
Effect of N-Acetylcysteine Administration on 30-Day Mortality in Critically Ill Patients with Septic Shock Caused by Carbapenem-Resistant Klebsiella pneumoniae and Acinetobacter baumannii: A Retrospective Case-Control Study

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Baseline Assessment
4.2. Definitions
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kang, C.-I.; Kim, S.-H.; Park, W.B.; Lee, K.-D.; Kim, H.-B.; Kim, E.-C.; Oh, M.-D.; Choe, K.-W. Bloodstream Infections Caused by Antibiotic-Resistant Gram-Negative Bacilli: Risk Factors for Mortality and Impact of Inappropriate Initial Antimicrobial Therapy on Outcome. Antimicrob. Agents Chemother. 2005, 49, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Garnacho-Montero, J.; Dimopoulos, G.; Poulakou, G.; Akova, M.; Cisneros, J.M.; de Waele, J.; Petrosillo, N.; Seifert, H.; Timsit, J.F.; Vila, J.; et al. Task force on management and prevention of Acinetobacter baumannii infections in the ICU. Intensiv. Care Med. 2015, 41, 2057–2075. [Google Scholar] [CrossRef] [PubMed]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Dickinson, J.D.; Kollef, M.H. Early and Adequate Antibiotic Therapy in the Treatment of Severe Sepsis and Septic Shock. Curr. Infect. Dis. Rep. 2011, 13, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Busani, S.; Serafini, G.; Mantovani, E.; Venturelli, C.; Giannella, M.; Viale, P.; Mussini, C.; Cossarizza, A.; Girardis, M. Mortality in Patients with Septic Shock by Multidrug Resistant Bacteria. J. Intensiv. Care Med. 2017, 34, 48–54. [Google Scholar] [CrossRef]
- Russo, A.; Giuliano, S.; Ceccarelli, G.; Alessandri, F.; Giordano, A.; Brunetti, G.; Venditti, M. Comparison of Septic Shock Due to Multidrug-Resistant Acinetobacter baumanniior Klebsiella pneumoniae Carbapenemase-Producing K. pneumoniae in Intensive Care Unit Patients. Antimicrob. Agents Chemother. 2018, 62, e02562-17. [Google Scholar] [CrossRef]
- Falcone, M.; Bassetti, M.; Tiseo, G.; Giordano, C.; Nencini, E.; Russo, A.; Graziano, E.; Tagliaferri, E.; Leonildi, A.; Barnini, S.; et al. Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae. Crit. Care 2020, 24, 1–12. [Google Scholar] [CrossRef]
- Marik, P.E.; Khangoora, V.; Rivera, R.; Hooper, M.H.; Catravas, J. Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock. Chest 2017, 151, 1229–1238. [Google Scholar] [CrossRef]
- Victor, V.M.; Rocha, M.; de la Fuente, M. Immune cells: Free radicals and antioxidants in sepsis. Int. Immunopharmacol. 2004, 4, 327–347. [Google Scholar] [CrossRef]
- Heming, N.; Lamothe, L.; Ambrosi, X.; Annane, D. Emerging drugs for the treatment of sepsis. Expert Opin. Emerg. Drugs 2016, 21, 27–37. [Google Scholar] [CrossRef]
- Pinsky, M.R. Antioxidant therapy for severe sepsis: Promise and perspective. Crit. Care Med. 2003, 31, 2697–2698. [Google Scholar] [CrossRef] [PubMed]
- Ergin, B.; Guerci, P.; Zafrani, L.; Nocken, F.; Kandil, A.; Gurel-Gurevin, E.; Demirci-Tansel, C.; Ince, C. Effects of N-acetylcysteine (NAC) supplementation in resuscitation fluids on renal microcirculatory oxygenation, inflammation, and function in a rat model of endotoxemia. Intensiv. Care Med. Exp. 2016, 4, 29. [Google Scholar] [CrossRef]
- Angus, D.C.; van der Poll, T. Severe Sepsis and Septic Shock. N. Engl. J. Med. 2013, 369, 840–851. [Google Scholar] [CrossRef]
