Antimicrobial Effects of Essential Oils on Oral Microbiota Biofilms: The Toothbrush In Vitro Model



Abstract
1. Introduction
2. Materials and Methods
2.1. Essential Oils
2.2. Bacterial Strains
2.3. Evaluation of Biofilm Production by Pure and Mixed Cultures
2.4. Evaluation of Essential Oil Antimicrobial Activity
2.5. Toothbrush In Vitro Model
2.6. Data Analysis
3. Results
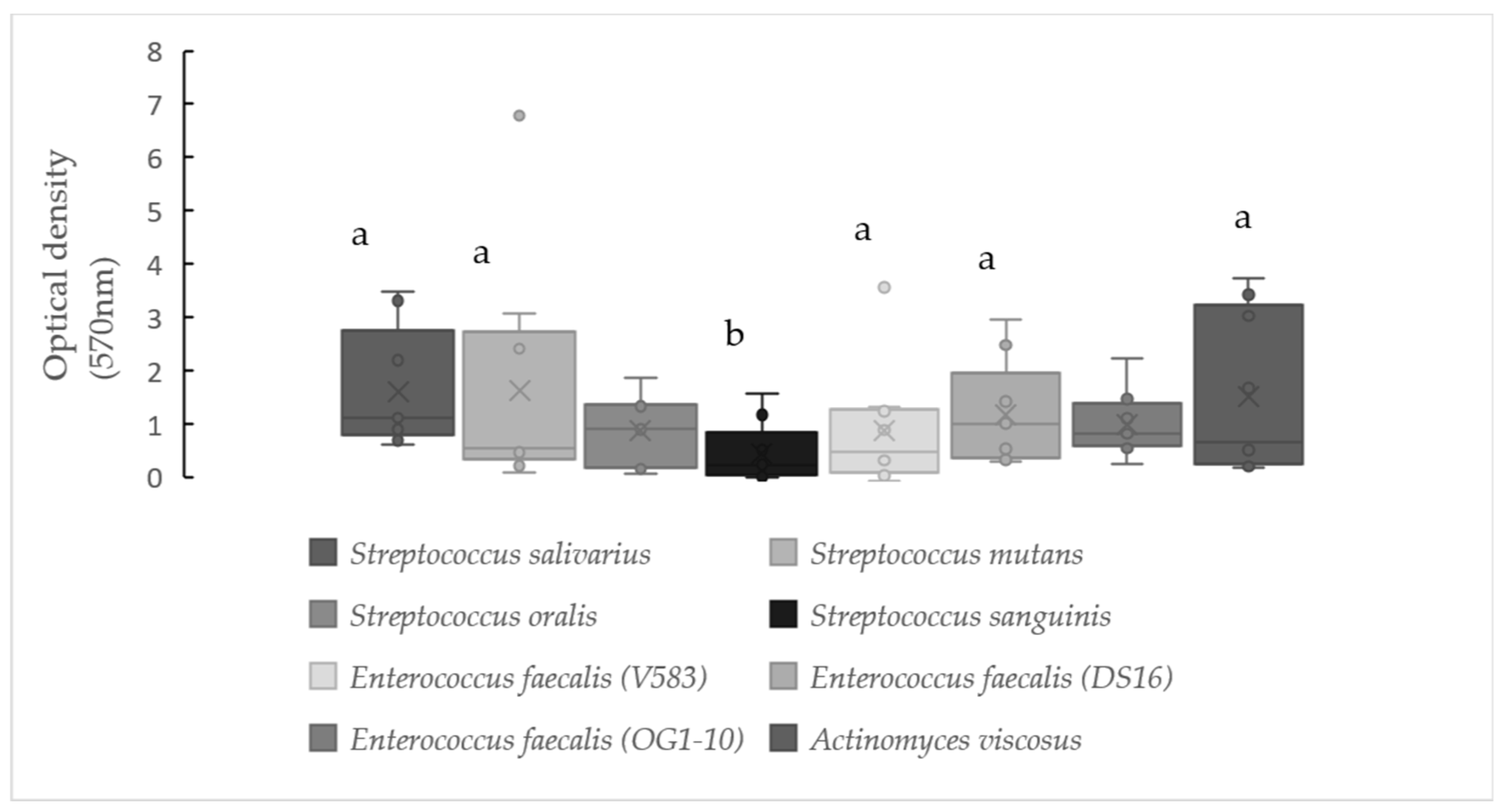
3.1. Evaluation of Biofilm Production by Pure and Mixed Cultures
3.2. Evaluation of Essential Oils Antimicrobial Activity
3.3. Toothbrush In Vitro Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roberts, A.P.; Mullany, P. Oral biofilms: A reservoir of transferable, bacterial, antimicrobial resistance. Expert Rev. Anti. Infect. Ther. 2010, 8, 1441–1450. [Google Scholar] [CrossRef]
- Faran Ali, S.M.; Tanwir, F. Oral microbial habitat a dynamic entity. J. Oral Biol. Craniofacial Res. 2012, 2, 181–187. [Google Scholar] [CrossRef]
- Zaura, E.; Nicu, E.A.; Krom, B.P.; Keijser, B.J.F. Acquiring and maintaining a normal oral microbiome: Current perspective. Front. Cell. Infect. Microbiol. 2014, 4, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Avila, M.; Ojcius, D.M.; Yilmaz, Ö. The oral microbiota: Living with a permanent guest. DNA Cell Biol. 2009, 28, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Jia, G.; Zhi, A.; Lai, P.F.H.; Wang, G.; Xia, Y.; Xiong, Z.; Zhang, H.; Che, N.; Ai, L. The oral microbiota—A mechanistic role for systemic diseases. Br. Dent. J. 2018, 224, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Chmit, M.; Kanaan, H.; Habib, J.; Abbass, M.; Mcheik, A.; Chokr, A. Antibacterial and antibiofilm activities of polysaccharides, essential oil, and fatty oil extracted from Laurus nobilis growing in Lebanon. Asian Pac. J. Trop. Med. 2014, 7, S546–S552. [Google Scholar] [CrossRef]
- Veras, H.N.H.; Rodrigues, F.F.G.; Botelho, M.A.; Menezes, I.R.A.; Coutinho, H.D.M.; Da Costa, J.G.M. Antimicrobial effect of lippia sidoides and thymol on Enterococcus faecalis biofilm of the bacterium isolated from root canals. Sci. World J. 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Jhajharia, K.; Mehta, L.; Parolia, A.; Shetty, K. Biofilm in endodontics: A review. J. Int. Soc. Prev. Community Dent. 2015, 5, 1–12. [Google Scholar] [CrossRef]
- Svanberg, M. Contamination of toothpaste and toothbrush by Streptococcus mutans. Eur. J. Oral Sci. 1978, 86, 412–414. [Google Scholar] [CrossRef]
