
Developing a Tool for Auditing the Quality of Antibiotic Dispensing in Community Pharmacies: A Pilot Study

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
The Audit Project Odense Methodology
- To assess the feasibility of registering antibiotic dispensing using the registration chart in the community pharmacy setting;
- To collect feedback from community pharmacists on the implementation of the APO method;
- To describe antibiotic dispensing practices in four European countries.
2. Results
2.1. Feasibility of the APO-Methodology in Community Pharmacy Practice
2.2. Antibiotic Dispensing Practice
2.3. Feedback on the Registration Chart
2.4. Revising the Registration Chart for the Main Study
3. Discussion
3.1. Strengths of the Study
3.2. Limitations of the Study
3.3. Comparison with Literature
3.4. Meaning of the Study and Future Studies
4. Materials and Methods
4.1. Study Design
4.2. Study Setting
4.3. Development of the Registration Chart
4.4. Data Collection
4.5. Questionnaire
4.6. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Additional Data

{kind=link}
{kind=link}
| Treatment Duration in Days | Total | Total (%) | Missing 7 (1.7%) |
|---|---|---|---|
| 1 | 5 | 1.2 | |
| 2 | 26 | 6.4 | |
| 3 | 30 | 7.3 | |
| 4 | 3 | 0.7 | |
| 5 | 42 | 10.3 | |
| 6 | 21 | 5.1 | |
| 7 | 131 | 32.0 | |
| 8 | 15 | 3.7 | |
| 9 | 5 | 1.2 | |
| 10 | 59 | 14.4 | |
| 11 | 1 | 0.2 | |
| 12 | 4 | 1.0 | |
| 13 | 1 | 0.2 | |
| 14 | 7 | 1.7 | |
| 15 | 2 | 0.5 | |
| 16 | 1 | 0.2 | |
| 20 | 9 | 2.2 | |
| 21 | 1 | 0.2 | |
| 30 | 3 | 0.7 | |
| 42 | 1 | 0.2 | |
| 44 | 1 | 0.2 | |
| 90 | 1 | 0.2 | |
| 98 | 3 | 0.7 | |
| unknown | 28 | 6.9 | |
| Advice provided | |||
| Treatment duration | 271 | 66.3 | |
| Risk of AMR | 74 | 18.1 | |
| Take shortly before sleeping | 17 | 4.2 | |
| Do not take shortly before sleeping | 3 | 0.7 | |
| Take with food or drinks | 45 | 11.0 | |
| Do not take with food or drinks | 44 | 10.8 | |
| Take while sitting or standing | 0 | 0.0 | |
| Advice regarding comedication | 35 | 8.6 | |
| Be careful with sunlight | 20 | 4.9 | |
| Information about side effects | 85 | 20.8 | |
| Seek medical help if symptoms worsen | 76 | 18.6 | |
| Bring back leftovers | 15 | 3.7 | |
| No advice given | 52 | 12.7 |
| Indication Known | Indication Unknown | |||
|---|---|---|---|---|
| TRD Known | TRD Unknown | TRD Known | TRD Unknown | |
| Agree | 0 | 5 | 26 | 0 |
| Insufficient info | 0 | 14 | 10 | 9 |
Appendix B

Appendix C

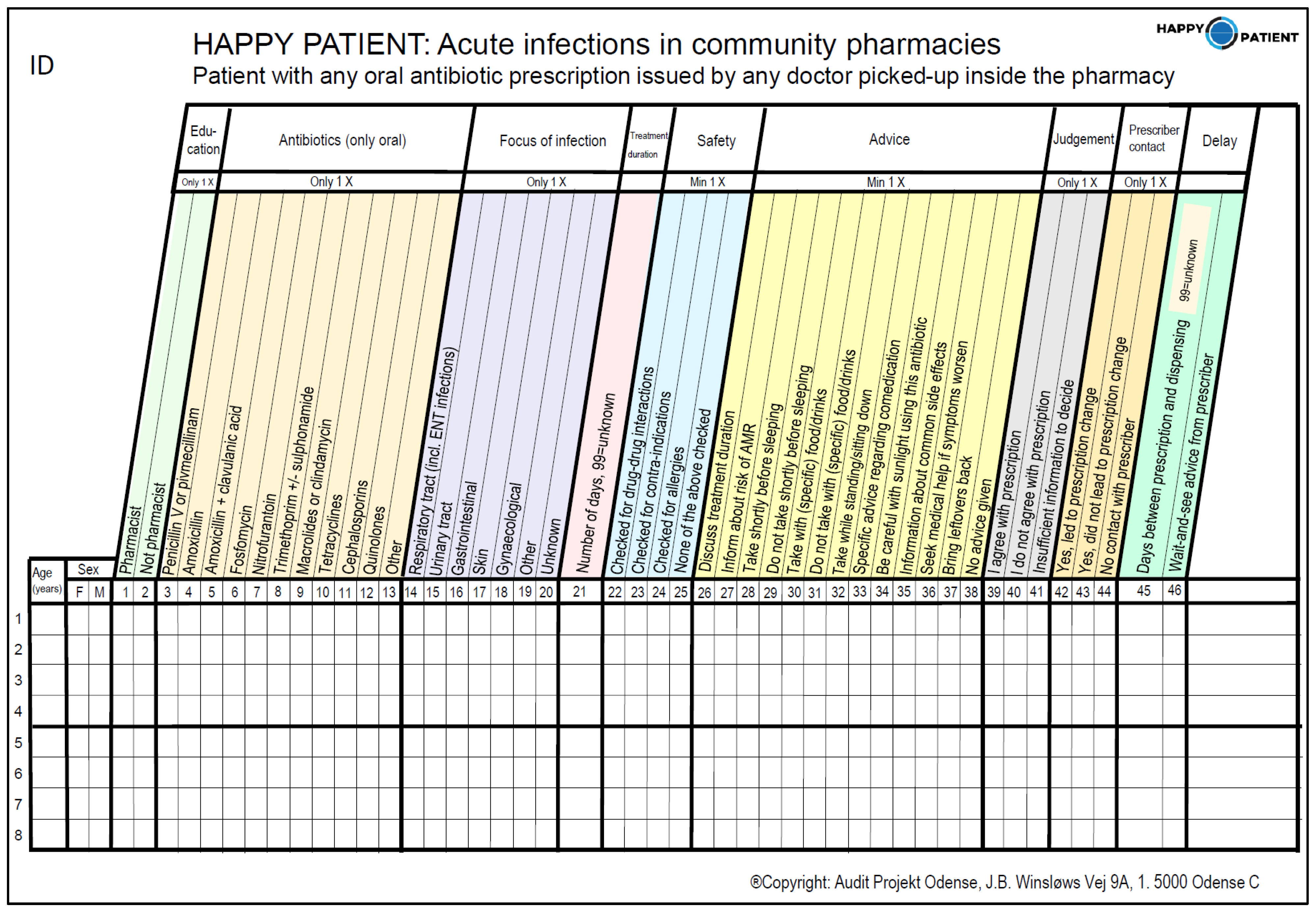
Appendix D. Instructions for Completing the APO Registration Chart
| Age | Please provide age in years. For children ages less than one year, please indicate 0. |