- Ait-Oufella, H.; Maury, E.; Lehoux, S.; Guidet, B.; Offenstadt, G. The endothelium: Physiological functions and role in microcirculatory failure during severe sepsis. Intensiv. Care Med. 2010, 36, 1286–1298. [Google Scholar] [CrossRef] [PubMed]
- Ince, C.; Mayeux, P.R.; Nguyen, T.; Gomez, H.; Kellum, J.A.; Ospina-Tascón, G.A.; Hernandez, G.; Murray, P.; de Backer, D. The Endothelium in Sepsis. Shock 2016, 45, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Ince, C. The microcirculation is the motor of sepsis. Crit. Care 2005, 9, S13–S19. [Google Scholar] [CrossRef]
- Chertoff, J. N-Acetylcysteine’s Role in Sepsis and Potential Benefit in Patients with Microcirculatory Derangements. J. Intensiv. Care Med. 2018, 33, 87–96. [Google Scholar] [CrossRef]
- Sadowska, A.M.; Verbraecken, J.; Darquennes, K.; de Backer, W.A. Role of N-acetylcysteine in the management of COPD. Int. J. Chronic Obstr. Pulm. Dis. 2006, 1, 425–434. [Google Scholar] [CrossRef]
- Green, J.L.; Heard, K.J.; Reynolds, K.M.; Albert, D. Oral and Intravenous Acetylcysteine for Treatment of Acetaminophen Toxicity: A Systematic Review and Meta-analysis. West. J. Emerg. Med. 2013, 14, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Blasi, F.; Page, C.; Rossolini, G.M.; Pallecchi, L.; Matera, M.G.; Rogliani, P.; Cazzola, M. The effect of N -acetylcysteine on biofilms: Implications for the treatment of respiratory tract infections. Respir. Med. 2016, 117, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Pollini, S.; Boncompagni, S.; di Maggio, T.; di Pilato, V.; Spanu, T.; Fiori, B.; Blasi, F.; Aliberti, S.; Sergio, F.; Rossolini, G.M.; et al. In vitro synergism of colistin in combination with N-acetylcysteine against Acinetobacter baumannii grown in planktonic phase and in biofilms. J. Antimicrob. Chemother. 2018, 73, 2388–2395. [Google Scholar] [CrossRef]
- Mascellino, M.; de Angelis, M.; Miele, M.C.; Stringaro, A.R.; Colone, M.; Oliva, A. Potential Role of N-Acetyl-Cysteine Towards Mul-ti-Drug Resistant Acinetobacter baumannii and Klebsiella pneumoniae. In Proceedings of the ASM Microbe, San Francisco, CA, USA, 20–24 June 2019; p. AAR02-637. [Google Scholar]
- Parry, M.F.; Neu, H.C. Effect of N-acetylcysteine on antibiotic activity and bacterial growth in vitro. J. Clin. Microbiol. 1977, 5, 58–61. [Google Scholar]
- Aslam, S.; Darouiche, R.O. Role of Antibiofilm-Antimicrobial Agents in Controlling Device-Related Infections. Int. J. Artif. Organs 2011, 34, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Marchese, A.; Bozzolasco, M.; Gualco, L.; Debbia, E.A.; Schito, G.C.; Schito, A.M. Effect of fosfomycin alone and in combination with N-acetylcysteine on E. coli biofilms. Int. J. Antimicrob. Agents 2003, 22, 95–100. [Google Scholar] [CrossRef]
- Oliva, A.; de Angelis, M.; Costantini, S.; Mascellino, M.T.; Mastroianni, C.M.; Vullo, V. High activity of N-acetylcysteine in combination with beta-lactam antibiotics against carbapenem-resistant Acinetobater baumannii. In Proceedings of the ECCMID 2018, Madrid, Spain, 21–24 April 2018. [Google Scholar]
- Rodríguez-Rosado, A.I.; Valencia, E.Y.; Rodríguez-Rojas, A.; Costas, C.; Galhardo, R.S.; Rodríguez-Beltrán, J.; Blázquez, J. N-acetylcysteine blocks SOS induction and mutagenesis produced by fluoroquinolones in Escherichia coli. J. Antimicrob. Chemother. 2019, 74, 2188–2196. [Google Scholar] [CrossRef] [PubMed]