- Branda, S.S.; Vik, Å.; Friedman, L.; Kolter, R. Biofilms: The matrix revisited. Trends Microbiol. 2005, 13, 20–26. [Google Scholar] [CrossRef]
- Meneses ML, L.M. Bacterial Biofilms. Analecta Vet. 2014, 32, 44–49. [Google Scholar]
- Simões, M.; Simões, L.C.; Vieira, M.J. A review of current and emergent biofilm control strategies. LWT-Food Sci. Technol. 2010, 43, 573–583. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; Mori, G.; Dibello, V.; Marrelli, M.; Mirgaldi, R.; De Vito, D.; Tatullo, M. Anti-plaque and antimicrobial efficiency of different oral rinses in a 3-day plaque accumulation model. J. Biol. Regul. Homeost. Agents 2016, 30, 1173–1178. [Google Scholar] [PubMed]
- Krishnan, K.; Chen, T.; Paster, B.J. A practical guide to the oral microbiome and its relation to health and disease. Oral Dis. 2017, 23, 276–286. [Google Scholar] [CrossRef]
- Da Silva, E.P.; De Martinis, E.C.P. Current knowledge and perspectives on biofilm formation: The case of Listeria monocytogenes. Appl. Microbiol. Biotechnol. 2013, 97, 957–968. [Google Scholar] [CrossRef]
- Giaouris, E.; Heir, E.; Hébraud, M.; Chorianopoulos, N.; Langsrud, S.; Møretrø, T.; Habimana, O.; Desvaux, M.; Renier, S.; Nychas, G.J. Attachment and biofilm formation by foodborne bacteria in meat processing environments: Causes, implications, role of bacterial interactions and control by alternative novel methods. Meat Sci. 2014, 97, 298–309. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Scacco, S.; Coletti, D.; Tatullo, M. Mesenchymal stem cells as promoters, enhancers, and playmakers of the translational regenerative medicine 2018. Stem Cells Int. 2018, 2018. [Google Scholar] [CrossRef]
- Marrelli, M.; Codispoti, B.; Shelton, R.M.; Scheven, B.A.; Cooper, P.R.; Tatullo, M.; Paduano, F. Dental pulp stem cell mechanoresponsiveness: Effects of mechanical stimuli on dental pulp stem cell behavior. Front. Physiol. 2018, 9, 1–9. [Google Scholar] [CrossRef]
- Huie, C.W. A review of modern sample-preparation techniques for the extraction and analysis of medicinal plants. Anal. Bioanal. Chem. 2002, 373, 23–30. [Google Scholar] [CrossRef]
- Wińska, K.; Mączka, W.; Łyczko, J.; Grabarczyk, M.; Czubaszek, A.; Szumny, A. Essential oils as antimicrobial agents—Myth or real alternative? Molecules 2019, 24, 2130. [Google Scholar] [CrossRef]
- Gracia-Valenzuela, M.H.; Orozco-Medina, C.; Molina-Maldonado, C. Efecto antibacteriano del aceite esencial de orégano (Lippia berlandieri) en bacterias patógenas de camarón Litopenaeus vannamei. Hidrobiologica 2012, 22, 201–206. [Google Scholar]
