Advances in Respiratory Monitoring: A Comprehensive Review of Wearable and Remote Technologies

 ,
, 
Abstract
1. Introduction
2. Chest and Abdominal Movement Detection
2.1. Chest Belts and Their Modern Alternatives
2.2. Seismocardiography, Ballistocardiography, and Similar Methods
2.3. Chest Impedance Measurement—Bioamplifiers
2.4. Optical Fibers
2.5. Radar Systems
2.6. Camera Systems

{kind=link}
{kind=link}
| Sensor Type | Application | Sensing Element | Key Parameters | Ref. |
|---|---|---|---|---|
| Chest belt | Respiration | Resistance based | BLE 1, IMU 2, Motion detection | [35] |
| Chest belt | RR 3, HR 4, HRV 5, activity | Proprietary sensor | Bluetooth, Mobile app, 24 h working time | [45] |
| Patch on chest and abdomen | RR, RV 6 | Piezoresistive sensors | Bluetooth, Small footprint, Linear response | [36] |
| Band over chest or abdomen | Apnea, cough, and deep breathing | Piezoelectric sensor | Bluetooth, Mobile app, Fish lateral line structure, PVDF 7, Low detection limit 0.5 mN, Sensitivity 0.24 V/N, Response time 4 ms | [37] |
| Patch on chest | RR | Piezoelectric | PVDF, Matlab R2022b post processing | [38] |
| Belt around abdomen or thorax | Sleep monitoring | Textile RIP 8 sensor | Digital frequency-counting algorithm, Wireless communication, 800 mAh Li-pol battery, 380 kHz resonance frequency, Peak consumption 140 mW | [39] |
| Chest belt | Respiratory flow, RR, RV | Capacitive sensor, accelerometer | Bluetooth, IMU, Motion correction, Sampling rate 30 Hz | [41] |
| Chest and abdomen e-textile belts | RR, RV | Capacitive sensor | E-textile sensors, Bluetooth, Estimation error reduction, Operational frequency 100 Hz | [42] |
| Waist belt | RR | Capacitive sensor | Working pressure range up to 200 kPa, Durability over 6000 cycles | [43] |
| Chest belt | RR, apnea | Rotating thin-film triboelectric nanogenerator | Retractable self-powered sensor, Wi-Fi, 1 million stretching cycles | [34] |
| Patch on the chest | Breathing, vital signs, disease progression | Proprietary sensor | Breathing pattern, Tidal volume, HR, BT 9, Activity, Wireless communication, Mobile app, AI-Powered disease progression assessment | [20] |
| Sensor under clothes | Respiration, activity, HR | PPG sensor | Bluetooth, Cellular-based hub, Mobile app | [21] |
| E-Textile Antenna | RR, HR | RF antenna sensor | Broadband monopole antenna, Conductive fabric | [46] |
| Textile vest | SCG, BCG, ECG, respiration | Accelerometer, piezoresistive plethysmograph | Accelerometer ST LIS3LV02DL, ±2 g, 12-bit, Textile ECG electrodes, Textile piezoresistive plethysmograph, Sampling rate 200 Hz, Bluetooth | [74] |
| Body attachment | SCG, ECG, respiration | Accelerometer, piezoelectric respiratory belt | MMA8451Q accelerometer, 14-bit, Sampling rate 800 Hz, Piezoelectric respiratory belt transducer MLT1132, ECG Front-end AD8232, Freescale FRDM-KL25Z acquisition board, FFT processing | [75] |
| Body attachment | Force- cardiography | Force-sensing resistor | FSR03CE, FCG compared to EDR 10 and respiration band, NI-USB6009 DAQ board, 13-bit, Sampling rate 5 kHz | [23] |
| Clip attached to bra | Respiration, stress, activity | Accelerometer | RR, HR, BLE 7 | [77] |
| Chest strap | Respiration monitoring | Accelerometer, Inductive type respiration sensor | Random forest classifier, Sampling rate 1 kHz, 16-bit, Bluetooth, Minimalization of movement artefacts | [79] |
| Chest mounted | SCG, respiration, apnea | MEMS 11 accelerometer | Accelerometer LIS3L02AL, 0–100 Hz, Frequency domain analysis of inspiration, expiration, and apnea. | [82] |
| Soft skin attached to the neck | Respiratory, swallowing biomechanics | Mechano-acoustic sensors, 2 × IMU | 2× IMU units, 200 Hz sampling rate for x,y-axis, 1600 Hz for z-axis, haptic sensor, RR, HR, swallowing, NFC, BLE | [24] |
| Behind the ear | BCG, PPG, blood pressure | 2 capacitive electrodes | BCG—25 mm × 25 mm hybrid sensor for differential sensing and dry electrode for feedback, High-impedance LMC6064 amplifier | [83] |
| Chest attached | Biopotential sensors, respiration sounds | Biopotential electrodes, piezoelectric microphone | EMG 12, Intercostals and diaphragm movement, Microphone: 20–100 Hz, 16-bit, 2.4 GHz wireless communication | [29] |
| Under the mattress | BCG, HRV and sleep tracking | BCG | RR, HR, HRV, Sleep monitoring, Bed movements, Stress level, Snoring, Sleep quality | [86] |
| Under the mattress | BCG, HR, RR | Accelerometer, force sensors | Piezoelectric PVDF film and electret polymer material, Sensor location testing | [87] |
| Mattress | BCG, HR, RR, breathing patterns | Multi-channel optical sensor-array | 2× IR LEDs SFH4250 and photodiode BPW34FAS, Dynamic forces modulated the light intensity, NI USB-6009 acquisition unit | [88] |
| Bed embedded | BCG, pattern recognition, HR, RR | Load cell | Off-the-shelf load cell installed on a typical hospital bed with a ML 13 algorithm, Low-cost, Detection rate 83.9% | [91] |
| Mattress | BCG, HR, RR | Two pressure pads on mattress | BCG evaluation in a sleep monitoring system | [92] |
| Mattress | BCG, HR, RR, apnea | Set of oil pressure sensors | 16-bit, Sampling rate 100 Hz, KSVM 14 model, Apnea precision rate 90.46% | [93] |
| Bed installed | BCG, HR, RR | 4 load cells | 4× CBCL-6L, Wheatstone bridge, AD8221 amplifier, HR error 2.55%, RR error 2.66% | [94] |
| Bed | BCG, respiratory disorders | Tensimeters on the bed legs | CNN 15 analysis, Accuracy of 96.4%, Sensitivity 92.5%, Specificity 98.1% | [95] |
| Force plate | BCG, RR, posture | Biomechanical force plate | 3D piezoelectric load cells 9286B, Kistler®, 600 × 400 mm, Sampling rate 960 Hz, Time warping averaging | [96] |
| Seat | BCG, HR, RR | Pressure sensor | Air cushion connected to Treston DMP 331 | [97] |
| 3 electrodes on the chest | RR, detection of tachypnoea | Impedance pneumo-graph | Dual vector approach | [98] |
| Electrodes on the chest | RR | EIP 16, 3D accelerometer | Adaptive noise cancellation, Band-pass filtering | [99] |
| Electrodes on the chest | RR, RV | EIP | Segregated envelope and carrier detection | [100] |
| Integrated circuit | ECG, EEG, RR | EIP ADS129xR | 8-channels, 24-bit Analog Front-End, Sampling rate 250 Hz–32 kHz, −115 dB CMRR, Internal oscillator | [101] |
| Integrated circuit | ECG, respiration | EIP AFE4960 | 2 channels, 22-bit, Single ADC, SPI and I2C interface, Sine wave or square wave excitation | [102] |
| Integrated circuit | ECG, optical HR, respiration | EIP AFE4500 | 4 input channels, 22-bit, single ADC, SPI and I2C interface | [103] |
| Integrated circuit | ECG, respiration, pace detection | EIP ADAS1000 | 5 acquisition channels and one driven lead, Serial interface SPI/QSPI, AC and DC lead-off detection | [104] |
| Integrated circuit | ECG, respiration, pace detection | EIP MAX30001 | High Input Impedance (>1 GΩ), High-Speed SPI interface, 32-Word ECG and 8-Word BioZ FIFOs, EMI filtering, ESD protection, DC leads-off detection | [105] |
| Integrated circuit | PPG, ECG, BioZ, EDA | EIP AS7058 | 2 ADC (20-bit) for PPG acquisition, 1 ADC (20-bit) for ECG/BIOZ acquisition, SPI and I2C interface | [106] |
| Chest belt | HR, RR, BP, PWT | 400 µm multimode OF 17 | Laboratory testing, HRV 2.5%, NA 18 = 0.5, Single digital camera for signal acquisition | [118] |
| Chest belt | RR | D-shaped POF 19 | RR under different movement | [126] |
| Chest belt | RR | POF sensor | Error 3 min−1 | [125] |
| Chest belt | RR | FBG 20 sensor | Tested wavelengths 525, 660, 850, 1310, 1550 nm MRI 21 compatible, Elongation up to 3% | [22] |
| Textile | RR, apnea | Two FBGs | RR during sport, 10 mm of grating length, | [116] |
| T-shirt | HR, RR | Three FBGs glued on the textile with silicone rubber | Highly stretchable and compressible | [107] |
| Mattress | HR, RR, activity | POF sensor | HR error 2 min−1, RR error 1 min−1 | [127] |
| Mattress embedded | RR | 4 × 4 matrix structures of POFs | 645 nm and silicon photodiode, Arduino Resolution 2.2–4.5%/N | [128] |
| Smart bed | ECG, HR, BP 22, PPG, BT | Inspired O2 FBG in fabric | Monitoring patient under MRI | [117] |
| Chest belt | RR | POF-GPL 23 sensor | Polymethylmethacrylate core with a diameter of 485 μm, Base material-thermoplastic polyurethane | [129] |
| Chest belt | RR HR | Multimode silica OF with an elastomer OF | Filtering 0.1 Hz to 0.4 Hz | [121] |
| Smartphone | RR | Smartphone-integrated POF | Cloud connectivity | [142] |
| Chair back | BCG, HR, RR | Microbend OF | Gaussian mixture model and classification based on K-Nearest Neighbors, Accuracy 94.6%. | [122] |
| Radar | HR, RR, athletes monitoring | Stationary parabolic antenna | Operational frequency 24.1 GHz, Transmitter output 30 mW, Radius 0.6 m, Antenna gain 40 dB | [130] |
| Micro-radar | RR | Wearable neck pendent radar | Operational frequency 24 GHz, Wi-Fi communication | [131] |
| Radar | SCG, HR, suitable for RR | Two stationary antennas | Operational frequency 5.8 GHz, Transmitting power 6 dBm | [132] |
| Radar | BCG, RR, HR | Stationary antenna | Operational frequency 24 GHz, Transmitter power output 35 mW | [133] |
| Antenna worn on the chest or abdomen | RR, RV, HR | Monopole helical antenna | Operational frequency 1.82/1.90 GHz, Transmitting power 12.84/10.42 dBm | [134] |
| Camera system | RR, HR, HRV | Commercial camera | Motion compensation, Two-phase temporal filtering, Signal pruning | [135] |
| Camera system | RR, RV | Infrared cameras | Twelve retro-reflexive markers, 8 IR cameras, Sampling rate 100 Hz | [136] |
| Camera system | RR | Infrared camera | Tracking region of interest, Mean shift localization | [137] |
| Camera system | RR, HR | Infrared camera | Long-wave IR sensing, Wavelet analysis, Thermal sensitivity of 0.025 °C, 14-bit dynamic range | [138] |
| Camera system | RR | Infrared camera | Thermal sensitivity of 0.08 K, 50 fps | [14] |
| Camera system | Respiration phases | Infrared camera | FLIR A325sc with 50 μm lens, 60 fps, Resolution 320 × 240, No image segmentation | [140] |