- Garozzo, A.; Tempera, G.; Ungheri, D.; Timpanaro, R.; Castro, A. N-Acetylcysteine Synergizes with Oseltamivir in Protecting Mice from Lethal Influenza Infection. Int. J. Immunopathol. Pharmacol. 2007, 20, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Geiler, J.; Michaelis, M.; Naczk, P.; Leutz, A.; Langer, K.; Doerr, H.-W.; Cinatl, J. N-acetyl-l-cysteine (NAC) inhibits virus replication and expression of pro-inflammatory molecules in A549 cells infected with highly pathogenic H5N1 influenza A virus. Biochem. Pharmacol. 2010, 79, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, P.; Ungheri, D. Synergistic Combination of N-Acetylcysteine and Ribavirin to Protect from Lethal Influenza Viral Infection in a Mouse Model. Int. J. Immunopathol. Pharmacol. 2004, 17, 99–102. [Google Scholar] [CrossRef]
- Hsu, B.-G.; Lee, R.-P.; Yang, F.-L.; Harn, H.-J.; Chen, H.I. Post-treatment with N-acetylcysteine ameliorates endotoxin shock-induced organ damage in conscious rats. Life Sci. 2006, 79, 2010–2016. [Google Scholar] [CrossRef]
- Spies, C.; Giese, C.; Meier-Hellmann, A.; Specht, M.; Hannemann, L.; Schaffartzik, W.; Reinhart, K. Einfluss der prophylaktischen Gabe von N-Azetylzystein auf klinische Indikatoren der Gewebeoxygenierung unter Hyperoxie bei kardialen Risikopatienten. Anaesthesist 1996, 45, 343–350. [Google Scholar] [CrossRef]
- Spapen, H.; Zhang, H.; Demanet, C.; Vleminckx, W.; Vincent, J.-L.; Huyghens, L. Does N-Acetyl-L-Cysteine Influence Cytokine Response During Early Human Septic Shock? Chest 1998, 113, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Ortolani, O.; Conti, A.; de Gaudio, A.R.; Masoni, M.; Novelli, G. Protective Effects of N-Acetylcysteine and Rutin on the Lipid Peroxidation of the Lung Epithelium during the Adult Respiratory Distress Syndrome. Shock 2000, 13, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Rank, N.; Michel, C.; Haertel, C.; Med, C.; Lenhart, A.; Welte, M.; Meier-Hellmann, A.; Spies, C. N-acetylcysteine increases liver blood flow and improves liver function in septic shock patients: Results of a prospective, randomized, double-blind study. Crit. Care Med. 2000, 28, 3799–3807. [Google Scholar] [CrossRef]
- Paterson, R.L.; Galley, H.F.; Webster, N.R. The effect of N-acetylcysteine on nuclear factor-κB activation, interleukin-6, interleukin-8, and intercellular adhesion molecule-1 expression in patients with sepsis. Crit. Care Med. 2003, 31, 2574–2578. [Google Scholar] [CrossRef]
- Szakmany, T.; Hauser, B.; Radermacher, P. N-acetylcysteine for sepsis and systemic inflammatory response in adults. Cochrane Database Syst. Rev. 2012, 2012, CD006616. [Google Scholar] [CrossRef] [PubMed]
- Aisa-Alvarez, A.; Soto, M.E.; Guarner-Lans, V.; Camarena-Alejo, G.; Franco-Granillo, J.; Martínez-Rodríguez, E.A.; Ávila, R.G.; Pech, L.M.; Pérez-Torres, I. Usefulness of Antioxidants as Adjuvant Therapy for Septic Shock: A Randomized Clinical Trial. Medicina 2020, 56, 619. [Google Scholar] [CrossRef]
- Falcone, M.; Russo, A.; Iacovelli, A.; Restuccia, G.; Ceccarelli, G.; Giordano, A.; Farcomeni, A.; Morelli, A.; Venditti, M. Predictors of outcome in ICU patients with septic shock caused by Klebsiella pneumoniae carbapenemase–producing K. pneumoniae. Clin. Microbiol. Infect. 2016, 22, 444–450. [Google Scholar] [CrossRef]
- Lopez-Cortes, L.E.; Cisneros, J.M.; Fernández-Cuenca, F.; Bou, G.; Tomas, M.; Garnacho-Montero, J.; Pascual, A.; Martinez-Martinez, L.; Vilá, J.; Pachón, J.; et al. Monotherapy versus combination therapy for sepsis due to multidrug-resistant Acinetobacter baumannii: Analysis of a multicentre prospective cohort. J. Antimicrob. Chemother. 2014, 69, 3119–3126. [Google Scholar] [CrossRef]
