
Stability and Compatibility Aspects of Drugs: The Case of Selected Cephalosporins

 ,
, 


Abstract
1. Introduction
2. Results
2.1. Stability of CFE and CFU in Parenteral Infusion Fluids and PN Admixtures
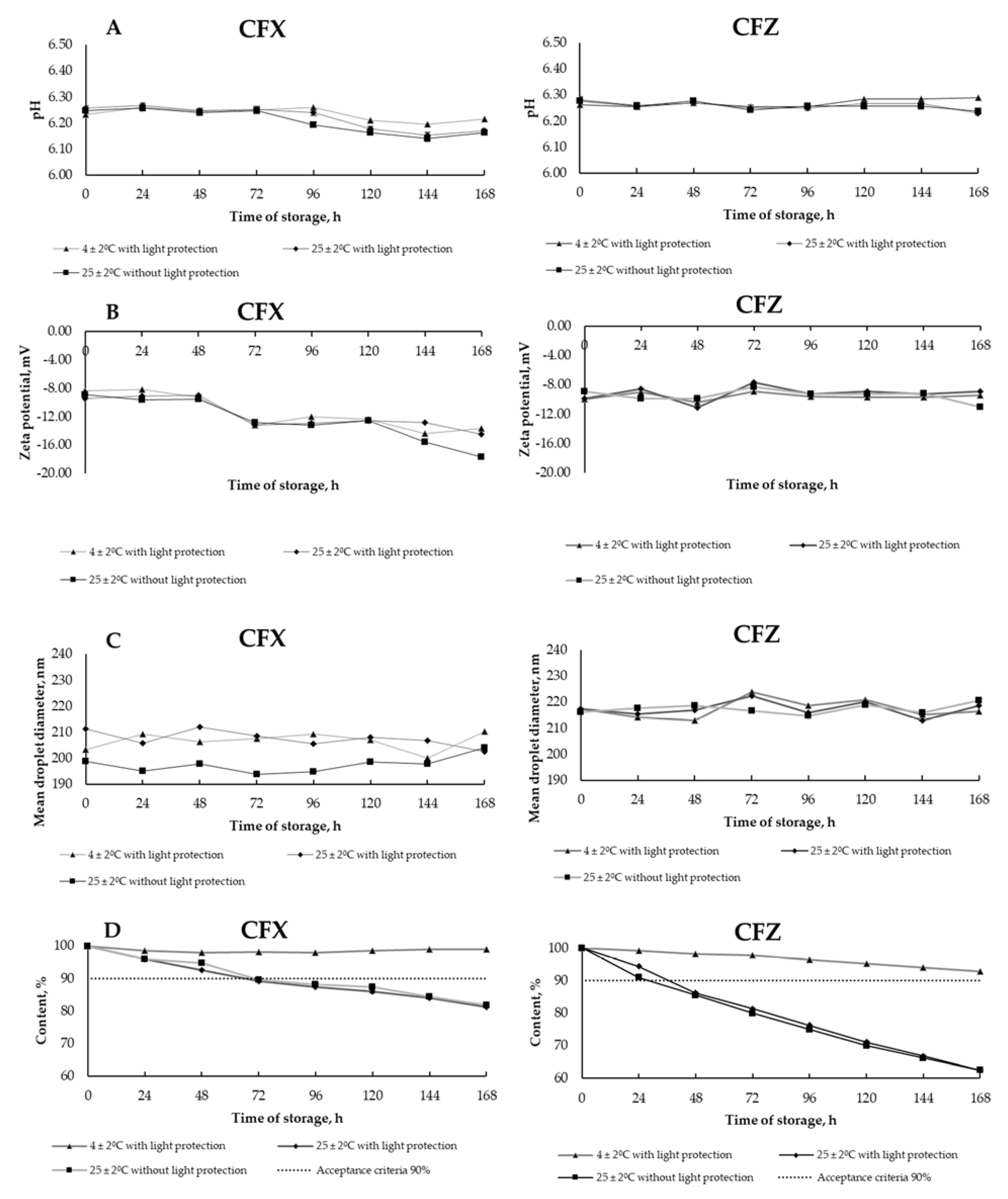
2.2. The Interaction between CFX I CFZ and PN Admixtures
2.3. Compatibility of CFL and Ready-to-Use PN Admixture
3. Discussion

{kind=link}
| Drug | Stability and Compatibility Results | Brand Name | References |
|---|---|---|---|
| Cefuroxime sodium (CFU) | CFU was stable for 7 days at 3 °C in water for injection. | Zinacef, Glaxo Inc, Philadelphia, PA, USA | [22] |
| A drug stored in 0.9% sodium chloride over 4 months at −18 °C was stable. | Cefuroxime Sandoz, Basel, Switzerland | [23] | |
| The drug was stable for 13 days at 4 °C stored in polyvinyl chloride (PVC) bags. | Zinacef, Glaxo Inc, USA | [55] | |
| During simulated Y-site administration, the drug was compatible with propofol injectable emulsion for one hour at 23 °C. | No data, Lilly, Indiana, IN, USA | [62] | |
| CFU was incompatible with ciprofloxacin. | Zinacef, Glaxo Wellcome Inc, Middlesex, UK | [50] | |
| Ceftazidime pentahydrate (CFZ) | CFZ was stable for 10 days at 3 °C in water for injection. | Ceptaz, Glaxo Inc, Philadelphia, PA, USA | [22] |
| CFZ was stable for 24 h at a temperature of 25 °C; | No data | [49] | |
| CFZ in glucose and normal saline was stable for 1 day, stored at room temperature, and for 4 days at 4 °C. | No data, GlaxoSmithKline, Mississauga, Canada | [60] | |
| CFZ in sterile water in either glass vials or plastic syringes was stable for 8 h at room temperature or 96 h at 4 °C. | Fortaz, Glaxo Inc, USA | [24] | |
| CFZ is sterile water for injection was stable at −20 °C for 30 days, thawed at 5 °C for 4 days, and at 37 °C for a day. | No data, Glaxo Inc, USA | [26] | |
| CFZ in sterile water in either glass vials or plastic syringes is stable for 8 h at room temperature or 96 h at 4 °C. | Fortaz, Glaxo Inc, USA | [24] | |
| CFZ was stable in water for injection stored over 24 h at 25 °C. | Glazidim; Glaxosmithkline, Rixensart, Belgium | [38] | |
| During simulated Y-site administration, the drug was compatible with propofol injectable emulsion for one hour at 23 °C. | No data, SmithKline Beecham, Philadelphia, PA, USA | [62] | |
| CFZ was compatible with amikacin, tobramycin, gentamycin, fluconazole, ketamine, sufentanil, valproic acid, morphine, urapidil, furosemide, adrenaline, insulin, methylprednisolone; CFZ was incompatible with N−acetylcysteine, dobutamine, nicardipine, theophylline, piritramide, phenytoin, midazolam, propofol, clarithromycin, erythromycin, and vancomycin. | Glazidim; GlaxoSmithkline, Rixensart, Belgium | [63] | |
| CFZ and linezolid were physically compatible and chemically stable for at least 7 days, stored at 4 °C, and for 3 days at 23 °C protected from light. | No data, McNeil Pharmaceutical, Ohio, OH, USA | [51] | |
| The drug was compatible with Olimel N5E and Numeta G16E. | No data, Fresenius Kabi, Uppsala, Sweden | [45] | |
| CFZ was incompatible with ciprofloxacin. | Tazicef, SmithKline Beecham, USA | [50] | |
| Cefepime dichlorohydrogen monohydrate (CFE) | CFE was stable in normal saline over 24 h at room temperature. | No data | [25] |
| CFE was stable in water for injection stored over 20.5 h at 25 °C and 13 h at 37 °C. | Maxipime, Bristol-Myers-Squibb, Brussels, Belgium | [38] | |
| Cefepime was most stable in the pH range 4 to 6. | Bulk material, Bristol-Myers-Squibb, New York, NY, USA | [56] | |
