Innovative Methodologies for the Early Detection of Breast Cancer: A Review Categorized by Target Biological Samples

 ,
,  ,
,  and
and 
Abstract
1. Introduction
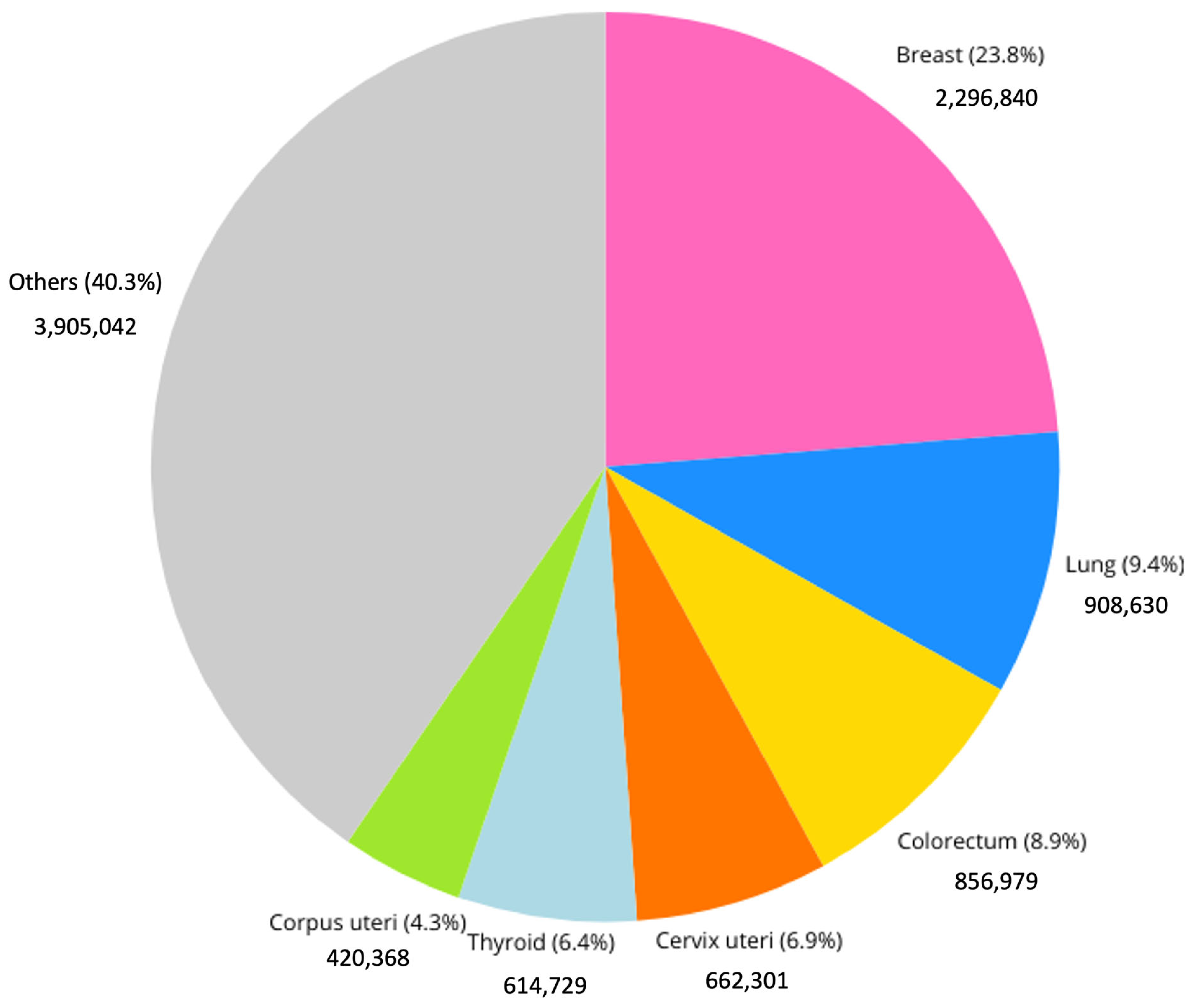
1.1. Epidiemology and Current Challenges
1.2. Conventional Methods for Breast Cancer Detection
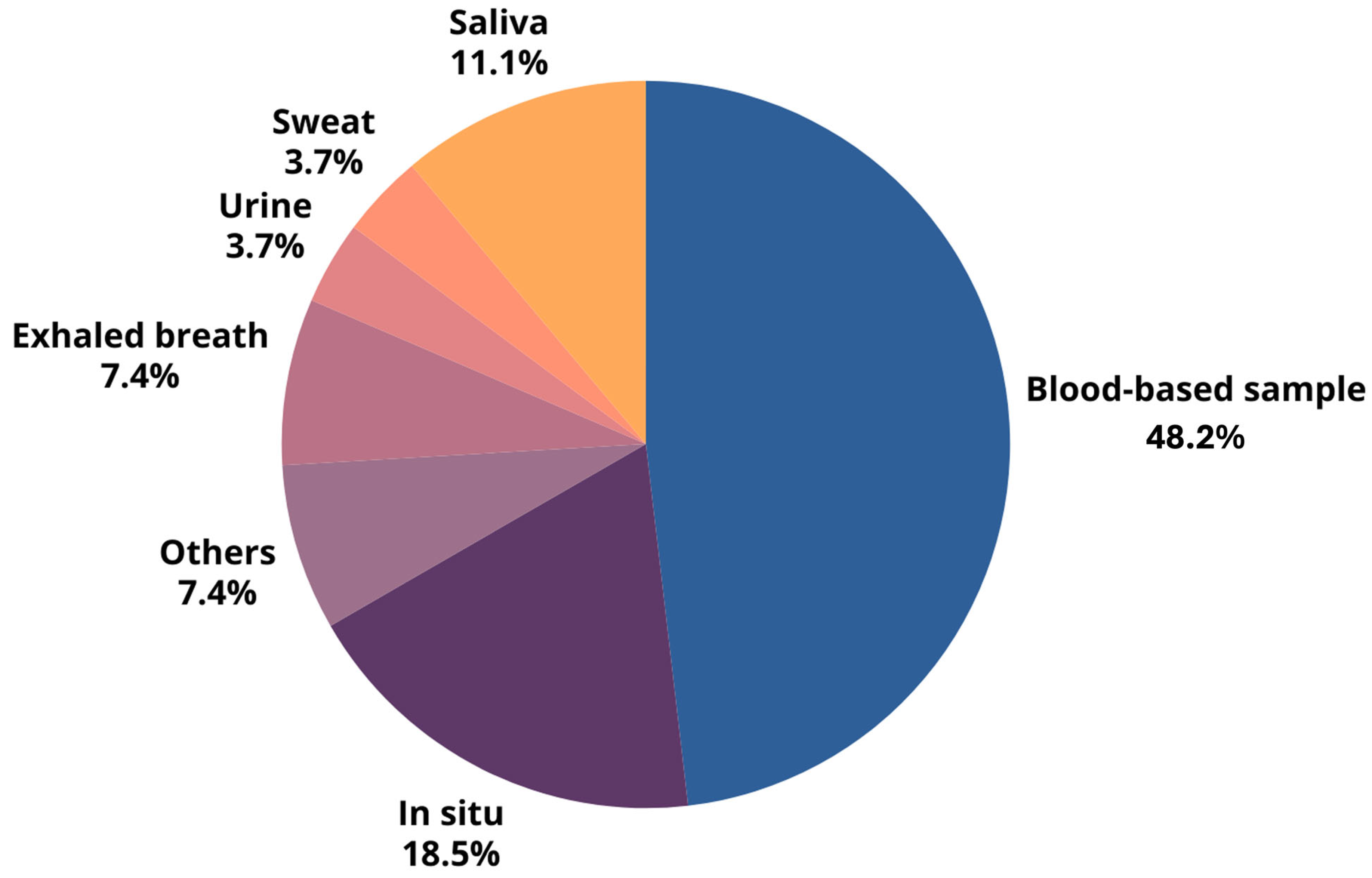
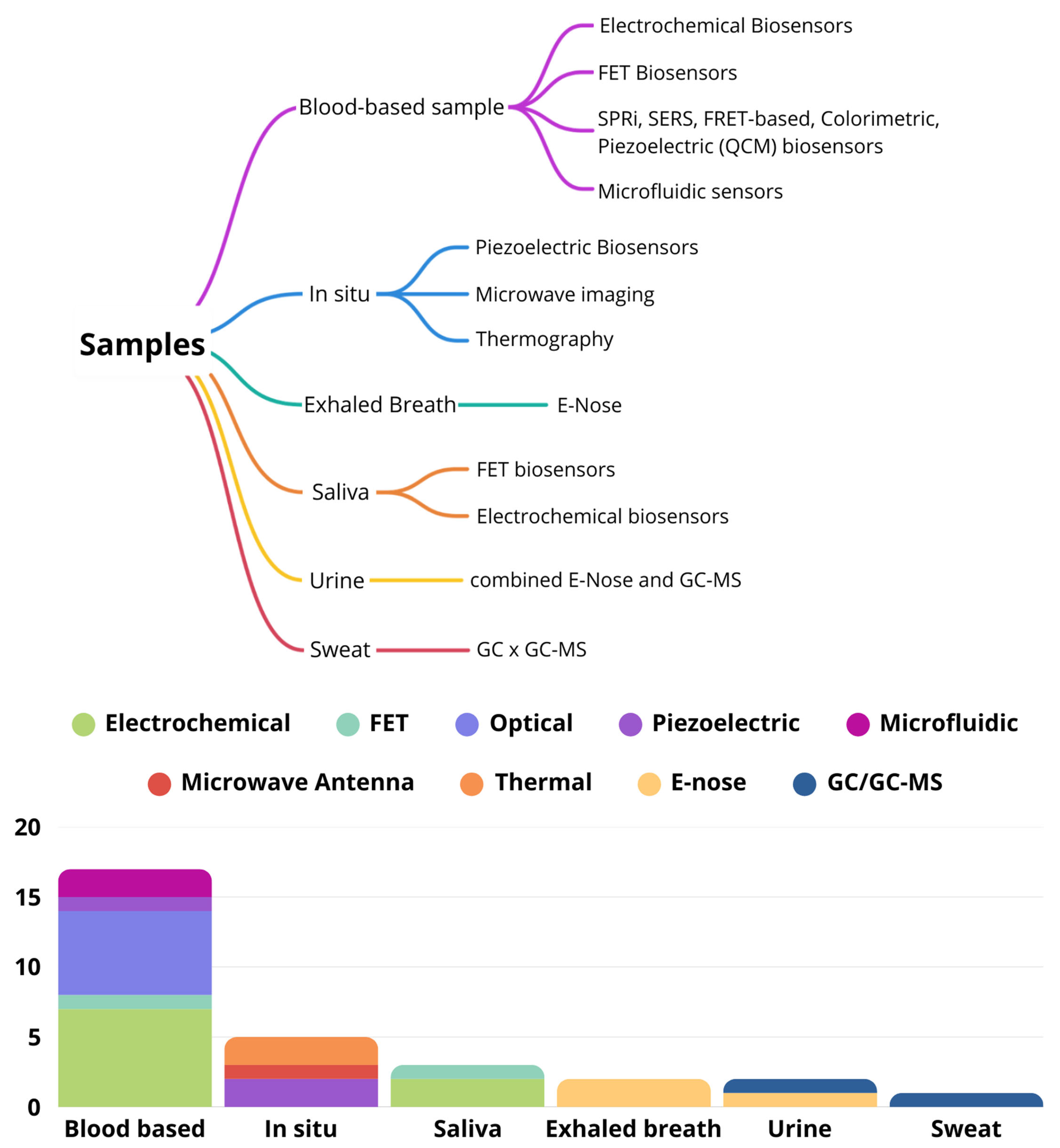
2. Emerging Diagnostic Methods
3. Analysis of Blood, Serum, and Plasma
3.1. Electrochemical Biosensors
3.2. Optical and Acoustic Biosensors
3.3. Microfluidic Devices
3.4. Pros and Cons of Blood, Serum, and Plasma Samples
- Pros: High Biomarker Abundance: Blood, serum, and plasma contain rich sources of biomarkers essential for diagnosing and monitoring disease progression [22,34]. Early Detection: These samples allow for the detection of biomarkers at early stages, crucial for timely intervention and improved survival rates [20]. Variety of Detection Methods: Techniques such as electrochemical biosensors, SPR sensors, and microfluidic devices can be employed, offering flexibility and sensitivity in biomarker detection [19,32]. Stability of Samples: Serum and plasma can be stored for extended periods, maintaining the stability of many biomarkers, which is advantageous for longitudinal studies [34].
