
Comparative Effectiveness of Ampicillin/Sulbactam versus Cefazolin as Targeted Therapy for Bacteremia Caused by Beta-Lactamase-Producing Methicillin-Sensitive Staphylococcus aureus: A Single-Center Retrospective Study
 ,
,  ,
,
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
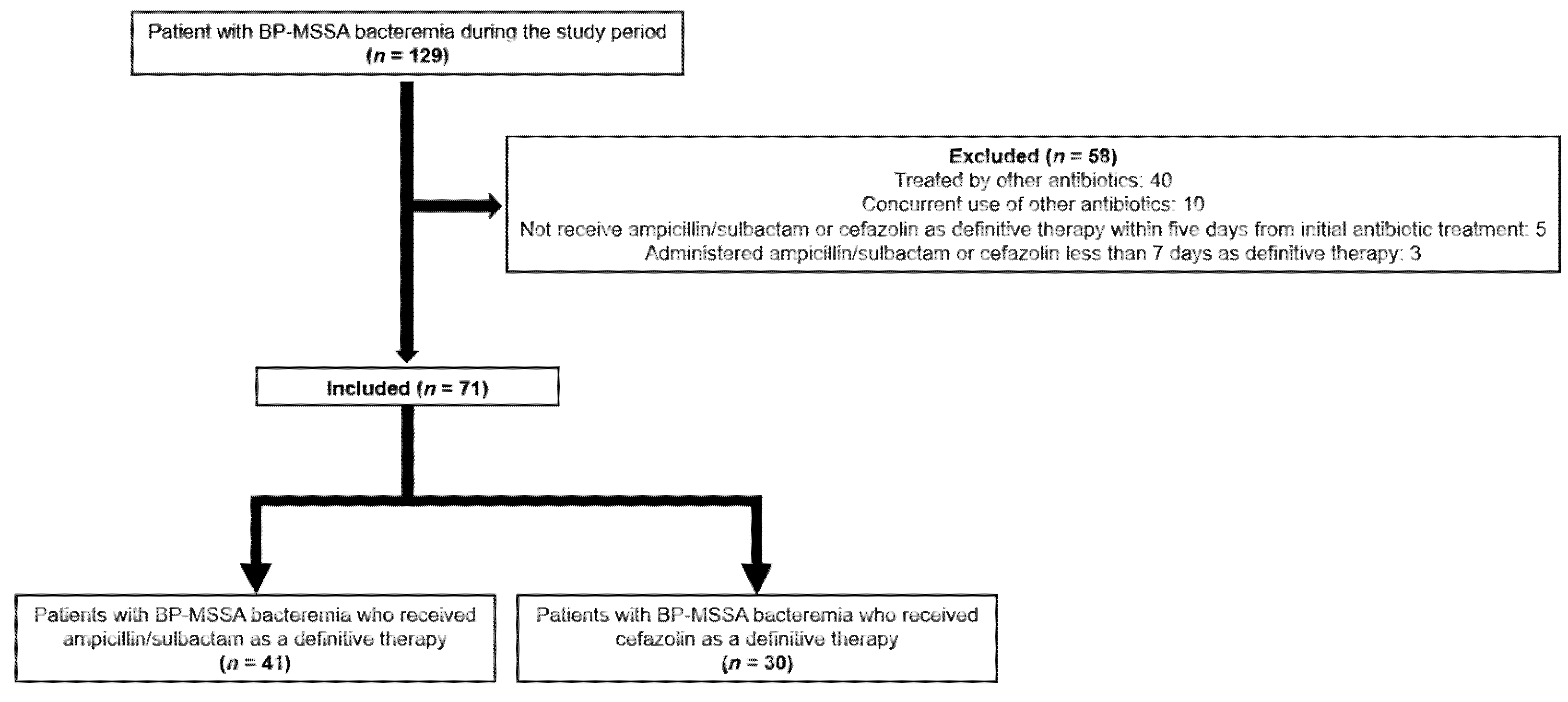
4.1. Patient Population
4.2. Inclusion Criteria
4.3. Exclusion Criteria
4.4. Data Collection
4.5. Hematological and Blood Chemistry Analyses
4.6. Microbiological Evaluation
4.7. Statistical Analysis
4.8. Ethical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bai, A.D.; Showler, A.; Burry, L.; Steinberg, M.; Ricciuto, D.R.; Fernandes, T.; Chiu, A.; Raybardhan, S.; Science, M.; Fernando, E.; et al. Comparative effectiveness of cefazolin versus cloxacillin as definitive antibiotic therapy for MSSA bacteraemia: Results from a large multicentre cohort study. J. Antimicrob. Chemother. 2015, 70, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Abraham, L.; Bamberger, D.M. Staphylococcus aureus bacteremia: Contemporary management. Mo Med. 2020, 117, 341–345. [Google Scholar] [PubMed]
- Lewis, P.O.; Heil, E.L.; Covert, K.L.; Cluck, D.B. Treatment strategies for persistent methicillin-resistant Staphylococcus aureus bacteraemia. J. Clin. Pharm. Ther. 2018, 43, 614–625. [Google Scholar] [CrossRef] [PubMed]
- Lowy, F.D. Staphylococcus aureus infections. N. Engl. J. Med. 1998, 339, 520–532. [Google Scholar] [CrossRef]