| C diluted with 0.9% sodium chloride or 5% glucose in polyethylene containers showed stability for 48 h at 24 in daylight or 15 days at 4 ± 2 °C in the dark. | Axepim Bristol-Myers-Squibb, Rueil-Malmaison, France | [57] | |
| CFE was stable up to 2 days in the solutions stored at 22–24 °C. | Maxipime, Bristol-Myers-Squibb, USA | [58] | |
| The drug was stable in normal saline for 2 days at 23 °C. | No data, Bristol-Myers-Squibb, USA | [59] | |
| CFE was compatible with amikacin, tobramycin, gentamycin, vancomycin, fluconazole, ketamine, sufentanil, valproic acid, morphine, urapidil, furosemide, insulin, methylprednisolone; CFE was incompatible with N−acetylcysteine, dobutamine, nicardipine, theophylline, piritramide, phenytoin, midazolam, propofol, and vancomycin. | Maxipime, Bristol-Myers-Squibb, Belgium | [63] | |
| The drug was compatible with Nutriflex Lipid Special parenteral nutrition admixture. | Cefepime Orpha, Orpha Pharma, Küsnacht, Swizetland | [34] | |
| Ceftriaxone sodium (CFX) | Drug solutions in glucose and normal saline were stable for 2 days at room temperature and 14 days at 4 °C. | No data, Mississauga, Roche, Canada | [60] |
| CFX was accelerated decomposed after mixing with linezolid. | No data, Ortho-McNeil Pharmaceutical, Raritan, NJ, USA | [51] | |
| The drug was incompatible with labetalol. | No data, Roche, Indiana, IN, USA | [53] | |
| During simulated Y-site administration, the drug was compatible with propofol injectable emulsion for one hour at 23 °C. | No data, Roche, USA | [62] | |
| CFX mixed with metronidazole was stable for 3 days at 25 ± 1 °C. | No data | [52] | |
| Ceftriaxone and metronidazole mixed at concentrations of 20 and 15 mg/mL, respectively, immediately formed precipitates. | Rocephin, Roche, USA | [64] | |
| CFL was stable in normal saline over 24 h at room temperature. | No data | [25] | |
| Cefazolin sodium (CFL) | CFL in sterile water for injection was stable at −20 °C for 30 days, thawed at 5 °C for 4 days, and at 37 °C for one day. | No data, Smith Kline and French Laboratories, Philadelphia, PA, USA | [26] |
| CFL in glucose or normal saline was stable at least 3 days at room temperature and for at least 26 days at 4 °C. | No data, Novopharm, Markham, ON, Canada | [60] | |
| The drug was stable in normal saline stored at 5 °C for 22 days and at 25 °C for 7 days. | No data | [21] | |
| CFL stored in polypropylene syringes or PVC minibags was stable for up to 30 days stored at 5 °C with light protection, followed by an additional 72 h at 21 °C to 25 °C with exposure to light. | No data | [65] | |
| CFL was stable for at least 30 days at 4 °C. | Cefacidal, Bristol-Myers, Roma, Italy | [55] | |
| During simulated Y-site administration, the drug was compatible with propofol injectable emulsion for one hour at 23 °C. | Marsam, New Britain, CT, USA | [62] | |
| CFL precipitated with piritramid solutions. | No data | [54] | |
| CFL with linezolid was physically compatible and chemically stable for at least 7 days, stored at 4 °C protected from light. | No data, Bayer Corporation, Whippany, NJ, USA | [51] |
4. Materials and Methods
4.1. Materials
4.2. Analysis of CFU and CFE
4.3. Analysis of CFX and CFZ
4.4. Analysis of CFL
4.5. Characteristic of PN Admixture
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- USP. General Chapters: Injections; The United States Pharmacopeia: Rockville, MD, USA, 2009; p. 413. [Google Scholar]
- USP. Globule Size Distribution in Lipid Injectable Emulsions; The United States Pharmacopeia: Rockville, MD, USA, 2009; pp. 314–316. [Google Scholar]
