
Impact of the COVID-19 Pandemic on Antibiotic Prescribing for Common Infections in The Netherlands: A Primary Care-Based Observational Cohort Study

 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Study Population
2.2. Number of Common Infectious Disease Episodes, in Total and with Antibiotic Prescription
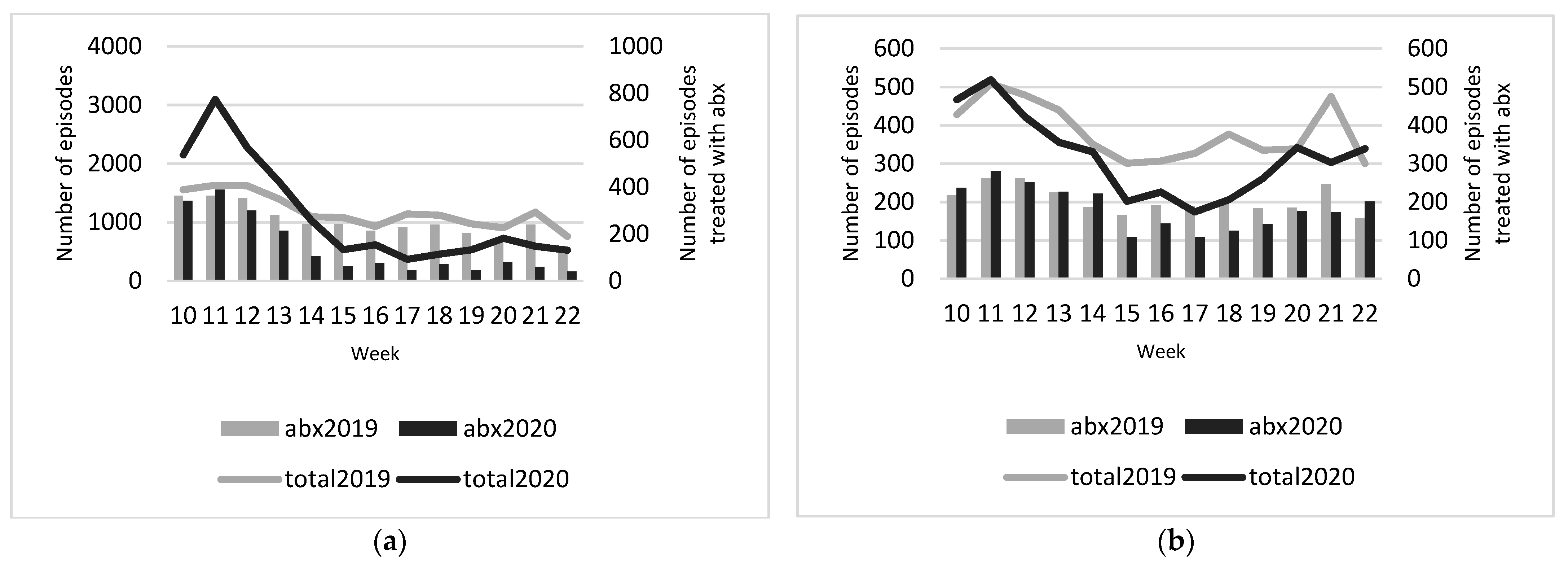
2.3. Number of Infectious Disease Episodes and Episodes with Antibiotic Prescription during the Pandemic Weeks
2.4. Respiratory Tract and Ear Infections: Differences between Age Groups
2.5. Analysis of Specific Diagnoses, Including Complications
2.6. Remote-Only GP Consultations for Respiratory Tract and Ear Infections
3. Discussion
4. Materials and Methods
4.1. Objectives
4.2. Design and Study Population
4.3. Data Extraction
4.4. Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| ICPC Chapter | Months: March through May 2019 and March through May 2020 |
|---|---|
| H Ear/Respiratory | H71 acute otitis media H99 ear/mastoid disease H01 earache H04 ear discharge H70 otitis externa H72 serous otitis media H74 chronic otitis media/other otitis H74.01 chronic otitis media H74.02 mastoiditis R21 throat symptoms R22 tonsil symptoms R72 strep throat R74 acute upper RTI R76 tonsillitis/tonsillar abscess R76.01 tonsillitis R76.02 tonsillar abscess R77 laryngitisR80 influenza R83 other RTI R05 cough R09 sinus symptoms R75 sinusitis R78 bronchitis R81 pneumonia R82 pleurisy R71 whooping cough R70 tuberculosis |
| U Urinary | U01 dysuria U02 urgency U71 cystitis U70 pyelonephritis Y73 prostatitis |
| D Digestive | D11 diarrhoea D70 gastrointestinal infection D73 gastroenteritis D22 parasites D92 diverticular disease |
| S Skin | S09 infected finger/toe S10 boil/carbuncle S11 skin infection post-traumatic S76 other skin infection S84 impetigo |
References
- Dunlop, C.; Howe, A.; Li, D.; Allen, L.N. The coronavirus outbreak: The central role of primary care in emergency preparedness and response. BJGP Open 2020, 4. [Google Scholar] [CrossRef] [PubMed]
- Krist, A.H.; DeVoe, J.E.; Cheng, A.; Ehrlich, T.; Jones, S.M. Redesigning Primary Care to Address the COVID-19 Pandemic in the Midst of the Pandemic. Ann. Fam. Med. 2020, 18, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Leis, J.A.; Born, K.B.; Theriault, G.; Ostrow, O.; Grill, A.; Johnston, K.B. Using antibiotics wisely for respiratory tract infection in the era of covid-19. BMJ 2020, 371, m4125. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.N.; Shi, Z.; Gidengil, C.A.; Poon, S.J.; Uscher-Pines, L.; Mehrotra, A. Antibiotic Prescribing During Pediatric Direct-to-Consumer Telemedicine Visits. Pediatrics 2019, 143. [Google Scholar] [CrossRef] [PubMed]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Chatterjee, A.; Modarai, M.; Naylor, N.R.; Boyd, S.E.; Atun, R.; Barlow, J.; Holmes, A.H.; Johnson, A.; Robotham, J.V. Quantifying drivers of antibiotic resistance in humans: A systematic review. Lancet Infect. Dis 2018, 18, e368–e378. [Google Scholar] [CrossRef]
- Petersen, I.; Johnson, A.M.; Islam, A.; Duckworth, G.; Livermore, D.M.; Hayward, A.C. Protective effect of antibiotics against serious complications of common respiratory tract infections: Retrospective cohort study with the UK General Practice Research Database. BMJ 2007, 335, 982. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Nellums, L.B. Antibiotic prescribing in general practice during COVID-19. Lancet Infect. Dis 2020. [Google Scholar] [CrossRef]
- McBride, J.A.; Eickhoff, J.; Wald, E.R. Impact of COVID-19 Quarantine and School Cancelation on Other Common Infectious Diseases. Pediatr Infect. Dis J. 2020, 39, e449–e452. [Google Scholar] [CrossRef] [PubMed]
- Han, S.M.; Greenfield, G.; Majeed, A.; Hayhoe, B. Impact of Remote Consultations on Antibiotic Prescribing in Primary Health Care: Systematic Review. J. Med. Internet Res. 2020, 22, e23482. [Google Scholar] [CrossRef] [PubMed]
- European Center for Disease Control. Antimicrobial Consumption in the EU/EEA, Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2019.
- Surveillance Atlas of Infectious Disease. Available online: http://atlas.ecdc.europa.eu/public/index.aspx (accessed on 3 February 2021).
- van der Velden, A.W.; Pijpers, E.J.; Kuyvenhoven, M.M.; Tonkin-Crine, S.K.G.; Little, P.; Verheij, T.J.M. Effectiveness of physician-targeted interventions to improve antibiotic use for respiratory tract infections. Br. J. Gen. Pract 2012, 62, e801–e807. [Google Scholar] [CrossRef] [PubMed]
- Verheij, T.J.M.; Hopstaken, R.M.; Prins, J.M. Acuut Hoesten. 2011. Available online: https://richtlijnen.nhg.org/files/pdf/77_Acuut%20hoesten_februari-2011.pdf (accessed on 17 February 2021).
- Damoiseaux, R.A.M.J.; Venekamp, R.P.; Eekhof, J.A.H.; Bennebroek Gravenhorst, F.M.; Schoch, A.G.; Burgers, J.S.; Bouma, M.; Wittenberg, J. Otitis Media Acuta bij Kinderen. 2014. Available online: https://richtlijnen.nhg.org/standaarden/otitis-media-acuta-bij-kinderen (accessed on 17 February 2021).
