
Correlation between Antibiotic Consumption and Resistance of Invasive Streptococcus pneumoniae


Abstract
:1. Introduction
2. Results
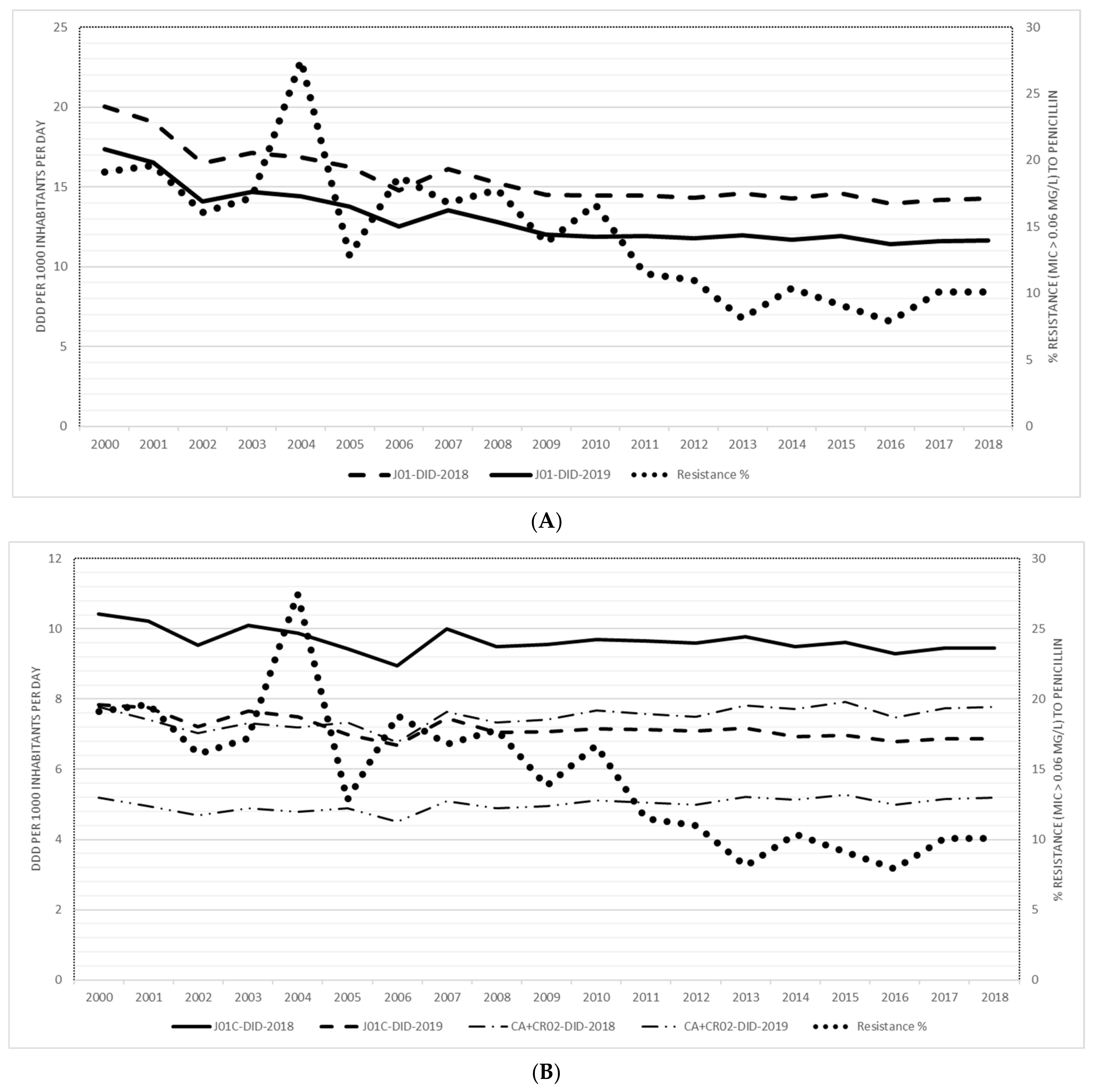
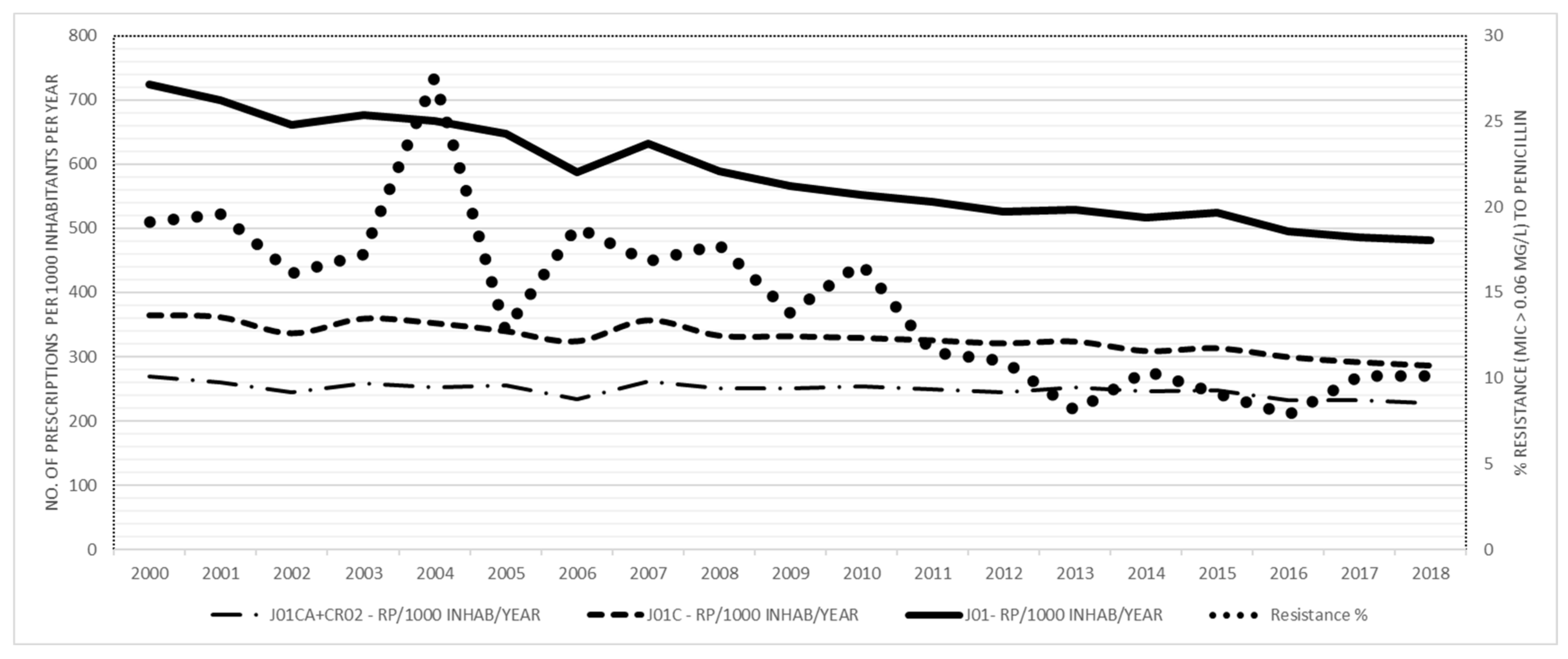
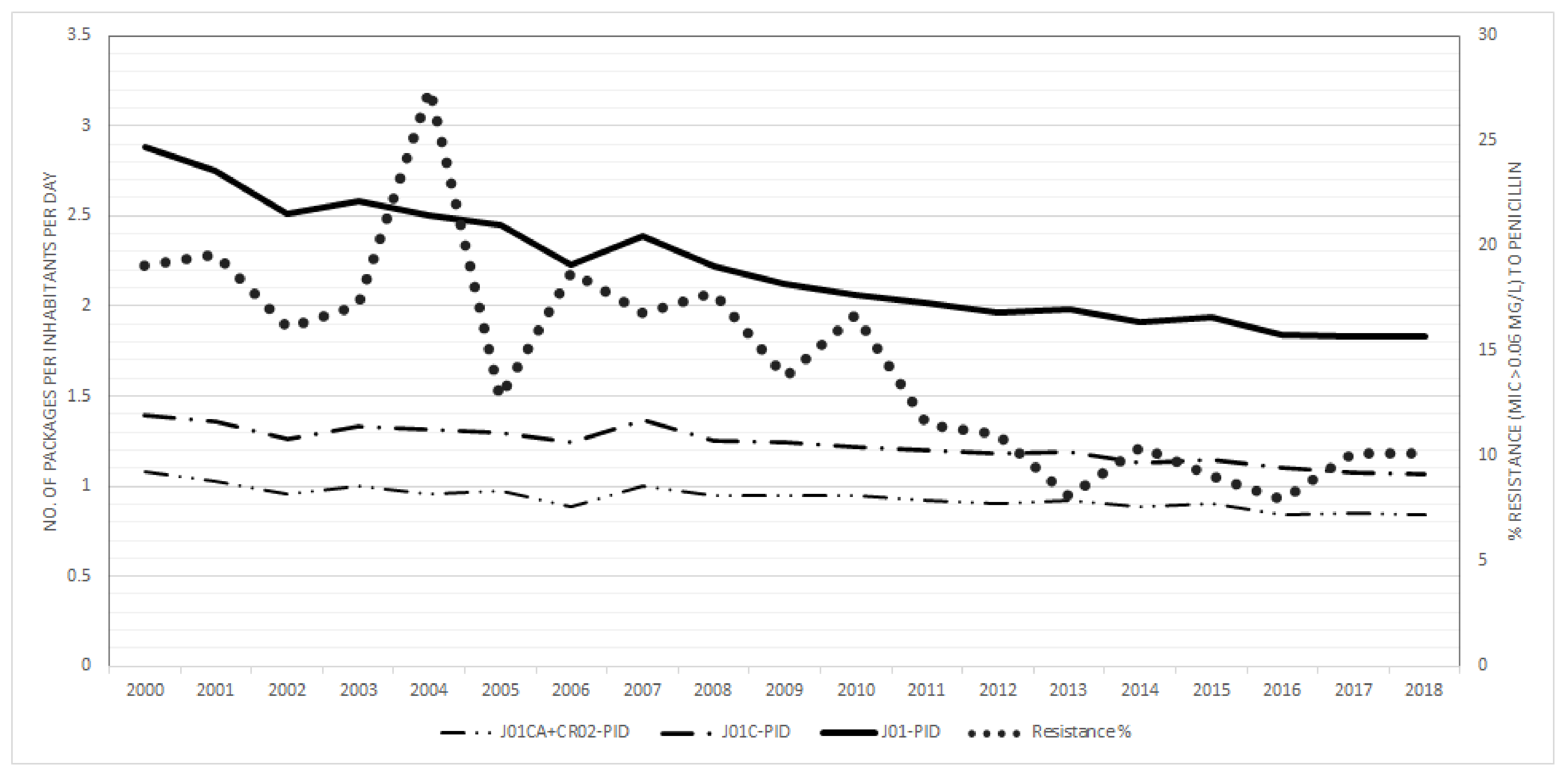