- Fekadu, T.; Teweldemedhin, M.; Esrael, E.; Asgedom, S.W. Prevalence of intravenous medication administration errors: A cross-sectional study. Integr. Pharm. Res. Pract. 2017, 6, 47–51. [Google Scholar] [CrossRef]
- Valentin, A.; Capuzzo, M.; Guidet, B.; Moreno, R.; Metnitz, B.; Bauer, P.; Metnitz, P. Errors in administration of parenteral drugs in intensive care units: Multinational prospective study. BMJ 2009, 338, 928–931. [Google Scholar] [CrossRef] [PubMed]
- Taxis, K.; Barber, N. Incidence and severity of intravenous drug errors in a German hospital. Eur. J. Clin. Pharmacol. 2004, 59, 815–817. [Google Scholar] [CrossRef]
- Mühlebach, S. Basics in clinical nutrition: Drugs and nutritional admixtures. E. Spen. Eur. E. J. Clin. Nutr. Metab. 2009, 4, e134–e136. [Google Scholar] [CrossRef]
- Akaho, E.; Nakayama, H. An innovative classification of, and a new structure-activity-relationship approach to degradation kinetics of cephalosporins: An attempt to enhance the therapeutic activity. J. Antibiot. 2003, 56, 379–391. [Google Scholar] [CrossRef][Green Version]
- Khan, D.A.; Banerji, A.; Bernstein, J.A.; Bilgicer, B.; Blumenthal, K.; Castells, M.; Ein, D.; Lang, D.M.; Phillips, E. Cephalosporin allergy: Current understanding and future challenges. J. Allergy Clin. Immunol. Pract. 2019, 7, 2105–2114. [Google Scholar] [CrossRef] [PubMed]
- Sriram, S.; Aishwarya, S.; Moithu, A.; Sebastian, A.; Kumar, A. Intravenous drug incompatibilities in the intensive care unit of a tertiary care hospital in India: Are they preventable? J. Res. Pharm. Pract. 2020, 9, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Crews, J.; Rueda-de-Leon, E.; Remus, D.; Sayles, R.; Mateus, J.; Shakeel, F. Total parenteral nutrition standardization and electronic ordering to reduce errors. Pediatr. Qual. Saf. 2018, 3, e093. [Google Scholar] [CrossRef] [PubMed]
- Stawny, M.; Gostyńska, A.; Nadolna, M.; Jelińska, A. Safe practice of Y-site drug administration: The case of colistin and parenteral nutrition. Pharmaceutics 2020, 12, 292. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.E.; Heldman, L.S.; Goo, E.D.; Whippo, P.E.; Perkinson, J.C. Fatal microvascular pulmonary emboli from precipitation of a total nutrient admixture solution. JPEN J. Parenter. Enteral. Nutr. 1996, 20, 81–87. [Google Scholar] [CrossRef]
- Driscoll, D.F.; Ling, P.-R.; Silvestri, A.P.; Bistrian, B.R. Fine vs. coarse complete all-in-one admixture infusions over 96 hours in rats: Fat globule size and hepatic function. Clin. Nutr. 2008, 27, 889–894. [Google Scholar] [CrossRef]
- Bradley, J.S.; Wassel, R.T.; Lee, L.; Nambiar, S. Intravenous ceftriaxone and calcium in the neonate: Assessing the risk for cardiopulmonary adverse events. Pediatrics 2009, 123, e609–e613. [Google Scholar] [CrossRef]
- Pertkiewicz, M.; Cosslett, A.; Mü Hlebach, C.S.; Dudrick, S.J. Educational paper basics in clinical nutrition: Stability of parenteral nutrition admixtures. E. Spen. Eur. E. J. Clin. Nutr. Metab. 2009, 4, e117–e119. [Google Scholar] [CrossRef]
- Huston, R.K.; Christensen, J.M.; Alshahrani, S.M.; Mohamed, S.M.; Heisel, C.F.; Stout, K.N. Calcium chloride and calcium gluconate in neonatal parenteral nutrition solutions with added cysteine: Compatibility studies using laser light obscuration methodology. J. Parenter. Enter. Nutr. 2019, 43, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Boullata, J.I.; Gilbert, K.; Sacks, G.; Labossiere, R.J.; Crill, C.; Goday, P.; Kumpf, V.J.; Mattox, T.W.; Plogsted, S.; Holcombe, B.; et al. A.S.P.E.N. clinical guidelines. J. Parenter. Enter. Nutr. 2014, 38, 334–377. [Google Scholar] [CrossRef]
