Duplex Vertical-Flow Rapid Tests for Point-of-Care Detection of Anti-dsDNA and Anti-Nuclear Autoantibodies

Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the VFA
2.2. Test Samples
2.3. Comparison with ELISA
2.4. Statistical Analysis
3. Results
3.1. Detection of Antinuclear Antibody Using Spiked Human Anti-dsDNA Positive Control Standard and the Duplex VFA
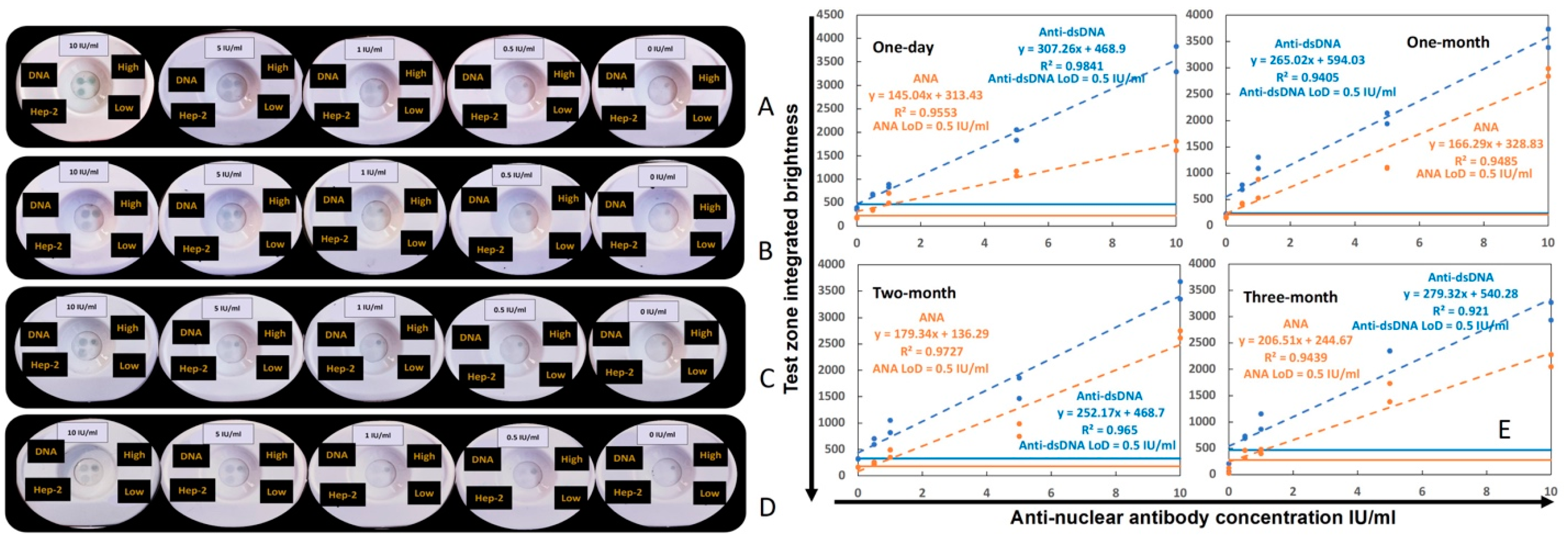
3.2. Impact of Storage Duration on the Performance of the ANA–αDNA VFA
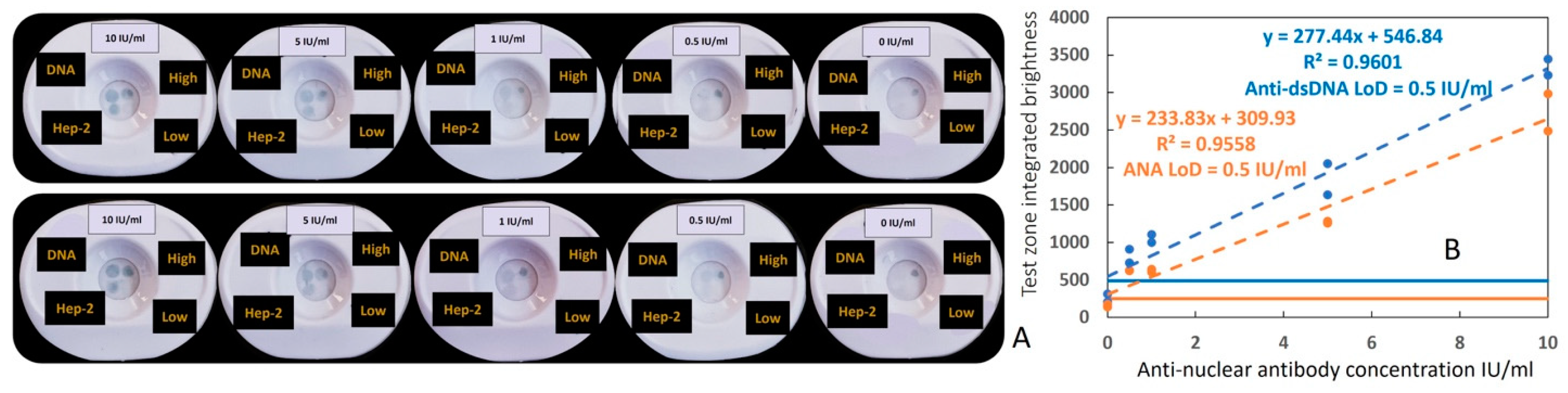
3.3. Inter-Operator Coefficient of Variation in Operating the Duplex ANA–αDNA VFA
3.4. Testing Clinical Serum Samples Using the Duplex ANA–αDNA VFA and ELISA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pisetsky, D.S. Antinuclear antibody testing—Misunderstood or misbegotten? Nat. Rev. Rheumatol. 2017, 13, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Bossuyt, X.; De Langhe, E.; Borghi, M.O.; Meroni, P.L. Understanding and interpreting antinuclear antibody tests in systemic rheumatic diseases. Nat. Rev. Rheumatol. 2020, 16, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Pisetsky, D.S. Antinuclear Antibodies in Rheumatic Disease: A Proposal for a Function-Based Classification. Scand. J. Immunol. 2012, 76, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.M.; Feltkamp, T.E.W.; Smolen, J.S.; Butcher, B.; Dawkins, R.; Fritzler, M.J.; Gordon, T.; Hardin, J.A.; Kalden, J.R.; Lahita, R.G.; et al. Range of antinuclear antibodies in “healthy” individuals. Arthritis Rheum. 1997, 40, 1601–1611. [Google Scholar] [CrossRef]
- Maddison, P.J. Mixed connective tissue disease: Overlap syndromes. Bailliere’s best practice & research. Clin. Rheumatol. 2000, 14, 111–124. [Google Scholar] [CrossRef]
- Kavanaugh, A.; Tomar, R.; Reveille, J.; Solomon, D.H.; Homburger, H.A. Guidelines for Clinical Use of the Antinuclear Antibody Test and Tests for Specific Autoantibodies to Nuclear Antigens. Arch. Pathol. Lab. Med. 2000, 124, 71–81. [Google Scholar] [CrossRef]
- Hernández-Molina, G.; Nuñez-Alvarez, C.; Avila-Casado, C.; Llorente, L.; Hernández-Hernández, C.; Calderillo, M.L.; Marroquín, V.; Recillas-Gispert, C.; Romero-Díaz, J.; Sánchez-Guerrero, J. Usefulness of IgA Anti-α-fodrin Antibodies in Combination with Rheumatoid Factor and/or Antinuclear Antibodies as Substitute Immunological Criterion in Sjögren Syndrome with Negative Anti-SSA/SSB Antibodies. J. Rheumatol. 2016, 43, 1852–1857. [Google Scholar] [CrossRef]