- Sakkas, H.; Papadopoulou, C. Antimicrobial activity of basil, oregano, and thyme essential oils. J. Microbiol. Biotechnol. 2017, 27, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Llana-Ruiz-Cabello, M.; Gutiérrez-Praena, D.; Pichardo, S.; Moreno, F.J.; Bermúdez, J.M.; Aucejo, S.; Cameán, A.M. Cytotoxicity and morphological effects induced by carvacrol and thymol on the human cell line Caco-2. Food Chem. Toxicol. 2014, 64, 281–290. [Google Scholar] [CrossRef] [PubMed]
- De La Chapa, J.J.; Singha, P.K.; Lee, D.R.; Gonzales, C.B. Thymol Inhibits Oral Squamous Cell Carcinoma Growth via Mitochondria-Mediated Apoptosis. J. Oral Pathol. Med. 2018, 176, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Heir, E.; Sundheim, G.; Holck, A.L. The Staphylococcus qacH gene product: A new member of the SMR family encoding multidrug resistance. FEMS Microbiol. Lett. 1998, 163, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Aue, D.L.; Buchalla, W.; Hiller, K.A.; Maisch, T.; Hellwig, E.; Al-Ahmad, A.; Cieplik, F. Cetylpyridinium chloride: Mechanism of action, antimicrobial efficacy in biofilms, and potential risks of resistance. Antimicrob. Agents Chemother. 2020, 64. [Google Scholar] [CrossRef] [PubMed]
- Cieplik, F.; Jakubovics, N.S.; Buchalla, W.; Maisch, T.; Hellwig, E.; Al-Ahmad, A. Resistance toward chlorhexidine in oral bacteria-is there cause for concern? Front. Microbiol. 2019, 10. [Google Scholar] [CrossRef]
- Sreenivasan, P.; Gaffar, A. Antiplaque biocides and bacterial resistance: A review. J. Clin. Periodontol. 2002, 29, 965–974. [Google Scholar] [CrossRef]
- CLSI. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically: Approved Standard, 9th ed.; Cockerill, F.R., Wiker, M.A., Alder, J., Dudley, M.N., Eliopoulos, G.M., Ferraro, M.J., Hardy, D.J., Hecht, D.W., Hindl, J.A., Eds.; CLSI: Annapolis Junction, MD, USA, 2012; Volume 32. [Google Scholar]
- Ceri, H.; Olson, M.E.; Stremick, C.; Read, R.R.; Morck, D.; Buret, A. The Calgary Biofilm Device: New technology for rapid determination of antibiotic susceptibilities of bacterial biofilms. J. Clin. Microbiol. 1999, 37, 1771–1776. [Google Scholar] [CrossRef]
- Peralta, S.; de Leles, S.; Dutra, A.; Cocco, A.; Radaelli, M.T.B.; Lund, R. Comparison of growth of viable oral bacteria and Streptococcus mutans in biofilm models using three different culture media. Afr. J. Microbiol. Res. 2015, 9, 388–393. [Google Scholar] [CrossRef][Green Version]