- Harraki, B.; Guiraud, P.; Rochat, M.H.; Alary, J.; Favier, A. Interactions related to trace elements in parenteral nutrition. Pharm. Acta Helv. 1995, 70, 269–278. [Google Scholar] [CrossRef]
- Gibbons, E.; Allwood, M.C.; Neal, T.; Hardy, G. Degradation of dehydroascorbic acid in parenteral nutrition mixtures. J. Pharm. Biomed. Anal. 2001, 25, 605–611. [Google Scholar] [CrossRef]
- Terracciano, J.; Rhee, E.G.; Walsh, J. Chemical stability of ceftolozane/tazobactam in polyvinylchloride bags and elastomeric pumps. Curr. Ther. Res. 2017, 84, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.D. Chemical stability of cefazolin sodium after reconstituting in 0.9% sodium chloride injection and storage in polypropylene syringes for pediatric use. Int. J. Pharm. Compd. 2003, 7, 152–154. [Google Scholar]
- Stiles, M.L.; Allen, L.V.; Fox, J.L. Stability of ceftazidime (with arginine) and of cefuroxime sodium in infusion-pump reservoirs. Am. J. Hosp. Pharm. 1992, 49, 2761–2764. [Google Scholar] [CrossRef] [PubMed]
- Fleury-Souverain, S.; Sadeghipour, F.; Bonnabry, P. Development of ready-to-use cefuroxime syringes for use in ophthalmology. Eur. J. Hosp. Pharm. 2014, 21, 34–38. [Google Scholar] [CrossRef]
- Stewart, J.T.; Warren, F.W.; Johnson, S.M.; Fox, J.L.; Mullaney, J. Stability of ceftazidime in plastic syringes and glass vials under various storage conditions. Am. J. Heal. Pharm. 1992, 49, 2765–2768. [Google Scholar] [CrossRef]
- Voumard, R.; Van Neyghem, N.; Cochet, C.; Gardiol, C.; Decosterd, L.; Buclin, T.; de Valliere, S. Antibiotic stability related to temperature variations in elastomeric pumps used for outpatient parenteral antimicrobial therapy (OPAT). J. Antimicrob. Chemother. 2017, 72, 1462–1465. [Google Scholar] [CrossRef]
- Stiles, M.L.; Tu, Y.-H.; Allen, L.V. Stability of cefazolin sodium, cefoxitin sodium, ceftazidime, and penicillin G sodium in portable pump reservoirs. Am. J. Heal. Pharm. 1989, 46, 1408–1412. [Google Scholar] [CrossRef]
- Tomczak, S.; Stawny, M.; Dettlaff, K.; Kieliszek, M.; Słomińska, D.; Jelińska, A. Physicochemical compatibility and stability of linezolid with parenteral nutrition. Molecules 2019, 24, 1242. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, J.C.; Rutherford, E.T.; Cunningham, G.N.; Daneshmand, K.A.; Falls, A.L. Stability of ondansetron hydrochloride in a total parenteral nutrient admixture. Am. J. Heal. Pharm. 1995, 52, 1557–1558. [Google Scholar] [CrossRef]
- Billion-Rey, F.; Guillaumont, M.; Frederich, A.; Aulagner, G. Stability of fat-soluble vitamins A (Retinol Palmitate), E (Tocopherol Acetate), and K1 (Phylloquinone) in total parenteral nutrition at home. J. Parenter. Enter. Nutr. 1993, 17, 56–60. [Google Scholar] [CrossRef]
- Baumgartner, T.G.; Henderson, G.N.; Fox, J.; Gondi, U. Stability of ranitidine and thiamine in parenteral nutrition solutions. Nutrition 1997, 13, 547–553. [Google Scholar] [CrossRef]
- Stawny, M.; Gostyńska, A.; Dettlaff, K.; Jelińska, A.; Kościelniak, M.; Ogrodowczyk, M. Development, validation, and stability assessment application of RP-HPLC-DAD method for quantification of ampicillin in total parenteral nutrition admixtures. Antibiotics 2019, 8, 268. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, S.; Radwan, V.; Jelińska, A.; Stawny, M. Application of the HPLC method in parenteral nutrition assessment: Stability Studies of ondansetron. Processes 2021, 9, 453. [Google Scholar] [CrossRef]