3. ECG-Derived Respiration
3.1. Determination of EDR from Amplitude
3.2. Determination of EDR from HRV
| Sensor Type | Application | Sensing Element | Key Parameters | Ref. |
|---|---|---|---|---|
| Wrist-worn EDR 1 | RR, ventilation | ECG 2, IMU 3 sensors | For asthma patients, IMU sample rate 250 Hz, Using during physical activity | [155] |
| Armband EDR | RR 4, tidal volume | ECG | EDRs from the morphology of the QRS complex: QRS slope range, R-wave angle, R-S amplitude | [157] |
| Chest sensor | RR, HRV 5 | ECG electrodes | 3 EDR algorithms from ECG | [158] |
| Wrist wearable EDR | RR, HRV, sleep studies | PPG 6 | Fitbit Charge, Power spectral density of HR, RMS 7 error = 0.648 min−1 | [166] |
| Mobile phone camera EDR | RR, HRV | Mobile phone camera | Incremental-Merge Segmentation algorithm, FFT 8, RMS error 3 ± 4.7 min−1 | [169] |
| EDR from ECG 6 | RR, HRV | ECG | Compared different techniques, Best error of 0.84 min−1 | [147] |
| EDR | RR, HRV | PPG dataset | Deep learning, MAE 9 2.5 ± 0.6 min−1 | [170] |
| Wrist wearable EDR | RR, HRV | PPG | 556 nm LED 10, Spectral kurtosis-based method, RMS error 1.2 ± 0.3 min−1, BLE 11 | [171] |
| Wrist wearable EDR | RR, HRV | PPG | CNN 12 algorithm, RR in the presence of high activity | [172] |
| Wrist wearable EDR | RR, HRV | PPG dataset | Different Machine learning, Sampling rate 500 Hz, MAE 1.91 min−1 | [173] |
| EDR | RR, HRV | PPG, ECG, accelerometer | Fusion algorithm, Probabilistic estimation for clinical practice | [174] |
| Arm, wrist, ankles EDR | RR, HRV | PPG | IR/green LEDs, 12 parameters, Data fusion model of 5 PPG features, Various postures | [175] |
| EDR | RR | Capnobase and PPG dataset | FFT analysis and peak detection, MAE 2.14 ± 5.59 min−1 and 1.59 ± 3.21 min−1 | [176] |
| Ring EDR | RR, HRV, sleep, BT 13, activity | PPG | Oura ring, BLE | [178] |
| Ring EDR | RR, HR, ECG, activity, BT | PPG | Galaxy ring, BLE, NFC 14 | [179] |
| Processor for wearable sensors | RR, HRV | EDR estimation | QRS detection with refractory period refreshing, Adaptive threshold, 55 nm technology, Estimation error 0.73, Power consumption 354 nW | [9] |
4. Acoustic-Based Methods
4.1. Electronic Stethoscopes
4.2. On-Body Microphones
4.3. Remote Microphones
| Sensor Type | Application | Sensing Element | Key Parameters | Ref. |
|---|---|---|---|---|
| Stand-alone stethoscope | Respiratory sound analysis | Digital stethoscope | 10 Hz–2 kHz, 100× amplification, Bluetooth for mobile phone connection, DSP 1, AI 2, Ambient noise cancelation, Real-time audio curve display, 150 g, 3.5 mm jack | [28] |
| Stethoscope connected to PC | Spectrogram classification | Own directional microphone | Directional microphone, Lubricated contact area, SVM 3 and CNN 4 algorithm, 3.5 mm jack | [190] |
| Wearable stethoscope | Advanced sound signal analysis | Soft and flexible wearable smart patch system | 36 Hz–2 kHz, SNR 5 14.8 dB, Real time abnormalities, 95% accuracy, Controlled motion artifact, BLE 6 | [191] |
| Stand-alone Stethoscope (Classic design) | Recording and data transmission | Digital stethoscope | 3–40 Hz, 40× amplification, Ambient noise cancelation, Sound signature spectrogram, Integrated HR, SpO2, BT and respiratory cycle, 48 h work time, Accuracy 92% | [192] |
| Body area network of stethoscopes | Advanced signal analysis | Body sensor area network | Strap or shirt option, SNR 48 dB, Integrated ECG monitor, BT, and body posture tracker | [193] |
| Body worn connected wireless to mobile phone | Asthmatic wheeze quantification | Digital MEMS microphone | ADMP441, I2C, Sensitivity −26 dBFS, Power consumption: 216–357 μW (signal streaming), 320–420 μW (classification on sensor), SNR 50–62 dB, Power 2520 μW at 1.8 V, Bluetooth | [198] |
| Body worn connected wireless to mobile phone | Asthmatic wheeze quantification | Electret condenser microphone | KEEG1542, Sensitivity −42 dB, Power consumption: 216–357 μW (signal streaming), 320–420 μW (classification on sensor), SNR 50–62 dB, Power 1000 μW @ 2.0 V, Bluetooth | [198] |
| Body worn connected wireless to mobile phone | Asthmatic wheeze quantification | Analog accelerometer | ADXL337, Sensitivity 300 mV/g, Power consumption: 216–357 μW (signal streaming), 320–420 μW (classification on sensor), SNR 50–62 dB, Power 900 μW @ 3.0 V, Bluetooth | [198] |
| Body worn connected wireless to mobile phone | Asthmatic wheeze quantification | Analog MEMS microphone | ADMP404, Sensitivity −38 dBV, Power consumption: 216–357 μW (signal streaming), 320–420 μW (classification on sensor), SNR 50–62 dB, Power 375 μW @ 1.5 V, Bluetooth | [198] |
| Body worn connected wireless to mobile phone | Asthmatic wheeze quantification | Digital accelerometer | ADXL345, SPI, Sensitivity 3.9 mg/LSB, Power consumption: 216–357 μW (signal streaming), 320–420 μW (classification on sensor), SNR 50–62 dB, Power 350 μW @ 2.5 V, Bluetooth | [198] |
| Body worn connected wireless to mobile phone | Asthmatic wheeze quantification | Analog MEMS microphone | ICS-40310, Sensitivity −37 dBV, Power consumption: 216–357 μW (signal streaming), 320-420 μW (classification on sensor), SNR 50–62 dB, Power 16 μW @ 1.0 V, Bluetooth | [198] |
| Body worn connected wireless to mobile phone | Asthma monitoring | Audio amplifier | MSP430 microcontroller, SPP, Orthogonal Matching Pursuit algorithm, Accuracy 80%, Bluetooth, 8 kb/s streaming | [195] |
| Body worn connected wireless to mobile phone | Asthmatic wheeze detection | Microphone or accelerometer | TMS320C5505, DSP, Accuracy 92% | [196] |
| Body worn connected to mobile phone using audio cable | Crackle sound detection | Electret microphone in plastic bell capsule | Microphone BT-2159000, Accuracy 84.68–89.16% | [199] |
| Body worn connected to mobile phone using audio cable | Tracheal sounds acquisition | Electret microphone | Microphone BT-21759000, 50–3000 Hz Correlation index for RR r2 = 0.97, | [200] |
| Neck-mounted connected to PC using audio cable | Breathing sounds | Microphone with aluminum conical bell | Microphone MD4530ASZ-1, 100–5000 Hz, Sensitivity −42 dB, Breathing detection accuracy 91.3% | [201] |
| Six wearable stethoscopes in vest | Diaphragm movement, sounds detection | Piezoelectric film in silicone rubber | ADC converter AD7988, Sampling rate 5 kHz, SPI | [203] |
| Chest worn microphone connected to PC using cable | Lung and heart sounds | Piezoelectric microphone | Ultrasensitive accelerometer, 9.2 V/g, 20–1000 Hz, LMP7721 amplifier, SNR 42–59 dB | [204] |
| Chest worn connected to PC or mobile phone | Activity recognition | Microphone | Activity identification accuracy 71.5% | [205] |
| Chest worn wireless connected to PC | Wheeze detector | Condenser microphone in stethoscope bell | TS-6022A, 500× amplification, 12-bit ADC–MSP430 processor, sampling rate 2 kHz, Bluetooth | [206] |
| Microphone fixed near nose connected wireless to mobile phone | Sleep RR detection, OSA 7 | Microphone | RR detecting accuracy 98.4%, OSA detecting accuracy 97.44% | [17] |
| Chest worn nanosensor | Mechano-acoustic cardiopulmonary signals | High-precision vibration sensor | Hermetically-sealed high-precision vibration sensor, Nano-gap transducers, 2 × 2 mm microsensor, 0.5 Hz–12 kHz, 10 μg–16 g, Sensitivity 76 mV/g | [208] |
| Clipped onto clothing wireless connected to mobile phone | Sound from nose/mouth, breathing | Microphone | Microphone, 3D accelerometer, Magnetometer, Barometer, Commercial, Bluetooth | [210] |
| Contact microphone on chest strap | HR, RR | Piezoelectric microphone | 20–200 Hz, L496ZG microcontroller, Power consumption 14.85 mW, HR Median percentage error 0.33% | [211] |
| Wireless thoracic and abdominal patch sensors with wireless communication to PC | Cough detection and RR | IMU and MEMS microphones | LSM9DSO IMU, ADMP401 MEMS microphone, SNR 62 dBA, MSP430 microcontroller, Power consumption 40–53.5 mW | [213] |
| Multiparameter cardiopulmonary acquisition device worn on shoulder | Breathing sound | Microphone in stethoscope bell | JL-0627C microphone, 12-bit, Bluetooth, Accuracy for RR 96.5%, Integrated ECG, SpO2 under motion 6-h working time | [213] |
| Multimodal chest sensors in vest | Bioimpedance tomography, RR, chest sounds | Electret microphones and chest impedance sensors | Integrated ECG, SpO2, Accelerometer, Bluetooth, 6-h working time, | [214] |
| Flexible wireless patch on upper torso | Detection of cough, RR, wheeze | Microphone and accelerometer | Integrated HR, BT, and activity level, Bluetooth | [217] |
| Textile pneumo vest with acoustic sensors | Lung function monitoring | Matrix of piezoceramic sensors | ML 8 algorithm | [218] |
| Soft skin-chest mounted wireless sensor | HR, RR, BT, and cough detection | Miniaturized mechanoacoustic motion sensors | LSMDSL IMU 9 sensor, Elastomer membrane, BLE, Immune to ambient noise, CNN network | [221] |
| Sound detection from distance | OSA | Mobil phone | iPhone 7 calibrated by oesophageal pressure manometry, ML algorithm, Prediction of ΔPes 10 with MAE 11 6.75 cm H2O, r = 0.83 | [222] |
| Mobile phone on the chest | OSA, snoring | Mobil phone | FFT 12 analysis, Online analysis on mobile phone, Snoring time correlation r = 0.93, Apnea-hypopnea index correlation r = 0.94, OSA sensitivity 0.7, OSA specificity 0.94 | [223] |
| Sound detection from distance | Asthmatic coughs and cough epochs | Mobil phone | CNN model, Gaussian mixture models, Matthew’s correlation coefficient 92%, Cough epochs count difference 0.24 | [224] |
| Mobile phone near mouth | Pediatric wheezing | Mobile phone | SVM algorithm, Sensitivity 71.4%, Specificity 88.9% | [225] |
| Mobile phone on the neck | RR | Mobile phone or headset | iPhone 4s–30 cm away from nose, PSD 13 calculation, Median error < 1% | [226] |
| IoT device in distance | Cough, breath, and wheeze analysis | Microphone | Embedded system, Renesas S5D9 120 MHz, Kernel-like minimum distance classifier, Accuracy up to 91.23% | [227] |