| Sex | Please state if the patient is female or male. |
| Occupation | Please indicate if the person who has dispensed the antibiotic is a pharmacist or another staff member of the pharmacy (e.g., pharmacist technician). |
| Antibiotics (only oral) | Please cross (X) which antibiotic (class) has been dispensed. If necessary, please use the list provided to determine the antibiotic class to which the prescribed antibiotic belongs. |
| Focus infection | Please cross for which type of infection the antibiotic was prescribed. Cross unknown if this information was not available. |
| Treatment duration | Please state the duration of the prescribed treatment in numbers. Use 99 if the treatment length was not specified on the prescription. |
| Safety (multiple answers possible) | Please indicate which checks have been performed during dispensing. Drug-drug interactions include interactions with all other medication used by the patient. Contra-indications may include all conditions, states, or diseases of a patient. Allergies include all allergies to the prescribed antibiotic and any cross-reactivity reactions related to them. Multiple answers may be crossed. |
| Advice (multiple answers possible) | Please cross the boxes that state the advice you provided to the patient during dispensing. Multiple answers may be crossed. |
| Agree with the prescription | Please indicate if you agree with the prescribed antibiotic in this specific situation. Please only include disagreements on a clinical basis (e.g., antibiotic unnecessary, wrong choice of antibiotic, wrong dose/duration). Disagreement with the prescription due to administrative reasons (missing patient/prescriber information) should not be included. |
| Prescriber contact | Please state if contact between you and the prescriber has led to any clinical changes (e.g., change of dose/antibiotic) to the prescription. Please tick ‘no contact with prescriber’ if there was no additional contact between the pharmacy and the prescriber. |
| Delayed prescribing | Please indicate the number of days between the date of prescribing and the date of dispensing. If the antibiotic is dispensed on the same day as the prescription was issued, please indicate ‘0’. If this information is unknown, please indicate ‘99’. Please cross ‘wait-and-see advice from prescriber’ if the delay between prescribing and dispensing was based on advice from the prescriber. If the patients delayed on their own initiative, please leave blank. |
Appendix E
| Generic Name | Class |
|---|---|
| 1. Amoxicillin | Amoxicillin |
