
A Culture Change: Impact of a Pediatric Antimicrobial Stewardship Program Based on Guideline Implementation and Prospective Audit with Feedback

Abstract
:1. Introduction
2. Results
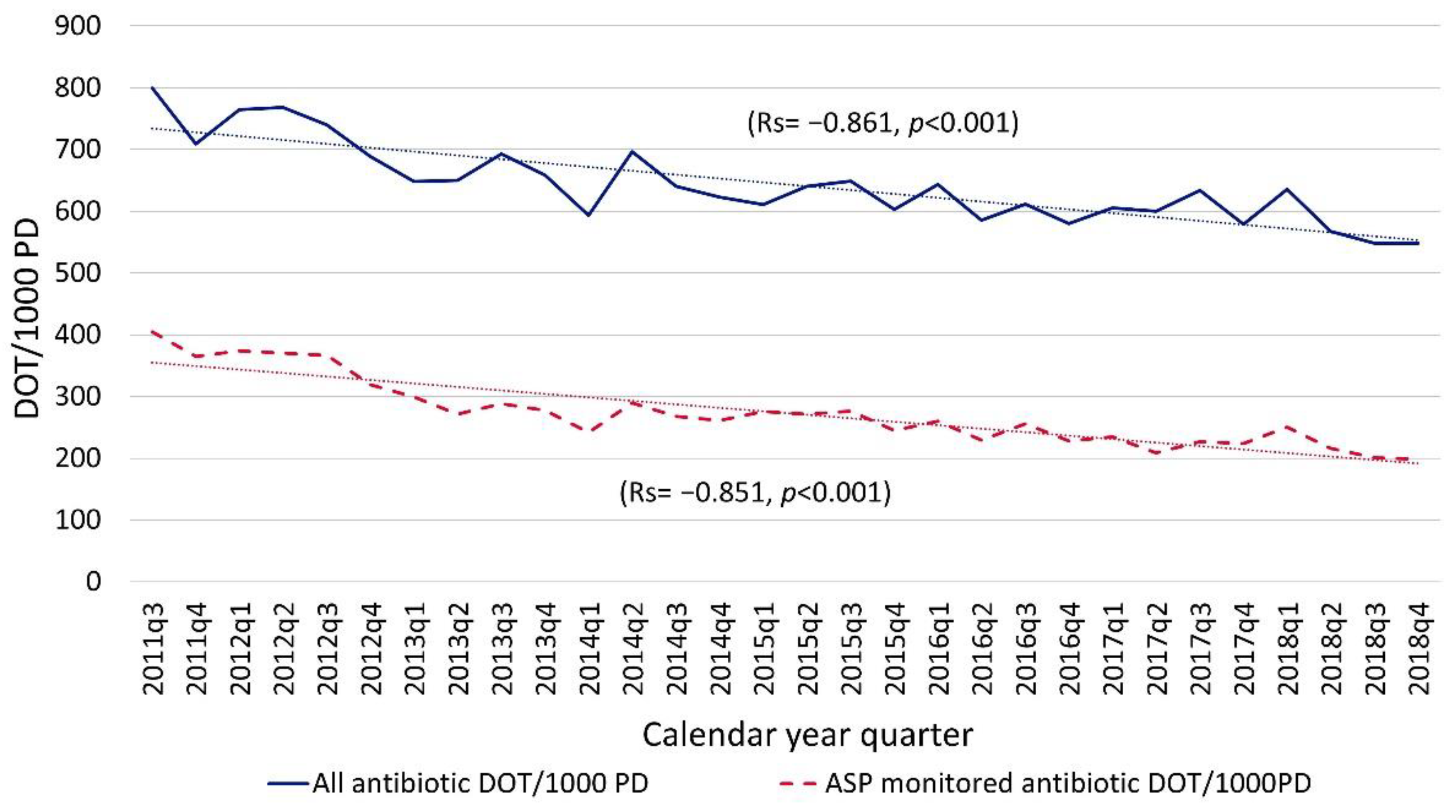
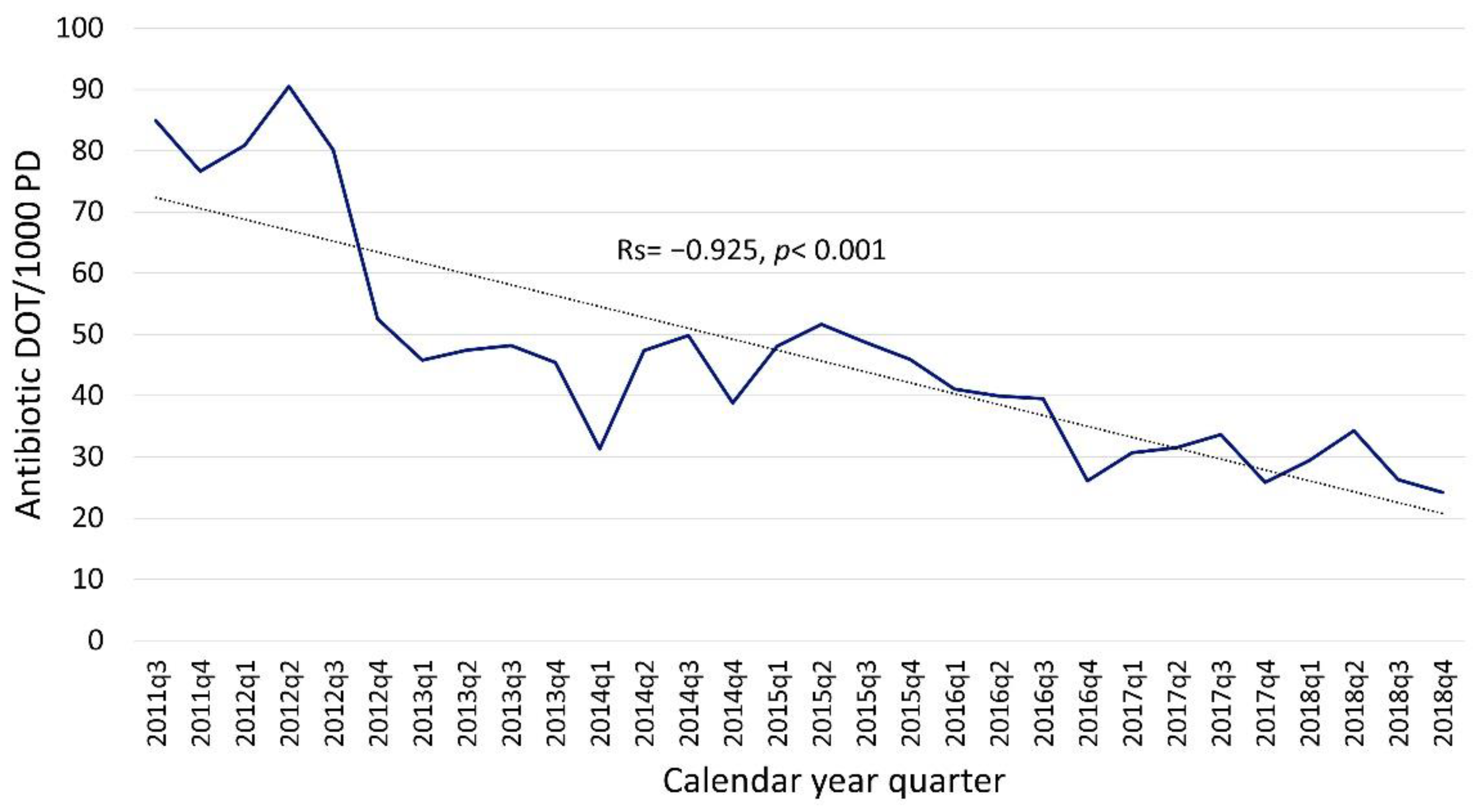
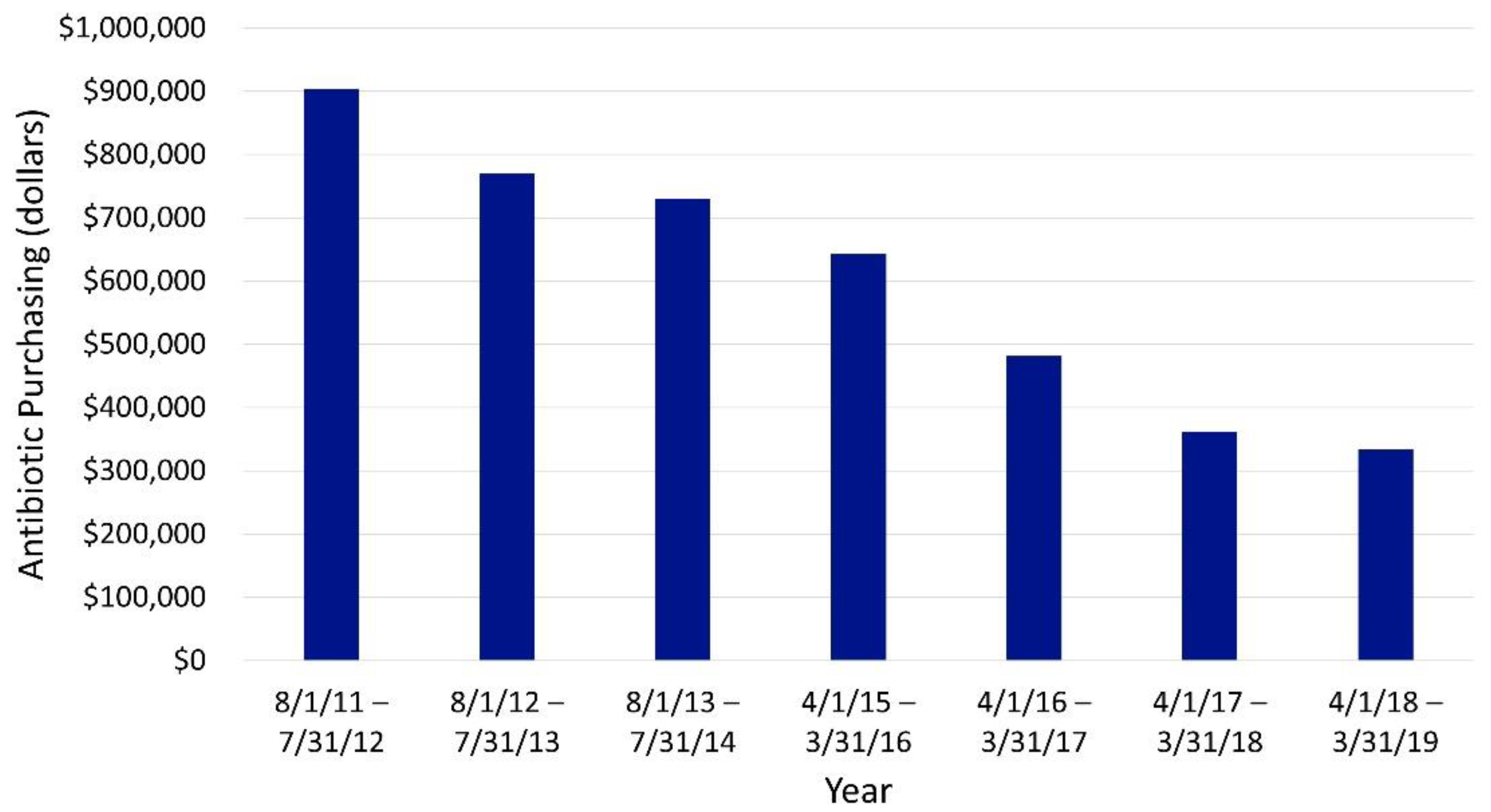
2.1. Process-Related Measures
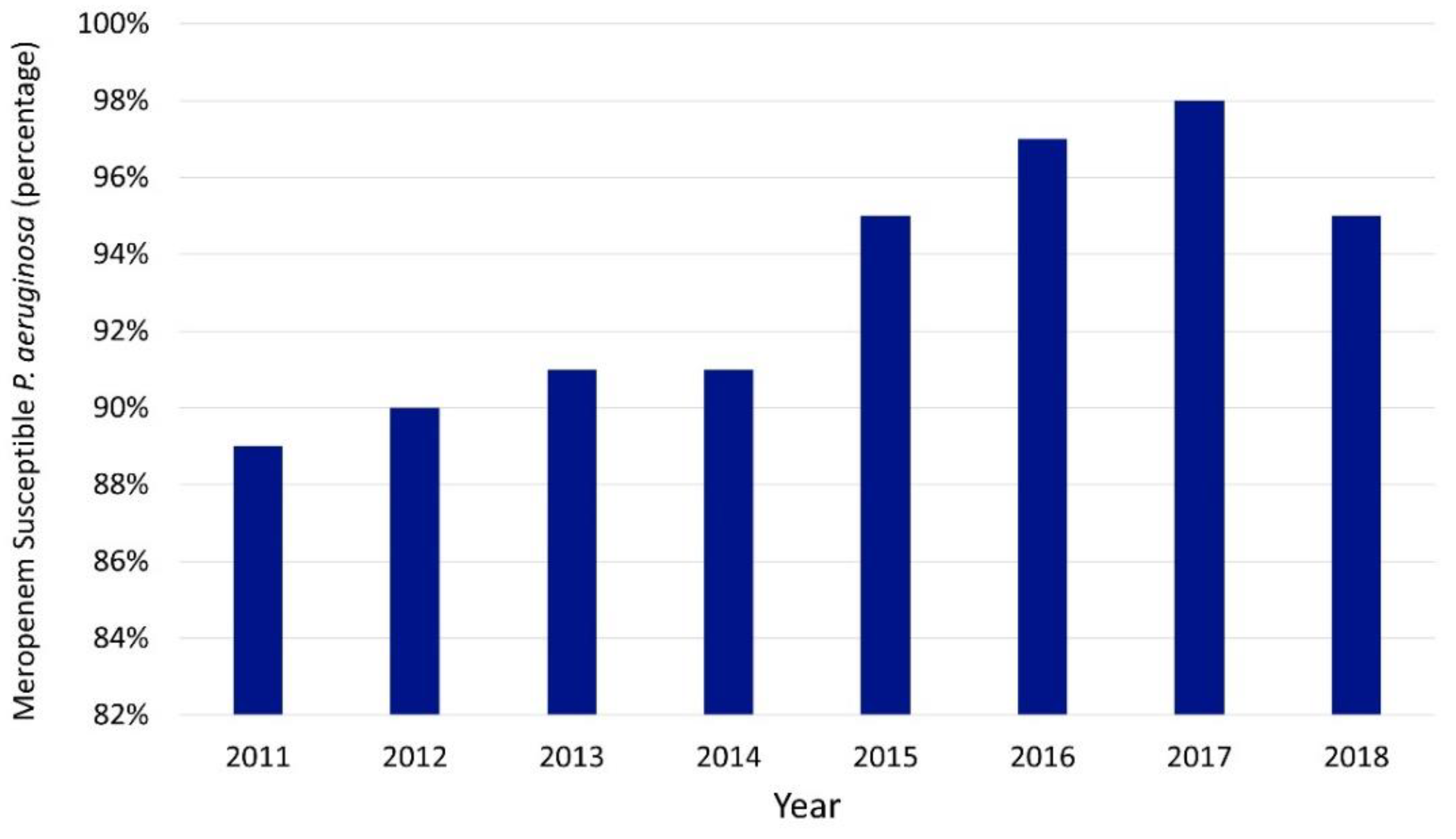
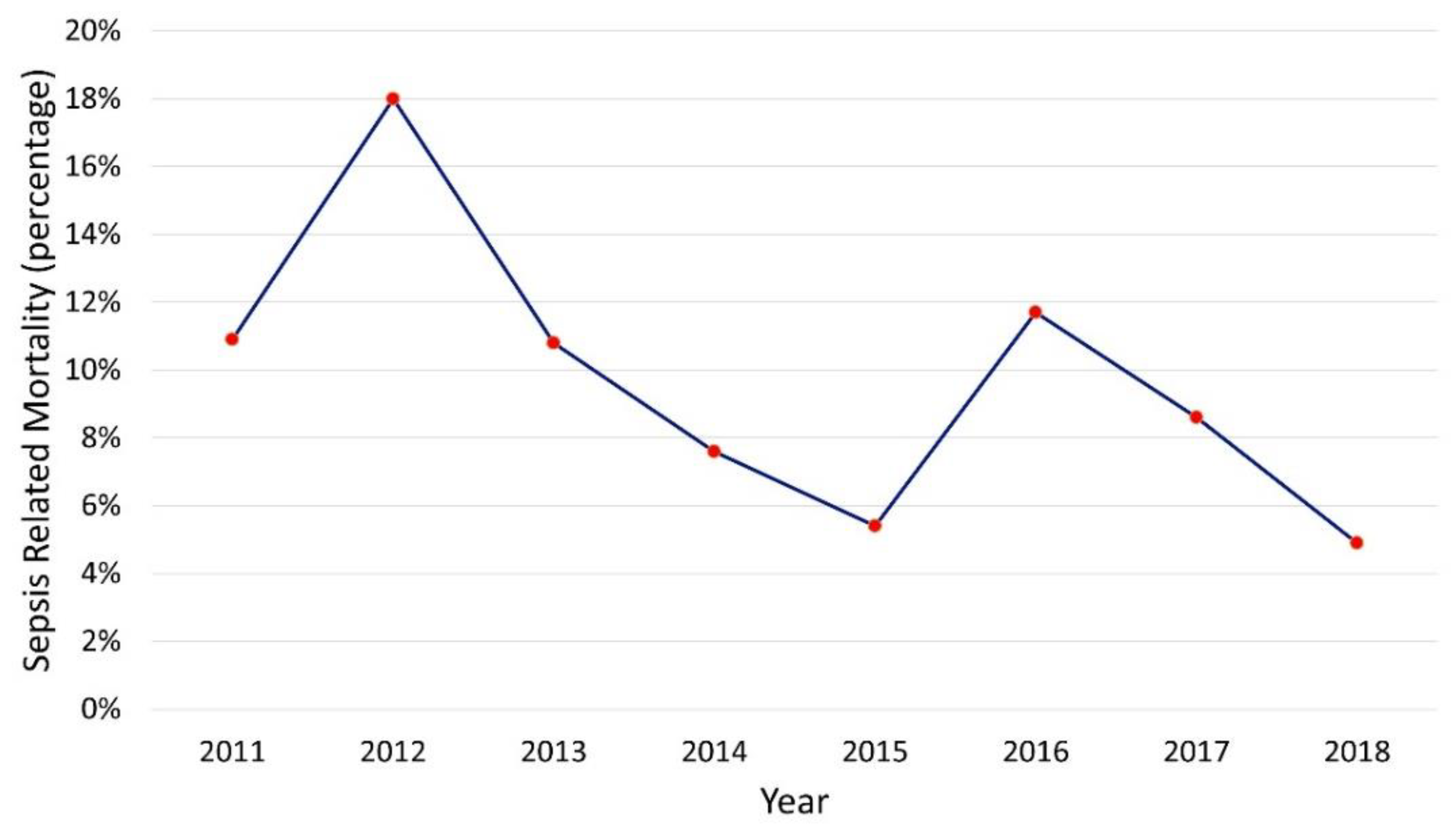
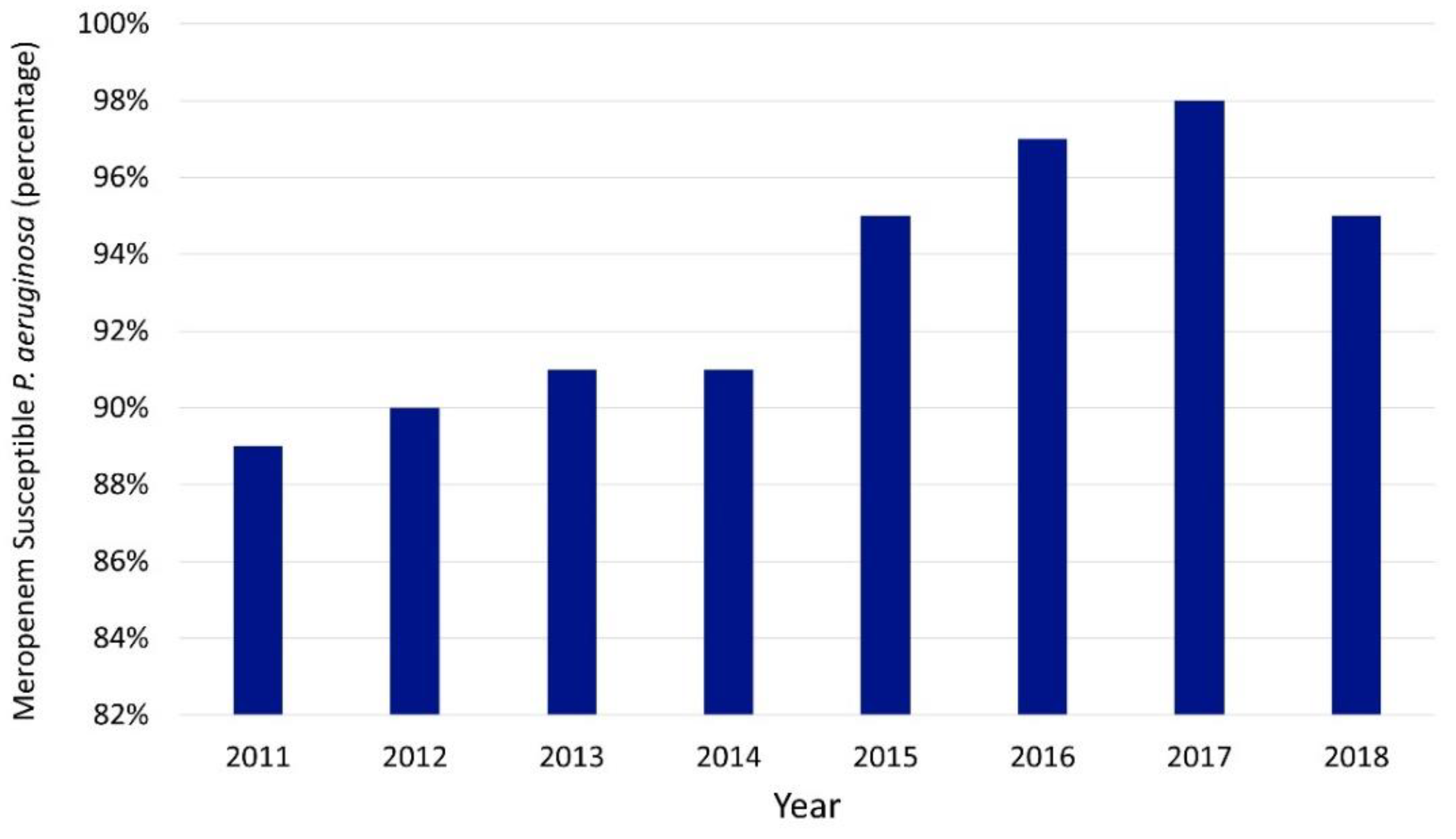
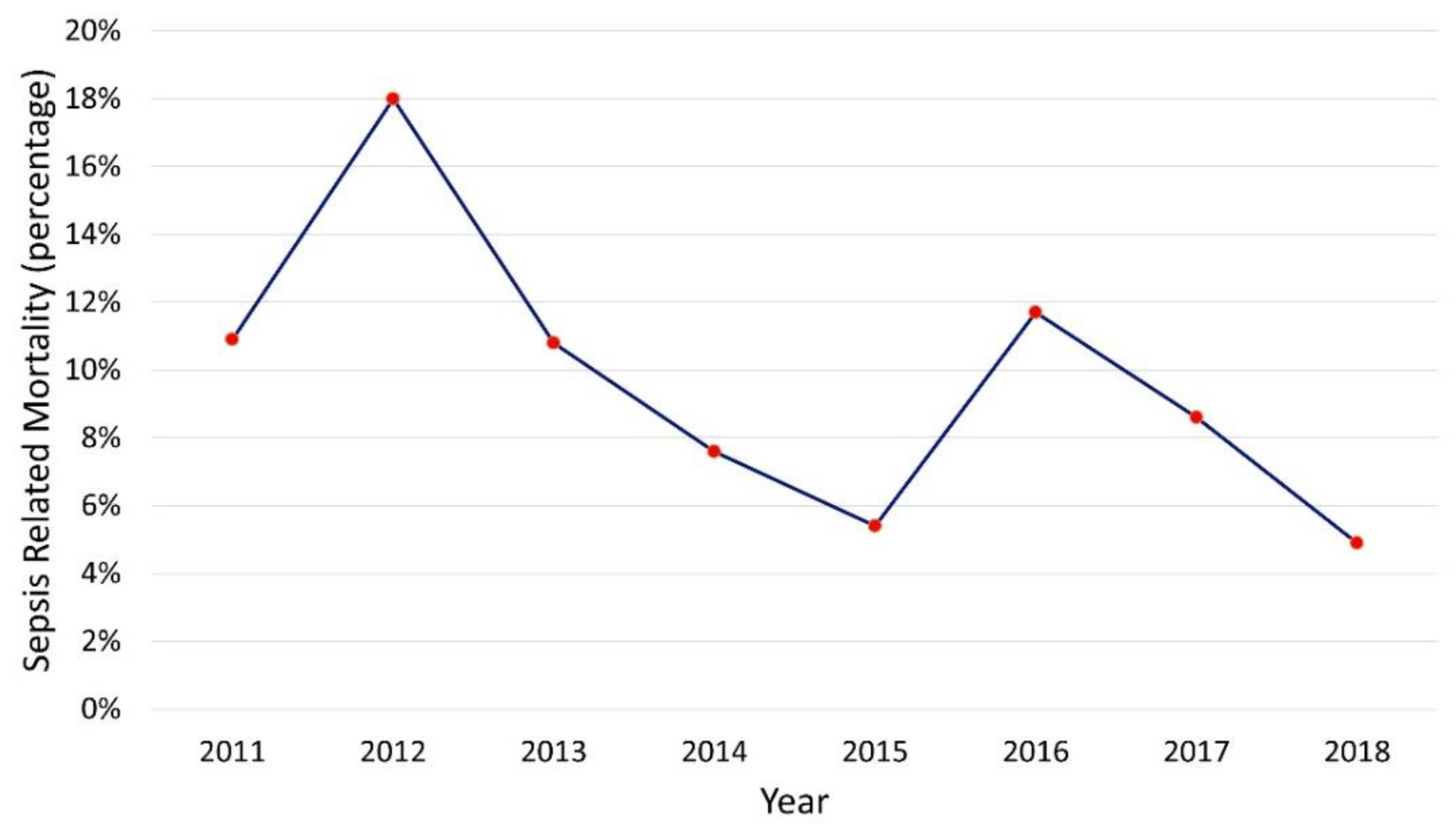
2.2. Outcome-Related Measures
3. Materials and Methods
3.1. Description of ASP
3.2. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gerber, J.S.; Kronman, M.P.; Ross, R.K.; Hersh, A.L.; Newland, J.G.; Metjian, T.A.; Zaoutis, T.E. Identifying targets for antimicrobial stewardship in children’s hospitals. Infect. Control. Hosp. Epidemiol. 2013, 34, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Stultz, J.S.; Nahata, M.C. Preventability of Voluntarily Reported or Trigger Tool-Identified Medication Errors in a Pediatric Institution by Information Technology: A Retrospective Cohort Study. Drug Saf. 2015, 38, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Bronzwaer, S.L.; Cars, O.; Buchholz, U.; Molstad, S.; Goettsch, W.; Veldhuijzen, I.K.; Kool, J.L.; Sprenger, M.J.; Degener, J.E.; European Antimicrobial Resistance Surveillance System. A European study on the relationship between antimicrobial use and antimicrobial resistance. Emerg. Infect. Dis. 2002, 8, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Chiotos, K.; Tamma, P.D.; Flett, K.B.; Karandikar, M.V.; Nemati, K.; Bilker, W.B.; Zaoutis, T.; Han, J.H. Increased 30-Day Mortality Associated with Carbapenem-Resistant Enterobacteriaceae in Children. Open Forum Infect. Dis. 2018, 5, ofy222. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Political Declaration of the High-Level Meeting of the General Assembly on Antimicrobial Resistance. 2016. Available online: https://digitallibrary.un.org/record/842813?ln=en (accessed on 1 October 2021).
- CDC. Antibiotic Resistance Threats in the United States, 2019; U.S. Department of Health and Human Services, CDC: Atlanta, GA, USA, 2019. Available online: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf (accessed on 1 October 2021).
- World Health Organization. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 1 October 2021).
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Gerber, J.S.; Jackson, M.A.; Tamma, P.D.; Zaoutis, T.E. AAP Committee on Infectious Diseases and Pediatric Infectious Diseases Society Diseases. Policy Statement: Antibiotic Stewardship in Pediatrics. J. Pediatr. Infect. Dis. Soc. 2021, 10, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Stultz, J.S.; Arnold, S.R.; Shelton, C.M.; Bagga, B.; Lee, K.R. Antimicrobial stewardship impact on Pseudomonas aeruginosa susceptibility to meropenem at a tertiary pediatric institution. Am. J. Infect. Control 2019, 47, 1513–1515. [Google Scholar] [CrossRef] [PubMed]
- Stultz, J.S.; Bice, T.; Johnstone, K.; Stuart, C.M.; Shelton, C.M.; Arnold, S.R.; Bagga, B.; Lee, K.R. Importance of Reviewing Antibiotic Courses by 48 Hours: Risk Factors for Third-Generation Cephalosporin Resistance among AmpC Harboring Organisms in Urine and Respiratory Cultures. Pediatr. Infect. Dis. J. 2021, 40, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.R.; Bagga, B.; Arnold, S.R. Reduction of Broad-Spectrum