- Gostyńska, A.; Piwowarczyk, L.; Nadolna, M.; Jelińska, A.; Dettlaff, K.; Ogrodowczyk, M.; Popielarz-Brzezińska, M.; Stawny, M. Toward safe Pharmacotherapy: The interplay between meropenem and parenteral nutrition admixtures. Antibiotics 2021, 10, 217. [Google Scholar] [CrossRef]
- Bouchoud, L.; Fonzo-Christe, C.; Klingmüller, M.; Bonnabry, P. Compatibility of intravenous medications with parenteral nutrition: In vitro evaluation. JPEN. J. Parenter. Enteral Nutr. 2013, 37, 416–424. [Google Scholar] [CrossRef]
- Avery, L.M.; Chen, I.H.; Reyes, S.; Nicolau, D.P.; Kuti, J.L. Assessment of the physical compatibility of Eravacycline and common parenteral drugs during simulated Y-site administration. Clin. Ther. 2019, 41, 2162–2170. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.M.; Villareal, C.L.; Meyer, L.M. Y-Site compatibility of intravenous Levetiracetam with commonly used critical care medications. Hosp. Pharm. 2019, 001857871989337. [Google Scholar] [CrossRef]
- Garcia, J.; Garg, A.; Song, Y.; Fotios, A.; Andersen, C.; Garg, S. Compatibility of intravenous ibuprofen with lipids and parenteral nutrition, for use as a continuous infusion. PLoS ONE 2018, 13, e0190577. [Google Scholar] [CrossRef]
- Viaene, E.; Chanteux, H.; Servais, H.; Mingeot-Leclercq, M.P.; Tulkens, P.M. Comparative stability studies of antipseudomonal β-lactams for potential administration through portable elastomeric pumps (home therapy for cystic fibrosis patients) and motor-operated syringes (intensive care units). Antimicrob. Agents Chemother. 2002, 46, 2327–2332. [Google Scholar] [CrossRef]
- El Saghir, F.; Meier, J.; Bornand, D.; Senn, M.; Deuster, S. Stability testing of piperacilline/tazobactam in elastomeric infusion pumps. Le Pharm. Hosp. Clin. 2017, 52, e32. [Google Scholar] [CrossRef]
- Xu, Q.A.; Trissel, L.A.; Saenz, C.A.; Ingram, D.S.; Williams, K.Y. Stability of three cephalosporin antibiotics in AutoDose Infusion System bags. J. Am. Pharm. Assoc. 2002, 42, 428–431. [Google Scholar] [CrossRef]
- Trissel, L.A.; Gilbert, D.L.; Martinez, J.F.; Baker, M.B.; Walter, W.V.; Mirtallo, J.M. Compatibility of medications with 3-in-1 parenteral nutrition admixtures. J. Parenter. Enter. Nutr. 1999, 23, 67–74. [Google Scholar] [CrossRef]
- Kanji, S.; Lam, J.; Johanson, C.; Singh, A.; Goddard, R.; Fairbairn, J.; Lloyd, T.; Monsour, D.; Kakal, J. Systematic review of physical and chemical compatibility of commonly used medications administered by continuous infusion in intensive care units. Crit. Care Med. 2010, 38, 1890–1898. [Google Scholar] [CrossRef] [PubMed]
- Newton, D.W. Y-site compatibility of intravenous drugs with parenteral nutrition. J. Parenter. Enter. Nutr. 2013, 37, 297–299. [Google Scholar] [CrossRef]
- Staven, V.; Wang, S.; Grønlie, I.; Tho, I. Physical stability of an all-in-one parenteral nutrition admixture for preterm infants upon mixing with micronutrients and drugs. Eur. J. Hosp. Pharm. 2020, 27, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Staven, V.; Iqbal, H.; Wang, S.; Grønlie, I.; Tho, I. Physical compatibility of total parenteral nutrition and drugs in Y-site administration to children from neonates to adolescents. J. Pharm. Pharmacol. 2017, 69, 448–462. [Google Scholar] [CrossRef]
- Staven, V.; Wang, S.; Grønlie, I.; Tho, I. Development and evaluation of a test program for Y-site compatibility testing of total parenteral nutrition and intravenous drugs. Nutr. J. 2016, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, S.; Stawny, M.; Jelińska, A. Co-administration of drugs and parenteral nutrition: In vitro compatibility studies of loop diuretics for safer clinical practice. Pharmaceutics 2020, 12, 1092. [Google Scholar] [CrossRef] [PubMed]