- Cons: Invasiveness: The collection of these samples can be uncomfortable for patients [33]. Handling and Storage: Proper handling and storage are required to prevent the degradation of the samples, which can affect the accuracy of the test results [34]. Potential for False Positives: There is a risk of cross-reactivity with non-target molecules, which can lead to false-positive results and unnecessary follow-up procedures [31]. Complex Fabrication and Maintenance: Advanced sensor technologies often require intricate preparation and maintenance, which can be resource-intensive and challenging to implement consistently across different settings [19,38]. Variability in Biomarker Levels: Biomarker levels can vary significantly between individuals and due to external factors, complicating result interpretation [38]. Waste Management: The disposal of biological waste must adhere to strict regulations, adding to operational complexity and costs [38]. Cost and Resource-intensive Nature: The collection and preparation of samples require resources and personnel, increasing operational costs, especially in mass screening contexts [34].
4. Analysis In Situ
4.1. Piezoelectric Sensors and Continuous Ultrasound Breast Monitor (cUSBr)
4.2. Microvawe Imaging
4.3. Thermography
4.4. Pros and Cons of In Situ Sample Analyses
- Pros:
- Real-time Monitoring: Technologies such as thermography systems allow for continuous monitoring, which is useful for the early detection of breast cancer [46]. Potential for Clinical Use: These systems can be integrated into clinical settings, enhancing diagnostic capabilities and the timeliness of interventions [42]. Detection of Anomalies: Technologies like ultrasound can provide significant imaging, facilitating the identification of tissue abnormalities [36]. Non-invasive Approach: The proposed technologies are designed to be non-invasive, reducing patient discomfort and improving the acceptance of procedures [44].
- Cons:
- Stringent Measurement Conditions: Patients are required to comply with specific conditions, which may restrict the practical applicability of these technologies [42]. Mechanical Challenges: Geometric variability and the deformability of breast tissue can complicate the accuracy of analyses and measurements [44]. Technical Limitations: these two technologies have technical gaps, such as dependence on technician experience and issues with skin contact [44]. Sensor Limitations: The sensors used may have limited bandwidths, affecting the effectiveness of analyses and the capability for self-screening [45].
5. Exhaled Breath
5.1. Electronic Nose Technology
5.2. Pros and Cons of VOC Analysis in Breath Samples
- Pros:
- Cons:
- Environmental Sensitivity: Accuracy can be affected by environmental factors like temperature and humidity [46]. Standardization Challenges: Variability in breath composition due to personal factors complicates standardization [46]. Factors such as diet, medication, and smoking habits can influence VOC profiles, requiring robust normalization methods. Need for Validation: Further validation in larger, diverse populations is necessary to confirm the results [46,47].
6. Saliva
6.1. Field-Effect Transistor (FET) Biosensors
6.2. Pros and Cons of Saliva Analysis
- Pros:
- Non-Invasive: Saliva collection is simple, non-invasive, and painless, making it suitable for frequent monitoring and reducing patient discomfort [48]. Cost-Effective: The use of saliva-based tests can reduce the costs associated with more invasive procedures, making them more accessible for patients [49]. Potential for Multiple Biomarkers: Saliva can contain a variety of biomarkers, allowing for the simultaneous detection of multiple conditions [49,50]. Lower Interference: Saliva generally has lower levels of interfering substances compared to blood, which can simplify the analysis and improve the accuracy of the results.
- Cons:
- Lower Biomarker Concentration: Biomarker concentrations in saliva may be lower than those in blood, potentially requiring more sensitive detection methods to achieve reliable results [51]. Variability: Factors such as hydration, food intake, and oral health can influence saliva composition, leading to variability in the results and potentially affecting diagnostic accuracy [49]. Standardization: Standardized protocols for saliva collection and processing are essential to ensure reliable and reproducible results, which can be challenging to implement across different settings [50]. Limited Research for Some Biomarkers: While there is growing interest in saliva-based diagnostics, some biomarkers may not yet have established correlations with disease states, necessitating further research [48,49,50].
7. Urine
Pros and Cons of Urine Analysis
- Pros:
- Non-Invasive: Urine collection is simple, non-invasive, and painless, making it suitable for frequent monitoring. Ease of Collection: Urine samples can be collected easily without the need for specialized medical personnel or equipment. Cost-Effective: The use of urine-based tests can reduce the costs related to more invasive procedures.
- Cons:
- Lower Biomarker Concentration: Biomarker concentrations in urine may be lower than those in blood, potentially requiring more sensitive detection methods. Variability: Factors such as diet, hydration, and lifestyle can influence urine composition and affect the consistency of results. Standardization Challenges: Standardized protocols for urine collection and processing are essential to ensure reliable and reproducible results.
8. Sweat
Pros and Cons of Sweat Analysis
- Pros:
- Non-Invasive Collection: Sweat sampling is a non-invasive method, making it more patient-friendly compared to blood or tissue samples. Cost-Effective: If validated, sweat analysis could serve as a low-cost alternative to traditional screening methods, particularly beneficial in resource-limited settings.
- Cons:
- Limited Sample Size: The small number of participants in the study may limit the applicability of the findings to the broader population. Variability in VOC Composition: Factors such as diet, hydration, and individual metabolism can influence sweat composition, leading to variability in VOC profiles. Standardization Challenges: There is a need for standardized protocols for sweat collection and analysis to ensure consistent and reliable results across different studies and populations.