- Zafarullah, M.; Li, W.Q.; Sylvester, J.; Ahmad, M. Molecular mechanisms of N -acetylcysteine actions. Cell. Mol. Life Sci. 2003, 60, 6–20. [Google Scholar] [CrossRef]
- Harman, L.S.; Mottle, C.; Mason, R.P. Free radical metabolites of L-cysteine oxidation. J. Biol. Chem. 1984, 259, 5606–5611. [Google Scholar] [CrossRef]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Ferrer, R.; Artigas, A.; Suarez, D.; Palencia, E.; Levy, M.M.; Arenzana, A.; Pérez, X.L.; Sirvent, J.-M. Effectiveness of Treatments for Severe Sepsis. Am. J. Respir. Crit. Care Med. 2009, 180, 861–866. [Google Scholar] [CrossRef]
- Levy, M.M.; Artigas, A.; Phillips, G.S.; Rhodes, A.; Beale, R.; Osborn, T.; Vincent, J.-L.; Townsend, S.; Lemeshow, S.; Dellinger, R.P. Outcomes of the Surviving Sepsis Campaign in intensive care units in the USA and Europe: A prospective cohort study. Lancet Infect. Dis. 2012, 12, 919–924. [Google Scholar] [CrossRef]
- Tumbarello, M.; Viale, P.; Viscoli, C.; Trecarichi, E.M.; Tumietto, F.; Marchese, A.; Spanu, T.; Ambretti, S.; Ginocchio, F.; Cristini, F.; et al. Predictors of Mortality in Bloodstream Infections Caused by Klebsiella pneumoniae Carbapenemase-Producing K. pneumoniae: Importance of Combination Therapy. Clin. Infect. Dis. 2012, 55, 943–950. [Google Scholar] [CrossRef]
- Tumbarello, M.; Trecarichi, E.M.; de Rosa, F.G.; Giannella, M.; Giacobbe, D.R.; Bassetti, M.; Losito, A.R.; Bartoletti, M.; del Bono, V.; Corcione, S.; et al. Infections caused by KPC-producing Klebsiella pneumoniae: Differences in therapy and mortality in a multicentre study. J. Antimicrob. Chemother. 2015, 70, 2133–2143. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Bassetti, M.; Ceccarelli, G.; Carannante, N.; Losito, A.R.; Bartoletti, M.; Corcione, S.; Granata, G.; Santoro, A.; Giacobbe, D.R.; et al. Bloodstream infections caused by carbapenem-resistant Acinetobacter baumannii: Clinical features, therapy and outcome from a multicenter study. J. Infect. 2019, 79, 130–138. [Google Scholar] [CrossRef]
- Augustine, M.R.; Testerman, T.L.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Albrecht, H.; Al-Hasan, M.N. Clinical Risk Score for Prediction of Extended-Spectrum β-Lactamase–Producing Enterobacteriaceae in Bloodstream Isolates. Infect. Control. Hosp. Epidemiol. 2016, 38, 266–272. [Google Scholar] [CrossRef]
- Gutiérrez-Gutiérrez, B.; Salamanca, E.; de Cueto, M.; Hsueh, P.-R.; Viale, P.; Paño-Pardo, J.R.; Venditti, M.; Tumbarello, M.; Daikos, G.; Pintado, V.; et al. A Predictive Model of Mortality in Patients with Bloodstream Infections due to Carbapenemase-Producing Enterobacteriaceae. Mayo Clin. Proc. 2016, 91, 1362–1371. [Google Scholar] [CrossRef] [PubMed]
- Giannella, M.; Trecarichi, E.; de Rosa, F.; del Bono, V.; Bassetti, M.; Lewis, R.; Losito, A.; Corcione, S.; Saffioti, C.; Bartoletti, M.; et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae bloodstream infection among rectal carriers: A prospective observational multicentre study. Clin. Microbiol. Infect. 2014, 20, 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). European Antimicrobial Resistance Surveillance Network (EARS-Net). Available online: https://www.ecdc.europa.eu/en/home (accessed on 20 January 2021).
