
Variations in Antibiotic Use and Sepsis Management in Neonatal Intensive Care Units: A European Survey

 ,
,  ,
,  , ,
, ,  and
and
Abstract
1. Introduction
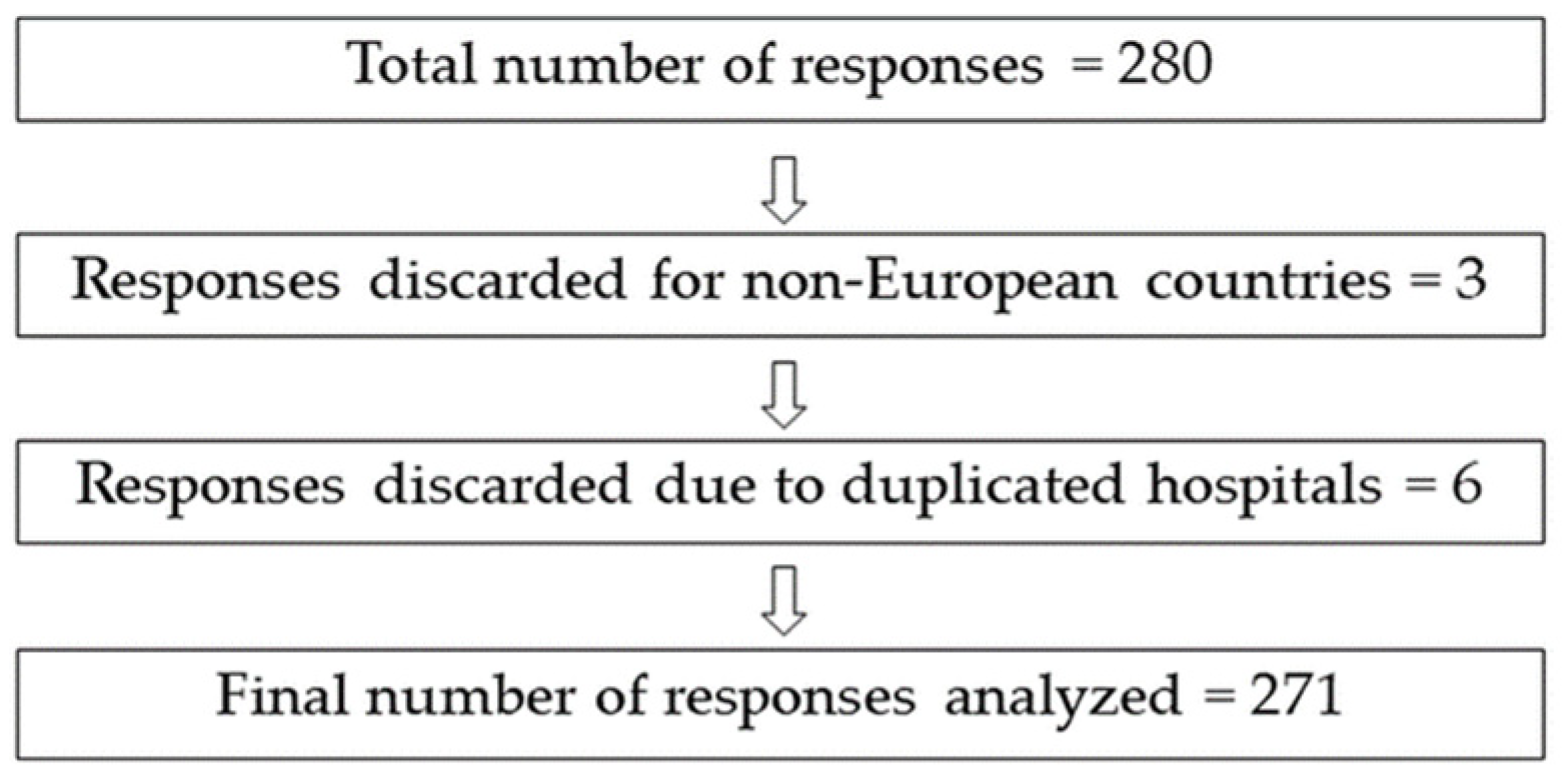
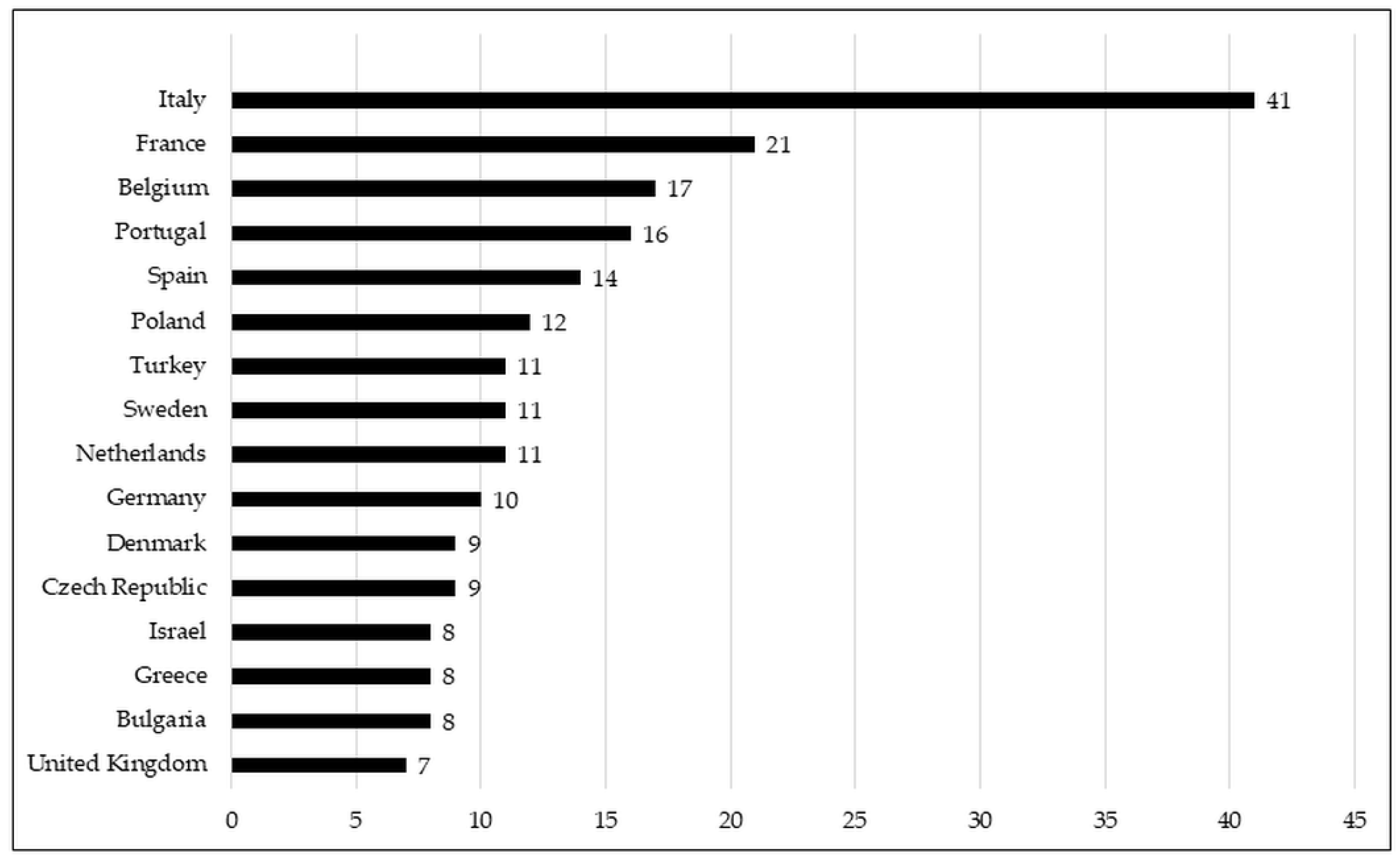
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McMullan, B.; Cooper, C.; Spotswood, N.; James, R.; Jones, C.; Konecny, P.; Blyth, C.; Karen, T. Antibiotic prescribing in neonatal sepsis: An Australian nationwide survey. BMJ Paediatr. Open 2020, 4, e000643. [Google Scholar] [CrossRef]
- St Clair, N.E.; Batra, M.; Kuzminski, J.; Lee, A.C.; O’Callahan, C. Global challenges, efforts, and controversies in neonatal care. Clin. Perinatol. 2014, 41, 749–772. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Reichert, F.; Cassini, A.; Horner, R.; Harder, T.; Markwart, R.; Tröndle, M.; Savova, Y.; Kissoon, N.; Schlattmann, P. Global incidence and mortality of neonatal sepsis: A systematic review and meta-analysis. Arch. Dis. Child. 2021, 106, 1–8. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Fleischmann-Struzek, C.; Goldfarb, D.M.; Schlattmann, P.; Schlapbach, L.J.; Reinhart, K.; Kissoon, N. The global burden of paediatric and neonatal sepsis: A systematic review. Lancet Respir. Med. 2018, 6, 223–230. [Google Scholar] [CrossRef]
- Edmond, K.M.; Kortsalioudaki, C.; Scott, S.; Schrag, S.J.; Zaidi, A.K.M.; Cousens, S.; Heath, P.T. Group B streptococcal disease in infants aged younger than 3 months: Systematic review and meta-analysis. Lancet 2012, 379, 547–556. [Google Scholar] [CrossRef]
- Al-Taiar, A.; Hammoud, M.S.; Cuiqing, L.; Lee, J.K.; Lui, K.-M.; Nakwan, N.; Isaacs, D. Neonatal infections in China, Malaysia, Hong Kong and Thailand. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F249–F255. [Google Scholar] [CrossRef]
- Trijbels-Smeulders, M.; de Jonge, G.A.; Pasker-de Jong, P.; Gerards, L.J.; Adriaanse, A.H.; van Lingen, R.A.; Kollée, L. Epidemiology of neonatal group B streptococcal disease in The Netherlands before and after introduction of guidelines for prevention. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F271–F276. [Google Scholar] [CrossRef]
- Van Herk, W.; Stocker, M.; van Rossum, A.M. Recognising early onset neonatal sepsis: An essential step in appropriate antimicrobial use. J. Infect. 2016, 72, S77–S82. [Google Scholar] [CrossRef]
