
Use of Procalcitonin during the First Wave of COVID-19 in the Acute NHS Hospitals: A Retrospective Observational Study


 , , , , , , , , , and add
Show full author list
, , , , , , , , , and add
Show full author list
Abstract
1. Introduction
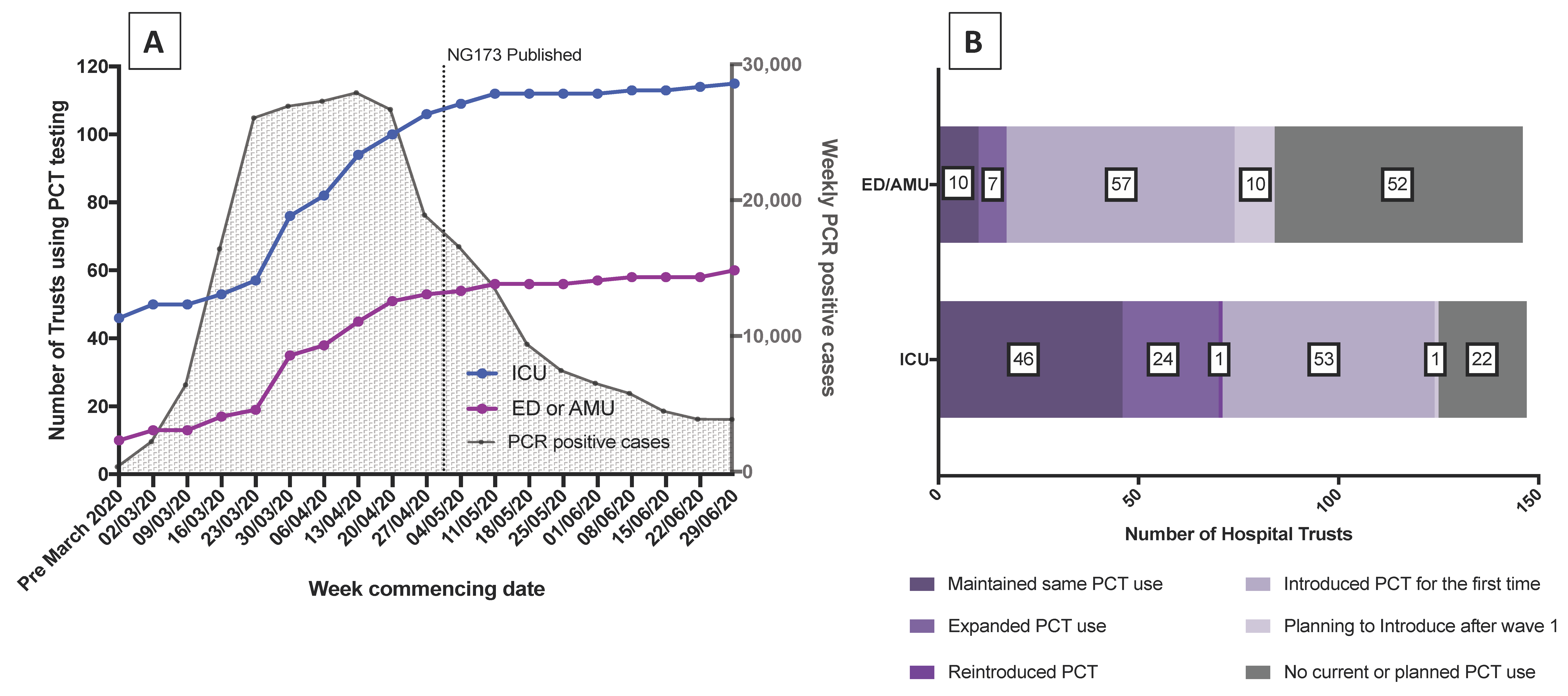
2. Results
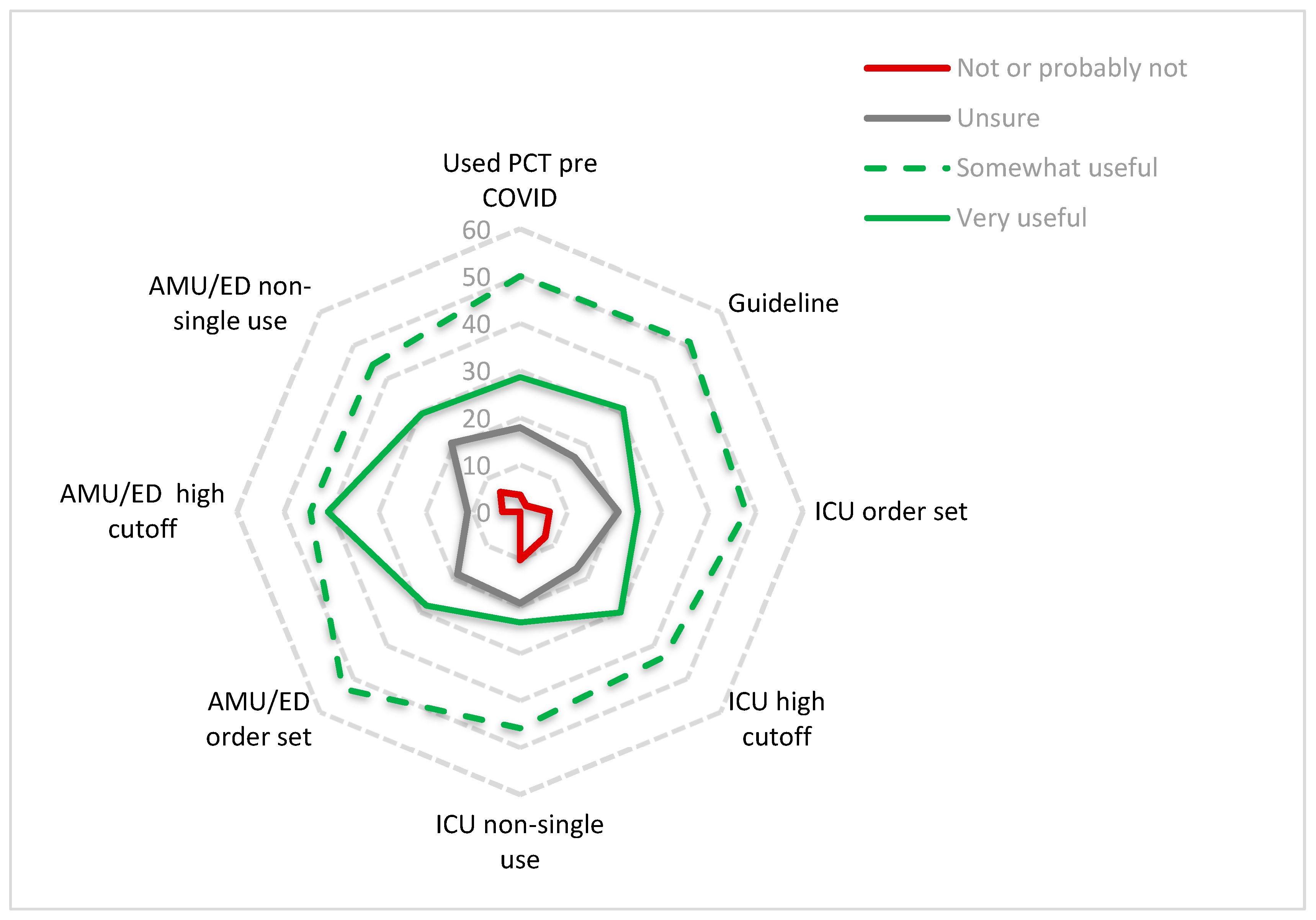
Perceptions of the Value of PCT and Future Plans
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Weekly Operational Update on COVID-19-8 February 2021. Available online: https://www.who.int/publications/m/item/weekly-operational-update-on-covid-19---8-february-2021 (accessed on 23 March 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. Jama 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Gov.UK. Coronovirus (COVID-19) in the UK. Available online: https://coronavirus.data.gov.uk/details/healthcare (accessed on 25 February 2021).