- Delgado, J.; Vodonos, A.; Malnick, S.; Kriger, O.; Wilkof-Segev, R.; Delgado, B.; Novack, V.; Rosenthal, A.; Menachem, Y.; Melzer, E.; et al. Autoimmune hepatitis in southern Israel: A 15-year multicenter study. J. Dig. Dis. 2013, 14, 611–618. [Google Scholar] [CrossRef]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.E.; Czaja, A.J.; Desmet, V.J.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef]
- Al-Chalabi, T.; Boccato, S.; Portmann, B.C.; McFarlane, I.G.; Heneghan, M.A. Autoimmune hepatitis (AIH) in the elderly: A systematic retrospective analysis of a large group of consecutive patients with definite AIH followed at a tertiary referral centre. J. Hepatol. 2006, 45, 575–583. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Brinks, R.; Dörner, T.; Daikh, D.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) SLE classification criteria item performance. Ann. Rheum. Dis. 2021, 80, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Egner, W. The use of laboratory tests in the diagnosis of SLE. J. Clin. Pathol. 2000, 53, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Satoh, M.; Chan, E.K.; Ho, L.A.; Rose, K.M.; Parks, C.G.; Cohn, R.D.; Jusko, T.A.; Walker, N.J.; Germolec, D.R.; Whitt, I.Z.; et al. Prevalence and sociodemographic correlates of antinuclear antibodies in the United States. Arthritis Rheum. 2012, 64, 2319–2327. [Google Scholar] [CrossRef] [PubMed]
- Selmi, C.; Ceribelli, A.; Generali, E.; Scirè, C.A.; Alborghetti, F.; Colloredo, G.; Porrati, L.; Achenza, M.I.S.; De Santis, M.; Cavaciocchi, F.; et al. Serum antinuclear and extractable nuclear antigen antibody prevalence and associated morbidity and mortality in the general population over 15 years. Autoimmun. Rev. 2016, 15, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Shovman, O.; Gilburd, B.; Barzilai, O.; Shinar, E.; Larida, B.; Zandman-Goddard, G.; Binder, S.R.; Shoenfeld, Y. Evaluation of the BioPlex™ 2200 ANA Screen: Analysis of 510 Healthy Subjects: Incidence of Natural/Predictive Autoantibodies. Ann. N. Y. Acad. Sci. 2005, 1050, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Mariz, H.A.; Sato, E.I.; Barbosa, S.H.; Rodrigues, S.H.; Dellavance, A.; Andrade, L.E.C. Pattern on the antinuclear antibody–HEp-2 test is a critical parameter for discriminating antinuclear antibody–positive healthy individuals and patients with autoimmune rheumatic diseases. Arthritis Rheum. 2011, 63, 191–200. [Google Scholar] [CrossRef]
- Hahn, B.H. Antibodies to DNA. N. Engl. J. Med. 1998, 338, 1359–1368. [Google Scholar] [CrossRef]
- Isenberg, D.A.; Manson, J.J.; Ehrenstein, M.R.; Rahman, A. Fifty years of anti-ds DNA antibodies: Are we approaching journey’s end? Rheumatology 2007, 46, 1052–1056. [Google Scholar] [CrossRef]