Antimicrobial Use in a Tertiary Children’s Hospital Post Antimicrobial Stewardship Program Guideline Implementation. Pediatr. Crit. Care Med. 2016, 17, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Bagga, B.; Buckingham, S.; Arnold, S.; Nesbitt, A.; Guimera, D.; Lee, K. Increasing Linezolid-resistant Enterococcus in a Children’s Hospital. Pediatr. Infect. Dis. J. 2018, 37, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Stultz, J.S.; Francis, N.; Ketron, S.; Bagga, B.; Shelton, C.M.; Lee, K.R.; Arnold, S.R. Analysis of Community-Acquired Urinary Tract Infection Treatment in Pediatric Patients Requiring Hospitalization: Opportunity for Use of Narrower Spectrum Antibiotics. J. Pharm. Technol. 2021, 37, 79–88. [Google Scholar] [CrossRef]
- Araujo da Silva, A.R.; Albernaz de Almeida Dias, D.C.; Marques, A.F.; Biscaia di Biase, C.; Murni, I.K.; Dramowski, A.; Sharland, M.; Huebner, J.; Zingg, W. Role of antimicrobial stewardship programmes in children: A systematic review. J. Hosp. Infect. 2018, 99, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Dona, D.; Barbieri, E.; Daverio, M.; Lundin, R.; Giaquinto, C.; Zaoutis, T.; Sharland, M. Implementation and impact of pediatric antimicrobial stewardship programs: A systematic scoping review. Antimicrob. Resist. Infect. Control 2020, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Horikoshi, Y.; Suwa, J.; Higuchi, H.; Kaneko, T.; Furuichi, M.; Aizawa, Y.; Fukuoka, K.; Okazaki, K.; Ito, K.; Shoji, T. Sustained pediatric antimicrobial stewardship program with consultation to infectious diseases reduced carbapenem resistance and infection-related mortality. Int. J. Infect. Dis. 2017, 64, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceradini, J.; Tozzi, A.E.; D’Argenio, P.; Bernaschi, P.; Manuri, L.; Brusco, C.; Raponi, M. Telemedicine as an effective intervention to improve antibiotic appropriateness prescription and to reduce costs in pediatrics. Ital. J. Pediatr. 2017, 43, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murki, S.; Jonnala, S.; Mohammed, F.; Reddy, A. Restriction of cephalosporins and control of extended spectrum beta-lactamase producing gram negative bacteria in a neonatal intensive care unit. Indian Pediatr. 