5. Parameters of Exhaled and Blood Gases
5.1. Composition of Breath Gases
5.2. Change in Breathing Gas Temperature, Humidity, and Pressure
5.3. Wearable Spirometry
5.4. Composition of Blood
| Sensor Type | Application | Sensing Element | Key Parameters | Ref. |
|---|---|---|---|---|
| Face mask | Detection of VOCs 1 | Chemiresistive MOS 2 sensor | Excellent stability, High response value, Low cost | [238] |
| Face mask | NH3 detection | Optical resistive sensor | High sensitivity, Fast response, Good environmental stability | [30] |
| Spirometry face mask | HR, Blood pressure, ECG, gas exchange, spirometry | Turbine-based NDIR CO2, fuel-cell-type O2 sensor, pressure sensor | Commercial mobile spiroergometry, Low weight, 6-h working time | [274] |
| Spirometry face mask | RR 3 and RV 4 | Turbine-based MEMS sensor | Insensitivity to ambient temperature, humidity, and gas content | [270] |
| Open-air headset for spirometry | RR and RV | Pressure, humidity, and temperature sensor | Compact size, 96% accuracy for face mask, 82% accuracy in open-air headset | [271] |
| Spirometry face-worn garments | RR, RV, FVC 5, IRV 6, ERV 7, IC 8 | Differential pressure sensor | Cheap version of sensing, Error margins for FVC 2–3% and for RV 1–3% | [272] |
| Spirometry mask with and earlobe type PPG | RR, RV, HR and SpO2, activity | Pressure sensor | Pressure, humidity, and temperature sensor BME280, IMU 9 for activity tracking | [273] |
| Face mask | RR, sleep apnea | Humidity sensor | Bluetooth connection | [32] |
| Face reusable respirators | RR, fit of the filter estimation, Contamination lvl | Pressure, temperature, relative humidity sensor | Protect workers from harmful dust, smoke, gases, and vapors | [245] |
| Nose sensing | RR, apnea and hypopnea | Pressure sensor | PPG, ACC, Microcontroller, Bluetooth | [265] |
| Sensor under the nostril and near the mouth | RR | Micro thermoelectric generators | Ultra-thin vertical structure-rapid heat conduction, Horizontal high-density integration-transient response and high fill speed, 28-pair microthermoelectric legs | [254] |
| Surgical mask | RR | Optical fiber | Thermally stable, Compact, Flexible, MRI conditions | [255] |
| Patch-like device | SpO2 | PPG | Emergency situations, Real-time monitoring | [277] |
| Ring | SpO2, HR, HRV | PPG | MAX30102, Error rates lower than 2.5% | [278] |
| Ear Monitor | RR, SpO2, HR, temperature | PPG | Bluetooth, MAX30100, TMP006 infrared sensor, analyzing respiratory sinus arrhythmia (RSA) | [281] |
| Watch | SpO2, HR | PPG | Bluetooth 4.0 | [284] |
| Transcutaneous sensing | Partial pressure CO2 monitoring | NDIR 10 sensor | Range 0–120 mmHg, Thermopile reading circuits | [288] |
| Transcutaneous sensing in wristband | Partial pressure CO2 monitoring | NDIR sensor | No need for skin heating, High accuracy, Long lifespan, Low-power consumption | [286] |
| Transcutaneous monitoring | PtcCO2 monitoring | Optical fluorescence thin film sensor | Range 0–75 mmHg | [290] |
| Transcutaneous sensor on a forearm | PtcCO2 monitoring | Optical fluorescence sensor | Highly sensitive in the CO2 range (0–50 mmHg), Insensitive to humidity | [31] |
| PPG sensor | Capnography measurement | Capno-base dataset | Deep neural network, Low cost, MSE 11 0.21, Cross-Correlation 0.946 | [291] |
6. Brief Summary
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Debnath, N.; Kumar, A.; Yadav, A.K. Probiotics as a Biotherapeutics for the Management and Prevention of Respiratory Tract Diseases. Microbiol. Immunol. 2022, 66, 277–291. [Google Scholar] [CrossRef]
- Momtazmanesh, S.; Moghaddam, S.S.; Ghamari, S.-H.; Rad, E.M.; Rezaei, N.; Shobeiri, P.; Aali, A.; Abbasi-Kangevari, M.; Abbasi-Kangevari, Z.; Abdelmasseh, M.; et al. Global Burden of Chronic Respiratory Diseases and Risk Factors, 1990–2019: An Update from the Global Burden of Disease Study 2019. eClinicalMedicine 2023, 59, 101936. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. Available online: https://vizhub.healthdata.org/ (accessed on 27 January 2024).
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, Regional, and National Causes of under-5 Mortality in 2000–2015: An Updated Systematic Analysis with Implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef]
- Troncoso, Á.; Ortega, J.A.; Seepold, R.; Madrid, N.M. Non-Invasive Devices for Respiratory Sound Monitoring. Procedia Comput. Sci. 2021, 192, 3040–3048. [Google Scholar] [CrossRef]
- Eurostat Respiratory Diseases Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php (accessed on 15 December 2023).
- Kozia, C.; Herzallah, R.; Lowe, D. ECG-Derived Respiration Using a Real-Time QRS Detector Based on Empirical Mode Decomposition. In Proceedings of the 2018, 12th International Conference on Signal Processing and Communication Systems (ICSPCS), Cairns, QLD, Australia, 17–19 December 2018; pp. 1–8. [Google Scholar]
- Lovett, P.B.; Buchwald, J.M.; Stürmann, K.; Bijur, P. The Vexatious Vital: Neither Clinical Measurements by Nurses nor an Electronic Monitor Provides Accurate Measurements of Respiratory Rate in Triage. Ann. Emerg. Med. 2005, 45, 68–76. [Google Scholar] [CrossRef]
- Fan, J.; Yang, S.; Liu, J.; Zhu, Z.; Xiao, J.; Chang, L.; Lin, S.; Zhou, J. A High Accuracy & Ultra-Low Power ECG-Derived Respiration Estimation Processor for Wearable Respiration Monitoring Sensor. Biosensors 2022, 12, 665. [Google Scholar] [CrossRef]
- Fieselmann, J.F.; Hendryx, M.S.; Helms, C.M.; Wakefield, D.S. Respiratory Rate Predicts Cardiopulmonary Arrest for Internal Medicine Inpatients. J. Gen. Intern. Med. 1993, 8, 354–360. [Google Scholar] [CrossRef]
- Subbe, C.P.; Davies, R.G.; Williams, E.; Rutherford, P.; Gemmell, L. Effect of Introducing the Modified Early Warning Score on Clinical Outcomes, Cardio-pulmonary Arrests and Intensive Care Utilisation in Acute Medical Admissions. Anaesthesia 2003, 58, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Goldhill, D.R.; McNarry, A.F.; Mandersloot, G.; McGinley, A. A Physiologically-based Early Warning Score for Ward Patients: The Association between Score and Outcome. Anaesthesia 2005, 60, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Cretikos, M.; Chen, J.; Hillman, K.; Bellomo, R.; Finfer, S.; Flabouris, A. The Objective Medical Emergency Team Activation Criteria: A Case–Control Study. Resuscitation 2007, 73, 62–72. [Google Scholar] [CrossRef] [PubMed]
- AL-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H.; Tan, S. Respiration Rate Monitoring Methods: A Review. Pediatr. Pulmonol. 2011, 46, 523–529. [Google Scholar] [CrossRef]
- Daiana da Costa, T.; de Fatima Fernandes Vara, M.; Santos Cristino, C.; Zoraski Zanella, T.; Nunes Nogueira Neto, G.; Nohama, P. Breathing Monitoring and Pattern Recognition with Wearable Sensors. In Wearable Devices—The Big Wave of Innovation; IntechOpen: London, UK, 2019. [Google Scholar]
- Dieffenderfer, J.; Goodell, H.; Mills, S.; McKnight, M.; Yao, S.; Lin, F.; Beppler, E.; Bent, B.; Lee, B.; Misra, V.; et al. Low-Power Wearable Systems for Continuous Monitoring of Environment and Health for Chronic Respiratory Disease. IEEE J. Biomed. Health Inform. 2016, 20, 1251–1264. [Google Scholar] [CrossRef]
- Fang, Y.; Jiang, Z.; Wang, H. A Novel Sleep Respiratory Rate Detection Method for Obstructive Sleep Apnea Based on Characteristic Moment Waveform. J. Health Eng. 2018, 2018, 1902176. [Google Scholar] [CrossRef]
- Molinaro, N.; Massaroni, C.; Lo Presti, D.; Saccomandi, P.; Di Tomaso, G.; Zollo, L.; Perego, P.; Andreoni, G.; Schena, E. Wearable Textile Based on Silver Plated Knitted Sensor for Respiratory Rate Monitoring. In Proceedings of the 2018, 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; pp. 2865–2868. [Google Scholar]
- Escobar-Linero, E.; Muñoz-Saavedra, L.; Luna-Perejón, F.; Sevillano, J.L.; Domínguez-Morales, M. Wearable Health Devices for Diagnosis Support: Evolution and Future Tendencies. Sensors 2023, 23, 1678. [Google Scholar] [CrossRef]
- Resmetrix Medical Building a Personalized Breathing Analytics Platform. Available online: www.resmetrix-medical.com (accessed on 19 December 2023).
- SpireHealth SpireHealth Technology. Available online: https://www.spirehealth.com/ (accessed on 19 December 2023).
- Witt, J.; Narbonneau, F.; Schukar, M.; Krebber, K.; De Jonckheere, J.; Jeanne, M.; Kinet, D.; Paquet, B.; Depre, A.; D’Angelo, L.T.; et al. Medical Textiles With Embedded Fiber Optic Sensors for Monitoring of Respiratory Movement. IEEE Sens. J. 2012, 12, 246–254. [Google Scholar] [CrossRef]
- Andreozzi, E.; Centracchio, J.; Punzo, V.; Esposito, D.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Respiration Monitoring via Forcecardiography Sensors. Sensors 2021, 21, 3996. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Arafa, H.M.; Yoo, J.-Y.; Kantarcigil, C.; Kim, J.-T.; Jeong, H.; Yoo, S.; Oh, S.; Kim, J.; Wu, C.; et al. Soft Skin-Interfaced Mechano-Acoustic Sensors for Real-Time Monitoring and Patient Feedback on Respiratory and Swallowing Biomechanics. npj Digit. Med. 2022, 5, 147. [Google Scholar] [CrossRef] [PubMed]
- Sleep Gadgets Interview: Somnofy Sleep Assistant w/ Alf-Egil Bogen. Available online: https://sleepgadgets.io/interview-somnofy-sleep-assistant/ (accessed on 19 December 2023).
- Hu, M.-H.; Zhai, G.-T.; Li, D.; Fan, Y.-Z.; Chen, X.-H.; Yang, X.-K. Synergetic Use of Thermal and Visible Imaging Techniques for Contactless and Unobtrusive Breathing Measurement. J. Biomed. Opt. 2017, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Svobodova, H.; Vavrinsky, E.; Turonova, D.; Donoval, M.; Daricek, M.; Telek, P.; Kopani, M. Optimization of the Position of Single-Lead Wireless Sensor with Low Electrodes Separation Distance for ECG-Derived Respiration. Adv. Electr. Electron. Eng. 2018, 16, 528–537. [Google Scholar] [CrossRef]
- Minttihealth Digital Stethoscope Mintti Smartho-D2. Available online: https://minttihealth.com/product/digital-stethoscope-mintti-smartho-d2 (accessed on 20 December 2023).