| 2. Amoxicillin and beta-lactamase inhibitor | Amoxicillin + clavulanic acid |
| 3. Azithromycin | Macrolides or clindamycin |
| 4. Cefadroxil | Cephalosporins |
| 5. Cefprozil | Cephalosporins |
| 6. Cefuroxime | Cephalosporins |
| 7. Ciprofloxacin | Quinolones |
| 8. Clarithromycin | Macrolides or clindamycin |
| 9. Clindamycin | Macrolides or clindamycin |
| 10. Doxycycline | Tetracyclines |
| 11. Erythromycin | Macrolides or clindamycin |
| 12. Fosfomycin | Fosfomycin |
| 13. Levofloxacin | Quinolones |
| 14. Nitrofurantoin | Nitrofurantoin |
| 15. Phenoxymethylpenicillin | Penicillin V or pivmecillinam |
| 16. Pivmecillinam | Penicillin V or pivmecillinam |
| 17. Sulfamethoxazole and trimethoprim | Trimethoprim +/− sulfonamide |
| 18. Tetracycline | Tetracyclines |
| 19. Trimethoprim | Trimethoprim +/− sulfonamide |
Appendix F. Questionnaire to Provide Feedback after Pilot Study
- (1)
- Are the instruction document and registration chart clear/easy to use? Please specify any possible improvements.
- (2)
- Was it easy to match the dispensed products with the antibiotic classes using the list of antibiotics provided? If not, please specify the problems you encountered.
- (3)
- Please state how much time it takes to fill in one registration chart.
- (4)
- Did you manage to register all patients with a prescription for an oral antibiotic for days? If not, please specify the problems you encountered.
- (5)
- Do you believe it to be possible to register all antibiotic dispensing for a period of four weeks?
- (6)
- Has the complete pharmacy staff participated in the pilot study or only a part of the staff?
- (7)
- Does the advice seem appropriate to the pharmacy setting in your country?
- (8)
- Are there any important topics/advises missing in the registration chart?
- (9)
- Are there any topics/advises you would consider irrelevant?
- (10)
- Do you have any additional comments?
References
- Rusic, D.; Bozic, J.; Bukic, J.; Vilovic, M.; Tomicic, M.; Seselja Perisin, A.; Leskur, D.; Modun, D.; Cohadzic, T.; Tomic, S. Antimicrobial Resistance: Physicians’ and Pharmacists’ Perspective. Microb. Drug Resist. 2020, 27, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Rusic, D.; Bukić, J.; Perisin, A.S.; Leskur, D.; Modun, D.; Petric, A.; Vilovic, M.; Bozic, J. Are We Making the Most of Community Pharmacies? Implementation of Antimicrobial Stewardship Measures in Community Pharmacies: A Narrative Review. Antibiotics 2021, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control EU Guidelines for the Prudent Use of Antimicrobials in Human Health; ECDC: Stockholm, Sweden, 2017.