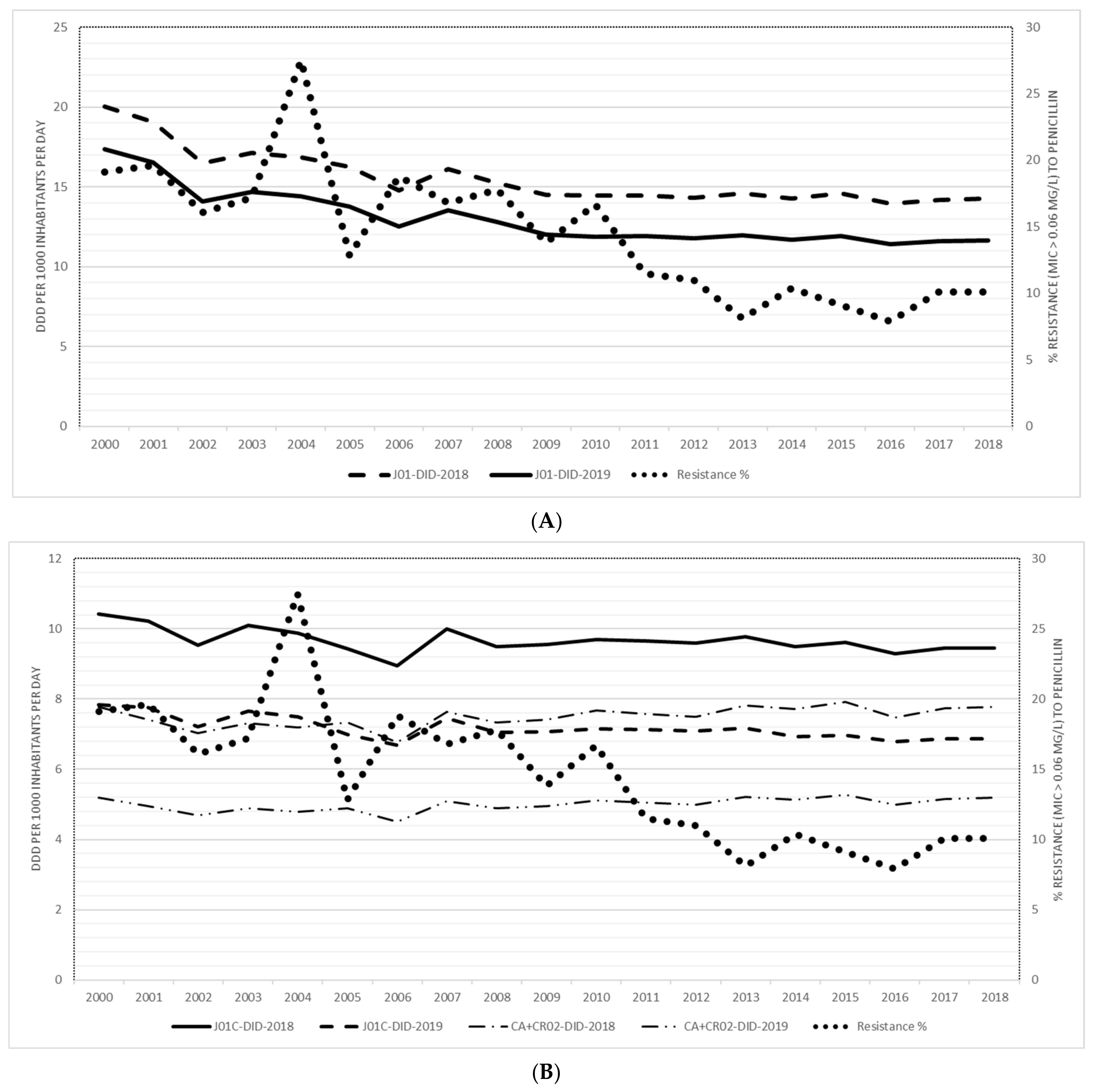
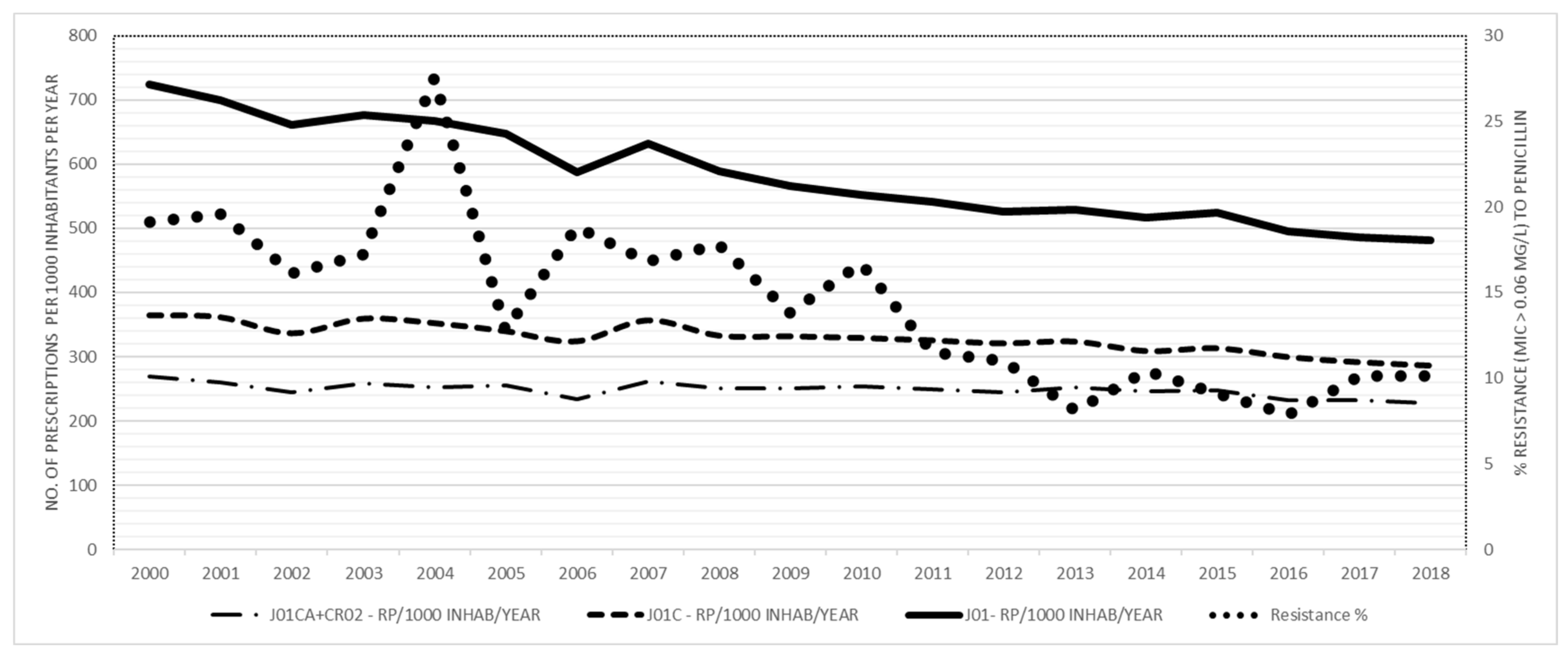
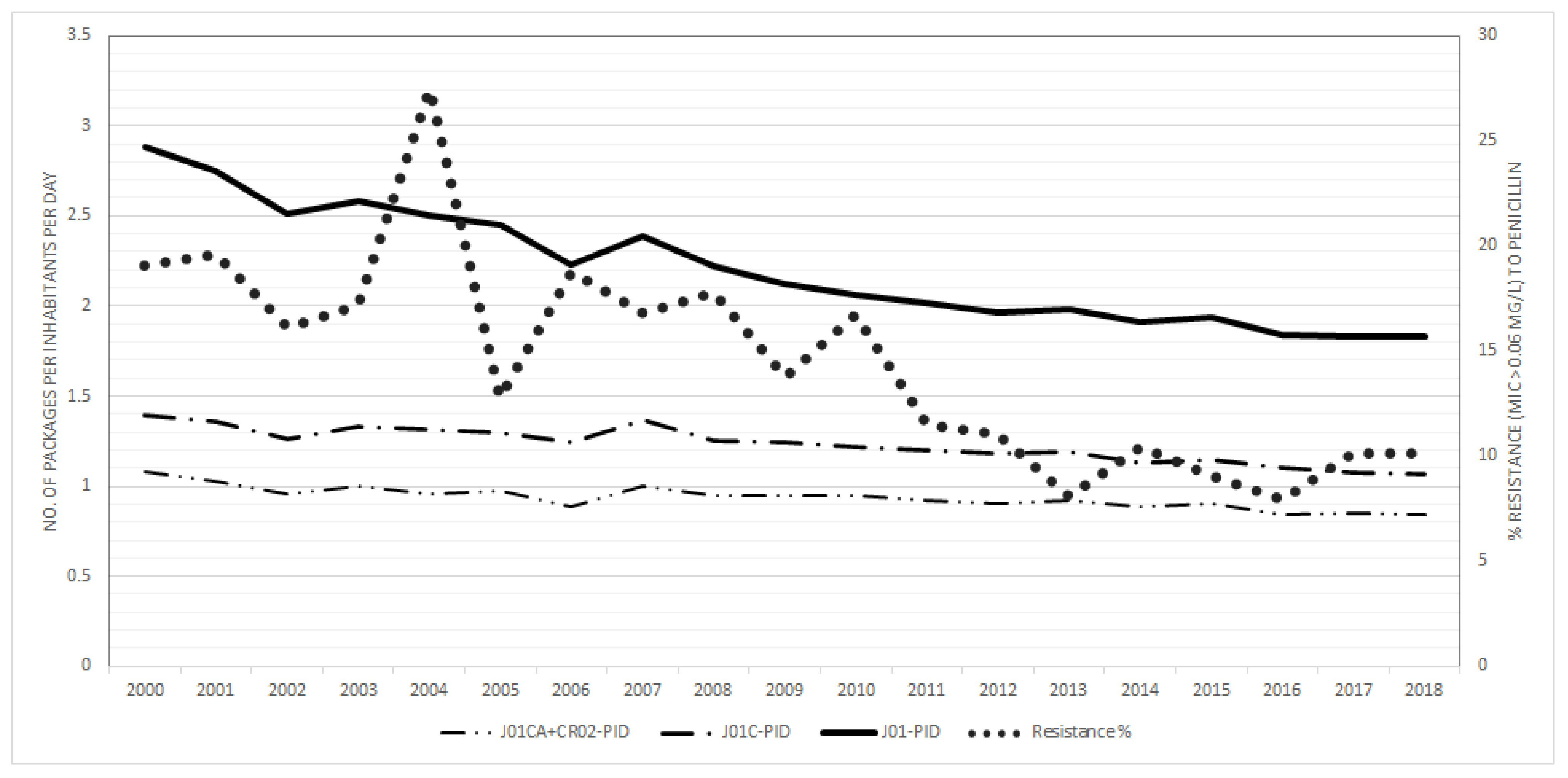
2.1. Consumption of Antibiotics and Resistance of Invasive S. pneumoniae to Penicillin