- Li, J.; Echevarria, K.L.; Traugott, K.A. β-Lactam therapy for methicillin-susceptible Staphylococcus aureus bacteremia: A comparative review of cefazolin versus antistaphylococcal penicillins. Pharmacotherapy 2017, 37, 346–360. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef]
- Lee, S.; Choe, P.G.; Song, K.H.; Park, S.W.; Kim, H.B.; Kim, N.J.; Kim, E.C.; Park, W.B.; Oh, M.D. Is cefazolin inferior to nafcillin for treatment of methicillin-susceptible Staphylococcus aureus bacteremia? Antimicrob Agents Chemother. 2011, 55, 5122–5126. [Google Scholar] [CrossRef]
- Twilla, J.D.; Algrim, A.; Adams, E.H.; Samarin, M.; Cummings, C.; Finch, C.K. Comparison of nafcillin and cefazolin for the treatment of methicillin-susceptible Staphylococcus aureus bacteremia. Am. J. Med. Sci. 2020, 360, 35–41. [Google Scholar] [CrossRef]
- Lee, S.; Song, K.H.; Jung, S.I.; Park, W.B.; Lee, S.H.; Kim, Y.S.; Kwak, Y.G.; Kim, Y.K.; Kiem, S.M.; Kim, H.I.; et al. Comparative outcomes of cefazolin versus nafcillin for methicillin-susceptible Staphylococcus aureus bacteraemia: A prospective multicentre cohort study in Korea. Clin. Microbiol. Infect. 2018, 24, 152–158. [Google Scholar] [CrossRef]
- Koizumi, R.; Kusama, Y.; Asai, Y.; Yoshiaki, G.; Muraki, Y.; Ohmagari, N. Effects of the cefazolin shortage on the sales, cost, and appropriate use of other antimicrobials. BMC Health Serv. Res. 2021, 21, 1118. [Google Scholar] [CrossRef] [PubMed]
- Nichi-iko. Cefazolin Sodium Details of Supply Issue. Available online: https://www.nichiiko.co.jp/company/press/detail/4656/814/4541_20190513_CEZ_J.pdf (accessed on 2 September 2021). (In Japanese).
