]
- Niaz, Q.; Godman, B.; Massele, A.; Campbell, S.; Kurdi, A.; Kagoya, H.R.; Kibuule, D. Validity of World Health Organisation prescribing indicators in Namibia’s primary healthcare: Findings and implications. Int. J. Qual. Health Care 2019, 31, 338–345. [Google Scholar] [PubMed]
- Fadare, J.O.; Adeoti, A.O.; Desalu, O.O.; Enwere, O.O.; Makusidi, A.M.; Ogunleye, O.; Sunmonu, T.A.; Truter, I.; Akunne, O.O.; Godman, B. The prescribing of generic medicines in Nigeria: Knowledge, perceptions and attitudes of physicians. Expert Rev. Pharm. Outcomes Res. 2016, 16, 639–650. [Google Scholar] [CrossRef]
- Cameron, A.; Mantel-Teeuwisse, A.K.; Leufkens, H.G.; Laing, R.O. Switching from originator brand medicines to generic equivalents in selected developing countries: How much could be saved? Value Health 2012, 15, 664–673. [Google Scholar]
- Godman, B.; Fadare, J.; Kwon, H.Y.; Dias, C.Z.; Kurdi, A.; Dias Godói, I.P.; Kibuule, D.; Hoxha, I.; Opanga, S.; Saleem, Z.; et al. Evidence-based public policy making for medicines across countries: Findings and implications for the future. J. Comp. Eff. Res. 2021, 10, 1019–1052. [Google Scholar]
- World_Health_Organization. The Anatomical Therapeutic Chemical Classification System with Defined Daily Doses-ATC/DDD: WHO Collaborating Centre for Drug Statistics Methodology. 2015. Available online: http://www.whocc.no/atc_ddd_index/ (accessed on 2 October 2022).
- Godman, B.; Egwuenu, A.; Haque, M.; Malande, O.O.; Schellack, N.; Kumar, S.; Saleem, Z.; Sneddon, J.; Hoxha, I.; Islam, S.; et al. Strategies to Improve Antimicrobial Utilization with a Special Focus on Developing Countries. Life 2021, 11, 528. [Google Scholar] [CrossRef] [PubMed]
- Godman, B.; Haque, M.; McKimm, J.; Abu Bakar, M.; Sneddon, J.; Wale, J.; Campbell, S.; Martin, A.P.; Hoxha, I.; Abilova, V.; et al. Ongoing strategies to improve the management of upper respiratory tract infections and reduce inappropriate antibiotic use particularly among lower and middle-income countries: Findings and implications for the future. Curr. Med. Res. Opin. 2020, 36, 301–327. [Google Scholar] [CrossRef]
- Godman, B.; McCabe, H.; DLeong, T.; Mueller, D.; Martin, A.P.; Hoxha, I.; Mwita, J.C.; Rwegerera, G.M.; Massele, A.; Costa, J.D.O.; et al. Fixed dose drug combinations-are they pharmacoeconomically sound? Findings and implications especially for lower- and middle-income countries. Expert Rev. Pharm. Outcomes Res. 2020, 20, 1–26. [Google Scholar] [CrossRef]
- Godman, B.; Basu, D.; Pillay, Y.; Mwita, J.C.; Rwegerera, G.M.; Anand Paramadhas, B.D.; Tiroyakgosi, C.; Okwen, P.M.; Niba, L.L.; Nonvignon, J.; et al. Review of Ongoing Activities and Challenges to Improve the Care of Patients With Type 2 Diabetes Across Africa and the Implications for the Future. Front. Pharmacol. 2020, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Godman, B.; Basu, D.; Pillay, Y.; Almeida, P.H.; Mwita, J.C.; Rwegerera, G.M.; Anand Paramadhas, B.D.; Tiroyakgosi, C.; Patrick, O.; Niba, L.L.; et al. Ongoing and planned activities to improve the management of patients with Type 1 diabetes across Africa; implications for the future. Hosp. Pract. 2020, 48, 51–67. [Google Scholar] [CrossRef] [PubMed]