- Stawny, M.; Olijarczyk, R.; Jaroszkiewicz, E.; Jelińska, A. Pharmaceutical point of view on parenteral nutrition. Sci. World J.. 2013, 2013, 415310. [Google Scholar] [CrossRef]
- Servais, H.; Tulkens, P.M. Stability and compatibility of ceftazidime administered by continuous infusion to intensive care patients. Antimicrob. Agents Chemother. 2001, 45, 2643–2647. [Google Scholar] [CrossRef] [PubMed]
- Elmore, R.L.; Contois, M.E.; Kelly, J.; Noe, A.; Poirier, A.; Celesk, R. Stability and compatibility of admixtures of intravenous ciprofloxacin and selected drugs. Clin. Ther. 1996, 18, 246–255. [Google Scholar] [CrossRef]
- Xu, Q.A.; Trissel, L.A.; Williams, K.Y. Compatibility and stability of linezolid injection admixed with three cephalosporin antibiotics. J. Am. Pharm. Assoc. 2000, 40, 509–514. [Google Scholar] [CrossRef]
- Gupta, V.D.; Maswoswe, J. Stability of ceftriaxone sodium when mixed with metronidazole injection. Int. J. Pharm. Compd. 1997, 1, 280. [Google Scholar]
- Leader, W.G.; Jones, J.M. Incompatibility between ceftriaxone sodium and labetalol hydrochloride. Am. J. Heal. Pharm. 1996, 53, 2639. [Google Scholar] [CrossRef]
- Eckle, V.S.; Heim, E.; Hahn, M.; Grasshoff, C. Incompatibility of piritramide with cephalosporins. Ann. Pharmacother. 2013, 47, 426–427. [Google Scholar] [CrossRef] [PubMed]
- Galanti, L.M.; Hecq, J.-D.; Vanbeckbergen, D.; Jamart, J. Long-term stability of cefuroxime and cefazolin sodium in intravenous infusions. J. Clin. Pharm. Ther. 1996, 21, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Fubara, J.O. Influence of pH, temperature and buffers on cefepime degradation kinetics and stability predictions in aqueous solutions. J. Pharm. Sci. 1998, 87, 1572–1576. [Google Scholar] [CrossRef]
- Rabouan-Guyon, S.M.; Guet, A.F.; Courtois, P.Y.; Barthes, D.M.C. Stability study of cefepime in different infusion solutions. Int. J. Pharm. 1997, 154, 185–190. [Google Scholar] [CrossRef]
- Stewart, J.T.; Maddox, F.C.; Warren, F.W. Stability of cefepime hydrochloride in polypropylene syringes. Am. J. Heal. Pharm. 1999, 56, 1134. [Google Scholar] [CrossRef] [PubMed]
- Trissel, L.A.; Xu, Q.A. Stability of cefepime hydrochloride in AutoDose infusion system bags. Ann. Pharmacother. 2003, 37, 804–807. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.E.; Iazzetta, J.; Law, S.; Biniecki, K. Stability of commonly used antibiotic solutions in an elastomeric infusion device. Can. J. Hosp. Pharm. 2010, 63, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Stawny, M.; Nadolna, M.; Jelińska, A. In vitro compatibility studies of vancomycin with ready-to-use parenteral nutrition admixtures for safer clinical practice. Clin. Nutr. 2019, 39, 2539–2546. [Google Scholar] [CrossRef]
- Trissel, L.A.; Gilbert, D.L.; Martinez, J.F. Compatibility of propofol injectable emulsion with selected drugs during simulated Y-site administration. Am. J. Heal. Pharm. 1997, 54, 1287–1292. [Google Scholar] [CrossRef]