- Ministry of Health, LaW. Alternative Drug List for Cefazolin Shortage. Available online: https://www.mhlw.go.jp/content/10900000/000498133.pdf (accessed on 2 September 2022). (In Japanese)
- Carr, D.R.; Stiefel, U.; Bonomo, R.A.; Burant, C.J.; Sims, S.V. A Comparison of cefazolin versus ceftriaxone for the treatment of methicillin-susceptible Staphylococcus aureus bacteremia in a tertiary care VA medical center. Open Forum. Infect Dis. 2018, 5, ofy089. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Zemer-Wassercug, N.; Talker, O.; Lishtzinsky, Y.; Lev, B.; Samra, Z.; Leibovici, L.; Bishara, J. Are all beta-lactams similarly effective in the treatment of methicillin-sensitive Staphylococcus aureus bacteraemia? Clin. Microbiol. Infect. 2011, 17, 1581–1586. [Google Scholar] [CrossRef] [PubMed]
- McDanel, J.S.; Perencevich, E.N.; Diekema, D.J.; Herwaldt, L.A.; Smith, T.C.; Chrischilles, E.A.; Dawson, J.D.; Jiang, L.; Goto, M.; Schweizer, M.L. Comparative effectiveness of beta-lactams versus vancomycin for treatment of methicillin-susceptible Staphylococcus aureus bloodstream infections among 122 hospitals. Clin. Infect. Dis. 2015, 61, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.; Wong, T.; Romney, M.; Leung, V. Comparative effectiveness of β-lactam versus vancomycin empiric therapy in patients with methicillin-susceptible Staphylococcus aureus (MSSA) bacteremia. Ann. Clin. Microbiol. Antimicrob. 2016, 15, 27. [Google Scholar] [CrossRef]
- van Hal, S.J.; Jensen, S.O.; Vaska, V.L.; Espedido, B.A.; Paterson, D.L.; Gosbell, I.B. Predictors of mortality in Staphylococcus aureus Bacteremia. Clin. Microbiol. Rev. 2012, 25, 362–386. [Google Scholar] [CrossRef]
- Gundlapalli, A.V.; Beekmann, S.E.; Graham, D.R.; Polgreen, P.M. Antimicrobial agent shortages: The new norm for infectious diseases physicians. Open Forum. Infect Dis. 2018, 5, ofy068. [Google Scholar] [CrossRef]
- Uda, A.; Shigemura, K.; Kitagawa, K.; Osawa, K.; Onuma, K.; Yan, Y.; Nishioka, T.; Fujisawa, M.; Yano, I.; Miyara, T. Risk factors for the acquisition of enterococcus faecium infection and mortality in patients with enterococcal bacteremia: A 5-year retrospective analysis in a tertiary care university hospital. Antibiotics 2021, 10, 64. [Google Scholar] [CrossRef]
- Uda, A.; Onuma, K.; Shigemura, K.; Kitagawa, K.; Yan, Y.; Osawa, K.; Yano, I.; Miyara, T. Impact of cefazolin shortage on clinical outcomes of adult patients with bacteremia caused by methicillin-susceptible Staphylococcus aureus in a tertiary care university hospital. Antibiotics 2021, 10, 1247. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Stevens, D.L.; Bisno, A.L.; Chambers, H.F.; Dellinger, E.P.; Goldstein, E.J.; Gorbach, S.L.; Hirschmann, J.V.; Kaplan, S.L.; Montoya, J.G.; Wade, J.C. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 59, e10–e52. [Google Scholar] [CrossRef]
- Peechakara, B.V.; Gupta, M. Ampicillin/Sulbactam. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, January 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK526117/ (accessed on 19 October 2022).
- Brook, I. Inoculum effect. Rev. Infect Dis. 1989, 11, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Shoji, T.; Hirai, Y.; Osawa, M.; Totsuka, K. Cefazolin therapy for methicillin-susceptible Staphylococcus aureus bacteremia in Japan. J. Infect. Chemother. 2014, 20, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Nannini, E.C.; Singh, K.V.; Murray, B.E. Relapse of type A beta-lactamase-producing Staphylococcus aureus native valve endocarditis during cefazolin therapy: Revisiting the issue. Clin. Infect. Dis. 2003, 37, 1194–1198. [Google Scholar] [CrossRef]
- Lee, S.; Kwon, K.T.; Kim, H.I.; Chang, H.H.; Lee, J.M.; Choe, P.G.; Park, W.B.; Kim, N.J.; Oh, M.D.; Song, D.Y.; et al. Clinical implications of cefazolin inoculum effect and β-lactamase type on methicillin-susceptible Staphylococcus aureus bacteremia. Microb. Drug. Resist. 2014, 20, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Song, K.H.; Jung, S.I.; Lee, S.; Park, S.; Kiem, S.M.; Lee, S.H.; Kwak, Y.G.; Kim, Y.K.; Jang, H.C.; Kim, Y.S.; et al. Characteristics of cefazolin inoculum effect-positive methicillin-susceptible Staphylococcus aureus infection in a multicentre bacteraemia cohort. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Saeki, M.; Shinagawa, M.; Yakuwa, Y.; Nirasawa, S.; Sato, Y.; Yanagihara, N.; Takahashi, S. Inoculum effect of high concentrations of methicillin-susceptible Staphylococcus aureus on the efficacy of cefazolin and other beta-lactams. J. Infect. Chemother. 2018, 24, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Seas, C.; Carvajal, L.P.; Diaz, L.; Echeverri, A.M.; Ferro, C.; Rios, R.; Porras, P.; Luna, C.; Gotuzzo, E.; et al. The cefazolin inoculum effect is associated with increased mortality in methicillin-susceptible Staphylococcus aureus bacteremia. Open Forum. Infect. Dis. 2018, 5, ofy123. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Drug Shortages: Root Causes and Potential Solutions. Available online: https://www.fda.gov/media/131130/download (accessed on 2 September 2021).