- World Health Organization. International Pharmaceutical Federation Joint FIP/WHO Guidelines on Good Pharmacy Practice: Standards for Quality of Pharmacy Services Background; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- World Health Organization Regional Office for Europe. The Legal and Regulatory Framework for Community Pharmacies in the WHO European Region; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Santos, S.C.; Boaventura, T.C.; Rocha, K.S.S.; Filho, A.D.D.O.; Onozato, T.; de Lyra, D.P., Jr. Can we document the practice of dispensing? A systematic review. J. Clin. Pharm. Ther. 2016, 41, 634–644. [Google Scholar] [CrossRef] [PubMed]
- Munck, A.; Damsgaard, J.; Gp, M.D.; Gilsa, D.; Hansen, Ê.; Bjerrum, L.; Sùndergaard, J. The Nordic Method for Quality Improvement in General Practice. Qual. Prim. Care 2003, 11, 73–78. [Google Scholar]
- Llor, C.; Cots, J.M.; Hernández, S.; Ortega, J.; Arranz, J.; Monedero, M.J.; Alcántara, J.D.D.; Pérez, C.; García, G.; Gómez, M.; et al. Effectiveness of two types of intervention on antibiotic prescribing in respiratory tract infections in Primary Care in Spain. Happy Audit Study. Atencion Primaria 2014, 46, 492–500. [Google Scholar] [CrossRef] [Green Version]
- Hansen, M.P.; Lykkegaard, J.; Søndergaard, J.; Munck, A.; Llor, C. How to improve practice by means of the Audit Project Odense method. Br. J. Gen. Pract. 2022, 72, 235–236. [Google Scholar] [CrossRef]
- Munck, A.P.; Gilså Hansen, D.; Lindman, A.; Ovhed, I.; Førre, S.; Bjarni Torsteinsson, J. A Nordic Collaboration on Medical Audit: The APO method for quality development and continuous medical education (CME) in primary health care. Scand. J. Prim. Health Care 1998, 16, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Paget, J.; Lescure, D.; Versporten, A.; Goossens, H.; Schellevis, F.; Van Dijk, L. Antimicrobial Resistance and Causes of Non-Prudent Use of Antibiotics in Human Medicine in the EU; European Commission: Brussels, Belgium, 2017. [Google Scholar]
- Torres, N.F.; Solomon, V.P.; Middleton, L.E. Pharmacists’ practices for non-prescribed antibiotic dispensing in Mozambique. Pharm. Pr. 2020, 18, 1965. [Google Scholar] [CrossRef]
- Zakaa El-din, M.; Samy, F.; Mohamed, A.; Hamdy, F.; Yasser, S.; Ehab, M. Egyptian community pharmacists’ attitudes and practices towards antibiotic dispensing and antibiotic resistance; A cross-sectional survey in Greater Cairo. Curr. Med. Res. Opin. 2019, 35, 939–946. [Google Scholar] [CrossRef]
- Darwish, R.M.; Baqain, G.N.; Aladwan, H.; Salamah, L.M.; Madi, R.; Al Masri, R.M. Knowledge, attitudes, and practices regarding antibiotic use and resistance among community pharmacists: A cross sectional study in Jordan. Int. J. Clin. Pharm. 2021, 43, 1198–1207. [Google Scholar] [CrossRef]
- Zawahir, S.; Lekamwasam, S.; Aslani, P. Antibiotic dispensing practice in community pharmacies: A simulated client study. Res. Soc. Adm. Pharm. 2018, 15, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Cachafeiro, M.; Piñeiro-Lamas, M.; Guinovart, M.C.; López-Vázquez, P.M.; Vazquez-Lago, J.; Figueiras, A. Magnitude and determinants of antibiotic dispensing without prescription in Spain: A simulated patient study. J. Antimicrob. Chemother. 2018, 74, 511–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianco, A.; Licata, F.; Trovato, A.; Napolitano, F.; Pavia, M. Antibiotic-Dispensing Practice in Community Pharmacies: Results of a Cross-Sectional Study in Italy. Antimicrob. Agents Chemother. 2021, 65, e02729-20. [Google Scholar] [CrossRef] [PubMed]
- Plachouras, D.; Kavatha, D.; Antoniadou, A.; Giannitsioti, E.; Poulakou, G.; Kanellakopoulou, K.; Giamarellou, H. Dispensing of antibiotics without prescription in Greece, 2008: Another link in the antibiotic resistance chain. Eurosurveillance 2010, 15, 19488. [Google Scholar] [CrossRef] [PubMed]
- Islam, A.; Akhtar, Z.; Hassan, Z.; Chowdhury, S.; Rashid, M.; Aleem, M.A.; Ghosh, P.K.; Mah-E-Muneer, S.; Parveen, S.; Ahmmed, K.; et al. Pattern of Antibiotic Dispensing at Pharmacies According to the WHO Access, Watch, Reserve (AWaRe) Classification in Bangladesh. Antibiotics 2022, 11, 247. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.P.; Do, T.X.; Nguyen, H.A.; Nguyen, C.T.T.; Meyer, J.C.; Godman, B.; Skosana, P.; Nguyen, B.T. A National Survey of Dispensing Practice and Customer Knowledge on Antibiotic Use in Vietnam and the Implications. Antibiotics 2022, 11, 1091. [Google Scholar] [CrossRef]
- Ndaki, P.M.; Mushi, M.F.; Mwanga, J.R.; Konje, E.T.; Ntinginya, N.E.; Mmbaga, B.T.; Keenan, K.; Sabiiti, W.; Kesby, M.; Benitez-Paez, F.; et al. Dispensing Antibiotics without Prescription at Community Pharmacies and Accredited Drug Dispensing Outlets in Tanzania: A Cross-Sectional Study. Antibiotics 2021, 10, 1025. [Google Scholar] [CrossRef]
- Institute for Evidence-Based Health Pharmacy Services in Europe: Evaluating Trends and Value; ISBE: Lisbon, Portugal, 2020.