- Giannoni, E.; Agyeman, P.K.A.; Stocker, M.; Posfay-Barbe, K.M.; Heininger, U.; Spycher, B.D.; Bernhard-Stirnemann, S.; Niederer-Loher, A.; Kahlert, C.R.; Donas, A.; et al. Neonatal Sepsis of Early Onset, and Hospital-Acquired and Community-Acquired Late Onset: A Prospective Population-Based Cohort Study. J. Pediatr. 2018, 201, 106–114.e4. [Google Scholar] [CrossRef]
- Chirico, G.; Loda, C. Laboratory aid to the diagnosis and therapy of infection in the neonate. Pediatr. Rep. 2011, 3, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sola, A. Abuse of antibiotics in perinatology: Negative impact for health and the economy. NeoReviews 2020, 21, e559–e570. [Google Scholar] [CrossRef] [PubMed]
- Cantey, J.B.; Pyle, A.K.; Wozniak, P.S.; Hynan, L.S.; Sanchez, P.J. Early Antibiotic Exposure and Adverse Outcomes in Preterm, Very Low Birth Weight Infants. J. Pediatr. 2018, 203, 62–67. [Google Scholar] [CrossRef]
- Goel, N.; Shrestha, S.; Smith, R.; Mehta, A.; Ketty, M.; Muxworthy, H.; Abelian, A.; Kirupaalar, V.; Saeed, S.; Jain, S. Screening for early onset neonatal sepsis: NICE guidance-based practice versus projected application of the Kaiser Permanente sepsis risk calculator in the UK population. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 105, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Kuzniewicz, M.W.; Puopolo, K.M.; Fischer, A.; Walsh, E.M.; Li, S.; Newman, T.B.; Kipnis, P.; Escobar, G.J. A quantitative, risk-based approach to the management of neonatal early-onset sepsis. JAMA Pediatr. 2017, 171, 365–371. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Draper, D.; Wi, S.; Newman, T.B.; Zupancic, J.; Lieberman, E.; Smith, M.; Escobar, G.J. Estimating the probability of neonatal early-onset infection on the basis of maternal risk factors. Pediatrics 2011, 128, e1155–e1163. [Google Scholar] [CrossRef]
- Achten, N.B.; Dorigo-Zetsma, J.W.; Van Der Linden, P.D.; Van Brakel, M.; Plötz, F.B. Sepsis calculator implementation reduces empiric antibiotics for suspected early-onset sepsis. Eur. J. Pediatr. 2018, 177, 741–746. [Google Scholar] [CrossRef]
- Pettinger, K.J.; Mayers, K.; McKechnie, L.; Phillips, B. Sensitivity of the Kaiser Permanente early-onset sepsis calculator: A systematic review and meta-analysis. EClinicalMedicine 2020, 19, 100227. [Google Scholar] [CrossRef]
- Patel, S.J.; Saiman, L. Principles and strategies of antimicrobial stewardship in the neonatal intensive care unit. Semin. Perinatol. 2012, 36, 431–436. [Google Scholar] [CrossRef]