2.2. Correlation between Consumption of Total Antibiotics for Systemic Use (J01), Penicillins (J01C) and Broad-Spectrum Penicillins (J01 CA + J01 CR02) and Resistance of Invasive S. pneumoniae to Penicillin (Intermediate and Resistant)
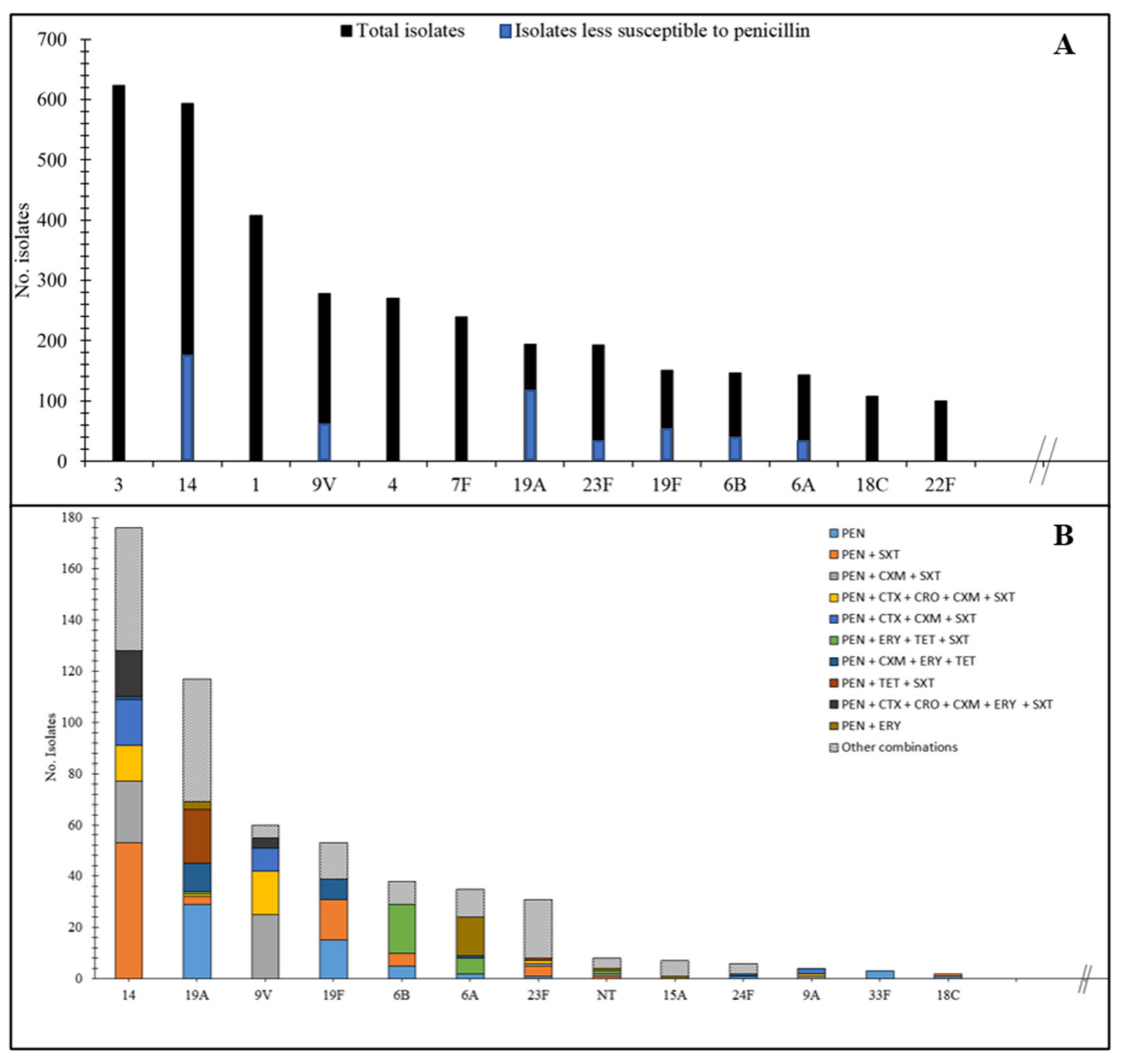
2.3. Resistance of Invasive S. pneumoniae to Penicillin and Co-resistance in Penicillin-resistant S. pneumoniae Isolates
3. Discussion
Limitations of the Study
4. Materials and methods
4.1. Collection of Isolates and Serotyping
4.2. Antibiotic Susceptibility Testing
4.3. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weiser, J.N.; Ferreira, D.M.; Paton, J.C. Streptococcus pneumoniae: Transmission, colonization and invasion. Nat. Rev. Microbiol. 2018, 16, 355–367. [Google Scholar] [CrossRef] [PubMed]
- WHO. Media Centre. News Release. WHO Publishes List of Bacteria for which New Antibiotics Are Urgently Needed. 2017. Available online: http://www.who.int/mediacentre/news/releases/2017/bacteria-antibiotics-needed/en/ (accessed on 15 March 2017).
