
Multidrug-Resistant Coagulase-Negative Staphylococci Isolated from Bloodstream in the uMgungundlovu District of KwaZulu-Natal Province in South Africa: Emerging Pathogens

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Results
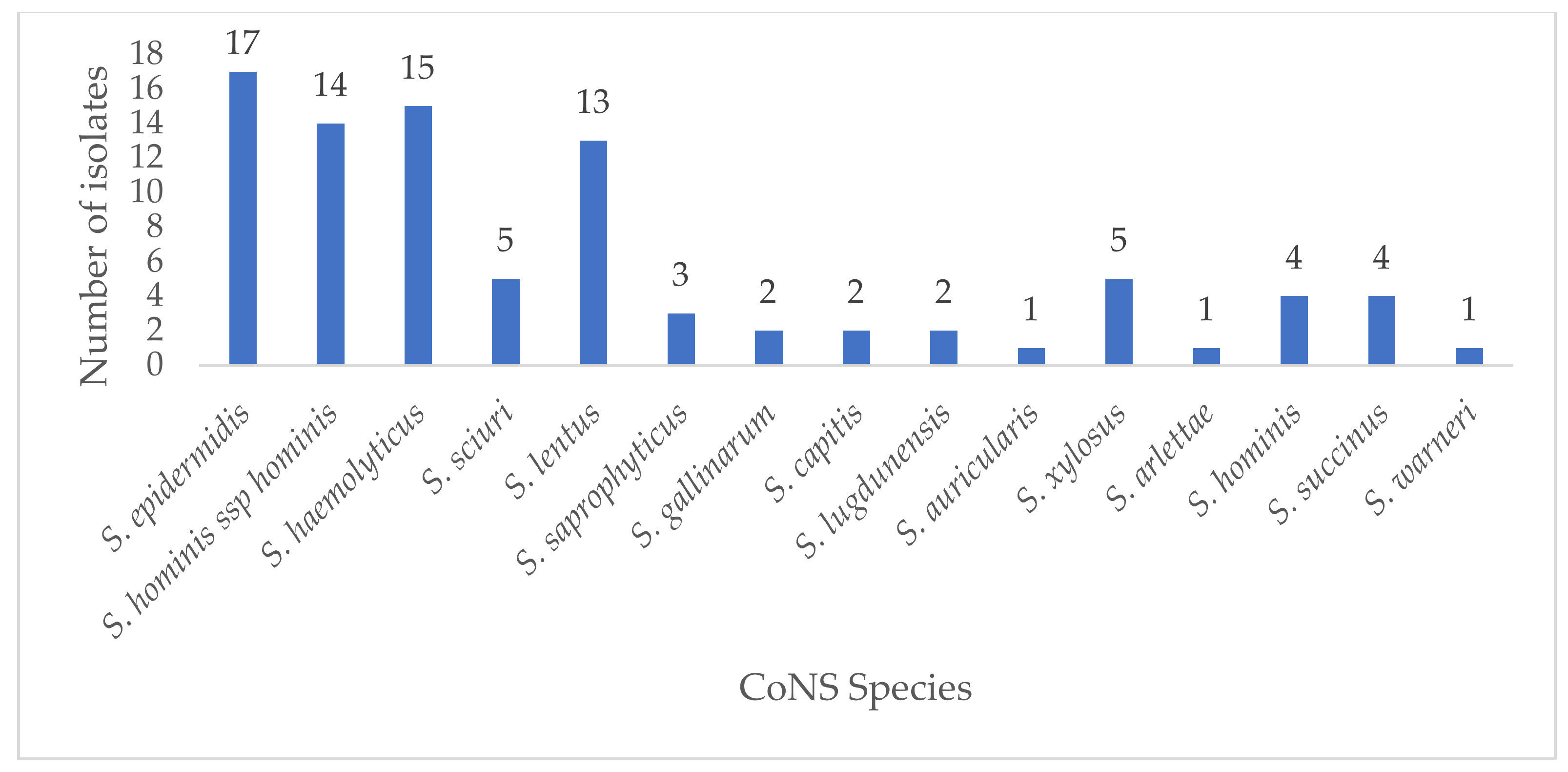
2.1. Isolation, Identification, and Species’ Distribution
2.2. Antibiotic Resistance Phenotypic Patterns of CoNS and mecA Detection
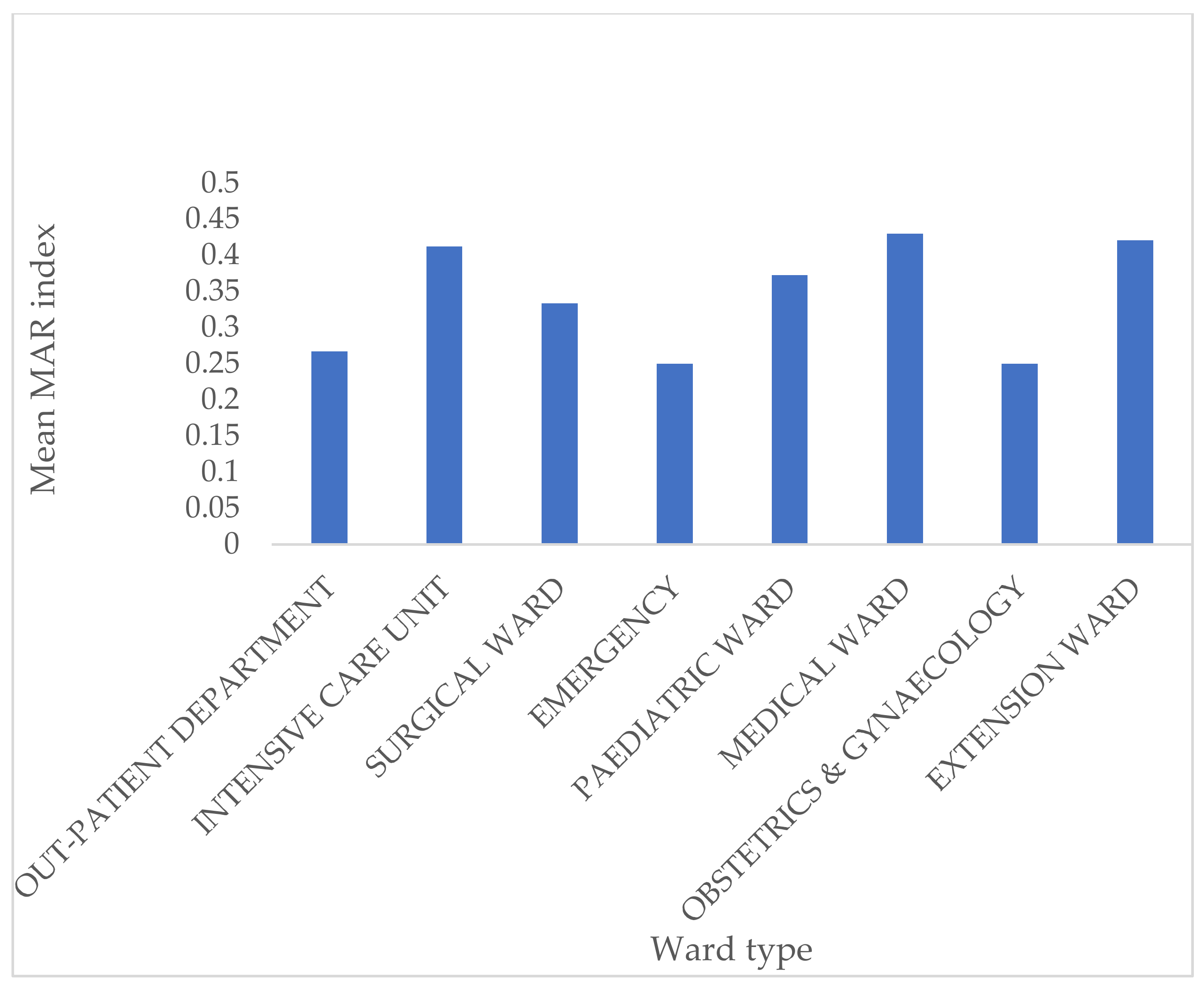
2.3. Multidrug Resistance and Multiple Antibiotic Resistance Index(MARI)
2.4. Demographic Characteristics of Patients and Statistical Analysis
3. Discussion
4. Materials and Methods
4.1. Ethical Considerations
4.2. Study Setting, Sample Collection, and Identification
4.3. Antimicrobial Susceptibility Testing and Determination of Methicillin-Resistant Coagulase-Negative Staphylococci (MRCoNS)
4.4. DNA Extraction and PCR Amplification of MecA
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gómez-Sanz, E.; Ceballos, S.; Ruiz-Ripa, L.; Zarazaga, M.; Torres, C. Clonally Diverse Methicillin and Multidrug Resistant Coagulase Negative Staphylococci Are Ubiquitous and Pose Transfer Ability Between Pets and Their Owners. Front. Microbiol. 2019, 10, 485. [Google Scholar] [CrossRef] [PubMed]
- Asante, J.; Amoako, D.G.; King, A.A.L.; Somboro, A.M.; Govinden, U.; Bester, L.A.; Essack, S.Y. Review of Clinically and Epidemiologically Relevant Coagulase-Negative Staphylococci in Africa. Microb. Drug Resist. 2020, 26, 951–970. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Heilmann, C.; Peters, G. Coagulase-Negative Staphylococci. Clin. Microbiol. Rev. 2014, 27, 870–926. [Google Scholar] [CrossRef] [PubMed]
- David, M.D.; Elliott, P.T. Coagulase-negative staphylococci. Br. J. Hosp. Med. 2015, 76, C126–C128. [Google Scholar] [CrossRef]
- García, P.; Benítez, R.; Lam, M.; Salinas, A.M.; Wirth, H.; Espinoza, C.F.; Garay, T.; Depix, M.S.; Labarca, J.; Guzmán, A.M. Coagulase-negative staphylococci: Clinical, microbiological and molecular features to predict true bacteraemia. J. Med Microbiol. 2004, 53, 67–72. [Google Scholar] [CrossRef]
- Iweriebor, C.; Ramalivhana, N.J.; Hattori, T.; Okoh, A.I.; Obi, C.L. Vancomycin resistant coagulase-negative Staphylococcal isolates from HIV positive patients in the Limpopo Province, South Africa. J. Microbiol. Antimicrob. 2013, 5, 18–24. [Google Scholar] [CrossRef][Green Version]