- Smeets, H.M.; Kortekaas, M.F.; Rutten, F.H.; Bots, M.L.; van der Kraan, W.; Daggelders, G.; Smits-Pelser, H.; Helsper, C.W.; Hoes, A.W.; de Wit, N.J. Routine primary care data for scientific research, quality of care programs and educational purposes: The Julius General Practitioners’ Network (JGPN). BMC Health Serv Res. 2018, 18, 735. [Google Scholar] [CrossRef] [PubMed]
- Soler, J.K.; Okkes, I.; Wood, M.; Lamberts, H. The coming of age of ICPC: Celebrating the 21st birthday of the International Classification of Primary Care. Fam. Pract 2008, 25, 312–317. [Google Scholar] [CrossRef] [PubMed]


| Episodes Total | Episodes with Antibiotics | Prescription Rate | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | n | RR (CI) | n | n | RR (CI) | % | % | % 2020 minus % 2019 (CI) | |
| Year | 2019 * | 2020 * | 2019 | 2020 | 2019 | 2020 | |||
| Resp/ear | 16,672 | 15,580 | 0.90 (0.88 to 0.92) † | 3567 | 2022 | 0.54 (0.52 to 0.58) † | 21% | 13% | −8.0% (−8.8% to −7.2%) † |
| Urinary | 5376 | 4421 | 0.79 (0.76 to 0.82) † | 2893 | 2540 | 0.84 (0.80 to 0.89) † | 54% | 57% | 3.0% (1.0% to 5.0%) † |
| GI | 2367 | 1338 | 0.54 (0.51 to 0.58) † | 73 | 58 | 0.76 (0.54 to 1.08) | 3% | 4% | 1.0% (−0.2% to 2.3%) † |
| Skin | 2848 | 2103 | 0.71 (0.67 to 0.75) † | 892 | 707 | 0.76 (0.69 to 0.84) † | 31% | 34% | 3.0% (0.4% to 5.6%) † |
| Total | 27,263 | 23,442 | 0.83 (0.81 to 0.84) † | 7425 | 5327 | 0.69 (0.67 to 0.71) † | 27% | 23% | −4.0% (−4.8% to −3.2%) † |
| Age | Registered Patients | Episodes Total | Episodes with Antibiotics | Prescription Rate | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | n | n | n | RR (CI) | n | n | RR (CI) | % | % | % 2020 minus % 2019 (CI) | |
| 2019 | 2020 | 2019 | 2020 | 2019 | 2020 | 2019 | 2020 | ||||
| 0–12 | 61,414 | 62,505 | 4262 | 2651 | 0.61 (0.58 to 0.64) † | 943 | 428 | 0.44 (0.40 to 0.50) † | 22% | 16% | −6.0% (−7.8% to −4.1%) † |
| 13–40 | 156,535 | 166,306 | 4998 | 5166 | 0.94 (0.91 to 0.98) † | 960 | 530 | 0.52 (0.47 to 0.58) † | 19% | 10% | −9.0% (−10.4% to −7.6%) † |
| 41–65 | 120,787 | 123,710 | 4555 | 5322 | 1.14 (1.10 to 1.19) † | 932 | 614 | 0.64 (0.58 to 0.71) † | 20% | 12% | −8.0% (−9.5% to −6.6%) † |
| >65 | 50,968 | 53,163 | 2857 | 2441 | 0.82 (0.78 to 0.86) † | 732 | 450 | 0.59 (0.52 to 0.66) † | 26% | 18% | −8.0% (−10.2 to −5.8%) † |
| Total | 389,704 * | 405,684 * | 16,672 | 15,580 | 0.90 (0.88 to 0.92) † | 3567 | 2022 | 0.54 (0.52 to 0.58) † | 21% | 13% | −8.0% (−8.8% to −7.2%) † |
| Year of Episode | Cough R05 | Influenza R80 | Bronchitis/ Bronchiolitis R78 | Acute Otitis Media H71 | Cystitis U71 | Acute Upper RTI R74 | Other RTI Including COVID-19 R83 | ||
|---|---|---|---|---|---|---|---|---|---|
| 2019 * | Episodes Total | n | 4194 | 282 | 582 | 1445 | 3619 | 3734 | 114 |
| Episodes with abx | n | 548 | 30 | 272 | 675 | 2523 | 521 | 29 | |
| Prescription Rate | % | 13% | 11% | 47% | 47% | 70% | 14% | 25% | |