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Dewys, W.D.; Begg, C.; Lavin, P.T.; Band, P.R.; Bennett, J.M.; Bertino, J.R.; Cohen, M.H.; Douglass, H.O., Jr.; Engstrom, P.F.; Ezdinli, E.Z.; et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am. J. Med. 1980, 69, 491–497. [Google Scholar] [CrossRef]
- Fernando, S.M.; Tran, A.; Taljaard, M.; Cheng, W.; Rochwerg, B.; Seely, A.J.E.; Perry, J.J. Prognostic accuracy of the quick sequential organ failure assessment for mortality in patients with suspected infection: A systematic review and meta-analysis. Ann. Intern. Med. 2018, 168, 266–275. [Google Scholar] [CrossRef]
- Minejima, E.; Delayo, V.; Lou, M.; Ny, P.; Nieberg, P.; She, R.C.; Wong-Beringer, A. Utility of qSOFA score in identifying patients at risk for poor outcome in Staphylococcus aureus bacteremia. BMC Infect. Dis. 2019, 19, 149. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M. Assessment of clinical criteria for sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Prina, E.; Menéndez, R.; Ceccato, A.; Cilloniz, C.; Méndez, R.; Gabarrus, A.; Barbeta, E.; Bassi, G.L.; Ferrer, M.; et al. New sepsis definition (Sepsis-3) and community-acquired pneumonia mortality: A validation and clinical decision-making study. Am. J. Respir. Crit. Care Med. 2017, 196, 1287–1297. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Ternavasio-De La Vega, H.G.; Castaño-Romero, F.; Ragozzino, S.; González, R.S.; Vaquero-Herrero, M.P.; Siller-Ruiz, M.; Spalter-Glicberg, G.; Ramírez-Baum, C.; Rodríguez-Rodríguez, S.; García-Sánchez, J.E.; et al. The updated Charlson comorbidity index is a useful predictor of mortality in patients with Staphylococcus aureus bacteraemia. Epidemiol. Infect. 2018, 146, 2122–2130. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Fifth Informational Supplement; CLSI Document M100-S25; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]
- CLSI. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard, 10th ed.; CLSI Document M7-A10; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]



{kind=link}
{kind=link}
| Variables | All Patients | SAM | CFZ | p-Value |
|---|---|---|---|---|
| N = 71 | N = 41 | N = 30 | ||
| Mean age (years ± SD) | 69.8 ± 18.7 | 71.3 ± 2.9 | 67.7 ± 3.4 | 0.429 |