- George, U.Z.; Moon, K.S.; Lee, S.Q. Extraction and Analysis of Respiratory Motion Using a Comprehensive Wearable Health Monitoring System. Sensors 2021, 21, 1393. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Chen, J.; Liu, Y.; Li, B.; Li, H.; Zhang, X.; Lv, C.; Dong, H. Wearable Dual-Signal NH 3 Sensor with High Sensitivity for Non-Invasive Diagnosis of Chronic Kidney Disease. Langmuir 2023, 39, 3420–3430. [Google Scholar] [CrossRef] [PubMed]
- Cascales, J.P.; Li, X.; Roussakis, E.; Evans, C.L. A Patient-Ready Wearable Transcutaneous CO2 Sensor. Biosensors 2022, 12, 333. [Google Scholar] [CrossRef] [PubMed]
- Honda, S.; Hara, H.; Arie, T.; Akita, S.; Takei, K. A Wearable, Flexible Sensor for Real-Time, Home Monitoring of Sleep Apnea. iScience 2022, 25, 104163. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kantharaju, P.; Yi, H.; Jacobson, M.; Jeong, H.; Kim, H.; Lee, J.; Matthews, J.; Zavanelli, N.; Kim, H.; et al. Soft Wearable Flexible Bioelectronics Integrated with an Ankle-Foot Exoskeleton for Estimation of Metabolic Costs and Physical Effort. npj Flex. Electron. 2023, 7, 3. [Google Scholar] [CrossRef]
- Li, C.; Xu, Z.; Xu, S.; Wang, T.; Zhou, S.; Sun, Z.; Wang, Z.L.; Tang, W. Miniaturized Retractable Thin-Film Sensor for Wearable Multifunctional Respiratory Monitoring. Nano Res. 2023, 16, 11846–11854. [Google Scholar] [CrossRef]
- Antonelli, A.; Guilizzoni, D.; Angelucci, A.; Melloni, G.; Mazza, F.; Stanzi, A.; Venturino, M.; Kuller, D.; Aliverti, A. Comparison between the AirgoTM Device and a Metabolic Cart during Rest and Exercise. Sensors 2020, 20, 3943. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.; Nguyen, T.; Pandey, V.; Zhou, Y.; Pham, H.N.; Bar-Yoseph, R.; Radom-Aizik, S.; Jain, R.; Cooper, D.M.; Khine, M. Respiration Rate and Volume Measurements Using Wearable Strain Sensors. npj Digit. Med. 2019, 2, 8. [Google Scholar] [CrossRef]
- Yuan, Y.; Chen, H.; Xu, H.; Jin, Y.; Chen, G.; Zheng, W.; Wang, W.; Wang, Y.; Gao, L. Highly Sensitive and Wearable Bionic Piezoelectric Sensor for Human Respiratory Monitoring. Sens. Actuators A Phys. 2022, 345, 113818. [Google Scholar] [CrossRef]
- Lei, K.-F.; Hsieh, Y.-Z.; Chiu, Y.-Y.; Wu, M.-H. The Structure Design of Piezoelectric Poly(Vinylidene Fluoride) (PVDF) Polymer-Based Sensor Patch for the Respiration Monitoring under Dynamic Walking Conditions. Sensors 2015, 15, 18801–18812. [Google Scholar] [CrossRef]
- Wu, D.; Wang, L.; Zhang, Y.-T.; Huang, B.-Y.; Wang, B.; Lin, S.-J.; Xu, X.-W. A Wearable Respiration Monitoring System Based on Digital Respiratory Inductive Plethysmography. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 4844–4847. [Google Scholar]
- Monaco, V.; Stefanini, C. Assessing the Tidal Volume through Wearables: A Scoping Review. Sensors 2021, 21, 4124. [Google Scholar] [CrossRef]
- Whitlock, J.; Sill, J.; Jain, S. A-Spiro: Towards Continuous Respiration Monitoring. Smart Health 2020, 15, 100105. [Google Scholar] [CrossRef]
- Enokibori, Y.; Suzuki, A.; Mizuno, H.; Shimakami, Y.; Kawabe, T.; Mase, K. An E-Textile-Based Wearable Spirometer and Its Adaptability for Context Changes Depending on Sweat and Meal. In Proceedings of the MHS2013, Nagoya, Japan, 10–13 November 2013; pp. 1–5. [Google Scholar]
- Park, S.W.; Das, P.S.; Chhetry, A.; Park, J.Y. A Flexible Capacitive Pressure Sensor for Wearable Respiration Monitoring System. IEEE Sens. J. 2017, 17, 6558–6564. [Google Scholar] [CrossRef]
- FIERCE Biotech, Spire Health Launches COPD Study with Its Machine-Washable Wearable. Available online: www.fiercebiotech.com/medtech/spire-health-launches-copd-tracking-study-its-machine-washable-wearable (accessed on 19 December 2023).
- Fourth Frontier, FRONTIER X2: World’s First Smart Heart Monitor. Available online: https://uk.fourthfrontier.com/products/frontier-x (accessed on 19 December 2023).
- Wagih, M.; Malik, O.; Weddell, A.S.; Beeby, S. E-Textile Breathing Sensor Using Fully Textile Wearable Antennas. In Proceedings of the E-Textiles 2021, Manchester, UK, 3–4 November 2021; p. 9. [Google Scholar]
- Bozhenko, B.S. Seismocardiography—A New Method in the Study of Functional Conditions of the Heart. Ter. Arkh. 1961, 33, 55–64. [Google Scholar] [PubMed]
- Marco, T. De Novel Wearable Seismocardiography and Clinical Status of Heart Failure Patients. Circ Heart Fail. 2018, 11, e004313. [Google Scholar] [CrossRef]
- Tadi, M.J.; Lehtonen, E.; Hurnanen, T.; Koskinen, J.; Eriksson, J.; Pänkäälä, M.; Teräs, M.; Koivisto, T. A Real-Time Approach for Heart Rate Monitoring Using a Hilbert Transform in Seismocardiograms. Physiol. Meas. 2016, 37, 1885–1909. [Google Scholar] [CrossRef] [PubMed]
- Tadi, M.J.; Lehtonen, E.; Koivisto, T.; Pankaala, M.; Paasio, A.; Teras, M. Seismocardiography: Toward Heart Rate Variability (HRV) Estimation. In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA) Proceedings, Turin, Italy, 7–9 May 2015; pp. 261–266. [Google Scholar]
- Taebi, A.; Solar, B.; Bomar, A.; Sandler, R.; Mansy, H. Recent Advances in Seismocardiography. Vibration 2019, 2, 64–86. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.; Whang, M. An Enhanced Method to Estimate Heart Rate from Seismocardiography via Ensemble Averaging of Body Movements at Six Degrees of Freedom. Sensors 2018, 18, 238. [Google Scholar] [CrossRef] [PubMed]
- Inan, O.T.; Migeotte, P.-F.; Park, K.-S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Informatics 2015, 19, 1414–1427. [Google Scholar] [CrossRef]
- Vavrinsky, E.; Subjak, J.; Donoval, M.; Wagner, A.; Zavodnik, T.; Svobodova, H. Application of Modern Multi-Sensor Holter in Diagnosis and Treatment. Sensors 2020, 20, 2663. [Google Scholar] [CrossRef]
- Di Rienzo, M.; Vaini, E.; Castiglioni, P.; Merati, G.; Meriggi, P.; Parati, G.; Faini, A.; Rizzo, F. Wearable Seismocardiography: Towards a Beat-by-Beat Assessment of Cardiac Mechanics in Ambulant Subjects. Auton. Neurosci. 2013, 178, 50–59. [Google Scholar] [CrossRef]
- Pandia, K.; Inan, O.T.; Kovacs, G.T.A.; Giovangrandi, L. Extracting Respiratory Information from Seismocardiogram Signals Acquired on the Chest Using a Miniature Accelerometer. Physiol. Meas. 2012, 33, 1643–1660. [Google Scholar] [CrossRef]
- Han, D.K.; Hong, J.H.; Shin, J.Y.; Lee, T.S. Accelerometer Based Motion Noise Analysis of ECG Signal. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Munich, Germany, 7–12 September 2009; pp. 198–201. [Google Scholar]
- Marcelli, E.; Capucci, A.; Minardi, G.; Cercenelli, L. Multi-Sense CardioPatch: A Wearable Patch for Remote Monitoring of Electro-Mechanical Cardiac Activity. ASAIO J. 2017, 63, 73–79. [Google Scholar] [CrossRef]
- Yu, S.; Liu, S. A Novel Adaptive Recursive Least Squares Filter to Remove the Motion Artifact in Seismocardiography. Sensors 2020, 20, 1596. [Google Scholar] [CrossRef]
- Taebi, A.; Mansy, H.A. Time-Frequency Distribution of Seismocardiographic Signals: A Comparative Study. Bioengineering 2017, 4, 32. [Google Scholar] [CrossRef] [PubMed]
- Luu, L.; Dinh, A. Artifact Noise Removal Techniques on Seismocardiogram Using Two Tri-Axial Accelerometers. Sensors 2018, 18, 1067. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.W. Certain Molar Movements of the Human Body Produced by the Circulation of the Blood. J. Anat. Physiol. 1877, 11, 533–536. [Google Scholar] [PubMed]
- Henderson, Y. The Mass-Movements of the Circulation as Shown by a Recoil Curve. Am. J. Physiol. Content 1905, 14, 287–298. [Google Scholar] [CrossRef]
- Heald, C.B.; Tucker, W.S. Recoil Curves as Shown by the Hot-Wire Microphone. Proc. R. Soc. London. Ser. B Contain. Pap. Biol. Character 1922, 93, 281–298. [Google Scholar] [CrossRef]
- Starr, I.; Krumbhaar, E.B. The Ballistocardiograph: An Instrument for Clinical Research and for Routine Clinical Diagnosis; Harvey Lec.: London, UK, 1947. [Google Scholar]
- Rubenstein, E. A Review of Clinical Ballistocardiography. N. Engl. J. Med. 1952, 247, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Balali, P.; Rabineau, J.; Hossein, A.; Tordeur, C.; Debeir, O.; van de Borne, P. Investigating Cardiorespiratory Interaction Using Ballistocardiography and Seismocardiography—A Narrative Review. Sensors 2022, 22, 9565. [Google Scholar] [CrossRef] [PubMed]
- Klum, M.; Urban, M.; Tigges, T.; Pielmus, A.-G.; Feldheiser, A.; Schmitt, T.; Orglmeister, R. Wearable Cardiorespiratory Monitoring Employing a Multimodal Digital Patch Stethoscope: Estimation of ECG, PEP, LVET and Respiration Using a 55 Mm Single-Lead ECG and Phonocardiogram. Sensors 2020, 20, 2033. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Wu, X.; Wang, J.; Li, H.; Cao, K.; Cao, H.; Zhong, K.; Yang, X. The Latest Progress and Development Trend in the Research of Ballistocardiography (BCG) and Seismocardiogram (SCG) in the Field of Health Care. Appl. Sci. 2021, 11, 8896. [Google Scholar] [CrossRef]
- Fisher, J.P.; Zera, T.; Paton, J.F.R. Respiratory–Cardiovascular Interactions. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2022; Volume 188, pp. 279–308. [Google Scholar]
- Wise, R.A.; Robotham, J.L.; Summer, W.R. Effects of Spontaneous Ventilation on the Circulation. Lung 1981, 159, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Magder, S. Heart-Lung Interaction in Spontaneous Breathing Subjects: The Basics. Ann. Transl. Med. 2018, 6, 348. [Google Scholar] [CrossRef]
- Feihl, F.; Broccard, A.F. Interactions between Respiration and Systemic Hemodynamics. Part I: Basic Concepts. Intensive Care Med. 2009, 35, 45–54. [Google Scholar] [CrossRef]
- Di Rienzo, M.; Meriggi, P.; Rizzo, F.; Vaini, E.; Faini, A.; Merati, G.; Parati, G.; Castiglioni, P. A Wearable System for the Seismocardiogram Assessment in Daily Life Conditions. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 4263–4266. [Google Scholar]
- Tadi, M.J.; Koivisto, T.; Pänkäälä, M.; Paasio, A. Accelerometer-Based Method for Extracting Respiratory and Cardiac Gating Information for Dual Gating during Nuclear Medicine Imaging. Int. J. Biomed. Imaging 2014, 2014, 690124. [Google Scholar] [CrossRef]
- Ceccarelli, M.; Taje, R.; Papuc, P.E.; Ambrogi, V. An Analysis of Respiration with the Smart Sensor SENSIRIB in Patients Undergoing Thoracic Surgery. Sensors 2022, 22, 1561. [Google Scholar] [CrossRef]
- iBreve The IBreve Wearable. Available online: https://www.ibreve.com (accessed on 19 December 2023).