| 2020 * | Episodes Total | n | 4487 | 466 | 319 | 562 | 3067 | 5001 | 831 |
| RR (CI) | 1.03 (0.99 to 1.07) | 1.59 (1.37 to 1.84) † | 0.53 (0.46 to 0.60) † | 0.37 (0.34 to 0.41) † | 0.81 (0.78 to 0.85) † | 1.29 (1.23 to 1.34) † | 7.00 (5.76 to 8.52) † | ||
| Episodes with abx | n | 360 | 29 | 102 | 257 | 2223 | 493 | 118 | |
| RR (CI) | 0.63 (0.55 to 0.72) † | 0.93 (0.56 to 1.55) | 0.36 (0.29 to 0.45) † | 0.37 (0.32 to 0.42) † | 0.85 (0.80 to 0.90) † | 0.91 (0.80 to 1.03) | 3.91 (2.60 to 5.87) † | ||
| Prescription Rate | % | 8% | 6% | 32% | 46% | 72% | 10% | 14% | |
| % 2020 minus % 2019 (CI) | −5.0% (−6.3 to −3.7%) † | −5.0% (−9.6% to −1.0%) † | −15.0% (−21.3% to −8.3%) † | −1.0% (−5.8 to 3.9%) | 2% (−0.2% to 4.2%) | −4.0% (−5.4% to −2.6%) † | −11.0% (−19.9% to −3.5%) † |
| Year of Episode | Pneumonia R81 | Mastoiditis H74_02 | Pyelonephritis U70 | ||
|---|---|---|---|---|---|
| 2019 ** | Episodes Total | n | 947 | 11 | 98 |
| Episodes with abx | n | 592 * | 5 * | 62 * | |
| Prescription rate | % | 63% | 46% | 63% | |
| 2020 ** | Episodes Total | n | 590 | 14 | 95 |
| RR (CI) | 0.60 (0.54 to 0.66) † | 1.22 (0.56 to 2.69) | 0.93 (0.70 to 1.23) | ||
| Episodes with abx | n | 292 * | 2 * | 60 * | |
| RR (CI) | 0.47 (0.41 to 0.54) † | 0.38 (0.07 to 1.98) | 0.93 (0.65 to 1.33) | ||
| Prescription rate | % | 50% | 67% | 63% | |
| % 2020 minus % 2019 (CI) | −13% (7.9% to 18%) † | 21% (−15.9% to 51.6%) | 0% (−13.4% to 13.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Pol, A.C.; Boeijen, J.A.; Venekamp, R.P.; Platteel, T.; Damoiseaux, R.A.M.J.; Kortekaas, M.F.; van der Velden, A.W. Impact of the COVID-19 Pandemic on Antibiotic Prescribing for Common Infections in The Netherlands: A Primary Care-Based Observational Cohort Study. Antibiotics 2021, 10, 196. https://doi.org/10.3390/antibiotics10020196
van de Pol AC, Boeijen JA, Venekamp RP, Platteel T, Damoiseaux RAMJ, Kortekaas MF, van der Velden AW. Impact of the COVID-19 Pandemic on Antibiotic Prescribing for Common Infections in The Netherlands: A Primary Care-Based Observational Cohort Study. Antibiotics. 2021; 10(2):196. https://doi.org/10.3390/antibiotics10020196
Chicago/Turabian Stylevan de Pol, Alma C., Josi A. Boeijen, Roderick P. Venekamp, Tamara Platteel, Roger A. M. J. Damoiseaux, Marlous F. Kortekaas, and Alike W. van der Velden. 2021. "Impact of the COVID-19 Pandemic on Antibiotic Prescribing for Common Infections in The Netherlands: A Primary Care-Based Observational Cohort Study" Antibiotics 10, no. 2: 196. https://doi.org/10.3390/antibiotics10020196
APA Stylevan de Pol, A. C., Boeijen, J. A., Venekamp, R. P., Platteel, T., Damoiseaux, R. A. M. J., Kortekaas, M. F., & van der Velden, A. W. (2021). Impact of the COVID-19 Pandemic on Antibiotic Prescribing for Common Infections in The Netherlands: A Primary Care-Based Observational Cohort Study. Antibiotics, 10(2), 196. https://doi.org/10.3390/antibiotics10020196