9. Conclusions
- -
- Traditional imaging—such as mammography, MRI, ultrasound, and PET—remains essential for breast cancer detection, offering validated accuracy, but requiring costly infrastructure and trained personnel [63]. These methods also come with drawbacks such as invasiveness, radiation, and long wait times;
- -
- In contrast, non-invasive approaches using biosensors and bodily fluids offer lower costs, faster results, and better accessibility, including potential home testing. Despite challenges like low biomarker levels and inconsistent results, these innovations show strong promise for early detection and continuous monitoring [64];
- -
- The shift toward non-invasive cancer detection is gaining momentum, with breath, saliva, urine, and sweat offering patient-friendly options for frequent monitoring. While blood tests remain the gold standard due to high biomarker levels, research is increasingly exploring multi-sample integration. Applying sensitive blood detection methods to non-invasive samples could boost accuracy, with fewer drawbacks;
- -
- Technologies like electronic noses and machine learning support early detection, though standardization and validation are still needed. AI integration is improving analysis and interpretation, moving diagnostics toward greater precision and personalization;
- -
- The integration of unobtrusive sensor technology for monitoring and frequent examination could favor early detection and early intervention in a collaborative synergy between robotics and sensors [65].
Author Contributions
Funding
Conflicts of Interest
References
- IARC. International Agency for Research on Cancer. 2024. Available online: https://www.iarc.who.int/ (accessed on 14 April 2025).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Kim, J.; Harper, A.; McCormack, V.; Sung, H.; Houssami, N.; Morgan, E.; Mutebi, M.; Garvey, G.; Soerjomataram, I.; Fidler-Benaoudia, M.M. Global patterns and trends in breast cancer incidence and mortality across 185 countries. Nat. Med. 2025, 31, 1154–1162. [Google Scholar] [CrossRef]
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Breast cancer statistics. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Breast Cancer Facts & Figures 2021–2022; American Cancer Society: Atlanta, GA, USA, 2022. [Google Scholar]
- Zheng, D.; He, X.; Jing, J. Overview of Artificial Intelligence in Breast Cancer Medical Imaging. J. Clin. Med. 2023, 12, 419. [Google Scholar] [CrossRef]
- Gegios, A.R.; Peterson, M.S.; Fowler, A.M. Breast Cancer Screening and Diagnosis: Recent Advances in Imaging and Current Limitations. Pet Clin. 2023, 18, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Monticciolo, D.L.; Newell, M.S.; Hendrick, R.E.; Helvie, M.A.; Moy, L.; Monsees, B.; Kopans, D.B.; Eby, P.R.; Sickles, E.A. Breast Cancer Screening for Average-Risk Women: Recommendations from the ACR Commission on Breast Imaging. J. Am. Coll. Radiol. 2017, 14, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Heller, S.L.; Moy, L. Breast MRI Screening: Benefits and Limitations. Curr. Breast Cancer Rep. 2016, 8, 248–257. [Google Scholar] [CrossRef]
- Emaus, M.; Bakker, M.; Peeters, H.; Loo, C.E.; Mann, R.M.; de Jong, M.D.F.; Bisschops, R.H.C.; Veltman, J.; Duvivier, K.M.; Lobbes, M.B.I.; et al. MR Imaging as an Additional Screening Modality for the Detection of Breast Cancer in Women Aged 50–75 Years with Extremely Dense Breasts: The DENSE Trial Study Design. Radiology 2015, 277, 527–537. [Google Scholar] [CrossRef]
- Berg, W.; Zhang, Z.; Lehrer, D.; Jong, R.A.; Pisano, E.D.; Barr, R.G.; Böhm-Vélez, M.; Mahoney, M.C.; Evans, W.P.; Larsen, L.H.; et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 2012, 307, 1394–1404. [Google Scholar]
- Kolb, T.M.; Lichy, J.; Newhouse, J.H. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: An analysis of 27,825 patient evaluations. Radiology 2002, 225, 165–175. [Google Scholar] [CrossRef]
- Mahoney, M.C.; Newell, M.S. Screening MR Imaging Versus Screening Ultrasound: Pros and Cons. Magn. Reson. Imaging Clin. N. Am. 2013, 21, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Alauddin, M.M. Positron emission tomography (PET) imaging with 18F-based radiotracers. Am. J. Nucl. Med. Mol. Imaging 2012, 2, 55–76. [Google Scholar] [PubMed]
- Heusner, T.A.; Kuemmel, S.; Umutlu, L.; Koeninger, A.; Freudenberg, L.S.; Hauth, E.A.; Kimmig, K.R.; Forsting, M.; Bockisch, A.; Antoch, G. Breast Cancer Staging in a Single Session: Whole-Body PET/CT Mammography. J. Nucl. Med. 2008, 49, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Crosby, D.; Bhatia, S.; Brindle, K.; Coussens, L.M.; Dive, C.; Emberton, M.; Esener, S.; Fitzgerald, R.C.; Gambhir, S.S.; Kuhn, P.; et al. Early detection of cancer. Science 2022, 375, 6586. [Google Scholar] [CrossRef]
- Ginsburg, O.; Yip, C.; Brooks, A.; Cabanes, A.; Caleffi, M.; Yataco, J.A.D.; Gyawali, B.; McCormack, V.; de Anderson, M.M.; Mehrotra, R.; et al. Breast cancer early detection: A phased approach to implementation. Cancer 2020, 126, 2379–2393. [Google Scholar] [CrossRef]
- Shahrokhian, S.; Salimian, R. Ultrasensitive Detection of Cancer Biomarkers Using Conducting Polymer/Electrochemically Reduced Graphene Oxide-Based Biosensor: Application toward BRCA1 Sensing. Sens. Actuators B Chem. 2018, 266, 160–169. [Google Scholar] [CrossRef]