- Ramasethu, J.; Kawakita, T. Antibiotic stewardship in perinatal and neonatal care. Semin. Fetal Neonatal Med. 2017, 22, 278–283. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.; Sengupta, S.; Puopolo, K.M. Challenges and opportunities for antibiotic stewardship among preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F327–F332. [Google Scholar] [CrossRef]
- Ho, T.; Buus-Frank, M.E.; Edwards, E.M.; Morrow, K.A.; Ferrelli, K.; Srinivasan, A.; Pollock, D.A.; Dukhovny, D.; Zupancic, J.A.; Pursley, D.M. Adherence of newborn-specific antibiotic stewardship programs to CDC recommendations. Pediatrics 2018, 142, e20174322. [Google Scholar] [CrossRef]
- Litz, J.E.; Goedicke-Fritz, S.; Härtel, C.; Zemlin, M.; Simon, A. Management of early-and late-onset sepsis: Results from a survey in 80 German NICUs. Infection 2019, 47, 557–564. [Google Scholar] [CrossRef]
- Joshi, P.; Barr, P. The use of lumbar puncture and laboratory tests for sepsis by Australian neonatologists. J. Paediatr. Child. Health 1998, 34, 74–78. [Google Scholar] [CrossRef]
- Pandolfini, C.; Kaguelidou, F.; Sequi, M.; Jacqz-Aigrain, E.; Choonara, I.; Turner, M.A.; Manzoni, P.; Bonati, M. Wide intra- and inter-country variability in drug use and dosage in very-low-birth-weight newborns with severe infections. Eur. J. Clin. Pharmacol. 2013, 69, 1031–1036. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Metsvaht, T.; Nellis, G.; Varendi, H.; Nunn, A.J.; Graham, S.; Rieutord, A.; Storme, T.; McElnay, J.; Mulla, H.; Turner, M.A.; et al. High variability in the dosing of commonly used antibiotics revealed by a Europe-wide point prevalence study: Implications for research and dissemination. BMC Pediatr. 2015, 15, 41. [Google Scholar] [CrossRef] [PubMed]
- Spyridis, N.; Syridou, G.; Goossens, H.; Versporten, A.; Kopsidas, J.; Kourlaba, G.; Bielicki, J.; Drapier, N.; Zaoutis, T.; Tsolia, M.; et al. Variation in paediatric hospital antibiotic guidelines in Europe. Arch. Dis. Child. 2016, 101, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Van Reempts, P.; Gortner, L.; Milligan, D.; Cuttini, M.; Petrou, S.; Agostino, R.; Field, D.; Den Ouden, L.; Børch, K.; Mazela, J. Characteristics of neonatal units that care for very preterm infants in Europe: Results from the MOSAIC study. Pediatrics 2007, 120, e815–e825. [Google Scholar] [CrossRef] [PubMed]