- May, L.; Klein, E.Y.; Rothman, R.E.; Laxminarayan, R. Trends in Antibiotic Resistance in Coagulase-Negative Staphylococci in the United States, 1999 to 2012. Antimicrob. Agents Chemother. 2013, 58, 1404–1409. [Google Scholar] [CrossRef]
- Amoako, D.G.; Somboro, A.M.; King, A.A.L.; Molechan, C.; Perrett, K.; Bester, L.A.; Essack, S.Y. Antibiotic Resistance in Staphylococcus aureus from Poultry and Poultry Products in uMgungundlovu District, South Africa, Using the “Farm to Fork” Approach. Microb. Drug Resist. 2020, 26, 402–411. [Google Scholar] [CrossRef]
- Mashaly, G.E.-S.; El-Mahdy, R. Vancomycin heteroresistance in coagulase negative Staphylococcus blood stream infections from patients of intensive care units in Mansoura University Hospitals, Egypt. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 63. [Google Scholar] [CrossRef]
- Natoli, S.; Fontana, C.; Favaro, M.; Bergamini, A.; Testore, G.P.; Minelli, S.; Bossa, M.C.; Casapulla, M.; Broglio, G.; Beltrame, A.; et al. Characterization of coagulase-negative staphylococcal isolates from blood with reduced susceptibility to glycopeptides and therapeutic options. BMC Infect. Dis. 2009, 9, 83. [Google Scholar] [CrossRef]
- Ibadin, E.; Enabulele, I.O.; Muinah, F. Prevalence of mecA gene among staphylococci from clinical samples of a tertiary hospital in Benin City, Nigeria. Afr. Heal. Sci. 2017, 17, 1000–1010. [Google Scholar] [CrossRef] [PubMed]
- Ballot, D.E.; Nana, T.; Sriruttan, C.; Cooper, P.A. Bacterial Bloodstream Infections in Neonates in a Developing Country. ISRN Pediatr. 2012, 2012, 508512. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, M.M.; Strasheim, W.; Lowe, M.; Ueckermann, V.; Kock, M.M. Molecular Epidemiology of Staphylococcus epidermidis Implicated in Catheter-Related Bloodstream Infections at an Academic Hospital in Pretoria, South Africa. Front. Microbiol. 2018, 9, 417. [Google Scholar] [CrossRef] [PubMed]
- Dhaouadi, S.; Soufi, L.; Campanile, F.; Dhaouadi, F.; Sociale, M.; Lazzaro, L.; Cherif, A.; Stefani, S.; Elandoulsi, R.B. Prevalence of meticillin-resistant and -susceptible coagulase-negative staphylococci with the first detection of the mecC gene among cows, humans and manure in Tunisia. Int. J. Antimicrob. Agents 2020, 55, 105826. [Google Scholar] [CrossRef]