- Godman, B.; Grobler, C.; Van-De-Lisle, M.; Wale, J.; Barbosa, W.B.; Massele, A.; Opondo, P.; Petrova, G.; Tachkov, K.; Sefah, I.; et al. Pharmacotherapeutic interventions for bipolar disorder type II: Addressing multiple symptoms and approaches with a particular emphasis on strategies in lower and middle-income countries. Expert Opin. Pharmacother. 2019, 20, 2237–2255. [Google Scholar] [CrossRef] [PubMed]
- Wettermark, B.; Godman, B.; Jacobsson, B.; Haaijer-Ruskamp, F.M. Soft regulations in pharmaceutical policy making: An overview of current approaches and their consequences. Appl. Health Econ. Health Policy 2009, 7, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Björkhem-Bergman, L.; Andersén-Karlsson, E.; Laing, R.; Diogene, E.; Melien, O.; Jirlow, M.; Malmström, R.E.; Vogler, S.; Godman, B.; Gustafsson, L.L. Interface management of pharmacotherapy. Joint hospital and primary care drug recommendations. Eur. J. Clin. Pharmacol. 2013, 69 (Suppl. 1), 73–78. [Google Scholar] [CrossRef] [PubMed]
- Mashaba, T.P.; Matlala, M.; Godman, B.; Meyer, J.C. Implementation and monitoring of decisions by pharmacy and therapeutics committees in South African public sector hospitals. Expert. Rev. Clin. Pharmacol. 2019, 12, 159–168. [Google Scholar] [CrossRef]
- MacBride-Stewart, S.; McTaggart, S.; Kurdi, A.; Sneddon, J.; McBurney, S.; do Nascimento, R.C.R.M.; Mueller, T.; Kwon, H.-Y.; Morton, A.; Seaton, R.A.; et al. Initiatives and reforms across Scotland in recent years to improve prescribing; findings and global implications of drug prescriptions. Int. J. Clin. Exp. Med. 2021, 14, 2563–2586. [Google Scholar]
- Nakwatumbah, S.; Kibuule, D.; Godman, B.; Haakuria, V.; Kalemeera, F.; Baker, A.; Mubita, M. Compliance to guidelines for the prescribing of antibiotics in acute infections at Namibia’s national referral hospital: A pilot study and the implications. Expert Rev. Anti-Infect. Ther. 2017, 15, 713–721. [Google Scholar] [CrossRef]
- Jacobs, T.G.; Robertson, J.; van den Ham, H.A.; Iwamoto, K.; Bak Pedersen, H.; Mantel-Teeuwisse, A.K. Assessing the impact of law enforcement to reduce over-the-counter (OTC) sales of antibiotics in low- and middle-income countries; a systematic literature review. BMC Health Serv. Res. 2019, 19, 536. [Google Scholar] [CrossRef]
- Alrasheedy, A.A.; Alsalloum, M.A.; Almuqbil, F.A.; Almuzaini, M.A.; Aba Alkhayl, B.S.; Albishri, A.S.; Alharbi, F.F.; Alharbi, S.R.; Alodhayb, A.K.; Alfadl, A.A.; et al. The impact of law enforcement on dispensing antibiotics without prescription: A multi-methods study from Saudi Arabia. Expert Rev. Anti-Infect. Ther. 2020, 18, 87–97. [Google Scholar] [CrossRef]