- Kaguelidou, F.; Pandolfini, C.; Manzoni, P.; Choonara, I.; Bonati, M.; Jacqz-Aigrain, E. European survey on the use of prophylactic fluconazole in neonatal intensive care units. Eur. J. Pediatr. 2012, 171, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Huizing, M.J.; Villamor-Martínez, E.; Vento, M.; Villamor, E. Pulse oximeter saturation target limits for preterm infants: A survey among European neonatal intensive care units. Eur. J. Pediatr. 2017, 176, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Suryawanshi, S.; Pandit, V.; Suryawanshi, P.; Panditrao, A. Antibiotic prescribing pattern in a tertiary level neonatal intensive care unit. J. Clin. Diagn. Res. 2015, 9, FC21–FC24. [Google Scholar] [CrossRef]
- WHO. Pocket Book of Hospital Care for Children: Guidelines for the Management of Common Childhood Illnesses, 2nd ed.; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Obiero, C.W.; Seale, A.C.; Berkley, J.A. Empiric Treatment of Neonatal Sepsis in Developing Countries. Pediatr. Infect. Dis. J. 2015, 34, 659–661. [Google Scholar] [CrossRef]
- Liem, T.Y.; Krediet, T.G.; Fleer, A.; Egberts, T.C.; Rademaker, C.M. Variation in antibiotic use in neonatal intensive care units in The Netherlands. J. Antimicrob. Chemother. 2010, 65, 1270–1275. [Google Scholar] [CrossRef] [PubMed]
- Benitz, W.E.; Achten, N.B. Technical assessment of the neonatal early-onset sepsis risk calculator. Lancet Infect. Dis. 2020, 21, e134–e140. [Google Scholar] [CrossRef]
- Kuzniewicz, M.W.; Walsh, E.M.; Li, S.; Fischer, A.; Escobar, G.J. Development and implementation of an early-onset sepsis calculator to guide antibiotic management in late preterm and term neonates. Jt. Comm. J. Qual. Patient Saf. 2016, 42, 232–239. [Google Scholar] [CrossRef]
- Leroux, S.; Zhao, W.; Bétrémieux, P.; Pladys, P.; Saliba, E.; Jacqz-Aigrain, E. Therapeutic guidelines for prescribing antibiotics in neonates should be evidence-based: A French national survey. Arch. Dis. Child. 2015, 100, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Young, T.E.; Mangum, B. Neofax; Thomson Reuters: Toronto, ON, Canada, 2020. [Google Scholar]
- Ahmed, A.M.; Mohammed, A.T.; Bastawy, S.; Attalla, H.A.; Yousef, A.A.; Abdelrazek, M.S.; Alkomos, M.F.; Ghareeb, A. Serum biomarkers for the early detection of the early-onset neonatal sepsis: A single-center prospective study. Adv. Neonatal Care 2019, 19, E26–E32. [Google Scholar] [CrossRef]