| Median age (years, range) | 75 (18–97) | 76 (19–97) | 73.5 (18–91) | |
| Male (n, %) | 51 (71.8) | 29 (70.7) | 22 (73.3) | 0.809 |
| Body mass index (kg/cm2) | 25.0 ± 4.8 | 20.3 ± 0.6 | 21.6 ± 0.8 | 0.181 |
| Hospital-acquired bacteremia | 31 (43.7) | 16 (39.0) | 15 (50.0) | 0.357 |
| PS (mean ± SD) PS ≥ 3–4 (n, %) | 1.7 ± 1.4 27 (38.0) | 1.9 ± 0.2 18 (43.9) | 1.5 ± 0.3 9 (30.0) | 0.245 0.233 |
| qSOFA ≥ 2 (n, %) | 14 (19.7) | 9 (22.0) | 5 (16.7) | 0.580 |
| Septic shock (n, %) | 7 (9.9) | 4 (9.8) | 3 (10.0) | 0.972 |
| Vasopressor use (n, %) | 1 (1.4) | 1 (2.4) | 0 (0) | 0.389 |
| Developed disseminated intravascular coagulation (n, %) | 25 (35.2) | 17 (41.5) | 8 (26.7) | 0.197 |
| Disease severity | ||||
| SOFA ≥ 4 (n, %) | 17 (23.9) | 12 (29.2) | 5 (16.7) | 0.219 |
| Underlying disease | ||||
| Atopic dermatitis (n, %) | 13 (18.3) | 8 (19.5) | 5 (16.7) | 0.759 |
| Diabetes mellitus (n, %) | 24 (33.8) | 14 (34.2) | 10 (33.3) | 0.943 |
| Hemodialysis (n, %) | 8 (11.3) | 3 (7.3) | 5 (16.7) | 0.269 |
| Cardiovascular disease (n, %) | 20 (28.2) | 11 (26.8) | 9 (30.0) | 0.769 |
| Cerebrovascular disease (n, %) | 20 (28.2) | 13 (31.7) | 7 (23.3) | 0.438 |
| Pulmonary disease (n, %) | 8 (11.3) | 3 (7.3) | 5 (16.7) | 0.269 |
| Renal dysfunction (n, %) | 21 (29.6) | 13 (31.7) | 8 (26.7) | 0.645 |
| Solid tumor (n, %) | 15 (21.1) | 6 (14.6) | 9 (30) | 0.117 |
| Hematological malignancy (n, %) | 3 (4.2) | 1 (2.4) | 2 (6.7) | 0.569 |
| Autoimmune disease (n, %) | 3 (4.2) | 3 (7.3) | 0 (0.0) | 0.257 |
| Under chemotherapy (n, %) | 4 (5.6) | 1 (2.4) | 3 (10.0) | 0.303 |
| Immunosuppressant (n, %) | 10 (14.1) | 6 (14.6) | 4 (13.3) | 0.876 |
| Charlson Comorbidity Index ≥ 4 (n, %) | 25 (35.2) | 13 (31.7) | 12 (40) | 0.470 |
| Laboratory data (mean ± SD) | ||||
| White blood cell (μL) | 13,697 ± 6707 | 14,356.1 ± 1048.1 | 12,796.7 ± 1225.3 | 0.336 |
| C-reactive protein (mg/dL) | 16.0 ± 9.2 | 16.9 ± 1.4 | 14.7 ± 1.7 | 0.324 |
| Creatinine (U/L) | 1.6 ± 2.2 | 1.8 ± 0.3 | 1.4 ± 0.4 | 0.549 |
| Albumin (g/dL) | 2.8 ± 0.6 | 2.7 ± 0.1 | 2.9 ± 0.1 | 0.325 |
| Primary site of infection (n, %) | ||||
| Primary bacteremia (entry sites were unknown) | 25 (35.2) | 13 (31.7) | 12 (40) | 0.469 |