- Toole, G.O.; Kaplan, H.B.; Kolter, R. Biofilm formation as microbial development. Annu. Rev. Microbiol. 2000, 49–79. [Google Scholar] [CrossRef] [PubMed]
- Balouiri, M.; Sadiki, M.; Ibnsouda, S.K. Methods for in vitro evaluating antimicrobial activity: A review. J. Pharm. Anal. 2016, 6, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Mann, C.M.; Markham, J.L. A new method for determining the minimum inhibitory concentration of essential oils. J. Appl. Microbiol. 1998, 84, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Rhee, K.Y.; Gardiner, D.F. Clinical Relevance of Bacteriostatic versus Bactericidal Activity in the Treatment of Gram-Positive Bacterial Infections. Clin. Infect. Dis. 2004, 39, 755–756. [Google Scholar] [CrossRef]
- O’Toole, G.A. Microtiter dish Biofilm formation assay. J. Vis. Exp. 2010, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Quendera, A.P.; Barreto, A.S.; Semedo-Lemsaddek, T. Antimicrobial activity of essential oils against foodborne multidrug-resistant enterococci and aeromonads in planktonic and biofilm state. Food Sci. Technol. Int. 2019, 25, 101–108. [Google Scholar] [CrossRef]
- Patil, S.; Rao, R.S.; Sanketh, D.S.; Amrutha, N. Microbial flora in oral diseases. J. Contemp. Dent. Pract. 2013, 14, 1202–1208. [Google Scholar] [CrossRef]
- Cisar, J.O.; Kolenbrander, P.E.; McIntire, F.C. Specificity of coaggregation reactions between human oral streptococci and strains of Actinomyces viscosus or Actinomyces naeslundii. Infect. Immun. 1979, 24, 742–752. [Google Scholar] [CrossRef]
- Wilson, C.E.; Cathro, P.C.; Rogers, A.H.; Briggs, N.; Zilm, P.S. Clonal diversity in biofilm formation by Enterococcus faecalis in response to environmental stress associated with endodontic irrigants and medicaments. Int. Endod. J. 2015, 48, 210–219. [Google Scholar] [CrossRef]
- Mothey, D.; Buttaro, B.A.; Piggot, P.J. Mucin can enhance growth, biofilm formation and survival of Streptococcus mutans. FEMS Microbiol. Lett. 2014, 27, 1–19. [Google Scholar] [CrossRef]
- Cvitkovitch, D.G.; Li, Y.H.; Ellen, R.P. Quorum sensing and biofilm formation in Streptococcal infections. J. Clin. Investig. 2003, 112, 1626–1632. [Google Scholar] [CrossRef] [PubMed]
- Valm, A.M. The Structure of Dental Plaque Microbial Communities in the Transition from Health to Dental Caries and Periodontal Disease. J. Mol. Biol. 2019, 431, 2957–2969. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef]
- Jakubovics, N.S. Intermicrobial Interactions as a Driver for Community Composition and Stratification of Oral Biofilms. J. Mol. Biol. 2015, 427, 3662–3675. [Google Scholar] [CrossRef] [PubMed]