- Lou, H.; Wojciak-Stothard, B.; Ruseva, M.M.; Cook, H.T.; Kelleher, P.; Pickering, M.C.; Xu, X.N. Autoantibody-dependent amplification of inflammation in SLE. Cell Death Dis. 2020, 11, 729. [Google Scholar] [CrossRef]
- Orme, M.E.; Voreck, A.; Aksouh, R.; Schreurs, M.W.J. Anti-dsDNA Testing Specificity for Systemic Lupus Erythematosus: A Systematic Review. J. Appl. Lab. Med. 2022, 7, 221–239. [Google Scholar] [CrossRef] [PubMed]
- Orme, M.E.; Voreck, A.; Aksouh, R.; Ramsey-Goldman, R.; Schreurs, M.W.J. Systematic review of anti-dsDNA testing for systemic lupus erythematosus: A meta-analysis of the diagnostic test specificity of an anti-dsDNA fluorescence enzyme immunoassay. Autoimmun. Rev. 2021, 20, 102943. [Google Scholar] [CrossRef] [PubMed]
- Wichainun, R.; Kasitanon, N.; Wangkaew, S.; Hongsongkiat, S.; Sukitawut, W.; Louthrenoo, W. Sensitivity and specificity of ANA and anti-dsDNA in the diagnosis of systemic lupus erythematosus: A comparison using control sera obtained from healthy individuals and patients with multiple medical problems. Asian Pac. J. Allergy Immunol. 2013, 31, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, M.R.; James, J.A.; Kohlhase, K.F.; Rubertone, M.V.; Dennis, G.J.; Harley, J.B. Development of Anti-dsDNA Autoantibodies Prior to Clinical Diagnosis of Systemic Lupus Erythematosus. Scand. J. Immunol. 2001, 54, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Alsaed, O.S.; Alamlih, L.I.; Al-Radideh, O.; Chandra, P.; Alemadi, S.; Al-Allaf, A.-W. Clinical utility of ANA-ELISA vs ANA-immunofluorescence in connective tissue diseases. Sci. Rep. 2021, 11, 8229. [Google Scholar] [CrossRef] [PubMed]
- Meroni, P.L.; Schur, P.H. ANA screening: An old test with new recommendations. Ann. Rheum. Dis. 2010, 69, 1420–1422. [Google Scholar] [CrossRef] [PubMed]
- Colglazier, C.L.; Sutej, P.G. Laboratory Testing in the Rheumatic Diseases: A Practical Review. South Med. J. 2005, 98, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Kendall, J.; Reeves, B.; Clancy, M. Point of care testing: Randomised controlled trial of clinical outcome. BMJ 1998, 316, 1052–1057. [Google Scholar] [CrossRef]
- Lewandrowski, K.; Flood, J.; Finn, C.; Tannous, B.; Farris, A.B.; Benzerx, T.I.; Lee-Lewandrowski, E. Implementation of Point-of-Care Rapid Urine Testing for Drugs of Abuse in the Emergency Department of an Academic Medical Center. Am. J. Clin. Pathol. 2008, 129, 796–801. [Google Scholar] [CrossRef]
- Lei, R.; Huo, R.; Mohan, C. Current and emerging trends in point-of-care urinalysis tests. Expert Rev. Mol. Diagn. 2020, 20, 69–84. [Google Scholar] [CrossRef]