- Mustafa, Z.U.; Salman, M.; Yasir, M.; Godman, B.; Majeed, H.A.; Kanwal, M.; Iqbal, M.; Riaz, M.B.; Hayat, K.; Hasan, S.S. Antibiotic consumption among hospitalized neonates and children in Punjab province, Pakistan. Expert Rev. Anti-Infect. Ther. 2021, 20, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Saleem, Z.; Hassali, M.A.; Versporten, A.; Godman, B.; Hashmi, F.K.; Goossens, H.; Saleem, F. A multicenter point prevalence survey of antibiotic use in Punjab, Pakistan: Findings and implications. Expert Rev. Anti-Infect. Ther. 2019, 17, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Kurdi, A.; Hasan, A.J.; Baker, K.I.; Seaton, R.A.; Ramzi, Z.S.; Sneddon, J.; Godman, B. A multicentre point prevalence survey of hospital antibiotic prescribing and quality indices in the Kurdistan regional government of Northern Iraq: The need for urgent action. Expert Rev. Anti-Infect. Ther. 2021, 19, 805–814. [Google Scholar] [CrossRef]
- Aiken, A.M.; Wanyoro, A.K.; Mwangi, J.; Juma, F.; Mugoya, I.K.; Scott, J.A. Changing use of surgical antibiotic prophylaxis in Thika Hospital, Kenya: A quality improvement intervention with an interrupted time series design. PLoS ONE 2013, 8, e78942. [Google Scholar] [CrossRef]
- Alabi, A.S.; Picka, S.W.; Sirleaf, R.; Ntirenganya, P.R.; Ayebare, A.; Correa, N.; Anyango, S.; Ekwen, G.; Agu, E.; Cook, R.; et al. Implementation of an antimicrobial stewardship programme in three regional hospitals in the south-east of Liberia: Lessons learned. JAC-Antimicrob. Resist. 2022, 4, dlac069. [Google Scholar] [CrossRef] [PubMed]
- Bashar, M.A.; Miot, J.; Shoul, E.; van Zyl, R.L. Impact of an antibiotic stewardship programme in a surgical setting. S. Afr. J. Infect. Dis. 2021, 36, 307. [Google Scholar] [CrossRef]
- Ngonzi, J.; Bebell, L.M.; Boatin, A.A.; Owaraganise, A.; Tiibajuka, L.; Fajardo, Y.; Lugobe, H.M.; Wylie, B.J.; Jacquemyn, Y.; Obua, C.; et al. Impact of an educational intervention on WHO surgical safety checklist and pre-operative antibiotic use at a referral hospital in southwestern Uganda. Int. J. Qual. Health Care 2021, 33, mzab089. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Level | Patients, n (%) |
|---|---|---|
| Hospital facility | Hospital 1 Hospital 2 Hospital 3 Hospital 4 Hospital 5 Hospital 6 Hospital 7 Hospital 8 Hospital 9 Hospital 10 | 31 (10.1) 27 (8.8) 16 (5.2) 60 (19.5) 65 (21.2) 36 (11.7) 6 (2.0) 7 (2.3) 7 (2.3) 52 (17.0) |
| Ward specialty | Adult Medical Ward Adult Surgical Ward Mixed Adult Ward Mixed Pediatric Ward Neonatal Intensive Care Unit Pediatrics Medical Ward Not recorded | 81 (27.9) 21 (7.2) 87 (30.0) 27 (9.3) 20 (6.9) 54 (18.6) 17 (5.6) |
| Gender | Female Male Not recorded | 163 (53.1) 139 (45.3) 5 (1.6) |
| Age (years) | <5 ≥5 Not recorded | 76 (24.8) 220 (71.7) 11 (3.5) |
| Central vascular catheter | Yes No Not recorded | 1 (0.3) 275 (89.6) 31 (10.1) |
| Urinary catheter | Yes No Not recorded | 59 (19.2) 210 (68.4) 38 (12.4) |
| Peripheral vascular catheter | Yes No Not recorded | 247 (80.5) 45 (14.7) 15 (4.9) |
| Intubation | Yes No Not recorded | 6 (2.0) 238 (77.5) 63 (20.5) |
| Malaria status | Yes No Unknown/not recorded | 28 (9.1) 112 (36.5) 167 (54.4) |
| HIV status | Yes No Unknown/not recorded | 36 (11.7) 75 (24.4) 196 (63.9) |
| HIV on Antiretroviral Therapy | Yes No Unknown/not recorded | 24 (7.8) 73 (23.8) 210 (68.4) |
| Tuberculosis status | Yes No Unknown/not recorded | 9 (2.9) 99 (32.2) 199 (64.8) |