- Palmer, R.J.; Gordon, S.M.; Cisar, J.O.; Kolenbrander, P.E. Coaggregation-mediated interactions of streptococci and actinomyces detected in initial human dental plaque. J. Bacteriol. 2003, 185, 3400–3409. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, F.; Shakir, M. The Influence of Enterococcus faecalis as a Dental Root Canal Pathogen on Endodontic Treatment: A Systematic Review. Cureus 2020, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ardizzoni, A.; Pericolini, E.; Paulone, S.; Orsi, C.F.; Castagnoli, A.; Oliva, I.; Strozzi, E.; Blasi, E. In vitro effects of commercial mouthwashes on several virulence traits of Candida albicans, viridans streptococci and Enterococcus faecalis colonizing the oral cavity. PLoS ONE 2018, 13, e0207262. [Google Scholar] [CrossRef]
- Azizi, A. Genetic, Chemical and Agro-Morphological Evaluation of the Medicinal Plant Origanum Vulgare L. for Marker Assisted Improvement of Pharmaceutical Quality; Justus Liebig University Giessen: Giessen, Germany, 2010. [Google Scholar]
- Sahin, F.; Güllüce, M.; Daferera, D.; Sökmen, A.; Sökmen, M.; Polissiou, M.; Agar, G.; Özer, H. Biological activities of the essential oils and methanol extract of Origanum vulgare ssp. vulgare in the Eastern Anatolia region of Turkey. Food Control 2004, 15, 549–557. [Google Scholar] [CrossRef]
- Jiang, C.; Sun, Y.; Zhu, X.; Gao, Y.; Wang, L.; Wang, J.; Wu, L.; Song, D. Solvent-free microwave extraction coupled with headspace single-drop microextraction of essential oils from flower of Eugenia caryophyllata Thunb. J. Sep. Sci. 2010, 33, 2784–2790. [Google Scholar] [CrossRef]
- Orhan, D.; Hartevioglu, A. Chemical Composition and Biological Activities of Oregano Essential Oil and Its Fractions Obtained by Vacuum Distillation. Spat. DD-Peer Rev. J. Complement. Med. Drug Discov. 2013, 3, 23. [Google Scholar] [CrossRef]
- Ahmad, A.; Van Vuuren, S.; Viljoen, A. Unravelling the complex antimicrobial interactions of essential oils—The case of Thymus vulgaris (Thyme). Molecules 2014, 19, 2896–2910. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, J.D.F.; Paroul, N.; Czyewski, E.; Lerin, L.; Rotava, I.; Cansian, R.L.; Mossi, A.; Toniazzo, G.; de Oliveira, D.; Treichel, H. Perfil da composição química e atividades antibacteriana e antioxidante do óleo essencial do cravo-da-índia (Eugenia caryophyllata Thunb.). Rev. Ceres 2010, 57, 589–594. [Google Scholar] [CrossRef]