- Kaae, S.; Ghazaryan, L.; Pagava, K.; Korinteli, I.; Makalkina, L.; Zhetimkarinova, G.; Ikhambayeva, A.; Tentiuc, E.; Ratchina, S.; Zakharenkova, P.; et al. The antibiotic knowledge, attitudes and behaviors of patients, doctors and pharmacists in the WHO Eastern European region—A qualitative, comparative analysis of the culture of antibiotic use in Armenia, Georgia, Kazakhstan, Moldova, Russia and Tajikistan. Res. Soc. Adm. Pharm. 2020, 16, 238–248. [Google Scholar] [CrossRef]
- Machowska, A.; Lundborg, C.S. Drivers of Irrational Use of Antibiotics in Europe. Int. J. Environ. Res. Public Health 2019, 16, 27. [Google Scholar] [CrossRef] [Green Version]
- Servia-Dopazo, M.; Figueiras, A. Determinants of antibiotic dispensing without prescription: A systematic review. J. Antimicrob. Chemother. 2018, 73, 3244–3253. [Google Scholar] [CrossRef]
- Roque, F.; Soares, S.; Breitenfeld, L.; López-Durán, A.; Figueiras, A.; Herdeiro, M.T. Attitudes of community pharmacists to antibiotic dispensing and microbial resistance: A qualitative study in Portugal. Int. J. Clin. Pharm. 2013, 35, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Lescure, D.; Paget, J.; Schellevis, F.; Van Dijk, L. Determinants of Self-Medication with Antibiotics in European and Anglo-Saxon Countries: A Systematic Review of the Literature. Front. Public Health 2018, 6, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjerrum, A.; García-Sangenís, A.; Modena, D.; Córdoba, G.; Bjerrum, L.; Chalkidou, A.; Lykkegaard, J.; Hansen, M.P.; Søndergaard, J.; Nexøe, J.; et al. Health alliance for prudent prescribing and yield of antibiotics in a patient-centred perspective (HAPPY PATIENT): A before-and-after intervention and implementation study protocol. BMC Prim. Care 2022, 23, 102. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control Summary of the Latest Data on Antibiotic Consumption in the European Union; ECDC: Stockholm, Sweden, 2017.
- World Health Organization Regional Office for Europe. European Strategic Action Plan on Antibiotic Resistance; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- World Health Organization Regional Office for Europe. The Role of Pharmacist in Encouraging Prudent Use of Antibiotics and Averting Antimicrobial Resistance: A Review of Policy and Experience; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2014. [Google Scholar]
| Greece | Lithuania | Poland | Spain | Total | Total (%) | Missing | |
|---|---|---|---|---|---|---|---|
| Dispenses registered | 55 (13.4%) | 103 (25.2%) | 74 (18.1%) | 177 (43.3%) | 409 | 100 | |
| Sex | 0 (0%) | ||||||
| Female | 32 | 69 | 42 | 97 | 240 | 58.7 | |
| Male | 23 | 34 | 32 | 80 | 169 | 41.3 | |
| Education | 7 (1.7%) | ||||||
| Pharmacist | 38 | 92 | 68 | 116 | 314 | 76.8 | |
| Not pharmacist | 17 | 8 | 6 | 57 | 88 | 21.5 | |
| Antibiotics dispensed | 2 (0.5%) | ||||||
| Penicillin V or pivmecillinam | 0 | 0 | 2 | 2 | 4 | 1.0 | |
| Amoxicillin | 7 | 20 | 6 | 36 | 69 | 16.9 | |
| Amoxicillin + clavulanic acid | 17 | 25 | 13 | 31 | 86 | 21.0 | |