- Oxa Oxa: The First Breathing Wearable. Available online: https://www.kickstarter.com/projects/1816762999/oxa-learn-to-reconnect-your-mind-and-body-using-breathwork (accessed on 19 December 2023).
- Sadat-Mohammadi, M.; Shakerian, S.; Liu, Y.; Asadi, S.; Jebelli, H. Non-Invasive Physical Demand Assessment Using Wearable Respiration Sensor and Random Forest Classifier. J. Build. Eng. 2021, 44, 103279. [Google Scholar] [CrossRef]
- Tavakolian, K.; Vaseghi, A.; Kaminska, B. Improvement of Ballistocardiogram Processing by Inclusion of Respiration Information. Physiol. Meas. 2008, 29, 771–781. [Google Scholar] [CrossRef]
- Biopac Systems. Available online: www.biopac.com (accessed on 19 December 2023).
- Pandia, K.; Inan, O.T.; Kovacs, G.T.A. A Frequency Domain Analysis of Respiratory Variations in the Seismocardiogram Signal. In Proceedings of the 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 6881–6884. [Google Scholar]
- Da He, D.; Winokur, E.S.; Heldt, T.; Sodini, C.G. The Ear as a Location for Wearable Vital Signs Monitoring. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 6389–6392. [Google Scholar]
- Morra, S.; Gauthey, A.; Hossein, A.; Rabineau, J.; Racape, J.; Gorlier, D.; Migeotte, P.-F.; le Polain de Waroux, J.B.; van de Borne, P. Influence of Sympathetic Activation on Myocardial Contractility Measured with Ballistocardiography and Seismocardiography during Sustained End-Expiratory Apnea. Am. J. Physiol. Integr. Comp. Physiol. 2020, 319, R497–R506. [Google Scholar] [CrossRef]
- Morra, S.; Hossein, A.; Gorlier, D.; Rabineau, J.; Chaumont, M.; Migeotte, P.-F.; Van De Borne, P. Ballistocardiography and Seismocardiography Detection of Hemodynamic Changes during Simulated Obstructive Apnea. Physiol. Meas. 2020, 41, 065007. [Google Scholar] [CrossRef]
- Emfit, QS. Available online: https://emfit.com/heart-rate-variability-hrv-during-sleep/ (accessed on 19 December 2023).
- Vehkaoja, A.; Kontunen, A.; Lekkala, J. Effects of Sensor Type and Sensor Location on Signal Quality in Bed Mounted Ballistocardiographic Heart Rate and Respiration Monitoring. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4383–4386. [Google Scholar]
- Bruser, C.; Kerekes, A.; Winter, S.; Leonhardt, S. Multi-Channel Optical Sensor-Array for Measuring Ballistocardiograms and Respiratory Activity in Bed. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 5042–5045. [Google Scholar]
- Korhonen, I.; Iivainen, T.; Lappalainen, R.; Tuomisto, T.; Kööbi, T.; Pentikäinen, V.; Tuomisto, M.; Turjanmaa, V. TERVA: System for Long-Term Monitoring of Wellness at Home. Telemed. J. e-Health 2001, 7, 61–72. [Google Scholar] [CrossRef]
- Alihanka, J.; Vaahtoranta, K.; Saarikivi, I. A New Method for Long-Term Monitoring of the Ballistocardiogram, Heart Rate, and Respiration. Am. J. Physiol. Integr. Comp. Physiol. 1981, 240, R384–R392. [Google Scholar] [CrossRef]
- Albukhari, A.; Lima, F.; Mescheder, U. Bed-Embedded Heart and Respiration Rates Detection by Longitudinal Ballistocardiography and Pattern Recognition. Sensors 2019, 19, 1451. [Google Scholar] [CrossRef]
- Mack, D.C.; Patrie, J.T.; Suratt, P.M.; Felder, R.A.; Alwan, M. Development and Preliminary Validation of Heart Rate and Breathing Rate Detection Using a Passive, Ballistocardiography-Based Sleep Monitoring System. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 111–120. [Google Scholar] [CrossRef]
- Zhao, W.; Ni, H.; Zhou, X.; Song, Y.; Wang, T. Identifying Sleep Apnea Syndrome Using Heart Rate and Breathing Effort Variation Analysis Based on Ballistocardiography. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4536–4539. [Google Scholar]
- Lee, W.; Yoon, H.; Han, C.; Joo, K.; Park, K. Physiological Signal Monitoring Bed for Infants Based on Load-Cell Sensors. Sensors 2016, 16, 409. [Google Scholar] [CrossRef] [PubMed]
- Cimr, D.; Studnicka, F.; Fujita, H.; Cimler, R.; Slegr, J. Application of Mechanical Trigger for Unobtrusive Detection of Respiratory Disorders from Body Recoil Micro-Movements. Comput. Methods Programs Biomed. 2021, 207, 106149. [Google Scholar] [CrossRef]
- Martín-Yebra, A.; Landreani, F.; Casellato, C.; Pavan, E.; Migeotte, P.-F.; Frigo, C.; Martínez, J.P.; Caiani, E.G. Evaluation of Respiratory- and Postural-Induced Changes on the Ballistocardiogram Signal by Time Warping Averaging. Physiol. Meas. 2017, 38, 1426–1440. [Google Scholar] [CrossRef]
- Vavrinsky, E.; Solarikova, P.; Stopjakova, V.; Tvarozek, V.; Brezi, I. Implementation of Microsensor Interface for Biomonitoring of Human Cognitive Processes. In Biomedical Engineering, Trends in Electronics, Communications and Software; IntechOpen: London, UK, 2011. [Google Scholar]
- Järvelä, K.; Takala, P.; Michard, F.; Vikatmaa, L. Clinical Evaluation of a Wearable Sensor for Mobile Monitoring of Respiratory Rate on Hospital Wards. J. Clin. Monit. Comput. 2022, 36, 81–86. [Google Scholar] [CrossRef]
- Fedotov, A.A.; Akulov, S.A.; Akulova, A.S. Motion Artifacts Reduction in Wearable Respiratory Monitoring Device. In Proceedings of the EMBEC & NBC 2017: Joint Conference of the European Medical and Biological Engineering Conference (EMBEC) and the Nordic-Baltic Conference on Biomedical Engineering and Medical Physics (NBC), Tampere, Finland, 13 June 2018; pp. 1121–1124. [Google Scholar]
- Khan, H.A.; Gore, A.; Ashe, J.; Chakrabartty, S. Virtual Spirometry and Activity Monitoring Using Multichannel Electrical Impedance Plethysmographs in Ambulatory Settings. IEEE Trans. Biomed. Circuits Syst. 2017, 11, 832–848. [Google Scholar] [CrossRef] [PubMed]
- Texas Instruments, Texas Instruments ADS129xR 24-Bit Analog Front-End Devices. Available online: https://www.mouser.sk/new/texas-instruments/tiads129xr (accessed on 19 December 2023).
- Texas Instruments Two-Channel ECG Analog Front End with Integrated Respiration and Pace Detection. Available online: https://www.ti.com/product/AFE4960 (accessed on 19 December 2023).
- Texas Instruments AFE4500 Integrated Analog Front End (AFE) for Bioimpedance Analysis and Electrical and Optical Biosensing. Available online: https://www.ti.com/product/AFE4500 (accessed on 19 December 2023).
- Analog Devices ADAS1000 Low Power, 5-Electrode Electrocardiogram (ECG) Analog Front End with Respiration Measurement and Pace Detection. Available online: www.analog.com/en/products/adas1000.html#product-overview (accessed on 19 December 2023).
- Analog Devices MAX30001 Ultra-Low-Power, Single-Channel Integrated Biopotential (ECG, R-to-R, and Pace Detection) and Bioimpedance (BioZ) AFE. Available online: www.analog.com/en/products/max30001.html#product-overview (accessed on 19 December 2023).
- OSRAM Ams, AS7058 High Performance Vital Sign—Analog Frontend. Available online: https://ams-osram.com/products/interfaces/analog-frontend/ams-as7058-high-performance-vital-sign-analog-frontend (accessed on 19 December 2023).