- Bellos, I.; Fitrou, G.; Pergialiotis, V.; Thomakos, N.; Perrea, D.N.; Daskalakis, G. The diagnostic accuracy of presepsin in neonatal sepsis: A meta-analysis. Eur. J. Pediatr. 2018, 177, 625–632. [Google Scholar] [CrossRef]
- Glaser, M.A.; Hughes, L.M.; Jnah, A.; Newberry, D.; Harris-Haman, P.A. Neonatal Sepsis: A Review of Pathophysiology and Current Management Strategies. Adv. Neonatal Care 2021, 21, 49–60. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Benitz, W.E.; Zaoutis, T.E.; Committee on Infectious Diseases. Management of neonates born at ≤34 6/7 weeks’ gestation with suspected or proven early-onset bacterial sepsis. Pediatrics 2018, 142, e20182896. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Benitz, W.E.; Zaoutis, T.E.; Committee on Infectious Diseases. Management of neonates born at ≥35 0/7 weeks’ gestation with suspected or proven early-onset bacterial sepsis. Pediatrics 2018, 142, e20182894. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.; Sánchez, P.; Stoll, B. Sepsis neonatal. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Simonsen, K.; Anderson-Berry, A.; Delair, S.; Davies, D. Sepsis neonatal de inicio temprano. Revis. Clín. Microbiol. 2016, 27, 21–47. [Google Scholar] [CrossRef]
- Tzialla, C.; Manzoni, P.; Achille, C.; Bollani, L.; Stronati, M.; Borghesi, A. New diagnostic possibilities for neonatal sepsis. Am. J. Perinatol. 2018, 35, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Pietrasanta, C.; Ronchi, A.; Vener, C.; Poggi, C.; Ballerini, C.; Testa, L.; Colombo, R.M.; Spada, E.; Dani, C.; Mosca, F. Presepsin (Soluble CD14 Subtype) as an Early Marker of Neonatal Sepsis and Septic Shock: A Prospective Diagnostic Trial. Antibiotics 2021, 10, 580. [Google Scholar] [CrossRef]
- Kurul, Ş.; Simons, S.H.; Ramakers, C.R.; De Rijke, Y.B.; Kornelisse, R.F.; Reiss, I.K.; Taal, H.R. Association of inflammatory biomarkers with subsequent clinical course in suspected late onset sepsis in preterm neonates. Crit. Care 2021, 25, 1–10. [Google Scholar] [CrossRef]
- Hasperhoven, G.; Al-Nasiry, S.; Bekker, V.; Villamor, E.; Kramer, B. Universal screening versus risk-based protocols for antibiotic prophylaxis during childbirth to prevent early-onset Group B streptococcal disease: A systematic review and meta-analysis. BJOG 2020, 127, 680–691. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.; Brocklehurst, P.; Steer, P.; Heath, P. Stenson BM on behalf of the Royal College of Obstetricians and Gynaecologists. Prevention of early-onset neonatal group B streptococcal disease. Green-top guideline no. 36. BJOG 2017, 124, e280–e305. [Google Scholar]