- Hansman, D.; Bullen, M.M. A resistant pneumococcus. Lancet 1967, 290, 264–265. [Google Scholar] [CrossRef]
- Whitney, C.G.; Farley, M.M.; Hadler, J.; Harrison, L.H.; Bennett, N.M.; Lynfield, R.; Reingold, A.; Cieslak, P.R.; Pilishvili, T.; Jackson, D.; et al. Decline in Invasive Pneumococcal Disease after the Introduction of Protein–Polysaccharide Conjugate Vaccine. N. Engl. J. Med. 2003, 348, 1737–1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crook, D.W.M.; Spratt, B.G. Multiple antibiotic resistance in Streptococcus pneumoniae. Br. Med. Bull. 1998, 54, 595–610. [Google Scholar] [CrossRef] [Green Version]
- Yahiaoui, R.Y.; Heijer, C.D.J.D.; Van Bijnen, E.M.E.; Paget, W.J.; Pringle, M.; Goossens, H.; Bruggeman, A.C.; Schellevis, F.G.; Stobberingh, E.E.; The APRES Study Team. Prevalence and antibiotic resistance of commensal Streptococcus pneumoniaein nine European countries. Future Microbiol. 2016, 11, 737–744. [Google Scholar] [CrossRef] [Green Version]
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef] [Green Version]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albrich, W.C.; Monnet, D.L.; Harbarth, S. Antibiotic Selection Pressure and Resistance inStreptococcus pneumoniaeandStreptococcus pyogenes. Emerg. Infect. Dis. 2004, 10, 514–517. [Google Scholar] [CrossRef]
- Bronzwaer, S.L.; Cars, O.; Buchholz, U.; Mölstad, S.; Goettsch, W.G.; Veldhuijzen, I.K.; Kool, J.L.; Sprenger, M.J.; Degener, J.E.; European Antimicrobial Resistance Surveillance System. A European study on the relationship between antimicrobial use and antimicrobial resistance in Europe. Emerg. Infect. Dis. 2002, 8, 278–282. [Google Scholar] [CrossRef] [PubMed]
- García-Rey, C.; Aguilar, L.; Baquero, F.; Casal, J.; Dal-Ré, R. Importance of Local Variations in Antibiotic Consumption and Geographical Differences of Erythromycin and Penicillin Resistance in Streptococcus pneumoniae. J. Clin. Microbiol. 2002, 40, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Goossens, H.; Ferech, M.; Stichele, R.V.; Elseviers, M.; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Van De Sande-Bruinsma, N.; Grundmann, H.; Verloo, D.; Tiemersma, E.; Monen, J.; Goossens, H.; Ferech, M.; European Antimicrobial Resistance Surveillance System Group; European Surveillance of Antimicrobial Consumption Project Group. Antimicrobial Drug Use and Resistance in Europe. Emerg. Infect. Dis. 2008, 14, 1722–1730. [Google Scholar] [CrossRef] [PubMed]
- Olesen, S.W.; Barnett, M.L.; MacFadden, D.R.; Brownstein, J.S.; Hernández-Díaz, S.; Lipsitch, M.; Grad, Y.H. The distribution of antibiotic use and its association with antibiotic resistance. eLife 2018, 7, 39435. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborating Centre for Drug Statistics. Methodology, ATC Classification Index with DDDs 2019; WHO: Oslo, Norway, 2018. [Google Scholar]
- Statistical Office of the Republic of Slovenia. Population, Slovenija, 1. January 2019; Statistical Office of the Republic of Slovenia: Ljubljana, Slovenia, 2019. [Google Scholar]
- WHO Collaborating Centre for Drug Statistics. Methodology, ATC Classification In-Dex with DDDs 2018; WHO: Oslo, Norway, 2017. [Google Scholar]
- Fürst, J.; Čižman, M.; Mrak, J.; Kos, D.; Campbell, S.; Coenen, S.; Gustafsson, L.L.; Fürst, L.; Godman, B. The influence of a sustained multifaceted approach to improve antibiotic prescribing in Slovenia during the past decade: Findings and implications. Expert Rev. Anti Infective Ther. 2014, 13, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Cižman, M.; Srovin, T.P.; Beovič, B.; Vrdelja, M.; Bajec, T.; Blagus, R. European Antibiotic Awareness Day (EAAD): Any impact on antibiotic consumption and public awareness in Slovenia? J. Antimicrob. Chemother. 2018, 73, 2567–2572. [Google Scholar] [CrossRef] [PubMed]
- Čižman, M.; Paragi, M.; Jovan-Kuhar, N.; Gubina, M.; Oražem, A.; Pokorn, M. Antimicrobial Resistance of Invasive Streptococcus pneumoniae in Slovenia, 1993–1995. Scand. J. Infect. Dis. 1997, 29, 251–254. [Google Scholar] [CrossRef]
- Bruyndonckx, R.; Hens, N.; Aerts, M.; Goossens, H.; Abrahantes, J.C.; Coenen, S. Exploring the association between resistance and outpatient antibiotic use expressed as DDDs or packages. J. Antimicrob. Chemother. 2015, 70, 1241–1244. [Google Scholar] [CrossRef] [Green Version]
- Čižman, M. Measurement units for antibiotic consumption in outpatients. J. Antimicrob. Chemother. 2014, 69, 2877–2878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versporten, A.; Gyssens, I.C.; Pulcini, C.; Monnier, A.A.; Schouten, J.; Milanič, R.; Benić, M.S.; Tebano, G.; Le Maréchal, M.; Zanichelli, V.; et al. Metrics to assess the quantity of antibiotic use in the outpatient setting: A systematic review followed by an international multidisciplinary consensus procedure. J. Antimicrob. Chemother. 2018, 73, vi59–vi66. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Consumption in Europe—Annual Report of the European Antimicrobial Consumption Surveillance Network (ESAC-net) 2017. 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-consumption-annual-epidemiological-report-2017 (accessed on 15 March 2018).