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals With Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Martén-Loeches, I.M.D.P.; Sanchez-Corral, A.M.D.; Diaz, E.M.D.P.; Granada, R.M.M.D.; Zaragoza, R.M.D.; Villavicencio, C.M.D.; Albaya, A.M.D.; Cerdá, E.M.D.; Catalán, R.M.M.D.; Luque, P.M.D.; et al. Community-Acquired Respiratory Coinfection in Critically Ill Patients With Pandemic 2009 Influenza A(H1N1) Virus. Chest 2011, 139, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influ. Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, V.M.; Gandhi, T.N.; Petty, L.A.; Patel, P.K.; Prescott, H.C.; Malani, A.N.; Ratz, D.; McLaughlin, E.; Chopra, V.; Flanders, S.A. Empiric Antibacterial Therapy and Community-onset Bacterial Coinfection in Patients Hospitalized with Coronavirus Disease 2019 (COVID-19): A Multi-hospital Cohort Study. Clin. Infect. Dis. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- NICE. COVID-19 Rapid Guideline: Antibiotics for Pneumonia in Adults in Hospital. Available online: https://www.nice.org.uk/guidance/ng173 (accessed on 20 January 2021).
- World Health Organisation. COVID-19 Clinical Management. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 23 March 2021).
- Luo, X.; Zhou, W.; Yan, X.; Guo, T.; Wang, B.; Xia, H.; Ye, L.; Xiong, J.; Jiang, Z.; Liu, Y.; et al. Prognostic Value of C-Reactive Protein in Patients with Coronavirus 2019. Clin. Infect. Dis. 2020, 71, 2174–2179. [Google Scholar] [CrossRef] [PubMed]
- Assicot, M.; Gendrel, D.; Carsin, H.; Raymond, J.; Guilbaud, J.; Bohuon, C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet 1993, 341, 515–518. [Google Scholar] [CrossRef]
- Simon, L.; Gauvin, F.; Amre, D.K.; Saint-Louis, P.; Lacroix, J. Serum Procalcitonin and C-Reactive Protein Levels as Markers of Bacterial Infection: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2004, 39, 206–217. [Google Scholar] [CrossRef] [PubMed]
- NICE. Procalcitonin Testing for Diagnosing and Monitoring Sepsis (ADVIA Centaur BRAHMS PCT Assay, BRAHMS PCT Sensitive Kryptor Assay, Elecsys BRAHMS PCT Assay, LIAISON BRAHMS PCT Assay and VIDAS BRAHMS PCT Assay). Available online: https://www.nice.org.uk/guidance/dg18 (accessed on 23 March 2021).
- Westwood, M.; Ramaekers, B.; Whiting, P.; Tomini, F.; Joore, M.; Armstrong, N.; Ryder, S.; Stirk, L.; Severens, J.; Kleijnen, J. Procalcitonin testing to guide antibiotic therapy for the treatment of sepsis in intensive care settings and for suspected bacterial infection in emergency department settings: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2015, 19, 3–236. [Google Scholar] [CrossRef] [PubMed]
- Carrol, E.; Sandoe, J. Procalcitonin: Evaluation of Antibiotic Use in COVID-19 Hospitalised Patients. (PEACH). Available online: https://dev.fundingawards.nihr.ac.uk/award/NIHR132254 (accessed on 23 March 2021).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Williams, E.J.; Mair, L.; de Silva, T.I.; Green, D.J.; House, P.; Cawthron, K.; Gillies, C.; Wigfull, J.; Parsons, H.; Partridge, D.G. Evaluation of procalcitonin as a contribution to antimicrobial stewardship in SARS-CoV-2 infection: A retrospective cohort study. J. Hosp. Infect. 2021, 110, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.; Williams, K.; Un, E.A.; Little, L.; Saad, A.; Lendrum, K.; Thompson, N.; Weatherley, N.D.; Pegden, A. Use of procalcitonin for antibiotic stewardship in patients with COVID-19: A quality improvement project in a district general hospital. Clin. Med. 2021, 21, e71. [Google Scholar] [CrossRef] [PubMed]
- Heesom, L.; Rehnberg, L.; Nasim-Mohi, M.; Jackson, A.I.R.; Celinski, M.; Dushianthan, A.; Cook, P.; Rivinberg, W.; Saeed, K. Procalcitonin as an antibiotic stewardship tool in COVID-19 patients in the intensive care unit. J. Glob. Antimicrob. Resist. 2020, 22, 782–784. [Google Scholar] [CrossRef]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: A patient level meta-analysis. Lancet Infect. Dis. 2018, 18, 95–107. [Google Scholar] [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Dark, P. BiomArker-Guided Duration of Antibiotic Treatment in Hospitalised PaTients with Suspected Sepsis: The ADAPT-Sepsis Trial. Available online: https://warwick.ac.uk/fac/sci/med/research/ctu/trials/adaptsepsis/ (accessed on 6 April 2021).