- Kolkman, D.G.; Fleuren, M.A.; Wouters, M.G.; de Groot, C.J.; Rijnders, M.E. Barriers and facilitators related to the uptake of four strategies to prevent neonatal early-onset group B haemolytic streptococcus disease: A qualitative study. BMC Pregnancy Childbirth 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Brown, A.P.; Denison, F.C. Selective or universal screening for GBS in pregnancy. Early Hum. Dev. 2018, 126, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Colomer, B.F.; Badia, M.C.; Cotallo, D.C.; Sastre, J.L.; Network, G.C. The Spanish National Network “Grupo Castrillo”: 22 Years of Nationwide Neonatal Infection Surveillance. Am. J. Perinatol. 2020, 37, S71–S75. [Google Scholar]
- Bedetti, L.; Marrozzini, L.; Baraldi, A.; Spezia, E.; Iughetti, L.; Lucaccioni, L.; Berardi, A. Pitfalls in the diagnosis of meningitis in neonates and young infants: The role of lumbar puncture. J. Matern. Fetal Neonatal Med. 2019, 32, 4029–4035. [Google Scholar] [CrossRef] [PubMed]
- Meadows, K.A. So you want to do research? 5: Questionnaire design. Br. J. Community Nurs. 2003, 8, 562–570. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) | |
|---|---|
Level of care of NICUs, n. (%)
| |
| 6 (2.2%) | |
| 44 (16.2%) | |
| 106 (39.1%) | |
| 102 (37.6%) | |
| 13 (4.8%) | |
| Care of premature newborns under 28 weeks until discharge, n. (%) | |
| 226 (83.4%) 45 (16.6%) |
| Neonatal admissions in 2020, median (IQR) | 444 (273; 864) |
| Number of admissions of babies < 1500 g in 2020, n. (%) | |
| 76 (28%) 64 (23.6%) 131 (48.3%) |
| Intensive care incubators in the NICU, median (IQR) | 2 (8; 21) |
| EOS n (%) | LOS n (%) | NEC n (%) | |
|---|---|---|---|
| Penicillin | 62 (22.9%) | 9 (3.3%) | 6 (2.2%) |
| Ampicillin | 204 (75.3%) | 38 (14%) | 58 (21.4%) |
| Gentamicin | 208 (76.8%) | 92 (33.9%) | 96 (35.4%) |
| Tobramycin | 6 (2.2%) | 2 (0.7%) | 4 (1.5%) |
| Amikacin | 45 (16.6%) | 86 (31.7%) | 60 (22.1%) |
| Cefotaxime | 13 (4.8%) | 76 (28%) | 44 (16.2%) |
| Ceftazidime | 2 (0.7%) | 17 (6.3%) | 15 (5.5%) |
| Meropenem | 2 (0.7%) | 42 (15.5%) | 64 (23.6%) |
| Vancomycin | 1 (0.4%) | 142 (52.4%) | 107 (39.5%) |
| Nafcililin | 0 (0%) | 0 (0%) | 0 (0%) |
| Metronidazole | 0 (0%) | 1 (0.4%) | 140 (51.7%) |
| Piperacillin-tazobactam | 1 (0.4%) | 37 (13.7%) | 46 (17%) |
| Teicoplanin | 0 (0%) | 11 (4.1%) | 8 (3%) |