- Lo Presti, D.; Massaroni, C.; D’Abbraccio, J.; Massari, L.; Caponero, M.; Longo, U.G.; Formica, D.; Oddo, C.M.; Schena, E. Wearable System Based on Flexible FBG for Respiratory and Cardiac Monitoring. IEEE Sens. J. 2019, 19, 7391–7398. [Google Scholar] [CrossRef]
- Chethana, K.; Guru Prasad, A.S.; Omkar, S.N.; Asokan, S. Fiber Bragg Grating Sensor Based Device for Simultaneous Measurement of Respiratory and Cardiac Activities. J. Biophotonics 2017, 10, 278–285. [Google Scholar] [CrossRef]
- Nedoma, J.; Kepak, S.; Fajkus, M.; Cubik, J.; Siska, P.; Martinek, R.; Krupa, P. Magnetic Resonance Imaging Compatible Non-Invasive Fibre-Optic Sensors Based on the Bragg Gratings and Interferometers in the Application of Monitoring Heart and Respiration Rate of the Human Body: A Comparative Study. Sensors 2018, 18, 3713. [Google Scholar] [CrossRef]
- Nedoma, J.; Fajkus, M.; Martinek, R.; Nazeran, H. Vital Sign Monitoring and Cardiac Triggering at 1.5 Tesla: A Practical Solution by an MR-Ballistocardiography Fiber-Optic Sensor. Sensors 2019, 19, 470. [Google Scholar] [CrossRef]
- Zhao, C.; Liu, D.; Xu, G.; Zhou, J.; Zhang, X.; Liao, C.; Wang, Y. Recent Advances in Fiber Optic Sensors for Respiratory Monitoring. Opt. Fiber Technol. 2022, 72, 103000. [Google Scholar] [CrossRef]
- Issatayeva, A.; Beisenova, A.; Tosi, D.; Molardi, C. Fiber-Optic Based Smart Textiles for Real-Time Monitoring of Breathing Rate. Sensors 2020, 20, 3408. [Google Scholar] [CrossRef]
- Yang, X.; Chen, Z.; Elvin, C.S.M.; Janice, L.H.Y.; Ng, S.H.; Teo, J.T.; Wu, R. Textile Fiber Optic Microbend Sensor Used for Heartbeat and Respiration Monitoring. IEEE Sens. J. 2015, 15, 757–761. [Google Scholar] [CrossRef]
- De Tommasi, F.; Lo Presti, D.; Caponero, M.A.; Carassiti, M.; Schena, E.; Massaroni, C. Smart Mattress Based on Multipoint Fiber Bragg Gratings for Respiratory Rate Monitoring. IEEE Trans. Instrum. Meas. 2023, 72, 4000710. [Google Scholar] [CrossRef]
- Li, L.; Yang, C.; Wang, Z.; Xiao, K.; Min, R. Stretchable Polymer Optical Fiber Embedded in the Mattress for Respiratory and Heart Rate Monitoring. Opt. Laser Technol. 2024, 171, 110356. [Google Scholar] [CrossRef]
- Ciocchetti, M.; Massaroni, C.; Saccomandi, P.; Caponero, M.A.; Polimadei, A.; Formica, D.; Schena, E. Smart Textile Based on Fiber Bragg Grating Sensors for Respiratory Monitoring: Design and Preliminary Trials. Biosensors 2015, 5, 602–615. [Google Scholar] [CrossRef] [PubMed]
- De Jonckheere, J.; Jeanne, M.; Grillet, A.; Weber, S.; Chaud, P.; Logier, R.; Weber, J. OFSETH: Optical Fibre Embedded into Technical Textile for Healthcare, an Efficient Way to Monitor Patient under Magnetic Resonance Imaging. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 3950–3953. [Google Scholar]
- Bennett, A.; Beiderman, Y.; Agdarov, S.; Beiderman, Y.; Hendel, R.; Straussman, B.; Zalevsky, Z. Monitoring of Vital Bio-Signs by Multimode Speckle Based Optical Fiber Sensor. Opt. Express 2020, 28, 20830–20844. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Lau, D.; Teo, J.T.; Ng, S.H.; Yang, X.; Kei, P.L. Simultaneous Measurement of Breathing Rate and Heart Rate Using a Microbend Multimode Fiber Optic Sensor. J. Biomed. Opt. 2014, 19, 057001. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Teo, J.T.; Ng, S.H.; Yang, X. Plastic Optical Fiber Microbend Sensor Used as Breathing Sensor. In Proceedings of the 2012 IEEE Sensors, Taipei, Taiwan, 28–31 October 2012; pp. 1–4. [Google Scholar]
- Zha, B.; Wang, Z.; Li, L.; Hu, X.; Ortega, B.; Li, X.; Min, R. Wearable Cardiorespiratory Monitoring with Stretchable Elastomer Optical Fiber. Biomed. Opt. Express 2023, 14, 2260. [Google Scholar] [CrossRef] [PubMed]
- Ben Nasr, M.C.; Ben Jebara, S.; Otis, S.; Abdulrazak, B.; Mezghani, N. A Spectral-Based Approach for BCG Signal Content Classification. Sensors 2021, 21, 1020. [Google Scholar] [CrossRef] [PubMed]
- Yoo, W.-J.; Jang, K.-W.; Seo, J.-K.; Heo, J.-Y.; Moon, J.-S.; Park, J.-Y.; Lee, B.-S. Development of Respiration Sensors Using Plastic Optical Fiber for Respiratory Monitoring Inside MRI System. J. Opt. Soc. Korea 2010, 14, 235–239. [Google Scholar] [CrossRef]
- Bilro, L.; Alberto, N.; Pinto, J.L.; Nogueira, R. Optical Sensors Based on Plastic Fibers. Sensors 2012, 12, 12184–12207. [Google Scholar] [CrossRef]
- Krehel, M.; Schmid, M.; Rossi, R.; Boesel, L.; Bona, G.-L.; Scherer, L. An Optical Fibre-Based Sensor for Respiratory Monitoring. Sensors 2014, 14, 13088–13101. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.L.; Liu, B.; Pang, Y.N.; Liu, J.; Shi, J.L.; Wan, S.P.; He, X.D.; Yuan, J.; Wu, Q. Low-Cost Wearable Sensor Based on a D-Shaped Plastic Optical Fiber for Respiration Monitoring. IEEE Trans. Instrum. Meas. 2021, 70, 4004808. [Google Scholar] [CrossRef]
- Han, P.; Li, L.; Zhang, H.; Guan, L.; Marques, C.; Savović, S.; Ortega, B.; Min, R.; Li, X. Low-Cost Plastic Optical Fiber Sensor Embedded in Mattress for Sleep Performance Monitoring. Opt. Fiber Technol. 2021, 64, 102541. [Google Scholar] [CrossRef]
- Sartiano, D.; Sales, S. Low Cost Plastic Optical Fiber Pressure Sensor Embedded in Mattress for Vital Signal Monitoring. Sensors 2017, 17, 2900. [Google Scholar] [CrossRef]
- Xu, J.; Li, T.; Li, Y.; Zhang, C.; Cheng, L.; Liu, L.; Miao, C. Fabrication and Application of a Grooved Optical Fiber Respiratory Sensor Based on Geometric Parameter Optimization by Optical Simulation. Opt. Laser Technol. 2023, 167, 109747. [Google Scholar] [CrossRef]
- Greneker, E.F. Radar Sensing of Heartbeat and Respiration at a Distance with Applications of the Technology. In Proceedings of the Radar Systems (RADAR 97), Edinburgh, UK, 14–16 October 1997; Volume 1997, pp. 150–154. [Google Scholar]
- Kukkapalli, R.; Banerjee, N.; Robucci, R.; Kostov, Y. Micro-Radar Wearable Respiration Monitor. In Proceedings of the 2016 IEEE SENSORS, Orlando, FL, USA, 30 October–3 November 2016; pp. 1–3. [Google Scholar]
- Xia, Z.; Shandhi, M.M.H.; Li, Y.; Inan, O.T.; Zhang, Y. The Delineation of Fiducial Points for Non-Contact Radar Seismocardiogram Signals Without Concurrent ECG. IEEE J. Biomed. Health Inform. 2021, 25, 1031–1040. [Google Scholar] [CrossRef]
- Lu, G.; Wang, J.; Yue, Y.; Jing, X. Study of the Ballistocardiogram Signal in Life Detection System Based on Radar. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 2191–2194. [Google Scholar]
- Sharma, P.; Hui, X.; Zhou, J.; Conroy, T.B.; Kan, E.C. Wearable Radio-Frequency Sensing of Respiratory Rate, Respiratory Volume, and Heart Rate. npj Digit. Med. 2020, 3, 98. [Google Scholar] [CrossRef]
- Chen, M.; Zhu, Q.; Zhang, H.; Wu, M.; Wang, Q. Respiratory Rate Estimation from Face Videos. In Proceedings of the 2019 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Chicago, IL, USA, 19–22 May 2019; pp. 1–4. [Google Scholar]
- Stubbe, L.; Houel, N.; Cottin, F. Accuracy and Reliability of the Optoelectronic Plethysmography and the Heart Rate Systems for Measuring Breathing Rates Compared with the Spirometer. Sci. Rep. 2022, 12, 19255. [Google Scholar] [CrossRef]
- Zhu, Z.; Fei, J.; Pavlidis, I. Tracking Human Breath in Infrared Imaging. In Proceedings of the Fifth IEEE Symposium on Bioinformatics and Bioengineering (BIBE’05), Minneapolis, MN, USA, 19–21 October 2005; pp. 227–231. [Google Scholar]
- Chekmenev, S.Y.; Rara, H.M.; Farag, A. Non-Contact, Wavelet-Based Measurement of Vital Signs Using Thermal Imaging; University of Louisville: Louisville, KY, USA, 2005. [Google Scholar]
- Procházka, A.; Charvátová, H.; Vyšata, O.; Kopal, J.; Chambers, J. Breathing Analysis Using Thermal and Depth Imaging Camera Video Records. Sensors 2017, 17, 1408. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, K.; Rabell, J.E.; Martin del Olmo, P.; Haesler, S. IR Thermography-Based Monitoring of Respiration Phase without Image Segmentation. J. Neurosci. Methods 2018, 301, 1–8. [Google Scholar] [CrossRef]
- Lewis, G.F.; Gatto, R.G.; Porges, S.W. A Novel Method for Extracting Respiration Rate and Relative Tidal Volume from Infrared Thermography. Psychophysiology 2011, 48, 877–887. [Google Scholar] [CrossRef]
- Gomes, L.G.; de Mello, R.; Leal-Junior, A. Respiration Frequency Rate Monitoring Using Smartphone-Integrated Polymer Optical Fibers Sensors with Cloud Connectivity. Opt. Fiber Technol. 2023, 78, 103313. [Google Scholar] [CrossRef]
- Pambianco, B.; Sbrollini, A.; Marcantoni, I.; Morettini, M.; Fioretti, S.; Burattini, L. Electrocardiogram Derived Respiratory Signal through the Segmented-Beat Modulation Method. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 5681–5684. [Google Scholar]
- Sadr, N.; de Chazal, P. A Fast Principal Component Analysis Method For Calculating The ECG Derived Respiration. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; pp. 5294–5297. [Google Scholar]
- Bailón, R.; Sörnmo, L.; Laguna, P. ECG-Derived Respiratory Frequency Estimation. Adv. Methods Tools ECG Data Anal. 2006, 1, 215–243. [Google Scholar]
- Sarkar, S.; Bhattacherjee, S.; Pal, S. Extraction of Respiration Signal from ECG for Respiratory Rate Estimation. In Proceedings of the Michael Faraday IET International Summit 2015, Kolkata, India, 12–13 September 2015. [Google Scholar]
- Schäfer, A.; Kratky, K.W. Estimation of Breathing Rate from Respiratory Sinus Arrhythmia: Comparison of Various Methods. Ann. Biomed. Eng. 2008, 36, 476–485. [Google Scholar] [CrossRef]
- Kim, J.M.; Hong, J.H.; Kim, N.J.; Cha, E.J.; Lee, T.-S. Two Algorithms for Detecting Respiratory Rate from ECG Signal. In World Congress on Medical Physics and Biomedical Engineering, Seoul, Republic of Korea, 27 August–1 September 2006; Springer: Berlin/Heidelberg, Germany, 2006; pp. 4069–4071. [Google Scholar]
- Brandwood, B.M.; Naik, G.R.; Gunawardana, U.; Gargiulo, G.D. Combined Cardiac and Respiratory Monitoring from a Single Signal: A Case Study Employing the Fantasia Database. Sensors 2023, 23, 7401. [Google Scholar] [CrossRef] [PubMed]
- Dong, K.; Zhao, L.; Cai, Z.; Li, Y.; Li, J.; Liu, C. An Integrated Framework for Evaluation on Typical ECG-Derived Respiration Waveform Extraction and Respiration. Comput. Biol. Med. 2021, 135, 104593. [Google Scholar] [CrossRef] [PubMed]
- Lenis, G.; Conz, F.; Dössel, O. Combining Different ECG Derived Respiration Tracking Methods to Create an Optimal Reconstruction of the Breathing Pattern. Curr. Dir. Biomed. Eng. 2015, 1, 54–57. [Google Scholar] [CrossRef]
- Widjaja, D.; Varon, C.; Dorado, A.; Suykens, J.A.K.; Van Huffel, S. Application of Kernel Principal Component Analysis for Single-Lead-ECG-Derived Respiration. IEEE Trans. Biomed. Eng. 2012, 59, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Langley, P.; Bowers, E.J.; Murray, A. Principal Component Analysis as a Tool for Analyzing Beat-to-Beat Changes in ECG Features: Application to ECG-Derived Respiration. IEEE Trans. Biomed. Eng. 2010, 57, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Varon, C.; Morales, J.; Lázaro, J.; Orini, M.; Deviaene, M.; Kontaxis, S.; Testelmans, D.; Buyse, B.; Borzée, P.; Sörnmo, L.; et al. A Comparative Study of ECG-Derived Respiration in Ambulatory Monitoring Using the Single-Lead ECG. Sci. Rep. 2020, 10, 5704. [Google Scholar] [CrossRef] [PubMed]
- Alam, R.; Peden, D.B.; Lach, J.C. Wearable Respiration Monitoring: Interpretable Inference With Context and Sensor Biomarkers. IEEE J. Biomed. Health Inform. 2021, 25, 1938–1948. [Google Scholar] [CrossRef]
- Sinnecker, D.; Dommasch, M.; Barthel, P.; Müller, A.; Dirschinger, R.J.; Hapfelmeier, A.; Huster, K.M.; Laugwitz, K.-L.; Malik, M.; Schmidt, G. Assessment of Mean Respiratory Rate from ECG Recordings for Risk Stratification after Myocardial Infarction. J. Electrocardiol. 2014, 47, 700–704. [Google Scholar] [CrossRef]
- Lazaro, J.; Reljin, N.; Bailon, R.; Gil, E.; Noh, Y.; Laguna, P.; Chon, K.H. Electrocardiogram Derived Respiration for Tracking Changes in Tidal Volume from a Wearable Armband. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 596–599. [Google Scholar]
- Klum, M.; Minn, T.; Tigges, T.; Pielmus, A.-G.; Orglmeister, R. Minimally Spaced Electrode Positions for Multi-Functional Chest Sensors: ECG and Respiratory Signal Estimation. Curr. Dir. Biomed. Eng. 2016, 2, 695–699. [Google Scholar] [CrossRef]
- Schipke, J.D.; Arnold, G.; Pelzer, M. Effect of Respiration Rate on Short-Term Heart Rate Variability. J. Clin. Basic Cardiol. 1999, 2, 92–95. [Google Scholar]
- Gąsior, J.S.; Sacha, J.; Jeleń, P.J.; Zieliński, J.; Przybylski, J. Heart Rate and Respiratory Rate Influence on Heart Rate Variability Repeatability: Effects of the Correction for the Prevailing Heart Rate. Front. Physiol. 2016, 7, 356. [Google Scholar] [CrossRef]
- Aysin, B.; Aysin, E. Effect of Respiration in Heart Rate Variability (HRV) Analysis. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 1776–1779. [Google Scholar]
- Soer, R.; Dijkstra, M.W.S.; Bieleman, H.J.; Oosterveld, F.G.J.; Rijken, N.H.M. Influence of Respiration Frequency on Heart Rate Variability Parameters: A Randomized Cross-Sectional Study. J. Back Musculoskelet. Rehabil. 2021, 34, 1063–1068. [Google Scholar] [CrossRef]
- Druschky, K.; Lorenz, J.; Druschky, A. Effects of Respiratory Rate on Heart Rate Variability in Neurologic Outpatients with Epilepsies or Migraine: A Preliminary Study. Med. Princ. Pract. 2020, 29, 318–325. [Google Scholar] [CrossRef]
- Yasuma, F.; Hayano, J. Respiratory Sinus Arrhythmia. Chest 2004, 125, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Elstad, M.; O’Callaghan, E.L.; Smith, A.J.; Ben-Tal, A.; Ramchandra, R. Cardiorespiratory Interactions in Humans and Animals: Rhythms for Life. Am. J. Physiol. Circ. Physiol. 2018, 315, H6–H17. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, A.; Su, H.-W.; Heneghan, C.; Blunt, L.; O’Connor, C.; Niehaus, L. Measurement of Respiratory Rate Using Wearable Devices and Applications to COVID-19 Detection. npj Digit. Med. 2021, 4, 136. [Google Scholar] [CrossRef] [PubMed]
- Capodilupo, E. Understanding Respiratory Rate: What It Is, What’s Normal & Why You Should Track It. Available online: https://www.whoop.com/thelocker/what-is-respiratory-rate-normal (accessed on 20 December 2023).