- Gubala, V.; Harris, L.F.; Ricco, A.J.; Tan, M.X.; Williams, D.E. Point of Care Diagnostics: Status and Future. Anal. Chem. 2011, 84, 487–515. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Ahmed, R.; Damayantharan, M.; Ünal, B.; Butt, H.; Yetisen, A.K. Lateral and Vertical Flow Assays for Point-of-Care Diagnostics. Adv. Healthc. Mater. 2019, 8, 1900244. [Google Scholar] [CrossRef] [PubMed]
- Schonhorn, J.E.; Fernandes, S.C.; Rajaratnam, A.; Deraney, R.N.; Rolland, J.P.; Mace, C.R. A device architecture for three-dimensional, patterned paper immunoassays. Lab Chip 2014, 14, 4653–4658. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.K.; Joung, H.-A.; Kim, S.; Kim, M.-G. Vertical flow immunoassay (VFA) biosensor for a rapid one-step immunoassay. Lab Chip 2013, 13, 768. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Lee, J.H. Paper-Based Biosensors with Lateral/Vertical Flow Assay. In Bioanalysis; Springer: Singapore, 2020; pp. 115–136. [Google Scholar] [CrossRef]
- Lei, R.; Wang, D.; Arain, H.; Mohan, C. Design of Gold Nanoparticle Vertical Flow Assays for Point-of-Care Testing. Diagnostics 2022, 12, 1107. [Google Scholar] [CrossRef]
- Li, J.; Macdonald, J. Multiplexed lateral flow biosensors: Technological advances for radically improving point-of-care diagnoses. Biosens. Bioelectron. 2016, 83, 177–192. [Google Scholar] [CrossRef]
- Vu, B.V.; Lei, R.; Mohan, C.; Kourentzi, K.; Willson, R.C. Flash Characterization of Smartphones Used in Point-of-Care Diagnostics. Biosensors 2022, 12, 1060. [Google Scholar] [CrossRef]
- Lei, R.; Vu, B.; Kourentzi, K.; Soomro, S.; Danthanarayana, A.N.; Brgoch, J.; Nadimpalli, S.; Petri, M.; Mohan, C.; Willson, R.C. A novel technology for home monitoring of lupus nephritis that tracks the pathogenic urine biomarker ALCAM. Front. Immunol. 2022, 13, 1044743. [Google Scholar] [CrossRef]
- Prajapati, A.; Verma, N.; Pandya, A. Highly sensitive vertical flow based point-of-care immunokit for rapid and early detection of human CRP as a cardiovascular risk factor. Biomed. Microdevices 2020, 22, 28. [Google Scholar] [CrossRef]
- Lei, R.; Arain, H.; Obaid, M.; Sabhnani, N.; Mohan, C. Ultra-Sensitive and Semi-Quantitative Vertical Flow Assay for the Rapid Detection of Interleukin-6 in Inflammatory Diseases. Biosensors 2022, 12, 756. [Google Scholar] [CrossRef]
- Doria, A.; Zen, M.; Canova, M.; Bettio, S.; Bassi, N.; Nalotto, L.; Rampudda, M.; Ghirardello, A.; Iaccarino, L. SLE diagnosis and treatment: When early is early. Autoimmun. Rev. 2010, 10, 55–60. [Google Scholar] [CrossRef]
- Doria, A.; Arienti, S.; Rampudda, M.; Canova, M.; Tonon, M.; Sarzi-Puttini, P. Preventive strategies in systemic lupus erythematosus. Autoimmun. Rev. 2008, 7, 192–197. [Google Scholar] [CrossRef]