- Donnelly, R.F. Stability of cefazolin sodium in polypropylene syringes and polyvinylchloride minibags. Can. J. Hosp. Pharm. 2011, 64, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Baririan, N. Stability and compatibility study of cefepime in comparison with ceftazidime for potential administration by continuous infusion under conditions pertinent to ambulatory treatment of cystic fibrosis patients and to administration in intensive care units. J. Antimicrob. Chemother. 2003, 51, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.C.; Orosz, S.T. Stability of ceftriaxone sodium and metronidazole hydrochloride. Am. J. Heal. Pharm. 1997, 54, 424–427. [Google Scholar] [CrossRef] [PubMed]

| Time, h | Water for Injection | 0.9% Sodium Chloride | 5% Glucose | 10% Glucose | Ringer’s Solution | PN Admixtures |
|---|---|---|---|---|---|---|
| Drug content (%) | ||||||
| CFE stored at 5 ± 1 °C with light protection | ||||||
| 0 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| 24 | 96.56 | 98.73 | 97.38 | 97.28 | 99.43 | 86.10 |
| 48 | 93.51 | 98.00 | 95.53 | 92.88 | 96.90 | 83.41 |
| 72 | 90.23 | 96.90 | 95.26 | 90.11 | 91.06 | 79.62 |
| 96 | 88.38 | 88.45 | 92.69 | 87.92 | 90.24 | 77.18 |
| CFE stored 25±2 °C with light protection | ||||||
| 0 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| 24 | 94.83 | 94.94 | 91.38 | 99.00 | 93.05 | 73.87 |
| 48 | 94.27 | 91.09 | 89.50 | 90.30 | 90.72 | 65.91 |
| 72 | 85.79 | 89.27 | 84.72 | 85.56 | 88.44 | 59.67 |
| 96 | 82.86 | 86.72 | 82.41 | 86.30 | 83.59 | 54.21 |
| CFU stored at 5±1 °C with light protection | ||||||
| 0 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| 24 | 98.99 | 99.55 | 99.75 | 92.64 | 97.93 | 74.57 |
| 48 | 94.45 | 91.63 | 97.97 | 91.05 | 95.59 | 59.87 |
| 72 | 86.32 | 79.13 | 94.8 | 76.36 | 81.17 | 42.97 |
| 96 | 77.31 | 63.64 | 77.17 | 70.44 | 76.36 | 38.27 |
| CFU stored 25 ± 2 °C with light protection | ||||||
| 0 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| 24 | 99.58 | 90.32 | 98.93 | 97.81 | 91.63 | 73.71 |
| 48 | 94.88 | 83.53 | 98.75 | 53.92 | 77.00 | 54.06 |
| 72 | 90.63 | 77.85 | 69.07 | 44.84 | 48.37 | 43.36 |
| 96 | 69.32 | 64.27 | 49.66 | 32.60 | 46.04 | 24.65 |
| Sample | Ratio | pH * | Osmolality ± SD | Zeta Potential ± SD | PDI | dF1 | dF2 | MDD | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (mOsm/kg H2O) | (mV) | (nm) | (nm) | (nm) | |||||||||||
| 0 h | 4 h | 0 h | 4 h | 0 h | 0 h | 0 h | 0 h | 0 h | 4 h | 0 h | 4 h | 0 h | 4 h | ||
| CFL-Kabiven | 1:1 | 5.48 | 5.49 | 683 ± 1 | 683 ± 6 | −12.1 ± 0.3 | −13.9 ± 0.2 | 0.15 ± 0.01 | 0.14 ± 0.02 | 326 ± 3 | 328 ± 4 | – | – | 281 ± 6 | 281 ± 6 |
| 2:1 | 5.49 | 5.5 | 537 ± 4 | 538 ± 4 | −14.2 ± 0.4 | −12.9 ± 0.4 | 0.16 ± 0.02 | 0.16 ± 0.01 | 320 ± 3 | 320 ± 10 | – | – | 278 ± 6 | 278 ± 6 | |
| 4:1 | 5.48 | 5.5 | 441 ± 1 | 438 ± 2 | −13.5 ± 0.7 | −14.8 ± 0.5 | 0.16 ± 0.01 | 0.16 ± 0.01 | 325 ± 3 | 331 ± 6 | 1243 ± 8 | 1443 ± 7 | 278 ±11 | 289 ± 11 | |
| CFL-Nutriflex LS | 1:1 | 5.47 | 5.45 | 984 ± 2 | 995 ± 3 | −12.2 ± 0.1 | −23 ± 1.4 | 0.06 ± 0.02 | 0.07 ± 0.02 | 233 ± 3 | 228 ± 1 | – | – | 219 ± 2 | 211 ± 2 |
| 2:1 | 5.47 | 5.46 | 735 ± 1 | 739 ± 1 | −14 ± 0.2 | −12.6 ± 0.4 | 0.06 ± 0.04 | 0.06 ± 0.02 | 229 ± 4 | 229 ± 6 | – | – | 213 ± 5 | 213 ± 2 | |
| 4:1 | 5.47 | 5.47 | 547 ± 4 | 549 ± 1 | −19.7 ± 1 | −27.7 ± 1.2 | 0.07 ± 0.03 | 0.08 ± 0.03 | 232 ± 7 | 226 ± 0 | – | – | 215 ± 3 | 208 ± 2 | |
| CFL-Olimel | 1:1 | 6.27 | 6.26 | 820 ± 4 | 865 ± 5 | −10.8 ± 0.4 | −12.9 ± 0.7 | 0.11 ± 0.01 | 0.12 ± 0.04 | 287 ± 5 | 280 ± 6 | – | 1662 ± 2 | 257 ± 2 | 256 ± 5 |
| 2:1 | 6.27 | 6.26 | 612 ± 1 | 639 ± 3 | −15 ± 0.3 | −11.8 ± 0.7 | 0.13 ± 0.01 | 0.12 ± 0.01 | 296 ± 8 | 293 ± 4 | – | – | 259 ± 4 | 259 ± 4 | |
| 4:1 | 6.24 | 6.29 | 476 ± 2 | 511 ± 1 | −10.9 ± 0.5 | −13.7 ± 1.5 | 0.13 ± 0.02 | 0.24 ± 0.01 | 287 ± 5 | 284 ± 4 | 1728 ± 3 | 3537 ± 8 | 260 ± 6 | 280 ± 0 | |