| Variable and n | Infection/Antibiotics Prescribed | Frequency, n (%) |
|---|---|---|
| Diagnosis, n = 307 | CNS | 9 (2.9) |
| CVS | 6 (2.0) | |
| ENT | 17 (5.5) | |
| GI | 23 (7.5) | |
| OBGY | 38 (12.4) | |
| Pneu | 36 (11.7) | |
| Sepsis | 13 (4.2) | |
| Other | 165 (53.7) | |
| Antibiotic (ATC code/and AWaRe classification) and Mode of action, n = 534 | Access | |
| J01CA04 (Amoxicillin)—Bactericidal; inhibits bacterial cell wall biosynthesis | 27 (5.1) | |
| J01CE01(Benzyl Penicillin)—Bactericidal; inhibits bacterial cell wall biosynthesis | 43 (8.1) | |
| J01CF02 (Cloxacillin)—Bactericidal; inhibits bacterial cell wall biosynthesis | 29 (5.4) | |
| J01GB03 (Gentamicin)—Bactericidal; interferes with bacterial protein synthesis | 25 (4.7) | |
| P01AB01 (Metronidazole)—Bactericidal; disrupts bacterial DNA synthesis | 58 (10.9) | |
| Watch | ||
| J01DD01 (Cefotaxime)—Bactericidal; inhibits bacterial cell wall biosynthesis | 70 (13.1) | |
| J01DD04 (Ceftriaxone)—Bactericidal; inhibits bacterial cell wall biosynthesis | 193 (36.1) | |
| JO1MA02 (Ciprofloxacin)—Bactericidal; inhibits bacterial DNA gyrase enzyme | 30 (5.6) | |
| Others * | 59 (11.1) | |
| Parenteral type, n = 307 | IM | 4 (1.3) |
| IV—Bolus | 205 (66.8) | |
| IV—Continuous (via a catheter) | 29 (9.4) | |
| Other | 69 (22.5) |
| Variable | % Undertaken/Adherence |
|---|---|
| Rationale for prescription documented in the patient’s notes/indication documented in patient’s notes | 15.7% |
| CST requested | 3% |
| % Empiric use * | 97% |
| Stop/review data stated in the patient’s notes | 32% |
| Compliance with Zambian STGs | 27% |
| INN prescribing | 83% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalungia, A.C.; Mukosha, M.; Mwila, C.; Banda, D.; Mwale, M.; Kagulura, S.; Ogunleye, O.O.; Meyer, J.C.; Godman, B. Antibiotic Use and Stewardship Indicators in the First- and Second-Level Hospitals in Zambia: Findings and Implications for the Future. Antibiotics 2022, 11, 1626. https://doi.org/10.3390/antibiotics11111626
Kalungia AC, Mukosha M, Mwila C, Banda D, Mwale M, Kagulura S, Ogunleye OO, Meyer JC, Godman B. Antibiotic Use and Stewardship Indicators in the First- and Second-Level Hospitals in Zambia: Findings and Implications for the Future. Antibiotics. 2022; 11(11):1626. https://doi.org/10.3390/antibiotics11111626
Chicago/Turabian StyleKalungia, Aubrey C., Moses Mukosha, Chiluba Mwila, David Banda, Matthews Mwale, Solomon Kagulura, Olanyika O. Ogunleye, Johanna C. Meyer, and Brian Godman. 2022. "Antibiotic Use and Stewardship Indicators in the First- and Second-Level Hospitals in Zambia: Findings and Implications for the Future" Antibiotics 11, no. 11: 1626. https://doi.org/10.3390/antibiotics11111626
APA StyleKalungia, A. C., Mukosha, M., Mwila, C., Banda, D., Mwale, M., Kagulura, S., Ogunleye, O. O., Meyer, J. C., & Godman, B. (2022). Antibiotic Use and Stewardship Indicators in the First- and Second-Level Hospitals in Zambia: Findings and Implications for the Future. Antibiotics, 11(11), 1626. https://doi.org/10.3390/antibiotics11111626