- Koelmeyer, R.; Nim, H.T.; Nikpour, M.; Sun, Y.B.; Kao, A.; Guenther, O.; Hoi, A. High disease activity status suggests more severe disease and damage accrual in systemic lupus erythematosus. Lupus Sci. Med. 2020, 7, e000372. [Google Scholar] [CrossRef]
- Bentow, C.; Lakos, G.; Martis, P.; Wahl, E.; Garcia, M.; Viñas, O.; Mahler, M. International multi-center evaluation of a novel chemiluminescence assay for the detection of anti-dsDNA antibodies. Lupus 2016, 25, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Andrejevic, S.; Jeremic, I.; Sefik-Bukilica, M.; Nikolic, M.; Stojimirovic, B.; Bonaci-Nikolic, B. Immunoserological parameters in SLE: High-avidity anti-dsDNA detected by ELISA are the most closely associated with the disease activity. Clin. Rheumatol. 2013, 32, 1619–1626. [Google Scholar] [CrossRef]
- Pan, N.; Amigues, I.; Lyman, S.; Duculan, R.; Aziz, F.; Crow, M.; Kirou, K. A surge in anti-dsDNA titer predicts a severe lupus flare within six months. Lupus 2013, 23, 293–298. [Google Scholar] [CrossRef]
- Narayanan, K.; Marwaha, V.; Shanmuganandan, K.; Shankar, S. Correlation between Systemic Lupus Erythematosus Disease Activity Index, C3, C4 and Anti-dsDNA Antibodies. Med. J. Armed Forces India 2010, 66, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xia, Y. Anti-double Stranded DNA Antibodies: Origin, Pathogenicity, and Targeted Therapies. Front. Immunol. 2019, 10, 1667. [Google Scholar] [CrossRef]
- Manson, J.J.; Ma, A.; Rogers, P.; Mason, L.J.; Berden, J.H.; van der Vlag, J.; D’Cruz, D.P.; Isenberg, D.A.; Rahman, A. Relationship between anti-dsDNA, anti-nucleosome and anti-alpha-actinin antibodies and markers of renal disease in patients with lupus nephritis: A prospective longitudinal study. Arthritis Res. Ther. 2009, 11, R154. [Google Scholar] [CrossRef]
- Sherer, Y.; Gorstein, A.; Fritzler, M.J.; Shoenfeld, Y. Autoantibody explosion in systemic lupus erythematosus: More than 100 different antibodies found in SLE patients. Semin. Arthritis Rheum. 2004, 34, 501–537. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C.; Mohan, C. Urinary Biomarkers in Lupus Nephritis: Are We There Yet? Arthritis Rheumatol. 2021, 73, 194–196. [Google Scholar] [CrossRef]
- Soomro, S.; Stanley, S.; Lei, R.; Saxena, R.; Petri, M.; Mohan, C. Comprehensive Urinomic Identification of Protein Alternatives to Creatinine Normalization for Diagnostic Assessment of Lupus Nephritis. Front. Immunol. 2022, 13, 853778. [Google Scholar] [CrossRef]
- Lei, R.; Thai, N.; Li, Y.; Petri, M.; Mohan, C. Analytical validation of urine ALCAM ELISA as a test for lupus nephritis. Expert Rev. Mol. Diagn. 2023, 23, 729–738. [Google Scholar] [CrossRef]