| Fosfomycin | 0 | 1 | 1 | 29 | 31 | 7.6 | |
| Nitrofurantoin | 0 | 10 | 1 | 2 | 13 | 3.2 | |
| Trimethoprim +/− Sulphonamides | 0 | 4 | 2 | 1 | 7 | 1.7 | |
| Macrolides or clindamycin | 1 | 9 | 26 | 31 | 67 | 16.4 | |
| Tetracyclines | 2 | 9 | 4 | 2 | 17 | 4.2 | |
| Cephalosporins | 11 | 12 | 10 | 16 | 49 | 12.0 | |
| Quinolones | 12 | 2 | 5 | 19 | 38 | 9.3 | |
| Other | 5 | 9 | 4 | 8 | 26 | 6.4 | |
| Focus of infection | 1 (0.2%) | ||||||
| Respiratory tract | 28 | 42 | 52 | 80 | 202 | 49.4 | |
| Urinary tract | 7 | 16 | 6 | 45 | 74 | 18.1 | |
| Gastrointestinal | 6 | 4 | 1 | 11 | 22 | 5.4 | |
| Skin | 2 | 1 | 5 | 11 | 19 | 4.7 | |
| Gynaecological | 1 | 1 | 1 | 0 | 3 | 0.7 | |
| Other | 9 | 10 | 1 | 23 | 43 | 10.5 | |
| Unknown | 2 | 29 | 8 | 6 | 45 | 11.0 | |
| Safety checks performed | |||||||
| Interactions | 25 | 10 | 23 | 58 | 116 | 28.4 | |
| Contraindications | 20 | 1 | 8 | 55 | 84 | 20.5 | |
| Allergies | 38 | 16 | 15 | 78 | 147 | 35.9 | |
| None of the above | 10 | 72 | 38 | 82 | 202 | 49.4 | |
| All safety checks performed | 12 | 0 | 0 | 42 | 54 | 13.2 | |
| Prescriber contact | 49 (12.0%) | ||||||
| Yes, and changes to prescription | 0 | 8 | 0 | 1 | 9 | 2.2 | |
| Yes, no changes to prescription | 2 | 0 | 0 | 3 | 5 | 1.2 | |
| No contact with prescriber | 34 | 89 | 74 | 149 | 346 | 84.6 | |
| Pharmacy judgement of prescription | 2 (0.5%) | ||||||
| Agree with prescription | 39 | 86 | 51 | 110 | 286 | 69.9 | |
| Do not agree with prescription | 5 | 3 | 0 | 6 | 14 | 3.4 | |
| Insufficient information to decide | 10 | 13 | 23 | 61 | 107 | 26.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambert, M.; Benkő, R.; Chalkidou, A.; Lykkegaard, J.; Hansen, M.P.; Llor, C.; Touboul, P.; Trečiokienė, I.; Karkana, M.-N.; Kowalczyk, A.; et al. Developing a Tool for Auditing the Quality of Antibiotic Dispensing in Community Pharmacies: A Pilot Study. Antibiotics 2022, 11, 1529. https://doi.org/10.3390/antibiotics11111529
Lambert M, Benkő R, Chalkidou A, Lykkegaard J, Hansen MP, Llor C, Touboul P, Trečiokienė I, Karkana M-N, Kowalczyk A, et al. Developing a Tool for Auditing the Quality of Antibiotic Dispensing in Community Pharmacies: A Pilot Study. Antibiotics. 2022; 11(11):1529. https://doi.org/10.3390/antibiotics11111529
Chicago/Turabian StyleLambert, Maarten, Ria Benkő, Athina Chalkidou, Jesper Lykkegaard, Malene Plejdrup Hansen, Carl Llor, Pia Touboul, Indrė Trečiokienė, Maria-Nefeli Karkana, Anna Kowalczyk, and et al. 2022. "Developing a Tool for Auditing the Quality of Antibiotic Dispensing in Community Pharmacies: A Pilot Study" Antibiotics 11, no. 11: 1529. https://doi.org/10.3390/antibiotics11111529
APA StyleLambert, M., Benkő, R., Chalkidou, A., Lykkegaard, J., Hansen, M. P., Llor, C., Touboul, P., Trečiokienė, I., Karkana, M.-N., Kowalczyk, A., & Taxis, K. (2022). Developing a Tool for Auditing the Quality of Antibiotic Dispensing in Community Pharmacies: A Pilot Study. Antibiotics, 11(11), 1529. https://doi.org/10.3390/antibiotics11111529