- Aznita, W.; Zainal-Abidin, Z.; Aznan, E.; Razi, M.N. The effectiveness of chlorhexidine, hexetidine and Eugenia caryophyllus extracts in commercialized oral rinses to reduce dental plaque microbes. Res. J. Biol. Sci. 2009, 4, 716–719. [Google Scholar]
- Kraivaphan, P.; Amornchat, C. Effect of an essential oil-containing dentifrice on established plaque and gingivitis. Southeast Asian J. Trop. Med. Public Health 2012, 43, 243–248. [Google Scholar] [PubMed]
- Timimi, E.A.; Casey, M. Effect of Thymus vulgaris extract on streptococci and mutans streptococci, in comparison to chlorhexidine gluconate (in vivo study). J. Bagh. Coll. Dent. 2012, 24, 116–121. [Google Scholar]
- Ciandrini, E.; Campana, R.; Federici, S.; Manti, A.; Battistelli, M.; Falcieri, E.; Papa, S.; Baffone, W. In vitro activity of Carvacrol against titanium-adherent oral biofilms and planktonic cultures. Clin. Oral Investig. 2014, 18, 2001–2013. [Google Scholar] [CrossRef]
- Burt, S. Essential oils: Their antibacterial properties and potential applications in foods—A review. Int. J. Food Microbiol. 2004, 94, 223–253. [Google Scholar] [CrossRef]
- Sim, J.X.F.; Khazandi, M.; Chan, W.Y.; Trott, D.J.; Deo, P. Antimicrobial activity of thyme oil, oregano oil, thymol and carvacrol against sensitive and resistant microbial isolates from dogs with otitis externa. Vet. Dermatol. 2019, 30, 524-e159. [Google Scholar] [CrossRef]
- Man, A.; Santacroce, L.; Jacob, R.; Mare, A.; Man, L. Antimicrobial activity of six essential oils against a group of human pathogens: A comparative study. Pathogens 2019, 8, 15. [Google Scholar] [CrossRef]
- Cieplik, F.; Kara, E.; Muehler, D.; Enax, J.; Hiller, K.A.; Maisch, T.; Buchalla, W. Antimicrobial efficacy of alternative compounds for use in oral care toward biofilms from caries-associated bacteria in vitro. Microbiologyopen 2019, 8, 1–10. [Google Scholar] [CrossRef]
- Marrelli, M.; Maletta, C.; Inchingolo, F.; Alfano, M.; Tatullo, M. Three-point bending tests of zirconia core/veneer ceramics for dental restorations. Int. J. Dent. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Marrelli, M.; Pujia, A.; Palmieri, F.; Gatto, R.; Falisi, G.; Gargari, M.; Caruso, S.; Apicella, D.; Rastelli, C.; Nardi, G.M.; et al. Innovative approach for the in vitro research on biomedical scaffolds designed and customized with CAD-CAM technology. Int. J. Immunopathol. Pharmacol. 2016, 29, 778–783. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Mixed Cultures | Essential Oils | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thyme | Oregano | Clove | |||||||||||