- Li, H.; Zheng, Y.; Chen, L.; Lin, S. High titers of antinuclear antibody and the presence of multiple autoantibodies are highly suggestive of systemic lupus erythematosus. Sci. Rep. 2022, 12, 1687. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Du, Y.; Wu, Q.; Li, H.; Nguyen, T.; Gidley, G.; Duran, V.; Goldman, D.; Petri, M.; Mohan, C. Salivary anti-nuclear antibody (ANA) mirrors serum ANA in systemic lupus erythematosus. Arthritis Res. Ther. 2022, 24, 3. [Google Scholar] [CrossRef] [PubMed]
- Stanescu, I.I.; Calenic, B.; Dima, A.; Gugoasa, L.A.; Balanescu, E.; Stefan-van Staden, R.I.; Baicus, C.; Badita, D.G.; Greabu, M. Salivary biomarkers of inflammation in systemic lupus erythematosus. Ann. Anat. Anat. Anz. 2018, 219, 89–93. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Healthy Controls | Active LN |
|---|---|---|
| n = 18 | n = 19 | |
| Race | ||
| White | 10 | 2 |
| Black | 6 | 8 |
| Hispanic | 0 | 8 |
| Asian | 2 | 1 |
| Age (yr) | ||
| Mean | 31 ± 9.2 | 30 ± 10.3 |
| Range | 18–53 | 19–60 |
| Sex | ||
| Female | 11 | 12 |
| Male | 7 | 7 |
| SLEDAI | ||
| Mean | N/A | 11 ± 6.0 |
| Range | N/A | 4–20 |
| rSLEDAI | ||
| Mean | N/A | 7 ± 3.5 |
| Range | N/A | 412 |
| IU/mL | ANA | Anti-dsDNA | ||||
|---|---|---|---|---|---|---|
| Operator-1 | Operator-2 | CV% | Operator-1 | Operator-2 | CV% | |
| 10 | 1711 | 2735 | 33 | 3561 | 3338 | 5 |
| 5 | 1121 | 1271 | 9 | 1944 | 1841 | 4 |
| 1 | 598 | 622 | 3 | 860 | 1054 | 14 |
| 0.5 | 349 | 624 | 40 | 676 | 818 | 13 |
| 0 | 182 | 157 | 11 | 374 | 261 | 25 |
| 19 | 12 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lei, R.; Arain, H.; Wang, D.; Arunachalam, J.; Saxena, R.; Mohan, C. Duplex Vertical-Flow Rapid Tests for Point-of-Care Detection of Anti-dsDNA and Anti-Nuclear Autoantibodies. Biosensors 2024, 14, 98. https://doi.org/10.3390/bios14020098
Lei R, Arain H, Wang D, Arunachalam J, Saxena R, Mohan C. Duplex Vertical-Flow Rapid Tests for Point-of-Care Detection of Anti-dsDNA and Anti-Nuclear Autoantibodies. Biosensors. 2024; 14(2):98. https://doi.org/10.3390/bios14020098
Chicago/Turabian StyleLei, Rongwei, Hufsa Arain, David Wang, Janani Arunachalam, Ramesh Saxena, and Chandra Mohan. 2024. "Duplex Vertical-Flow Rapid Tests for Point-of-Care Detection of Anti-dsDNA and Anti-Nuclear Autoantibodies" Biosensors 14, no. 2: 98. https://doi.org/10.3390/bios14020098
APA StyleLei, R., Arain, H., Wang, D., Arunachalam, J., Saxena, R., & Mohan, C. (2024). Duplex Vertical-Flow Rapid Tests for Point-of-Care Detection of Anti-dsDNA and Anti-Nuclear Autoantibodies. Biosensors, 14(2), 98. https://doi.org/10.3390/bios14020098