| Secondary bacteremia | ||||
| Catheter-associated bloodstream infection | 14 (19.7) | 7 (17.1) | 7 (23.3) | 0.512 |
| Skin and soft tissue infection | 13 (18.3) | 7 (17.1) | 6 (20) | 0.752 |
| Urinary tract infection | 4 (5.6) | 2 (4.9) | 2 (6.7) | 0.746 |
| Infective endocarditis | 3 (4.2) | 2 (4.9) | 1 (3.3) | 0.749 |
| Pneumonia | 4 (5.6) | 4 (9.8) | 0 (0.0) | 0.132 |
| Cholangitis | 1 (1.4) | 1 (2.4) | 0 (0.0) | 1.000 |
| Iliopsoas muscle abscess | 2 (2.8) | 2 (4.9) | 0 (0.0) | 0.505 |
| Shunt infection | 2 (2.8) | 2 (4.9) | 0 (0.0) | 0.505 |
| Subcutaneous abscess | 1 (1.4) | 1 (2.4) | 0 (0.0) | 1.000 |
| Spondylitis | 1 (1.4) | 0 (0.0) | 1 (3.3) | 0.422 |
| Surgical site infection | 1 (1.4) | 0 (0.0) | 1 (3.3) | 0.422 |
| Metastatic infection | 9 (12.7) | 6 (14.6) | 3 (10) | 0.724 |
| Follow-up two sets of blood culture (n, %) | 54 (76.1) | 30 (73.2) | 24 (80) | 0.505 |
| Continuous positive blood culture for > 7 days (n, %) | 4 (5.6) | 2 (4.8) | 2 (6.7) | 0.746 |
| Duration of antibiotic treatment (mean ± SD) | 29.1 ± 47.4 | 33.5 ± 6.9 | 23.5 ± 8.1 | 0.351 |
| Duration of intravenous treatment (mean ± SD) | 17.2 ± 10.7 | 18.2 ± 1.7 | 17.0 ± 2.0 | 0.630 |
| Length of hospital stay of community-acquired MSSA infection (mean ± SD) | 36.4 ± 60.9 | 47.4 ± 10.3 | 28.3 ± 13.6 | 0.270 |
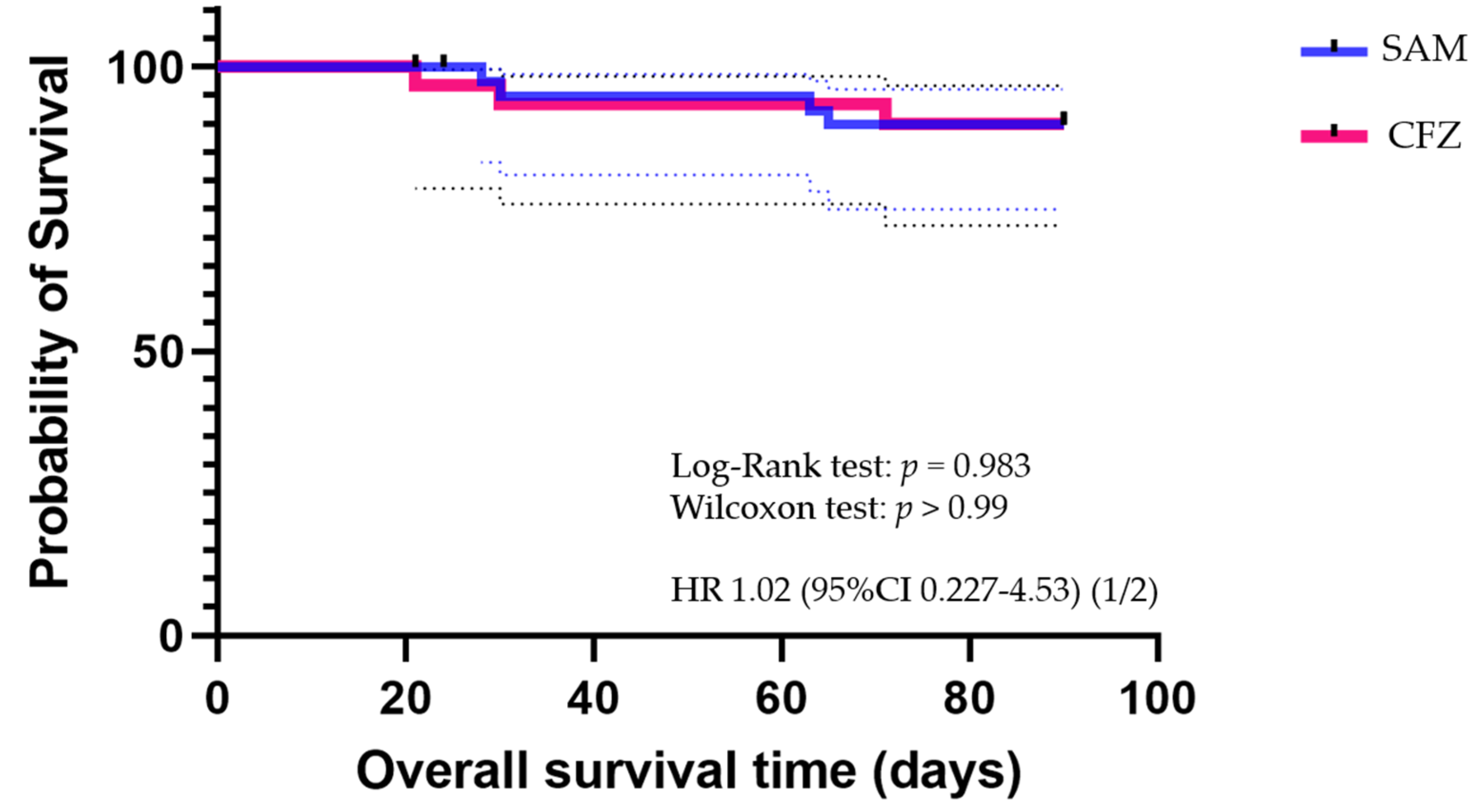
| All-cause 30-day mortality (n, %) | 6 (8.5) | 4 (9.7) | 2 (6.6) | 0.643 |
| Initial Antimicrobial Agents | All Patients (n, %) | SAM (n, %) | CFZ (n, %) | p-Value |
|---|---|---|---|---|
| N = 71 | N = 41 | N = 30 | ||
| Ampicillin/sulbactam | 14 (19.7) | 11 (26.8) | 3 (10.0) | 0.129 |
| Piperacillin/tazobactam | 12 (17.0) | 7 (17.1) | 5 (16.7) | 0.964 |
| Cefazolin | 5 (7.0) | 0 (0.0) | 5 (16.7) | 0.010 |
| Cefmetazole | 1 (1.4) | 1 (2.4) | 0 (0.0) | 1.000 |
| Ceftriaxone | 11 (15.5) | 7 (17.1) | 4 (13.3) | 0.749 |
| Cefozopran/sulbactam | 1 (1.4) | 1 (2.4) | 0 (0.0) | 1.000 |
| Cefepime | 1 (1.4) | 1 (2.4) | 0 (0.0) | 1.000 |
| Doripenem | 1 (1.4) | 1 (2.4) | 0 (0.0) | 1.000 |
| Meropenem | 8 (11.3) | 3 (7.3) | 5 (16.7) | 0.269 |
| Vancomycin | 8 (11.3) | 5 (12.2) | 3 (10.0) | 1.000 |
| Teicoplanin | 4 (5.6) | 3 (7.3) | 1 (3.3) | 0.632 |
| Daptomycin | 4 (5.6) | 1 (2.4) | 3 (10.0) | 0.303 |