- Becker, K.; van Alen, S.; Idelevich, E.A.; Schleimer, N.; Seggewiß, J.; Mellmann, A.; Kaspar, U.; Peters, G. Plasmid-Encoded Transferable mecB-Mediated Methicillin Resistance in Staphylococcus aureus. Emerg. Infect. Dis. 2018, 24, 242–248. [Google Scholar] [CrossRef]
- Adeyemi, A.I.; Sulaiman, A.A.; Solomon, B.B.; Chinedu, O.A.; Victor, I.A. Bacterial Bloodstream Infections in HIV-infected Adults Attending a Lagos Teaching Hospital. J. Heal. Popul. Nutr. 2010, 28, 318–326. [Google Scholar] [CrossRef]
- Klingenberg, C.; Rønnestad, A.; Anderson, A.; Abrahamsen, T.; Zorman, J.; Villaruz, A.; Flægstad, T.; Otto, M.; Sollid, J.E. Persistent strains of coagulase-negative staphylococci in a neonatal intensive care unit: Virulence factors and invasiveness. Clin. Microbiol. Infect. 2007, 13, 1100–1111. [Google Scholar] [CrossRef]
- Nicolosi, D.; Cinà, D.; Di Naso, C.; D’Angeli, F.; Salmeri, M.; Genovese, C. Antimicrobial Resistance Profiling of Coagulase-Negative Staphylococci in a Referral Center in South Italy: A Surveillance Study. Open Microbiol. J. 2020, 14, 91–97. [Google Scholar] [CrossRef]
- Center, K.J.; Reboli, A.C.; Hubler, R.; Rodgers, G.L.; Long, S.S. Decreased Vancomycin Susceptibility of Coagulase-Negative Staphylococci in a Neonatal Intensive Care Unit: Evidence of Spread of Staphylococcus warneri. J. Clin. Microbiol. 2003, 41, 4660–4665. [Google Scholar] [CrossRef]
- Paul, S.; Bezbaruah, R.L.; Roy, M.K.; Ghosh, A.C. Multiple antibiotic resistance (MAR) index and its reversion in Pseudomonas aeruginosa. Lett. Appl. Microbiol. 1997, 24, 169–171. [Google Scholar] [CrossRef]
- Patel, G.; Perez, F.; A Bonomo, R. Carbapenem-resistant Enterobacteriaceae and Acinetobacter baumannii: Assessing their impact on organ transplantation. Curr. Opin. Organ Transplant. 2010, 15, 676–682. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 6th ed.; Informational Supplement M100-S27; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2016; pp. 74–80. [Google Scholar]