2010, 47, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Yang, Y.; Wei, J.; Fan, S.; Yu, S.; Yao, K.; Wang, A.; Shen, X. Influencing the use of antibiotics in a Chinese pediatric intensive care unit. Pharm. World Sci. 2008, 30, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Gagliotti, C.; Buttazzi, R.; Di Mario, S.; Morsillo, F.; Moro, M.L. A regionwide intervention to promote appropriate antibiotic use in children reversed trends in erythromycin resistance to Streptococcus pyogenes. Acta Paediatr. 2015, 104, e422–e424. [Google Scholar] [CrossRef] [PubMed]
- Jindrak, V.; Marek, J.; Vanis, V.; Urbaskova, P.; Vlcek, J.; Janiga, L.; Maresova, V. Improvements in antibiotic prescribing by community paediatricians in the Czech Republic. Eurosurveillance 2008, 13, 19040. [Google Scholar] [CrossRef] [PubMed]
- The Center for Disease, Dynamics Economics & Policy. Resistance Map: Antibiotic Resistance of Pseudomonas aeruginosa in United States. 1999–2016. Available online: https://resistancemap.cddep.org/AntibioticResistance.php (accessed on 22 October 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Initiative | Date |
|---|---|
| Start of stewardship program | June 2011 |
| Critical care units’ empiric antibiotic use guidelines full implementation | August 2012 |
| Community-acquired pneumonia guideline implementation | December 2012 |
| Daily PAF on broad-spectrum antibiotics initiated | February 2013 |
| Daily PAF on positive sterile-site cultures initiated | March 2014 |
| Cystic fibrosis guideline implementation | September 2014 |
| Linezolid use guideline implementation | February 2015 |
| Linezolid added to daily PAF | April 2015 |
| Third-generation IV cephalosporins and vancomycin added to daily PAF | May 2015 |
| Practice change promoting narrower-spectrum antibiotics for perforated appendicitis | January 2016 |
| Practice change promoting narrower-spectrum antibiotic use for UTI | August 2017 |
| Revised/updated CVICU empiric antibiotic use guidelines | November 2017 |
| Revised/updated PICU empiric antibiotic use guidelines | March 2018 |
| Provider-driven 48 h antibiotic time-out implemented | April 2018 |
| Revised/updated NICU empiric antibiotic use guidelines | June 2018 |