- Mohammadpour-Haratbar, A.; Boraei, S.B.A.; Zare, Y.; Rhee, K.Y.; Park, S.-J. Graphene-based electrochemical biosensors for breast cancer detection. Biosensors 2023, 13, 80. [Google Scholar] [CrossRef]
- Hakimian, F.; Ghourchian, H. Ultrasensitive electrochemical biosensor for detection of microRNA-155 as a breast cancer risk factor. Anal. Chim. Acta 2020, 1136, 1–8. [Google Scholar] [CrossRef]
- Hu, R.; Wen, W.; Wang, Q.; Xiong, H.; Zhang, X.; Gu, H.; Wang, S. Novel electrochemical aptamer biosensor based on an enzyme–gold nanoparticle dual label for the ultrasensitive detection of epithelial tumor marker MUC1. Biosens. Bioelectron. 2014, 53, 384–389. [Google Scholar] [CrossRef]
- Zhao, S.; Yang, W.; Lai, R.Y. A folding-based electrochemical aptasensor for detection of vascular endothelial growth factor in human whole blood. Biosens. Bioelectron. 2011, 26, 2442–2447. [Google Scholar] [CrossRef]
- Marques, R.C.B.; Viswanathan, S.; Nouws, H.P.A.; Delerue-Matos, C.; Gonzales-Garcia, M.B. Electrochemical immunosensor for the analysis of the breast cancer biomarker HER2 ECD. Talanta 2014, 129, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Chandra, P.; Shim, Y.B. Ultrasensitive and Selective Electrochemical Diagnosis of Breast Cancer Based on a Hydrazine–Au Nanoparticle–Aptamer Bioconjugate. Anal. Chem. 2013, 85, 1058–1064. [Google Scholar] [CrossRef]
- Ribeiro, J.A.; Pereira, C.M.; Silva, A.F.; Sales, G.M.F. Disposable electrochemical detection of breast cancer tumour marker CA 15-3 using poly(Toluidine Blue) as imprinted polymer receptor. Biosens. Bioelectron. 2018, 109, 246–254. [Google Scholar] [CrossRef]
- Majd, S.M.; Salimi, A.; Ghasemi, F. An ultrasensitive detection of miRNA-155 in breast cancer via direct hybridization assay using two-dimensional molybdenum disulfide field-effect transistor biosensor. Biosens. Bioelectron. 2018, 105, 6–13. [Google Scholar] [CrossRef]
- Yazdani, Y.; Jalali, F.; Tahmasbi, H.; Akbari, M.; Talebi, N.; Shahrtash, S.A.; Mobed, A.; Alem, M.; Ghazi, F.; Dadashpour, M. Recent advancements in nanomaterial-based biosensors for diagnosis of breast cancer: A comprehensive review. Cancer Cell Int. 2025, 25, 50. [Google Scholar] [CrossRef]
- Sadeghi, M.; Sadeghi, S.; Naghib, S.M.; Garshasbi, H.R. A comprehensive review on electrochemical nano biosensors for precise detection of blood-based oncomarkers in breast cancer. Biosensors 2023, 13, 481. [Google Scholar] [CrossRef] [PubMed]
- Turk, Z.; Armani, A.; Jafari-Gharabaghlou, D.; Madakbas, S.; Bonabi, E.; Zarghami, N. A new insight into the early detection of HER2 protein in breast cancer patients with a focus on electrochemical biosensors approaches: A review. Int. J. Biol. Macromol. 2024, 272, 132710. [Google Scholar] [CrossRef]
- Wignarajah, S.; Chianella, I.; Tothill, I.E. Development of electrochemical immunosensors for HER-1 and HER-2 analysis in serum for breast cancer patients. Biosensors 2023, 13, 355. [Google Scholar] [CrossRef] [PubMed]
- Szymanska, B.; Lukaszewski, Z.; Hermanowicz-Szamatowicz, K.; Gorodkiewicz, E. An immunosensor for the determination of carcinoembryonic antigen by Surface Plasmon Resonance imaging. Anal. Biochem. 2020, 609, 113964. [Google Scholar] [CrossRef]
- Erol, K.; Hasabnis, G.; Altintas, Z. A Novel NanoMIP–SPR Sensor for the Point-of-Care Diagnosis of Breast Cancer. Micromachines 2023, 14, 1086. [Google Scholar] [CrossRef]
- Verma, P.; Kumar, A.; Jindal, P. Machine Learning Approach for SPR-based Photonic Crystal Fiber Sensor for Breast Cancer Cells Detection. In Proceedings of the 2022 IEEE 7th Forum on Research and Technologies for Society and Industry Innovation (RTSI), Paris, France, 24–26 August 2022. [Google Scholar]
- Han, Y.; Qiang, L.; Gao, Y.; Gao, J.; He, Q.; Liu, H.; Han, L.; Zhang, Y. Large-area surface-enhanced Raman spectroscopy substrate by hybrid porous GaN with Au/Ag for breast cancer miRNA detection. Appl. Surf. Sci. 2020, 541, 148456. [Google Scholar] [CrossRef]
- Wang, Y.; Wei, Z.; Luo, X.; Wan, Q.; Qiu, R.; Wang, S. An ultrasensitive homogeneous aptasensor for carcinoembryonic antigen based on upconversion fluorescence resonance energy transfer. Talanta 2018, 195, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Li, H.; Xu, J.; Huang, Y.; Zhang, X.; Weng, J.; Li, Z.; Sun, L. Ultrasensitive colorimetric biosensor for BRCA1 mutation based on multiple signal amplification strategy. Biosens. Bioelectron. 2020, 166, 112424. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhou, R.; Hao, Y.; Yang, P. A CD44-biosensor for evaluating metastatic potential of breast cancer cells based on quartz crystal microbalance. Sci. Bull. 2017, 62, 923–930. [Google Scholar] [CrossRef]
- Uliana, C.V.; Peverari, C.R.; Afonso, A.S.; Cominetti, M.R.; Faria, R.C. Fully disposable microfluidic electrochemical device for detection of estrogen receptor alpha breast cancer biomarker. Biosens. Bioelectron. 2017, 99, 156–162. [Google Scholar] [CrossRef]
- Nurlankyzy, M.; Kantoreyeva, K.; Myrkhiyeva, Z.; Ashikbayeva, Z.; Baiken, Y.; Kanayeva, D.; Tosi, D.; Bekmurzayeva, A. Label-free optical fiber biosensor for the detection of CD44-expressing breast cancer cells. Sens. Bio-Sens. Res. 2024, 44, 100661. [Google Scholar] [CrossRef]
- Gao, Y.; Qiang, L.; Chu, Y.; Han, Y.; Zhang, Y.; Han, L. Microfluidic chip for multiple detection of miRNA biomarkers in breast cancer based on three-segment hybridization. AIP Adv. 2020, 10, 045022. [Google Scholar] [CrossRef]