- Martineau, F.; Picard, F.J.; Grenier, L.; Roy, P.H.; Ouellette, M.; Bergeron, M.G. Multiplex PCR assays for the detection of clinically relevant antibiotic resistance genes in staphylococci isolated from patients infected after cardiac surgery. J. Antimicrob. Chemother. 2000, 46, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Asante, J.; Govinden, U.; Owusu-Ofori, A.; Bester, L.; Essack, S. Molecular characterization of methicillin-resistant Staphylococcus aureus isolates from a hospital in Ghana. Afr. J. Clin. Exp. Microbiol. 2019, 20, 164. [Google Scholar] [CrossRef][Green Version]



{kind=link}
{kind=link}
| Antibiotic | CoNS Isolates (n = 89) | MRCoNS Isolates (n = 68) | ||||
|---|---|---|---|---|---|---|
| No of Susceptible (%) | No of Intermediate (%) | Number Resistant (%) | No of Susceptible (%) | No of Intermediate (%) | Number of Resistant (%) | |
| Cefoxitin | 21 (23.6) | NA | 68 (76.4) | 0 (0.0) | NA | 68 (100.0) |
| Penicillin G | 0 (0) | NA | 89 (100) | 0 (0.0) | NA | 68 (100.0) |
| Ceftaroline | 68 (76.4) | 12 (13.5) | 9 (10.1) | 50 (73.5) | 12 (17.6) | 6 (8.8) |
| Ciprofloxacin | 41 (46.1) | 10 (11.2) | 38 (42.7) | 25 (36.8) | 7 (10.3) | 36 (52.9) |
| Moxifloxacin | 46 (51.7) | 6 (6.7) | 37 (41.6) | 30 (44.1) | 5 (7.4) | 33 (48.5) |
| Azithromycin | 19 (21.3) | 4 (4.5) | 66 (74.2) | 8 (11.8) | 3 (4.4) | 57 (83.8) |
| Erythromycin | 17 (19.1) | 6 (6.7) | 66 (74.2) | 6 (8.8) | 5 (7.4) | 57 (83.8) |
| Gentamicin | 85 (95.5) | 2 (2.2) | 2 (2.2) | 64 (94.1) | 2 (2.9) | 2 (2.9) |
| Amikacin | 80 (89.9) | 5 (5.6) | 4 (4.5) | 61 (89.7) | 3 (4.4) | 4 (5.9) |
| Chloramphenicol | 64 (71.9) | 2 (2.2) | 23 (25.8) | 47 (69.1) | 2 (2.9) | 19 (27.9) |
| Tetracycline | 62 (69.7) | 4 (4.5) | 23 (25.8) | 44 (64.7) | 3 (4.4) | 21 (30.9) |
| Doxycycline | 65 (73.0) | 3 (3.4) | 21 (23.6) | 46 (67.4) | 2 (2.9) | 20 (29.4) |
| Teicoplanin | 73 (82.0) | 10 (11.2) | 6 (6.7) | 59 (86.8) | 4 (5.9) | 5 (7.4) |
| Tigecycline | 84 (94.4) | NA | 5 (5.6) | 64 (94.1) | NA | 4 (5.9) |
| Linezolid | 85 (95.5) | NA | 4 (4.5) | 65 (95.6) | NA | 3 (4.4) |
| Clindamycin | 47 (52.8) | 10 (11.2) | 32 (35.9) | 32 (47.1) | 7 (10.3) | 29 (42.6) |
| Rifampicin | 51 (57.3) | 0 (0.0) | 38 (42.7) | 34 (50.0) | 0 (0.0) | 34 (50.0) |
| Sulfamethoxazole/trimethoprim | 24 (26.9) | 4 (4.5) | 61 (68.5) | 16 (23.5) | 3 (4.4) | 49 (72.1) |
| Nitrofurantoin | 82 (92.1) | 2 (2.2) | 5 (5.6) | 63 (92.6) | 2 (2.9) | 3 (4.4) |