| Statistics | MIC (a) | MBC (a) | MBIC (a) | MBEC (a) | MIC (a) | MBC (a) | MBIC (b) | MBEC (a) | MIC (b) | MBC (b) | MBIC (c) | MBEC (b) | |
| A | Mean | 7.2 | 9.0 | 12.6 | 45.2 | 7.8 | 9.5 | 18.8 | 58.7 | 30.1 | 41.8 | 37.6 | 322.1 |
| Min | 3.6 | 3.6 | 1.8 | 0.9 | 3.5 | 3.5 | 3.5 | 14.0 | 15.0 | 15.0 | 15.0 | 3.8 | |
| Q1 | 3.6 | 6.3 | 4.5 | 0.9 | 5.2 | 7.0 | 8.7 | 21.0 | 15.0 | 30.1 | 26.3 | 3.8 | |
| Median | 7.2 | 7.2 | 7.2 | 5.2 | 7.0 | 7.0 | 21.0 | 55.9 | 30.1 | 30.1 | 30.1 | 481.3 | |
| Q3 | 10.8 | 14.4 | 28.8 | 87.1 | 10.5 | 14.0 | 28.0 | 83.8 | 37.6 | 60.2 | 30.1 | 481.3 | |
| Max | 14.4 | 14.4 | 28.8 | 222.8 | 14.0 | 14.0 | 28.0 | 111.7 | 60.2 | 60.2 | 30.1 | 481.3 | |
| B | Mean | 5.2 | 7.2 | 20.4 | 27.1 | 7.8 | 9.8 | 14.8 | 112.9 | 37.0 | 42.6 | 40.1 | 481.3 |
| Min | 0.4 | 7.2 | 7.2 | 0.9 | 3.5 | 7.0 | 7.0 | 1.7 | 3.8 | 15.0 | 15.0 | 481.3 | |
| Q1 | 3.6 | 7.2 | 7.2 | 0.9 | 5.2 | 7.0 | 7.0 | 2.6 | 6.6 | 26.3 | 15.0 | 481.3 | |
| Median | 7.2 | 7.2 | 28.8 | 14.0 | 7.0 | 7.0 | 14.0 | 111.7 | 45.1 | 45.1 | 45.1 | 481.3 | |
| Q3 | 7.2 | 7.2 | 28.8 | 27.9 | 10.5 | 14.0 | 24.4 | 167.6 | 60.2 | 60.2 | 60.2 | 481.3 | |
| Max | 7.2 | 7.2 | 28.8 | 111.4 | 14.0 | 14.0 | 28.0 | 446.9 | 60.2 | 60.2 | 60.2 | 481.3 | |
| C | Mean | 11.6 | 16.2 | 28.8 | 21.9 | 12.8 | 16.0 | 22.7 | 46.4 | 55.2 | 45.1 | 51.1 | 361.0 |
| Min | 3.6 | 3.6 | 28.8 | 0.9 | 3.5 | 7.0 | 7.0 | 0.9 | 15.0 | 30.1 | 15.0 | 240.7 | |
| Q1 | 3.6 | 6.3 | 28.8 | 3.5 | 7.0 | 7.0 | 12.2 | 1.7 | 60.2 | 30.1 | 60.2 | 300.8 | |
| Median | 7.2 | 14.4 | 28.8 | 14.0 | 7.0 | 14.0 | 28.0 | 15.7 | 60.2 | 45.1 | 60.2 | 361.0 | |
| Q3 | 21.6 | 28.8 | 28.8 | 55.7 | 21.0 | 28.0 | 28.0 | 111.7 | 60.2 | 60.2 | 60.2 | 241.4 | |
| Max | 28.8 | 28.8 | 28.8 | 55.7 | 28.0 | 28.0 | 28.0 | 111.7 | 60.2 | 60.2 | 60.2 | 481.3 | |
| D | Mean | 5.2 | 9.6 | 22.2 | 107.0 | 6.6 | 8.4 | 27.9 | 57.0 | 45.1 | 46.8 | 42.1 | 327.0 |
| Min | 3.6 | 3.6 | 3.6 | 1.8 | 3.5 | 3.5 | 27.9 | 7.2 | 15.0 | 30.1 | 15.0 | 218.0 | |
| Q1 | 3.6 | 3.6 | 11.7 | 28.8 | 3.5 | 3.5 | 27.9 | 7.2 | 30.1 | 30.1 | 15.0 | 272.5 | |
| Median | 3.6 | 10.8 | 28.8 | 115.0 | 7.0 | 7.0 | 27.9 | 14.5 | 60.2 | 60.2 | 60.2 | 327.0 | |
| Q3 | 7.2 | 14.4 | 28.8 | 230.0 | 7.0 | 14.0 | 27.9 | 101.4 | 60.2 | 60.2 | 60.2 | 381.5 | |
| Max | 7.2 | 14.4 | 28.8 | 230.0 | 14.0 | 14.0 | 27.9 | 231.7 | 60.2 | 60.2 | 60.2 | 436.1 | |