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
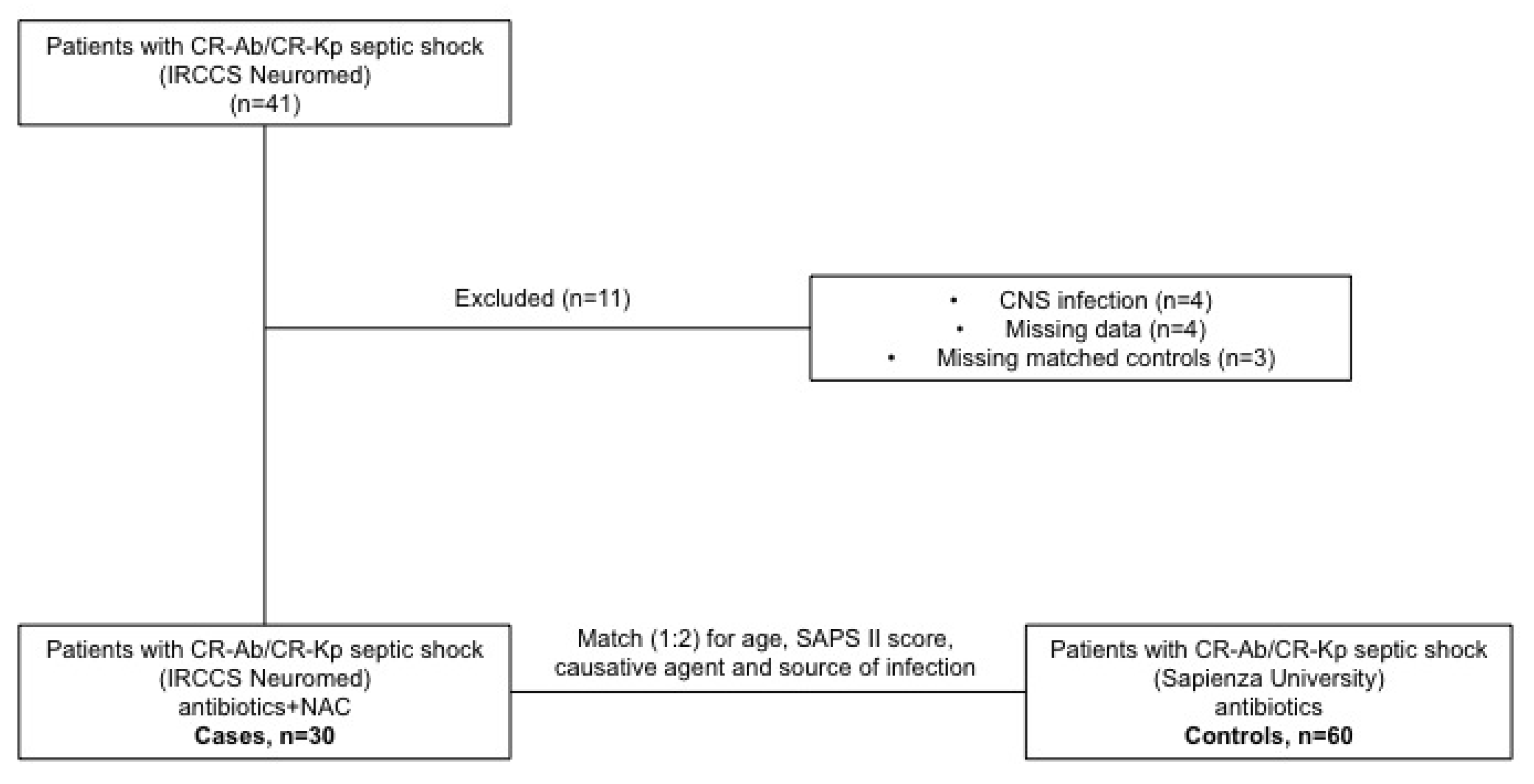
| Cases ° n = 30 | Controls ° n = 60 | p-Value | |
|---|---|---|---|
| Age, years (mean ± SD) | 58.1 ± 17.7 | 59.2 ± 14.19 | * |
| Male sex, n (%) | 24 (80) | 41 (68.3) | 0.32 |
| SAPS II | 35.33 ± 17.7 | 38.57 ± 11.5 | * |
| Lenght of ICU stay, days (mean ± SD) | 51.4 ± 27.9 | 27.8 ± 20 | <0.0001 |
| Previous (90-d) hospitalization, n (%) | 14 (46.6) | 21 (35) | 0.36 |
| Previous (90-d) ICU admission, n (%) | 4 (13.3) | 6 (10) | 0.72 |
| Previous (90-d) surgery, n (%) | 14 (43.3) | 17 (28.3) | 0.16 |
| Previous (90-d) antibiotic therapy, n (%) | 19 (63.3) | 29 (48.3) | 0.26 |
| Previous colonization with CR-Kp or CR-Ab, n (%) | 13 (43.3) | 17 (28.3) | 0.16 |
| Comorbidities, n (%) - chronic liver disease - neoplasm - diabetes mellitus - cardiovascular diseases - chronic renal failure - COPD | 6 (20) 6 (20) 6 (20) 18 (60) 0 (0) 3 (10) | 7 (11.6) 2 (3.3) 15 (25) 19 (31.6) 2 (3.3) 11 (18.3) | 0.34 0.01 0.79 0.01 0.55 0.37 |
| Causes of ICU admission, n (%) - respiratory failure - septic shock - stroke - post-surgery - trauma - cardiac arrest | 6 (20) 3 (10) 12 (40) 6 (20) 2 (6.6) 1 (3.3) | 20 (33.3) 14 (23.3) 4 (6.6) 7 (11.6) 9 (15) 6 (10) | 0.22 0.16 0.0002 0.34 0.32 0.41 |
| Source of infection, n (%) - pneumonia - primary bacteremia | 20 (66.7) 10 (33.3) | 40 (66.7) 20 (33.3) | * |