- Berryhill, S.; Morton, C.J.; Dean, A.; Berryhill, A.; Provencio-Dean, N.; Patel, S.I.; Estep, L.; Combs, D.; Mashaqi, S.; Gerald, L.B.; et al. Effect of Wearables on Sleep in Healthy Individuals: A Randomized Crossover Trial and Validation Study. J. Clin. Sleep Med. 2020, 16, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Karlen, W.; Raman, S.; Ansermino, J.M.; Dumont, G.A. Multiparameter Respiratory Rate Estimation from the Photoplethysmogram. IEEE Trans. Biomed. Eng. 2013, 60, 1946–1953. [Google Scholar] [CrossRef] [PubMed]
- Bian, D.; Mehta, P.; Selvaraj, N. Respiratory Rate Estimation Using PPG: A Deep Learning Approach. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 5948–5952. [Google Scholar]
- Dubey, H.; Constant, N.; Mankodiya, K. RESPIRE: A Spectral Kurtosis-Based Method to Extract Respiration Rate from Wearable PPG Signals. In Proceedings of the 2017 IEEE/ACM International Conference on Connected Health: Applications, Systems and Engineering Technologies (CHASE), Philadelphia, PA, USA, 17–19 July 2017; pp. 84–89. [Google Scholar]
- Dai, R.; Lu, C.; Avidan, M.; Kannampallil, T. RespWatch: Robust Measurement of Respiratory Rate on Smartwatches with Photoplethysmography. In Proceedings of the International Conference on Internet-of-Things Design and Implementation, Charlottesvle VA, USA, 18–21 May 2021; ACM: New York, NY, USA, 2021; pp. 208–220. [Google Scholar]
- Shuzan, N.I.; Chowdhury, M.H.; Hossain, S.; Chowdhury, M.E.H.; Reaz, M.B.I.; Uddin, M.M.; Khandakar, A.; Bin Mahbub, Z.; Ali, S.H.M. A Novel Non-Invasive Estimation of Respiration Rate From Motion Corrupted Photoplethysmograph Signal Using Machine Learning Model. IEEE Access 2021, 9, 96775–96790. [Google Scholar] [CrossRef]
- Pimentel, M.A.F.; Charlton, P.H.; Clifton, D.A. Probabilistic Estimation of Respiratory Rate from Wearable Sensors. In Wearable Electronics Sensors; Springer: Cham, Switzerland, 2015; pp. 241–262. ISBN 978-3-319-18190-5. [Google Scholar]
- Cernat, R.A.; Ungureanu, C.; Aarts, R.M.; Arends, J.B.A.M. Real-Time Extraction of the Respiratory Rate from Photoplethysmographic Signal Using Wearable Devices. In Proceedings of the European Conference on Ambient Intelligence, Eindhoven, The Netherlands, 11–13 November 2014; pp. 1–17. [Google Scholar]
- Suleman, M.; Motaman, K.; Hasanpoor, Y.; Ghamari, M.; Alipour, K.; Zadeh, M. Respiratory Events Estimation From PPG Signals Using a Simple Peak Detection Algorithm. In Proceedings of the 29th National and 7th International Iranian Conference on Biomedical Engineering (ICBME), Tehran, Iran, 21–22 December 2022; pp. 119–123. [Google Scholar]
- Beh, W.-K.; Yang, Y.-C.; Lo, Y.-C.; Lee, Y.-C.; Wu, A.-Y. Machine-Aided PPG Signal Quality Assessment (SQA) for Multi-Mode Physiological Signal Monitoring. ACM Trans. Comput. Healthc. 2023, 4, 1–20. [Google Scholar] [CrossRef]
- OURA, How Oura Measures Respiratory Rate From Your Finger. Available online: https://ouraring.com/blog/respiratory-rate/ (accessed on 20 December 2023).
- SAMMOBILE, Samsung Galaxy Ring. Available online: https://www.sammobile.com/samsung/galaxy-ring (accessed on 20 December 2023).
- Lehrer, S. Understanding Lung Sounds, 3rd ed.; CreateSpace Independent Publishing Platform: North Charleston, SC, USA, 2018; ISBN 9781981284061. [Google Scholar]
- Fouzas, S.; Anthracopoulos, M.B.; Bohadana, A. Clinical Usefulness of Breath Sounds. In Breath Sounds; Springer International Publishing: Cham, Switzerland, 2018; pp. 33–52. [Google Scholar]
- Ohshimo, S.; Sadamori, T.; Tanigawa, K. Innovation in Analysis of Respiratory Sounds. Ann. Intern. Med. 2016, 164, 638. [Google Scholar] [CrossRef]
- Kim, Y.; Hyon, Y.; Lee, S.; Woo, S.-D.; Ha, T.; Chung, C. The Coming Era of a New Auscultation System for Analyzing Respiratory Sounds. BMC Pulm. Med. 2022, 22, 119. [Google Scholar] [CrossRef]
- Acharya, J.; Basu, A. Deep Neural Network for Respiratory Sound Classification in Wearable Devices Enabled by Patient Specific Model Tuning. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 535–544. [Google Scholar] [CrossRef]
- Aras, S.; Özturk, M.; Gangal, A. Automatic Detection of the Respiratory Cycle from Recorded, Single-Channel Sounds from Lungs. TURKISH J. Electr. Eng. Comput. Sci. 2018, 26, 11–22. [Google Scholar] [CrossRef]
- Lozano-García, M.; Fiz, J.A.; Martínez-Rivera, C.; Torrents, A.; Ruiz-Manzano, J.; Jané, R. Novel Approach to Continuous Adventitious Respiratory Sound Analysis for the Assessment of Bronchodilator Response. PLoS ONE 2017, 12, e0171455. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Abhishek, K.; Ghalib, M.R.; Nerurkar, P.; Shah, K.; Chandane, M.; Bhirud, S.; Patel, D.; Busnel, Y. Towards Cough Sound Analysis Using the Internet of Things and Deep Learning for Pulmonary Disease Prediction. Trans. Emerg. Telecommun. Technol. 2022, 33, e4184. [Google Scholar] [CrossRef]
- Liu, R.; Cai, S.; Zhang, K.; Hu, N. Detection of Adventitious Respiratory Sounds Based on Convolutional Neural Network. In Proceedings of the 2019 International Conference on Intelligent Informatics and Biomedical Sciences (ICIIBMS), Shanghai, China, 21–24 November 2019; pp. 298–303. [Google Scholar]
- Emmanouilidou, D.; McCollum, E.D.; Park, D.E.; Elhilali, M. Computerized Lung Sound Screening for Pediatric Auscultation in Noisy Field Environments. IEEE Trans. Biomed. Eng. 2018, 65, 1564–1574. [Google Scholar] [CrossRef]
- Aykanat, M.; Kılıç, Ö.; Kurt, B.; Saryal, S. Classification of Lung Sounds Using Convolutional Neural Networks. EURASIP J. Image Video Process. 2017, 2017, 65. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, Y.-S.; Yeo, M.-K.; Mahmood, M.; Zavanelli, N.; Chung, C.; Heo, J.Y.; Kim, Y.; Jung, S.-S.; Yeo, W.-H. Fully Portable Continuous Real-Time Auscultation with a Soft Wearable Stethoscope Designed for Automated Disease Diagnosis. Sci. Adv. 2022, 8, eabo5867. [Google Scholar] [CrossRef] [PubMed]
- Sanolla Sounds of Life AI Powered Primary Care Diagnostic Solutions. Available online: https://sanolla.com (accessed on 19 December 2023).