- Du, W.; Zhang, L.; Suh, E.; Lin, D.; Marcus, C.; Ozkan, L.; Ahuja, A.; Fernandez, S.; Shuvo, I.I.; Sadat, D.; et al. Conformable ultrasound breast patch for deep tissue scanning and imaging. Sci. Adv. Eng. 2023, 9, eadh5325. [Google Scholar] [CrossRef]
- Xu, X.; Chung, Y.; Brooks, A.D.; Shih, W.-H.; Shih, W.Y. Development of array piezoelectric fingers towards in vivo breast tumor detection. Rev. Sci. Instrum. 2016, 87, 124301. [Google Scholar] [CrossRef]
- Elsheakh, D.N.; Mohamed, R.A.; Fahmy, O.M.; Ezzat, K.; Eldamak, A.R. Complete Breast Cancer Detection and Monitoring System by Using Microwave Textile-Based Antenna Sensors. Biosensors 2023, 13, 87. [Google Scholar] [CrossRef]
- Elouerghi, A.; Bellarbi, L.; Khomsi, Z.; Jbari, A.; Errachid, A.; Yaakoubi, N. A Flexible Wearable Thermography System Based on Bioheat Microsensors Network for Early Breast Cancer Detection: IoT Technology. J. Electr. Comput. Eng. 2022, 2022, 5921691. [Google Scholar] [CrossRef]
- Sree, V.S.; Royea, R.; Buckman, K.J.; Benardis, M.; Holmes, J.; Fletcher, R.L.; EYK, N.; Acharya, R.; Ellenhorn, J.D.I. An introduction to the Cyrcadia Breast Monitor: A wearable breast health monitoring device. Comput. Methods Programs Biomed. 2020, 197, 105758. [Google Scholar]
- Yang, H.-Y.; Wang, Y.-C.; Peng, H.-Y.; Huang, C.-H. Breath biopsy of breast cancer using sensor array signals and machine learning analysis. Sci. Rep. 2022, 11, 103. [Google Scholar] [CrossRef] [PubMed]
- Díaz de León-Martínez, L.; Rodríguez-Aguilar, M.; Gorocica-Rosete, P.; Domínguez-Reyes, C.A.; Martínez-Bustos, V.; Tenorio-Torres, J.A.; Ornelas-Rebolledo, O.; Cruz-Ramos, J.A.; Balderas-Segura, B.; Flores-Ramírez, R. Identification of profiles of volatile organic compounds in exhaled breath by means of an electronic nose as a proposal for a screening method for breast cancer: A case-control study. J. Breath Res. 2020, 14, 046009. [Google Scholar] [CrossRef]
- Wan, H.-H.; Zhu, H.; Chiang, C.-C.; Li, J.-S.; Ren, F.; Tsai, C.-T.; Liao, Y.-T.; Neal, D.; Esquivel-Upshaw, J.F.; Pearton, S.J. High sensitivity saliva-based biosensor in detection of breast cancer biomarkers: HER2 and CA15-3. J. Vac. Sci. Technol. B 2024, 42, 023202. [Google Scholar] [CrossRef]
- Wei, F.; Patel, P.; Liao, W.; Chaudhry, K.; Zhang, L.; Arellano-Garcia, M.; Hu, S.; Elashoff, D.; Zhou, H.; Shukla, S.; et al. Electrochemical Sensor for Multiplex Biomarkers Detection. Imaging Diagn. Progn. 2009, 15, 13. [Google Scholar] [CrossRef]
- Torrente-Rodríguez, R.M.; Campuzano, S.; Ruiz-Valdepeñas Montiel, V.; Gamella, M.; Pingarrón, J.M. Electrochemical bioplatforms for the simultaneous determination of interleukin (IL)-8 mRNA and IL-8 protein oral cancer biomarkers in raw saliva. Biosens. Bioelectron. 2016, 77, 538–548. [Google Scholar] [CrossRef]
- Benet, J.G.; Seo, M.; Khine, M.; Padró, J.G.; Martínez, A.P.; Kurdahi, F. Breast cancer detection by analyzing the volatile organic compound (VOC) signature in human urine. Sci. Rep. 2022, 12, 14873. [Google Scholar]
- Leemans, M.; Cuzuel, V.; Bauër, P.; Aissa, H.B.; Cournelle, G.; Baelde, A.; Thuleau, A.; Cognon, G.; Pouget, N.; Guillot, E.; et al. Screening of Breast Cancer from Sweat Samples Analyzed by 2D-GC-MS: A Preliminary Study. Cancers 2023, 15, 2939. [Google Scholar] [CrossRef]
- Elsheakh, D.N.; Fahmy, O.M.; Farouk, M.; Ezzat, K.; Eldamak, A.R. An early breast cancer detection by using wearable flexible sensors and artificial intelligent. IEEE Access 2024, 12, 48511–48529. [Google Scholar] [CrossRef]
- Katsika, L.; Boureka, E.; Kalogiannidis, I.; Tsakiridis, I.; Tirodimos, I.; Lallas, K.; Tsimtsiou, Z.; Dagklis, T. Screening for Breast Cancer: A Comparative Review of Guidelines. Life 2024, 14, 777. [Google Scholar] [CrossRef] [PubMed]
- Wahab, M.R.A.; Palaniyandi, T.; Viswanathan, S.; Baskar, G.; Surendran, H.; Gangadharan, S.G.D.; Sugumaran, A.; Sivaji, A.; Kaliamoorthy, S.; Kumarasamy, S. Biomarker-specific biosensors revolutionise breast cancer diagnosis. Clin. Chim. Acta 2024, 555, 117792. [Google Scholar] [CrossRef]
- Chugh, V.; Basu, A.; Kaushik, A.; Bhansali, S.; Basu, A.K. Employing nano-enabled artificial intelligence (AI)-based smart technologies for prediction, screening, and detection of cancer. Nanoscale 2024, 16, 5458–5486. [Google Scholar] [CrossRef]
- Joshi, A.; GK, A.V.; Sakorikar, T.; Kamal, A.M.; Vaidya, J.S.; Pandya, H.J. Recent advances in biosensing approaches for point-of-care breast cancer diagnostics: Challenges and future prospects. Nanoscale Adv. 2021, 3, 5542–5564. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.L.; Loke, S.Y.; Lim, H.Q.; Balasundaram, G.; Chan, P.; Chong, B.K.; Tan, E.Y.; Lee, A.S.G.; Olivo, M. Circulating microRNA breast cancer biomarker detection in patient sera with surface plasmon resonance imaging biosensor. J. Biophotonics 2021, 14, e202100153. [Google Scholar] [CrossRef] [PubMed]
- Loyez, M.; Lobry, M.; Hassan, E.M.; DeRosa, M.C.; Caucheteur, C.; Wattiez, R. HER2 breast cancer biomarker detection using a sandwich optical fiber assay. Talanta 2021, 221, 121452. [Google Scholar] [CrossRef]
- Yildizhan, Y.; Driessens, K.; Tsao, H.S.K.; Boiy, R.; Thomas, D.; Geukens, N.; Hendrix, A.; Lammertyn, J.; Spasic, D. Detection of breast cancer-specific extracellular vesicles with fiber-optic SPR biosensor. Int. J. Mol. Sci. 2023, 24, 3764. [Google Scholar] [CrossRef]