| Causative agent, n (%) - CR-Kp - CR-Ab | 18 (60) 12 (40) | 36 (60) 24 (40) | * |
| Colistin-resistant strains, n (%) | 8 (26.7) | 29 (31.7) | 0.54 |
| Adequate source control, n (%) | 10 (33.3) | 31 (51.6) | 0.12 |
| Number of antibiotics used as definitive therapy, n (%) - no definite therapy - 1 antibiotic - 2 antibiotics - 3 antibiotics - 4 antibiotics | 1 (3.4) 0 (0) 12 (40) 13 (43.3) 4 (13.3) | 1 (1.7) 5 (8.3) 19 (31.6) 28 (46.7) 7 (11.7) | 0.99 0.16 0.48 0.82 0.99 |
| Type of antimicrobial combinations, n (%) - Carbapenem-containing regimen - Colistin-containing regimen - Tigecycline-containing regimen - Aminoglycoside-containing regimen - Rifampin-containing regimen | 22 (73.3) 24 (80) 7 (23.3) 6 (20) 2 (6.7) | 44 (73.3) 33 (55) 33 (55) 8 (13.33) 13 (20) | 0.99 0.02 0.007 0.53 0.12 |
| ≥2 in-vitro active antibiotics within 24 h from septic shock, n (%) | 5 (16.7) | 14 (23.3) | 0.58 |
| ≥2 in-vitro active antibiotics definitive, n (%) | 6 (20) | 16 (26.7) | 0.60 |
| Time to initial definitive therapy, days (mean ± SD) | 2.7 ± 0.4 | 2.65 ± 0.2 | 0.86 |
| NAC dosage, mg/die (mean± SD) Range | 1520 ± 504 (1200–3000) | NA | |
| Length of antibiotic therapy, days (mean± SD) | 15.1 ± 7.9 | 12.3 ± 8.3 | 0.12 |
| Length of NAC therapy, days (mean± SD) | 16.6 ± 7.1 | NA | |
| Adverse effects of NAC therapy, n(%) | 0 (0) | NA | |
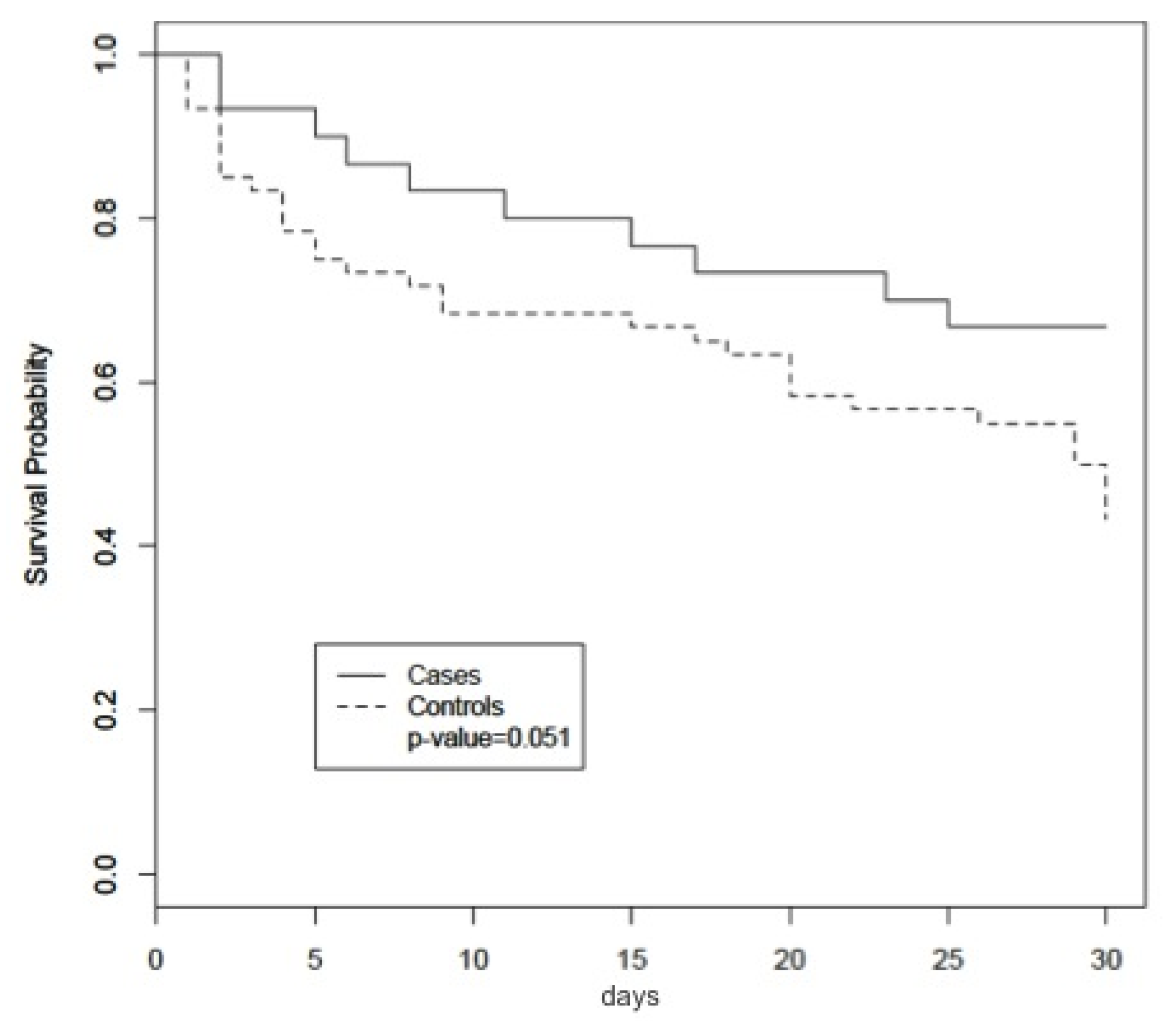