| Levofloxacin | 1 (1.4) | 0 (0.0) | 1 (3.3) | 0.422 |
| Variables | All Patients | SAM | CFZ | p-Value |
|---|---|---|---|---|
| N = 71 | N = 41 | N = 30 | ||
| None (n, %) | 49 (69.0) | 24 (58.5) | 25 (83.3) | 0.026 |
| Diarrhea (n, %) | 7 (9.8) | 6 (14.6) | 1 (3.3) | 0.115 |
| Elevated eosinocyte levels (n, %) | 4 (5.6) | 2 (4.8) | 2 (6.6) | 0.747 |
| Drug rush (n, %) | 4 (5.6) | 3 (7.3) | 1 (3.3) | 0.472 |
| Liver dysfunction (n, %) | 13 (18.3) | 11 (26.8) | 2 (6.6) | 0.030 |
| Thrombopenia (n, %) | 1 (1.4) | 0 | 1 (3.3) | 0.239 |
| Complicated CDI | 0 | 0 | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirai, J.; Asai, N.; Hagihara, M.; Kishino, T.; Kato, H.; Sakanashi, D.; Ohashi, W.; Mikamo, H. Comparative Effectiveness of Ampicillin/Sulbactam versus Cefazolin as Targeted Therapy for Bacteremia Caused by Beta-Lactamase-Producing Methicillin-Sensitive Staphylococcus aureus: A Single-Center Retrospective Study. Antibiotics 2022, 11, 1505. https://doi.org/10.3390/antibiotics11111505
Hirai J, Asai N, Hagihara M, Kishino T, Kato H, Sakanashi D, Ohashi W, Mikamo H. Comparative Effectiveness of Ampicillin/Sulbactam versus Cefazolin as Targeted Therapy for Bacteremia Caused by Beta-Lactamase-Producing Methicillin-Sensitive Staphylococcus aureus: A Single-Center Retrospective Study. Antibiotics. 2022; 11(11):1505. https://doi.org/10.3390/antibiotics11111505
Chicago/Turabian StyleHirai, Jun, Nobuhiro Asai, Mao Hagihara, Takaaki Kishino, Hideo Kato, Daisuke Sakanashi, Wataru Ohashi, and Hiroshige Mikamo. 2022. "Comparative Effectiveness of Ampicillin/Sulbactam versus Cefazolin as Targeted Therapy for Bacteremia Caused by Beta-Lactamase-Producing Methicillin-Sensitive Staphylococcus aureus: A Single-Center Retrospective Study" Antibiotics 11, no. 11: 1505. https://doi.org/10.3390/antibiotics11111505
APA StyleHirai, J., Asai, N., Hagihara, M., Kishino, T., Kato, H., Sakanashi, D., Ohashi, W., & Mikamo, H. (2022). Comparative Effectiveness of Ampicillin/Sulbactam versus Cefazolin as Targeted Therapy for Bacteremia Caused by Beta-Lactamase-Producing Methicillin-Sensitive Staphylococcus aureus: A Single-Center Retrospective Study. Antibiotics, 11(11), 1505. https://doi.org/10.3390/antibiotics11111505