| Fluoroquinolones added to daily PAF | October 2018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagga, B.; Stultz, J.S.; Arnold, S.; Lee, K.R. A Culture Change: Impact of a Pediatric Antimicrobial Stewardship Program Based on Guideline Implementation and Prospective Audit with Feedback. Antibiotics 2021, 10, 1307. https://doi.org/10.3390/antibiotics10111307
Bagga B, Stultz JS, Arnold S, Lee KR. A Culture Change: Impact of a Pediatric Antimicrobial Stewardship Program Based on Guideline Implementation and Prospective Audit with Feedback. Antibiotics. 2021; 10(11):1307. https://doi.org/10.3390/antibiotics10111307
Chicago/Turabian StyleBagga, Bindiya, Jeremy S. Stultz, Sandra Arnold, and Kelley R. Lee. 2021. "A Culture Change: Impact of a Pediatric Antimicrobial Stewardship Program Based on Guideline Implementation and Prospective Audit with Feedback" Antibiotics 10, no. 11: 1307. https://doi.org/10.3390/antibiotics10111307
APA StyleBagga, B., Stultz, J. S., Arnold, S., & Lee, K. R. (2021). A Culture Change: Impact of a Pediatric Antimicrobial Stewardship Program Based on Guideline Implementation and Prospective Audit with Feedback. Antibiotics, 10(11), 1307. https://doi.org/10.3390/antibiotics10111307