| Outcome, n (%) - 7-day mortality - 14-day mortality - 30-day mortality | 4 (13.3) 6 (20) 10 (33.3) | 15 (25) 19 (31.7) 34 (56.7) | 0.18 0.32 0.051 |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Controls (not receiving NAC) | 1.99 | 0.98–4.04 | 0.05 | 3.61 | 1.59–8.22 | 0.002 |
| Sex | 0.88 | 0.46–1.68 | 0.70 | 1.35 | 0.68–2.69 | 0.38 |
| Age | 1.02 | 1.00–1.05 | 0.015 | 1.02 | 0.99–1.05 | 0.17 |
| SAPS II | 1.01 | 0.99–1.03 | 0.30 | 1.01 | 0.98–1.05 | 0.25 |
| CR-Ab | 3.29 | 1.81–6.00 | <0.001 | 2.79 | 1.07–7.24 | 0.03 |
| ≥2 in-vitro active antibiotics | 0.22 | 0.08–0.63 | 0.005 | 0.21 | 0.06–0.73 | 0.014 |
| Number of antibiotics in definitive therapy | 0.69 | 0.47–1.03 | 0.07 | 0.65 | 0.39–1.09 | 0.10 |
| Pneumonia | 1.74 | 0.86–3.53 | 0.12 | 0.79 | 0.32–1.94 | 0.62 |
| Use of colistin | 0.94 | 0.51–1.73 | 0.86 | 0.50 | 0.19–1.32 | 0.16 |
| Time to definitive antibiotic therapy | 0.81 | 0.69–0.96 | 0.01 | 0.82 | 0.69–0.97 | 0.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliva, A.; Bianchi, A.; Russo, A.; Ceccarelli, G.; Cancelli, F.; Aloj, F.; Alunni Fegatelli, D.; Mastroianni, C.M.; Venditti, M. Effect of N-Acetylcysteine Administration on 30-Day Mortality in Critically Ill Patients with Septic Shock Caused by Carbapenem-Resistant Klebsiella pneumoniae and Acinetobacter baumannii: A Retrospective Case-Control Study. Antibiotics 2021, 10, 271. https://doi.org/10.3390/antibiotics10030271