| Flucloxacillin | 0 (0%) | 23 (8.5%) | 3 (1.1%) |
| Oxacillin | 0 (0%) | 14 (5.2%) | 0 (0%) |
| For Diagnosis of Sepsis n (%) | To Stop Antibiotics n (%) | |
|---|---|---|
| C reactive protein | 264 (97.4%) | 238 (87.8%) |
| Procalcitonin | 135 (49.8%) | 79 (29.2%) |
| Cytokines | 31 (11.4%) | 7 (2.6%) |
| PCR base methods | 46 (17%) | 13 (4.8%) |
| DNA microarray-based methods | 12 (4.4%) | 6 (2.2%) |
| Blood culture | 258 (95.2%) | 209 (77.1%) |
| HeRo monitoring | 20 (7.4%) | 9 (3.3%) |
| Full blood count | 32 (11.8%) | 17 (6.3%) |
| Questions | Responses | |
|---|---|---|
| n | % | |
| I always perform a lumbar puncture if the newborn is clinically stable | 43 | 15.9 |
| I decide to perform a lumbar puncture based on the patients’ history, risk factors, clinical features | 191 | 70.5 |
| I decide to perform a lumbar puncture depending on blood markers (CRP, for example) | 62 | 22.9 |
| I decide to perform a lumbar puncture depending on the positivity or negativity of the blood culture | 94 | 34.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garrido, F.; Allegaert, K.; Arribas, C.; Villamor, E.; Raffaeli, G.; Paniagua, M.; Cavallaro, G.; on behalf of European Antibiotics Study Group (EASG). Variations in Antibiotic Use and Sepsis Management in Neonatal Intensive Care Units: A European Survey. Antibiotics 2021, 10, 1046. https://doi.org/10.3390/antibiotics10091046
Garrido F, Allegaert K, Arribas C, Villamor E, Raffaeli G, Paniagua M, Cavallaro G, on behalf of European Antibiotics Study Group (EASG). Variations in Antibiotic Use and Sepsis Management in Neonatal Intensive Care Units: A European Survey. Antibiotics. 2021; 10(9):1046. https://doi.org/10.3390/antibiotics10091046
Chicago/Turabian StyleGarrido, Felipe, Karel Allegaert, Cristina Arribas, Eduardo Villamor, Genny Raffaeli, Miren Paniagua, Giacomo Cavallaro, and on behalf of European Antibiotics Study Group (EASG). 2021. "Variations in Antibiotic Use and Sepsis Management in Neonatal Intensive Care Units: A European Survey" Antibiotics 10, no. 9: 1046. https://doi.org/10.3390/antibiotics10091046
APA StyleGarrido, F., Allegaert, K., Arribas, C., Villamor, E., Raffaeli, G., Paniagua, M., Cavallaro, G., & on behalf of European Antibiotics Study Group (EASG). (2021). Variations in Antibiotic Use and Sepsis Management in Neonatal Intensive Care Units: A European Survey. Antibiotics, 10(9), 1046. https://doi.org/10.3390/antibiotics10091046