- Yadav, A.K.; Verma, D.; Solanki, P.R. Enhanced Electrochemical Biosensing of the Sp17 Cancer Biomarker in Serum Samples via Engineered Two-Dimensional MoS2 Nanosheets on the Reduced Graphene Oxide Interface. ACS Appl. Biol. Mater. 2023, 6, 4250–4268. [Google Scholar] [CrossRef]
- Yadav, A.K.; Verma, D.; Kumar, A.; Bhatt, A.N.; Solanki, P.R. Biocompatible epoxysilane substituted polymer-based nano biosensing platform for label-free detection of cancer biomarker SP17 in patient serum samples. Int. J. Biol. Macromol. 2023, 239, 124325. [Google Scholar] [CrossRef]
- Katal, S.; McKay, M.J.; Taubman, K. PET molecular imaging in breast cancer: Current applications and future perspectives. J. Clin. Med. 2024, 13, 3459. [Google Scholar] [CrossRef]
- Ghosh, S.; Rajendran, R.L.; Mahajan, A.A.; Chowdhury, A.; Bera, A.; Guha, S.; Chakraborty, K.; Chowdhury, R.; Paul, A.; Jha, S.; et al. Harnessing exosomes as cancer biomarkers in clinical oncology. Cancer Cell Int. 2024, 24, 278. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.R.; Mughees, M.; Shaikh, S.; Choudhary, F.; Nizam, A.; Rizwan, A.; Narang, J. From Biosensors to Robotics: Pioneering Advances in Breast Cancer Management. Sensors 2024, 24, 6149. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Pros | Cons |
|---|---|---|
| Mammography | Reduction in breast cancer mortality Widely accessible Cost-effective for mass screening | Limited sensitivity in dense breast tissue Exposure to radiation False positives |
| MRI | High sensitivity (also in dense breasts) Effective for high-risk populations Improved detection of mammography-occult cancers | High cost Higher rate of false positives No definitive evidence of mortality reduction when used alone for screening |
| Ultrasound | No ionizing radiation exposure Well tolerated Detect small/node-negative cancers Less expensive | High rate of false positives Operator-dependent variability Less consistent than mammography or MRI |
| PET | Functional imaging to detect metabolic activity of tumors and evaluate treatment response Improves accuracy of cancer staging when combined with CT | High cost Complex image interpretation Lower specificity for small lesions and specific tracers Not suitable for routine screening |
| Ref. | Technique | Sample | Detection Accuracy | Sensitivity Specificity | Finality | Key Advantages | Key Limitations |
|---|---|---|---|---|---|---|---|
| [18] Shahrokhian et al., 2018 | Electrochemical DNA biosensor | Human serum | LOD: 3 fM | Both high | Detection of BRCA1 gene | Label-free, rapid, economical | Complexity of electrode preparation, interference |
| [20] Hakimian et al., 2020 | Electrochemical biosensor (CV) | Serum | Detection range: 2 10−20–2 10−12 mol | Ultrasensitive | Detection of miRNA-155 | Simple | Biological variability |
| [21] Hu et al., 2014 | Electrochemical bioaptasensor (DPV) | Serum | LOD: 2.2 nM | Both high | Detection of MUC1 | High sensitivity, wide linear range | Interference from complex sample components |
| [22] Zhao et al., 2011 | Electrochemical bioaptasensor (ACV) | Human serum and blood | LOD: 5 pM (190 pg/mL) | Both high | Detection of VEGF | Simple preparation, Regenerable, reusable, | Aptamer degradation, matrix interference |
| [23] Marques et al., 2014 | Electrochemical biosensor (LSV) | Human serum | LOD: 4.4 ng/mL | Not specified | Analysis of HER2 ECD | Sensitive, useful for follow-up | Enzyme stability, long analysis time |
| [24] Zhu et al., 2013 | Electrochemical biosensor (SWV) | Human serum | LOD: 0.037 ± 0.002 pg/mL | Both high | Detection of HER2 | Ultrasensitive, easy microscopic observation | Surface modification process |
| [25] Ribeiro et al., 2018 | Electrochemical biosensor based on MIP (CV-DPV) | Artificial/spike serum | LOD: <0.10 U/mL | Both high | Detection of CA15-3 | Cost-Effectiveness, Stability, Reusability | Interferences, Sample Variability, Quantification Limitations |
| [26] Majd et al., 2018 | FET biosensor (MoS2) | Human serum | LOD: 0.03 fM | Ultrasensitive, High | Detection of miRNA-155 | Label-free, good reproducibility | Stability issues with MoS2 and DNA probes |
| [31] Szymanska et al., 2020 | SPRi sensor | Blood plasma | LOD: 0.1 ng/mL | High sensitivity | Detection of CEA | Real-time analysis, high sensitivity | Non-specificity for breast cancer, interference |
| [32] Erol et al., 2023 | NanoMIP–SPR sensor | Human serum | LOD: 11.6 pg/mL | Both high | Detection of HER2 | Portable, label-free, rapid, cost-effective | Long-term stability, Specific training and equipment |
| [33] Verma et al., 2022 | PCF-SPR biosensor | Breast cancer cells | MSE: 0.1163 | Both high | Detection of MCF-7/MDA-MB-231 | High Sensitivity, Machine Learning | Design Parameters, Costs and Complexity |
| [34] Han et al., 2020 | SERS sensor | Human serum (miR-K12-5-5) | LOD: 8.84 × 10−10 M | High sensitivity | Detection of miR-K12-5-5p | Enhancement Factor, Uniformity, Stability | Stability, Need for Validation, Cross-reactivity |
| [35] Wang et al., 2018 | FRET-based aptasensor (UCNPs) | Human serum | LOD: 7.9 pg/mL–10.7 pg/mL | Both high | Detection of CEA | Simple configuration, direct operation | Non-specificity for breast cancer, FRET Complexity |