Oliva A, Bianchi A, Russo A, Ceccarelli G, Cancelli F, Aloj F, Alunni Fegatelli D, Mastroianni CM, Venditti M. Effect of N-Acetylcysteine Administration on 30-Day Mortality in Critically Ill Patients with Septic Shock Caused by Carbapenem-Resistant Klebsiella pneumoniae and Acinetobacter baumannii: A Retrospective Case-Control Study. Antibiotics. 2021; 10(3):271. https://doi.org/10.3390/antibiotics10030271
Chicago/Turabian StyleOliva, Alessandra, Alessandro Bianchi, Alessandro Russo, Giancarlo Ceccarelli, Francesca Cancelli, Fulvio Aloj, Danilo Alunni Fegatelli, Claudio Maria Mastroianni, and Mario Venditti. 2021. "Effect of N-Acetylcysteine Administration on 30-Day Mortality in Critically Ill Patients with Septic Shock Caused by Carbapenem-Resistant Klebsiella pneumoniae and Acinetobacter baumannii: A Retrospective Case-Control Study" Antibiotics 10, no. 3: 271. https://doi.org/10.3390/antibiotics10030271
APA StyleOliva, A., Bianchi, A., Russo, A., Ceccarelli, G., Cancelli, F., Aloj, F., Alunni Fegatelli, D., Mastroianni, C. M., & Venditti, M. (2021). Effect of N-Acetylcysteine Administration on 30-Day Mortality in Critically Ill Patients with Septic Shock Caused by Carbapenem-Resistant Klebsiella pneumoniae and Acinetobacter baumannii: A Retrospective Case-Control Study. Antibiotics, 10(3), 271. https://doi.org/10.3390/antibiotics10030271