- French, N. PROcalcitonin and NEWS2 Evaluation for Timely Identification of Sepsis and Optimal Use of Antibiotics in the Emergency Department. Available online: https://www.cardiff.ac.uk/centre-for-trials-research/research/studies-and-trials/view/pronto (accessed on 6 April 2021).
- Carrol, E. Biomarker-Guided Duration of Antibiotic Treatment in Children Hospitalised with Confirmed or Suspected Bacterial Infection Trial. Available online: https://www.cardiff.ac.uk/centre-for-trials-research/research/studies-and-trials/view/batch (accessed on 6 April 2021).
- World Health Organization. Guidance for Managing Ethical Issues in Infectious Disease Outbreaks; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Horby, P.P. A Randomised Trial of Treatments to Prevent Death in Patients Hospitalised with COVID-19 (Coronavirus). Available online: https://doi.org/10.1186/ISRCTN50189673 (accessed on 23 March 2021).
- Bulter, C. Platform Randomised Trial for Interventons Against COVID-19 in Older People. Available online: https://www.principletrial.org/ (accessed on 23 March 2021).
- San Mateo, CA, USA. SurveyMonkey Inc. Available online: www.surveymonkey.com (accessed on 9 November 2020).
- Infection Group, United Kingdom Clinical Pharmacy Association. Available online: https://ukclinicalpharmacy.org/ (accessed on 9 November 2020).
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| ICU | Non-ICU | |
|---|---|---|
| PCT cut-off (ng/L) | n = 116 | n = 78 |
| 0.1 | 1(1%) | 0 |
| 0.2 | 1 (1%) | 0 |
| 0.25 | 51 (44%) | 41 (53%) |
| 0.5 | 54 (47%) | 27 (35%) |
| No cut off specified, cut-off varied dependent on clinical context | 9 (8%) | 10 (13%) |
| Timing of PCT testing | n = 114 | n = 76 |
| Single measurement | 14 (12%) | 39 (51%) |
| Two measurements | 23 (20%) | 21 (28%) |
| Serial | 72 (63%) | 9 (12%) |
| Other (i.e., varied dependent on clinical context) | 5 (4%) | 7 (9%) |
| PCT part of biochemistry order set | n = 122 | n = 107 |
| Yes | 50 (41%) | 33 (31%) |
| Hospital guideline | n = 114 | |
| PCT part of a Hospital guideline for managing COVID-19 | 55 (48%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Powell, N.; Howard, P.; Llewelyn, M.J.; Szakmany, T.; Albur, M.; Bond, S.E.; Euden, J.; Brookes-Howell, L.; Dark, P.; Hellyer, T.P.; et al. Use of Procalcitonin during the First Wave of COVID-19 in the Acute NHS Hospitals: A Retrospective Observational Study. Antibiotics 2021, 10, 516. https://doi.org/10.3390/antibiotics10050516
Powell N, Howard P, Llewelyn MJ, Szakmany T, Albur M, Bond SE, Euden J, Brookes-Howell L, Dark P, Hellyer TP, et al. Use of Procalcitonin during the First Wave of COVID-19 in the Acute NHS Hospitals: A Retrospective Observational Study. Antibiotics. 2021; 10(5):516. https://doi.org/10.3390/antibiotics10050516
Chicago/Turabian StylePowell, Neil, Philip Howard, Martin J. Llewelyn, Tamas Szakmany, Mahableswhar Albur, Stuart E Bond, Joanne Euden, Lucy Brookes-Howell, Paul Dark, Thomas P Hellyer, and et al. 2021. "Use of Procalcitonin during the First Wave of COVID-19 in the Acute NHS Hospitals: A Retrospective Observational Study" Antibiotics 10, no. 5: 516. https://doi.org/10.3390/antibiotics10050516
APA StylePowell, N., Howard, P., Llewelyn, M. J., Szakmany, T., Albur, M., Bond, S. E., Euden, J., Brookes-Howell, L., Dark, P., Hellyer, T. P., Hopkins, S., McCullagh, I. J., Ogden, M., Pallmann, P., Parsons, H., Partridge, D. G., Shaw, D. E., Shinkins, B., Todd, S., ... Sandoe, J. A. T. (2021). Use of Procalcitonin during the First Wave of COVID-19 in the Acute NHS Hospitals: A Retrospective Observational Study. Antibiotics, 10(5), 516. https://doi.org/10.3390/antibiotics10050516