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Consumption in Europe—Annual Report of the European Antimicrobial Consumption Surveillance Network (ESAC-net) 2018. 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2018 (accessed on 15 March 2019).
- Čižman, M. The use and resistance to antibiotics in the community. Int. J. Antimicrob. Agents 2003, 21, 297–307. [Google Scholar] [CrossRef]
- Enne, V.I. Reducing antimicrobial resistance in the community by restricting prescribing: Can it be done? J. Antimicrob. Chemother. 2009, 65, 179–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kastrin, T.; Paragi, M.; Erčulj, V.; Žohar Čretnik, T.; Slovenian Meningitidis Study Group; Bajec, T.; Čižman, M. Lack of correlation between reduced outpatient consumption of macrolides and macrolide resistance of invasive Streptococcus pneumoniae isolates in Slovenia during 1997–2017. J. Glob. Antimicrob. Resist. 2019, 16, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Richter, S.S.; Heilmann, K.P.; Dohrn, C.L.; Riahi, F.; Beekmann, S.E.; Doern, G.V. Changing Epidemiology of Antimicrobial-Resistant Streptococcus pneumoniae in the United States, 2004–2005. Clin. Infect. Dis. 2009, 48, e23–e33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sogstad, M.K.; Littauer, P.; Aaberge, I.S.; Caugant, D.A.; Høiby, E.A. Rapid Spread in Norway of an Erythromycin-Resistant Pneumococcal Clone, Despite Low Usage of Macrolides. Microb. Drug Resist. 2007, 13, 29–36. [Google Scholar] [CrossRef]
- Paragi, M.; Mioč, V.; Kastrin, T.; Žohar Čretnik, T. National laboratory surveillance of invasive pneumococcal diseases before and after the introduction of the vaccination into the national immunisation program in Slovenia. In Proceedings of the Kongres Mikrobiologa Srbije, Mikromed 2018 REGIO, Belgrade, Serbia, 10–12 May 2018; Udruženje Mikrobiologa Srbije: Belgrade, Serbia, 2018; p. 68. [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; 23th Informational Supplement; Clinical and Laboratory Standards Institute: Annapolis Junction, MD, USA, 2013. [Google Scholar]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 8.1. 2018. Available online: https://kaldur.landspitali.is/focal/gaedahandbaekur/gnhsykla.nsf/5e27f2e5a88c898e00256500003c98c2/815dc680f051520400257ab4003a3ba8/$FILE/Antifungal_breakpoints_v_8.1_March_2017.002.pdf/Antifungal_breakpoints_v_8.1_March_2017.pdf (accessed on 15 March 2017).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Consumption in the Population | Spearman’s rho2 Rank Correlation Coefficient | |||
|---|---|---|---|---|
| DID WHO 2018 | DID WHO 2019 | RxIDs | PIDs | |
| Total (J01) consumption vs resistance in total population | 0.78 *** | 0.80 *** | 0.86 *** | 0.85 *** |
| Consumption of beta-lactams, penicillins (J01C) | - | 0.59 ** | 0.82 *** | 0.84 *** |
| Consumption of extended spectrum penicillin (J01CA) and penicillin with β-lactamase inhibitors (CR02) | −0.58 ** | −0.57 * | 0.57 * | 0.72 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Čižman, M.; Mioč, V.; Bajec, T.; Paragi, M.; Kastrin, T.; Gonçalves, J. Correlation between Antibiotic Consumption and Resistance of Invasive Streptococcus pneumoniae. Antibiotics 2021, 10, 758. https://doi.org/10.3390/antibiotics10070758
Čižman M, Mioč V, Bajec T, Paragi M, Kastrin T, Gonçalves J. Correlation between Antibiotic Consumption and Resistance of Invasive Streptococcus pneumoniae. Antibiotics. 2021; 10(7):758. https://doi.org/10.3390/antibiotics10070758
Chicago/Turabian StyleČižman, Milan, Verica Mioč, Tom Bajec, Metka Paragi, Tamara Kastrin, and José Gonçalves. 2021. "Correlation between Antibiotic Consumption and Resistance of Invasive Streptococcus pneumoniae" Antibiotics 10, no. 7: 758. https://doi.org/10.3390/antibiotics10070758
APA StyleČižman, M., Mioč, V., Bajec, T., Paragi, M., Kastrin, T., & Gonçalves, J. (2021). Correlation between Antibiotic Consumption and Resistance of Invasive Streptococcus pneumoniae. Antibiotics, 10(7), 758. https://doi.org/10.3390/antibiotics10070758