| [36] Bai et al., 2020 | Colorimetric biosensor | DNA extracted from blood | LOD: 10−18 M | Both high | BRCA1 mutation | Low cost, rapid, good reproducibility | Weak direct signals at low concentrations |
| [37] Yang et al., 2017 | QCM biosensor | BC cells (tumor tissue) | LOD: 300 cells/mL | High sensitivity | Metastatic potential | High sensitivity, label-free, real-time detection | Low specificity and clinical applicability |
| [39] Nurlankyzy et al., 2024 | Fiber-optic ball resonator sensor | CD44-expressing cancer cells | 335 cell/mL | High sensitivity | Early detection of breast cancer | Label-free and fast | Not tested in situ so far |
| [38] Uliana et al., 2017 | μFED | Calf serum | LOD: 10.0 fg/mL | Both high | Detection of ERα | Easy to produce, Multiple Applicability | Limitations in Testing |
| [40] Gao et al., 2020 | Microfluidic chip (three-segment hybridization) | Blood-extracted biomarker | LOD: 1 pM | Both high | Detection of miRNAs | Sensitive, rapid, economical | Requires optimization of hybridization conditions |
| [41] Du et al., 2023 | CUSBr | Breast tissue | LOD: 0.3 cm (cysts); 0.1 cm (anomalies) | Moderate (3 dB contrast) | Monitoring of anomalies/cysts | Non-invasive, standardized, repeatable | Operational skills, Image quality, Long-term stability, skin contact issues |
| [42] Xu et al., 2016 | Piezoelectric Finger array | Model tumors, Gelatin matrix | 96% accuracy (46/48 lesions) | High sensitivity | Anomalies in the elastic modulus | Direct measurement of tissue stiffness, in situ | Manual operation, time-consuming, small sample size |
| [43] Elsheakh et al., 2023 | Microwave textile-based antenna sensor | Phantom for breast tissue | 89% (Mean CatBoost) accuracy | Both moderate | BC detection/ classification | Non-invasive, wearable | Advanced equipment, Parameter limitations |
| [44] Elouerghi et al., 2022 | Thermography system (bioheat microsensors) | Mammary phantom | Accuracy 0.1 °C | 85% sensitivity 90% specificity | Thermal anomalies | Wearable, Non-invasive | Need for robust calibration to ensure accurate readings |
| [45] Sree et al., 2020 | Cyrcadia Breast Monitor | Breast tissue | 78% accuracy of ML model | 84% sensitivity 72% specificity | Anomaly detection | Machine Learning model, Non-invasive monitoring | Limitations in Data, Need for Further Validation |
| [46] Yang et al., 2021 | E-Nose | Alveolar exhaled breath | 91% accuracy | 86% sensitivity 97% specificity | BC detection/ classification | Machine Learning, Intra-operative applicability | Influenced by anesthetics, individual variability |
| [47] Díaz de León-Martínez et al., 2020 | E-Nose | Exhaled Breath | 98% CDA model accuracy | Both high | Screening for breast cancer | Machine Learning, Non-invasive, early screening | Sensitive to environmental factors, small sample size |
| [48] Wan et al., 2024 | Field-effect transistor (FET)-based biosensor | Saliva | LOD: 1 fg/mL | 70/dec HER2, 30/dec CA15-3 | Detection of HER2, CA15-3 | Non-invasive, rapid, easy to use | Cross-reactivity, need for clinical validation |
| [49] Wei et al., 2009 | Electrochemical biosensor | Saliva | LOD: 3.9 fM (mRNA), 7.4 pg/mL (protein) | 90% for both | Detection of IL8 mRNA/protein | Simultaneous detection, Non-invasive | Non-specificity for breast cancer, Limited sample size |
| [50] Torrente-Rodríguez et al., 2015 | Amperometric biosensor | Saliva | LOD: 0.21 nM (mRNA), 72.4 pg/mL (protein) | High sensitivity | Detection of IL8 mRNA/protein | Simultaneous detection, Non-invasive, easy to automate | Non-specificity for breast cancer, cross-reactivity |
| [51] Benet et al., 2022 | E-Nose and GC-MS | Urine | 92.31% (GC-MS) 75% (E-Nose) | 85.71% (GC-MS) 50% (E-Nose) | Detection of BCs VOCs | Non-invasive, low-cost, Machine Learning | Specificity of sensors, Variability of VOCs |
| [52] Leemans et al., 2022 | GC × GC − MS | Sweat | F1-score: 0.93 | 1.0 sensitivity 0.8 specificity | Identification of BC- VOCs | Non-invasive, low-cost, Machine Learning | Limited sample size, Variability in VOCs |
| [53] Elsheakh, D. N. et al. | Werable flexible antenna-based sensors | In situ | Simulation with tumors down to 5–10 mm | NA | Early detection and monitoring | Wearable | Only simulation tests so far |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grasso, A.; Altomare, V.; Fiorini, G.; Zompanti, A.; Pennazza, G.; Santonico, M. Innovative Methodologies for the Early Detection of Breast Cancer: A Review Categorized by Target Biological Samples. Biosensors 2025, 15, 257. https://doi.org/10.3390/bios15040257
Grasso A, Altomare V, Fiorini G, Zompanti A, Pennazza G, Santonico M. Innovative Methodologies for the Early Detection of Breast Cancer: A Review Categorized by Target Biological Samples. Biosensors. 2025; 15(4):257. https://doi.org/10.3390/bios15040257
Chicago/Turabian StyleGrasso, Antonella, Vittorio Altomare, Giulia Fiorini, Alessandro Zompanti, Giorgio Pennazza, and Marco Santonico. 2025. "Innovative Methodologies for the Early Detection of Breast Cancer: A Review Categorized by Target Biological Samples" Biosensors 15, no. 4: 257. https://doi.org/10.3390/bios15040257
APA StyleGrasso, A., Altomare, V., Fiorini, G., Zompanti, A., Pennazza, G., & Santonico, M. (2025). Innovative Methodologies for the Early Detection of Breast Cancer: A Review Categorized by Target Biological Samples. Biosensors, 15(4), 257. https://doi.org/10.3390/bios15040257