| CFL-Nutriflex OS | 1:1 | 5.62 | 5.59 | 971 ± 4 | 1008 ± 1 | −9.3 ± 0.1 | −9.9 ± 0.1 | 0.09 ± 0.01 | 0.57 ± 0.04 | 243 ± 4 | 343 ± 4 | – | 5005 ± 7 | 222 ± 3 | 550 ±11 |
| 2:1 | 5.59 | 5.59 | 728 ± 2 | 846 ± 1 | −11.3 ± 0.4 | −11.9 ± 0.1 | 0.07 ± 0.01 | 0.57 ± 0.09 | 244 ± 3 | 1469 ± 4 | – | 1970 ± 6 | 225 ± 1 | 663 ± 4 | |
| 4:1 | 5.6 | 5.59 | 531 ± 1 | 557 ± 6 | −13.1 ± 1 | −15.7 ± 0.9 | 0.10 ± 0.02 | 0.10 ± 0.02 | 237 ± 5 | 240 ± 6 | – | – | 217 ± 1 | 218 ± 1 | |
| CFL-Smofkabiven | 1:1 | 5.45 | 5.46 | 916 ± 4 | 891 ± 5 | −9.4 ± 0.7 | −9.7 ± 0.3 | 0.09 ± 0.02 | 0.13 ±0.001 | 277 ± 1 | 271 ± 9 | – | – | 249 ± 4 | 237 ± 2 |
| 2:1 | 5.45 | 5.47 | 686 ± 1 | 668 ± 3 | −9.8 ± 0.4 | −9.6 ± 0.3 | 0.12 ± 0.01 | 0.12 ± 0.02 | 276 ± 7 | 270 ± 7 | – | – | 247 ± 4 | 240 ± 3 | |
| 4:1 | 5.46 | 5.48 | 521 ± 4 | 505 ± 2 | −12.6 ± 0.4 | −11.6 ± 0.1 | 0.11 ± 0.01 | 0.15 ± 0.02 | 264 ± 5 | 250 ± 7 | – | 3454 ± 8 | 236 ± 1 | 231 ± 1 | |
| Ingredient | Pharmaceutical Preparation | Unit | PN A | PN B |
|---|---|---|---|---|
| Amino acids | Aminoplasmal BB 10% E | g/L | 20 | 24 |
| Lipid emulsion | Lipofundin MCT/LCT 20% | 70 | 88 | |
| Carbohydrates | Glucose 40% | 24 | 24 | |
| Sodium | Natrium chloratum 10% | mmol/L | 45 | 41 |
| Potassium | Kalium chloratum 15% | 20 | 16 | |
| Calcium | Calcium gluconate 10% | 2.5 | 1.8 | |
| Phosphates | Glycophos | 15 | 8 | |
| Magnesium | Inj. Magnesii sulfurici 20% | 1.5 | 2.5 |
| Factor | CFZ | CFX | ||
|---|---|---|---|---|
| Column | C18 with a precolumn C18; LiChrospher 100, (5 µm); 4 mm i.d., 150 × 4.6 mm; Merck Darmstadt Germany | C18 with a precolumn C18; LiChrospher 100, (5 µm); 4 mm i.d.; 250 × 4.6 mm; Merck Darmstadt Germany | ||
| Column temperature | 25 °C | 40 °C | ||
| Mobile phase | Phase A: 0.5 mL 12% acetic acid, 50 mL 0.2 mol/L potassium dihydrogen phosphate buffer, 50 mL acetonitrile, and up to 1000 mL water Phase B: 0.5 mL 12% acetic acid, 50 mL 0.2 mol/L potassium dihydrogen phosphate buffer, 400 mL acetonitrile and up to 1000 mL water | Phase A: Acetonitrile Phase B: 50 mmol/L dihydrogen ammonium phosphate solution | ||
| Elution | Isocratic 95:5 ratio A:B | Gradient | ||
| Time, min | Mobile phase A (%, V/V) | Mobile phase B (%, V/V) | ||
| 0–20 | 100 → 65 | 0 → 35 | ||
| 21–25 | 65 → 100 | 35 → 0 | ||
| Flow rate | 1 mL/min | 1 mL/min | ||
| Detection | 255 nm | 254 nm | ||
| Injection | 10 µL | 10 µL | ||
| Run time | 25 min | 25 min | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomczak, S.; Gostyńska, A.; Nadolna, M.; Reisner, K.; Orlando, M.; Jelińska, A.; Stawny, M. Stability and Compatibility Aspects of Drugs: The Case of Selected Cephalosporins. Antibiotics 2021, 10, 549. https://doi.org/10.3390/antibiotics10050549
Tomczak S, Gostyńska A, Nadolna M, Reisner K, Orlando M, Jelińska A, Stawny M. Stability and Compatibility Aspects of Drugs: The Case of Selected Cephalosporins. Antibiotics. 2021; 10(5):549. https://doi.org/10.3390/antibiotics10050549
Chicago/Turabian StyleTomczak, Szymon, Aleksandra Gostyńska, Malwina Nadolna, Karolina Reisner, Marta Orlando, Anna Jelińska, and Maciej Stawny. 2021. "Stability and Compatibility Aspects of Drugs: The Case of Selected Cephalosporins" Antibiotics 10, no. 5: 549. https://doi.org/10.3390/antibiotics10050549
APA StyleTomczak, S., Gostyńska, A., Nadolna, M., Reisner, K., Orlando, M., Jelińska, A., & Stawny, M. (2021). Stability and Compatibility Aspects of Drugs: The Case of Selected Cephalosporins. Antibiotics, 10(5), 549. https://doi.org/10.3390/antibiotics10050549