| Vancomycin * | 77 (86.5) | 13 (13.5) | 0 (0.0) | 62 (91.2) | 6 (8.8) | 0 (0.0) |
| MAR Index | Number of Isolates |
|---|---|
| 0.05 | 5 (5.6%) |
| 0.10 | 5 (5.6%) |
| 0.15 | 10 (11.2%) |
| 0.20 | 5 (5.6%) |
| 0.25 | 10 (11.2%) |
| 0.30 | 6 (6.7%) |
| 0.35 | 8 (8.9%) |
| 0.40 | 12 (13.5%) |
| 0.45 | 10 (11.2%) |
| 0.50 | 8 (8.9%) |
| 0.55 | 2 (2.2%) |
| 0.60 | 6 (6.7%) |
| 0.70 | 1 (1.1%) |
| 0.80 | 1 (1.1%) |
| Department | Number of Isolates with MAR Index > 0.2 (n = 64) | Percentage |
|---|---|---|
| Emergency | 5 | 7.8% |
| ICU | 11 | 17.2% |
| Medical Ward | 10 | 15.6% |
| Obstetrics/gynecology | 1 | 1.6% |
| OPD | 7 | 10.9% |
| Surgical Ward | 5 | 7.8% |
| Extension Ward | 7 | 10.9% |
| Pediatric Ward | 9 | 14.1% |
| Resistance Pattern 1 | Number |
|---|---|
| FOX-PEN-CIP-MXF-AZM-ERY-GEN-CLI-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CHL-CLI-RIF-SXT | 3 |
| PEN- AZM-ERY-CHL-CLI-SXT | 1 |
| PEN-CPT-CHL-RIF-NIT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CLI-RIF | 4 |
| FOX-PEN-CIP-MXF-AZM-ERY-GEN-DOX-RIF-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-AMK-CLI-RIF | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CHL-TET-DOX-TGC-TEC-LZD-CLI-RIF-SXT-NIT | 1 |
| FOX-PEN-MXF-AZM-ERY-CHL-CLI | 1 |
| PEN-AZM-ERY-SXT | 3 |
| FOX-PEN-AZM-ERY-SXT | 6 |
| PEN-CPT-MXF- CHL-TET-DOX-TGC-TEC-LZD-RIF-SXT-NIT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CLI-RIF-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-TET-DOX-RIF-SXT | 2 |
| FOX-PEN-AMK-CHL-TET-DOX-TGE-TGC-LZD-RIF-SXT-NIT | 1 |
| FOX-PEN-CPT-CIP-MXF-AZM-ERY-CHL-TET-DOX-CLI-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CHL-TET-DOX-TGC-TEC-LZD-RIF-SXT-NIT | 1 |
| PEN- CIP-MXF-AZM-ERY-CHL-CLI-RIF-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CHL-TET-DOX-CLI-RIF-SXT | 2 |
| FOX-PEN-MXF-AZM-ERY-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-AMK-CHL-CLI-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-TET-CLI-RIF | 1 |
| FOX-PEN-AZM-ERY-CLI-RIF-SXT | 1 |
| FOX-PEN-CPT-MXF-AZM-ERY-TET-DOX-CLI-RIF-SXT | 1 |
| FOX-PEN-CPT-CIP-MXF-AZM-ERY-AMK-CHL-CLI-RIF-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-RIF-SXT | 1 |
| FOX-PEN-AZM-ERY-CHL-TET-DOX-SXT | 2 |