| Mixed Cultures | Essential Oils | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Thyme (a) | Oregano (a) | Clove (b) | ||||||||
| Statistics | MIC | MBC | MBIC | MIC | MBC | MBIC | MIC | MBC | MBIC | |
| A | Mean | 15.3 | - | 2.0 | 12.4 | - | 10.3 | - | 62.8 | 11.3 |
| Min | 13.9 | 2.0 | 7.1 | 2.0 | 62.8 | 7.1 | ||||
| Q1 | 15.7 | 2.0 | 7.5 | 3.4 | 62.8 | 7.1 | ||||
| Median | 15.7 | 2.0 | 15.7 | 11.8 | 62.8 | 7.2 | ||||
| Q3 | 15.7 | 2.0 | 15.7 | 15.7 | 62.8 | 13.7 | ||||
| Max | 15.7 | 2.0 | 15.7 | 15.7 | 62.8 | 31.4 | ||||
| B | Mean | 11.4 | - | 2.0 | 14.0 | - | 6.6 | - | 62.8 | 8.6 |
| Min | 7.0 | 2.0 | 7.1 | 2.0 | 62.8 | 7.1 | ||||
| Q1 | 9.2 | 2.0 | 11.4 | 2.0 | 62.8 | 7.1 | ||||
| Median | 11.4 | 2.0 | 15.7 | 2.0 | 62.8 | 7.4 | ||||
| Q3 | 13.5 | 2.0 | 15.7 | 15.7 | 62.8 | 7.9 | ||||
| Max | 15.7 | 2.0 | 15.7 | 15.7 | 62.8 | 15.7 | ||||
| C | Mean | 14.9 | 15.7 | 2.0 | 15.4 | 15.7 | 2.0 | - | 62.8 | 16.5 |
| Min | 14.0 | 15.7 | 2.0 | 14.2 | 15.7 | 2.0 | 62.8 | 7.1 | ||
| Q1 | 14.4 | 15.7 | 2.0 | 15.0 | 15.7 | 2.0 | 62.8 | 7.2 | ||
| Median | 14.9 | 15.7 | 2.0 | 15.7 | 15.7 | 2.0 | 62.8 | 11.0 | ||
| Q3 | 15.3 | 15.7 | 2.0 | 15.7 | 15.7 | 2.0 | 62.8 | 15.7 | ||
| Max | 15.7 | 15.7 | 2.0 | 15.7 | 15.7 | 2.0 | 62.8 | 56.9 | ||
| D | Mean | 10.9 | - | 2.0 | 15.4 | - | 6.6 | - | 31.4 | 18.7 |
| Min | 7.9 | 2.0 | 14.2 | 2.0 | 31.4 | 7.1 | ||||
| Q1 | 9.4 | 2.0 | 15.0 | 2.0 | 31.4 | 7.1 | ||||
| Median | 11.0 | 2.0 | 15.7 | 2.0 | 31.4 | 7.4 | ||||
| Q3 | 12.5 | 2.0 | 15.7 | 15.7 | 31.4 | 31.4 | ||||
| Max | 14.0 | 2.0 | 15.7 | 15.7 | 31,4 | 62.8 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aires, A.; Barreto, A.S.; Semedo-Lemsaddek, T. Antimicrobial Effects of Essential Oils on Oral Microbiota Biofilms: The Toothbrush In Vitro Model. Antibiotics 2021, 10, 21. https://doi.org/10.3390/antibiotics10010021
Aires A, Barreto AS, Semedo-Lemsaddek T. Antimicrobial Effects of Essential Oils on Oral Microbiota Biofilms: The Toothbrush In Vitro Model. Antibiotics. 2021; 10(1):21. https://doi.org/10.3390/antibiotics10010021
Chicago/Turabian StyleAires, Andreia, António Salvador Barreto, and Teresa Semedo-Lemsaddek. 2021. "Antimicrobial Effects of Essential Oils on Oral Microbiota Biofilms: The Toothbrush In Vitro Model" Antibiotics 10, no. 1: 21. https://doi.org/10.3390/antibiotics10010021
APA StyleAires, A., Barreto, A. S., & Semedo-Lemsaddek, T. (2021). Antimicrobial Effects of Essential Oils on Oral Microbiota Biofilms: The Toothbrush In Vitro Model. Antibiotics, 10(1), 21. https://doi.org/10.3390/antibiotics10010021