| PEN-MXF-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CLI-RIF-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-TET-DOX-CLI-RIF-SXT | 1 |
| FOX-PEN-AZM-ERY-TET-CLI | 1 |
| PEN-CIP-MXF-AZM-ERY-TET-CLI-RIF-SXT | 1 |
| FOX-PEN-CIP-AZM-ERY-TET-DOX-RIF-SXT | 1 |
| FOX-PEN-TET-DOX-TGC-RIF | 1 |
| FOX-PEN-AZM-ERY-RIF | 1 |
| FOX-PEN-CPT-AZM-ERY-TET-DOX-SXT | 2 |
| FOX-PEN-AZM-ERY-CHL-SXT | 1 |
| FOX-PEN-AZM-ERY-CHL-CLI-RIF-SXT | 2 |
| FOX-PEN-CIP-MXF-AZM-ERY-CLI-SXT | 1 |
| FOX-PEN-CIP-AZM-ERY-TET-DOX-SXT | 1 |
| FOX-PEN-CPT-CIP-AZM-ERY-CLI-RIF-SXT | 1 |
| FOX-PEN-CIP-AZM-ERY-TET-DOX | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CHL-TET-DOX-SXT | 1 |
| FOX-PEN-CIP-AZM-ERY-CLI-SXT | 1 |
| FOX-PEN-CIP-MXF-ERY-RIF | 1 |
| FOX-PEN-AZM-ERY-TEC-RIF-SXT | 1 |
| FOX-PEN-AZM-ERY-TEC | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-CHL-CLI-SXT | 1 |
| FOX-PEN-CIP-MXF-AZM-ERY-RIF | 1 |
| FOX-PEN-CIP-MXF-RIF | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asante, J.; Hetsa, B.A.; Amoako, D.G.; Abia, A.L.K.; Bester, L.A.; Essack, S.Y. Multidrug-Resistant Coagulase-Negative Staphylococci Isolated from Bloodstream in the uMgungundlovu District of KwaZulu-Natal Province in South Africa: Emerging Pathogens. Antibiotics 2021, 10, 198. https://doi.org/10.3390/antibiotics10020198
Asante J, Hetsa BA, Amoako DG, Abia ALK, Bester LA, Essack SY. Multidrug-Resistant Coagulase-Negative Staphylococci Isolated from Bloodstream in the uMgungundlovu District of KwaZulu-Natal Province in South Africa: Emerging Pathogens. Antibiotics. 2021; 10(2):198. https://doi.org/10.3390/antibiotics10020198
Chicago/Turabian StyleAsante, Jonathan, Bakoena A. Hetsa, Daniel G. Amoako, Akebe Luther King Abia, Linda A. Bester, and Sabiha Y. Essack. 2021. "Multidrug-Resistant Coagulase-Negative Staphylococci Isolated from Bloodstream in the uMgungundlovu District of KwaZulu-Natal Province in South Africa: Emerging Pathogens" Antibiotics 10, no. 2: 198. https://doi.org/10.3390/antibiotics10020198
APA StyleAsante, J., Hetsa, B. A., Amoako, D. G., Abia, A. L. K., Bester, L. A., & Essack, S. Y. (2021). Multidrug-Resistant Coagulase-Negative Staphylococci Isolated from Bloodstream in the uMgungundlovu District of KwaZulu-Natal Province in South Africa: Emerging Pathogens. Antibiotics, 10(2), 198. https://doi.org/10.3390/antibiotics10020198