- Emokpae, L.E.; Emokpae, R.N.; Bowry, E.; Bin Saif, J.; Mahmud, M.; Lalouani, W.; Younis, M.; Joyner, R.L. A Wearable Multi-Modal Acoustic System for Breathing Analysis. J. Acoust. Soc. Am. 2022, 151, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Liu, D.; Jiang, Z.; Wang, H. Monitoring of Sleep Breathing States Based on Audio Sensor Utilizing Mel-Scale Features in Home Healthcare. J. Healthc. Eng. 2023, 2023, 6197564. [Google Scholar] [CrossRef]
- Werthammer, J.; Krasner, J.; DiBenedetto, J.; Stark, A.R. Apnea Monitoring by Acoustic Detection of Airflow. Pediatrics 1983, 71, 53–55. [Google Scholar] [CrossRef]
- Oletic, D.; Bilas, V. Energy-Efficient Respiratory Sounds Sensing for Personal Mobile Asthma Monitoring. IEEE Sens. J. 2016, 30, 2130008. [Google Scholar] [CrossRef]
- Oletic, D.; Arsenali, B.; Bilas, V. Low-Power Wearable Respiratory Sound Sensing. Sensors 2014, 14, 6535–6566. [Google Scholar] [CrossRef]
- Oletic, D.; Bilas, V. System-Level Power Consumption Analysis of the Wearable Asthmatic Wheeze Quantification. J. Sensors 2018, 2018, 6564158. [Google Scholar] [CrossRef]
- Reyes, B.; Olvera-Montes, N.; Charleston-Villalobos, S.; González-Camarena, R.; Mejía-Ávila, M.; Aljama-Corrales, T. A Smartphone-Based System for Automated Bedside Detection of Crackle Sounds in Diffuse Interstitial Pneumonia Patients. Sensors 2018, 18, 3813. [Google Scholar] [CrossRef]
- Reyes, B.; Reljin, N.; Chon, K. Tracheal Sounds Acquisition Using Smartphones. Sensors 2014, 14, 13830–13850. [Google Scholar] [CrossRef]
- Corbishley, P.; Rodriguez-Villegas, E. Breathing Detection: Towards a Miniaturized, Wearable, Battery-Operated Monitoring System. IEEE Trans. Biomed. Eng. 2008, 55, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Yang, H.; Liao, Q.; Si, W.; Chu, Y.; Chu, X.; Qin, L. A Review of Flexible Acceleration Sensors Based on Piezoelectric Materials: Performance Characterization, Parametric Analysis, Frontier Technologies, and Applications. Coatings 2023, 13, 1252. [Google Scholar] [CrossRef]
- Yilmaz, G.; Rapin, M.; Pessoa, D.; Rocha, B.M.; de Sousa, A.M.; Rusconi, R.; Carvalho, P.; Wacker, J.; Paiva, R.P.; Chételat, O. A Wearable Stethoscope for Long-Term Ambulatory Respiratory Health Monitoring. Sensors 2020, 20, 5124. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Yu, S.; Liu, H.; Liu, J.; Xiao, Y.; Wu, D.; Pan, X.; Zhou, C.; Lei, Y.; Liu, S. A Two-Stage Amplified PZT Sensor for Monitoring Lung and Heart Sounds in Discharged Pneumonia Patients. Microsyst. Nanoeng. 2021, 7, 55. [Google Scholar] [CrossRef]
- Yatani, K.; Truong, K.N. BodyScope. In Proceedings of the 2012 ACM Conference on Ubiquitous Computing, Pittsburgh, PA, USA, 5–8 September 2012; ACM: New York, NY, USA, 2012; pp. 341–350. [Google Scholar]
- Li, S.-H.; Lin, B.-S.; Tsai, C.-H.; Yang, C.-T.; Lin, B.-S. Design of Wearable Breathing Sound Monitoring System for Real-Time Wheeze Detection. Sensors 2017, 17, 171. [Google Scholar] [CrossRef] [PubMed]
- Yuasa, Y.; Suzuki, K. Wearable Device for Monitoring Respiratory Phases Based on Breathing Sound and Chest Movement. Adv. Biomed. Eng. 2019, 8, 85–91. [Google Scholar] [CrossRef]
- Gupta, P.; Moghimi, M.J.; Jeong, Y.; Gupta, D.; Inan, O.T.; Ayazi, F. Precision Wearable Accelerometer Contact Microphones for Longitudinal Monitoring of Mechano-Acoustic Cardiopulmonary Signals. npj Digit. Med. 2020, 3, 19. [Google Scholar] [CrossRef] [PubMed]
- Montazeri Ghahjaverestan, N.; Kabir, M.; Saha, S.; Zhu, K.; Gavrilovic, B.; Alshaer, H.; Taati, B.; Yadollahi, A. Automatic Respiratory Phase Identification Using Tracheal Sounds and Movements During Sleep. Ann. Biomed. Eng. 2021, 49, 1521–1533. [Google Scholar] [CrossRef] [PubMed]
- Zansors RESPATM. Available online: https://www.zansors.com/respa (accessed on 20 December 2023).
- Tailor, S.A.; Chauhan, J.; Mascolo, C. A First Step towards On-Device Monitoring of Body Sounds in the Wild. In Proceedings of the Adjunct Proceedings of the 2020 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2020 ACM International Symposium on Wearable Computers, Virtual, 12–17 September 2020; ACM: New York, NY, USA, 2020; pp. 708–712. [Google Scholar]
- Med-Tech Innovation, Wearable to Assess Lung Function with Acoustic Levels. Available online: www.med-technews.com/news/Digital-in-Healthcare-News/wearable-to-assess-lung-function/ (accessed on 20 December 2023).
- Elfaramawy, T.; Fall, C.L.; Arab, S.; Morissette, M.; Lellouche, F.; Gosselin, B. A Wireless Respiratory Monitoring System Using a Wearable Patch Sensor Network. IEEE Sens. J. 2019, 19, 650–657. [Google Scholar] [CrossRef]
- Lin, B.-S.; Jhang, R.-J.; Lin, B.-S. Wearable Cardiopulmonary Function Evaluation System for Six-Minute Walking Test. Sensors 2019, 19, 4656. [Google Scholar] [CrossRef]
- Frerichs, I.; Vogt, B.; Wacker, J.; Paradiso, R.; Braun, F.; Rapin, M.; Caldani, L.; Chételat, O.; Weiler, N. Multimodal Remote Chest Monitoring System with Wearable Sensors: A Validation Study in Healthy Subjects. Physiol. Meas. 2020, 41, 015006. [Google Scholar] [CrossRef]
- Yin, S.; Fang, H.; Hou, X. Athlete’s Respiratory Frequency and Physical Energy Consumption Model Based on Speech Recognition Technology. Int. J. Speech Technol. 2020, 23, 389–397. [Google Scholar] [CrossRef]
- Health Care Originals, ADAMM: For Personal Use. Available online: https://www.healthcareoriginals.com/personal (accessed on 20 December 2023).
- High-Tech Vest Monitors Lung Function. Available online: https://healthcare-in-europe.com/en/news/high-tech-vest-monitors-lung-function.htm (accessed on 20 December 2023).
- Cotur, Y.; Kasimatis, M.; Kaisti, M.; Olenik, S.; Georgiou, C.; Güder, F. Stretchable Composite Acoustic Transducer for Wearable Monitoring of Vital Signs. Adv. Funct. Mater. 2020, 30, 1910288. [Google Scholar] [CrossRef]
- Chen, X.; Luo, F.; Yuan, M.; Xie, D.; Shen, L.; Zheng, K.; Wang, Z.; Li, X.; Tao, L. A Dual-Functional Graphene-Based Self-Alarm Health-Monitoring E-Skin. Adv. Funct. Mater. 2019, 29, 1904706. [Google Scholar] [CrossRef]
- Ni, X.; Ouyang, W.; Jeong, H.; Kim, J.-T.; Tzavelis, A.; Mirzazadeh, A.; Wu, C.; Lee, J.Y.; Keller, M.; Mummidisetty, C.K.; et al. Automated, Multiparametric Monitoring of Respiratory Biomarkers and Vital Signs in Clinical and Home Settings for COVID-19 Patients. Proc. Natl. Acad. Sci. USA 2021, 118, e2026610118. [Google Scholar] [CrossRef] [PubMed]
- Markandeya, M.N.; Abeyratne, U.R.; Hukins, C. Overnight Airway Obstruction Severity Prediction Centered on Acoustic Properties of Smart Phone: Validation with Esophageal Pressure. Physiol. Meas. 2020, 41, 105002. [Google Scholar] [CrossRef] [PubMed]
- Nakano, H.; Hirayama, K.; Sadamitsu, Y.; Toshimitsu, A.; Fujita, H.; Shin, S.; Tanigawa, T. Monitoring Sound To Quantify Snoring and Sleep Apnea Severity Using a Smartphone: Proof of Concept. J. Clin. Sleep Med. 2014, 10, 73–78. [Google Scholar] [CrossRef]
- Barata, F.; Tinschert, P.; Rassouli, F.; Steurer-Stey, C.; Fleisch, E.; Puhan, M.A.; Brutsche, M.; Kotz, D.; Kowatsch, T. Automatic Recognition, Segmentation, and Sex Assignment of Nocturnal Asthmatic Coughs and Cough Epochs in Smartphone Audio Recordings: Observational Field Study. J. Med. Internet Res. 2020, 22, e18082. [Google Scholar] [CrossRef]
- Bokov, P.; Mahut, B.; Flaud, P.; Delclaux, C. Wheezing Recognition Algorithm Using Recordings of Respiratory Sounds at the Mouth in a Pediatric Population. Comput. Biol. Med. 2016, 70, 40–50. [Google Scholar] [CrossRef]
- Nam, Y.; Reyes, B.A.; Chon, K.H. Estimation of Respiratory Rates Using the Built-in Microphone of a Smartphone or Headset. IEEE J. Biomed. Health Inform. 2016, 20, 1493–1501. [Google Scholar] [CrossRef]
- Xue, B.; Shi, W.; Chotirmall, S.H.; Koh, V.C.A.; Ang, Y.Y.; Tan, R.X.; Ser, W. Distance-Based Detection of Cough, Wheeze, and Breath Sounds on Wearable Devices. Sensors 2022, 22, 2167. [Google Scholar] [CrossRef]
- Chen, G.; Shen, S.; Tat, T.; Zhao, X.; Zhou, Y.; Fang, Y.; Chen, J. Wearable Respiratory Sensors for COVID-19 Monitoring. View 2022, 3, 20220024. [Google Scholar] [CrossRef]
- Costanzo, I.; Sen, D.; Guler, U. A Prototype Towards a Transcutaneous Oxygen Sensing Wearable. In Proceedings of the 2019 IEEE Biomedical Circuits and Systems Conference (BioCAS), Nara, Japan, 17–19 October 2019; pp. 1–4. [Google Scholar]
- Velumani, M.; Prasanth, A.; Narasimman, S.; Chandrasekhar, A.; Sampson, A.; Meher, S.R.; Rajalingam, S.; Rufus, E.; Alex, Z.C. Nanomaterial-Based Sensors for Exhaled Breath Analysis: A Review. Coatings 2022, 12, 1989. [Google Scholar] [CrossRef]
- Mürtz, M. Breath Diagnostics Using Laser Spectroscopy. Opt. Photonics News 2005, 16, 30. [Google Scholar] [CrossRef]
- Yang, D.; Gopal, R.A.; Lkhagvaa, T.; Choi, D. Metal-Oxide Gas Sensors for Exhaled-Breath Analysis: A Review. Meas. Sci. Technol. 2021, 32, 102004. [Google Scholar] [CrossRef]
- Mazzatenta, A.; Pokorski, M.; Di Giulio, C. Volatile Organic Compounds (VOCs) in Exhaled Breath as a Marker of Hypoxia in Multiple Chemical Sensitivity. Physiol. Rep. 2021, 9, e15034. [Google Scholar] [CrossRef]
- Jalal, A.H.; Alam, F.; Roychoudhury, S.; Umasankar, Y.; Pala, N.; Bhansali, S. Prospects and Challenges of Volatile Organic Compound Sensors in Human Healthcare. ACS Sensors 2018, 3, 1246–1263. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, A.; Leonardi, S.G.; Neri, G. Detection of Hazardous Volatile Organic Compounds (VOCs) by Metal Oxide Nanostructures-Based Gas Sensors: A Review. Ceram. Int. 2016, 42, 15119–15141. [Google Scholar] [CrossRef]
- Lahlalia, A.; Filipovic, L.; Selberherr, S. Modeling and Simulation of Novel Semiconducting Metal Oxide Gas Sensors for Wearable Devices. IEEE Sens. J. 2018, 18, 1960–1970. [Google Scholar] [CrossRef]
- Su, Y.; Wang, J.; Wang, B.; Yang, T.; Yang, B.; Xie, G.; Zhou, Y.; Zhang, S.; Tai, H.; Cai, Z.; et al. Alveolus-Inspired Active Membrane Sensors for Self-Powered Wearable Chemical Sensing and Breath Analysis. ACS Nano 2020, 14, 6067–6075. [Google Scholar] [CrossRef]
- Ou, L.-X.; Liu, M.-Y.; Zhu, L.-Y.; Zhang, D.W.; Lu, H.-L. Recent Progress on Flexible Room-Temperature Gas Sensors Based on Metal Oxide Semiconductor. Nano-Micro Lett. 2022, 14, 206. [Google Scholar] [CrossRef]
- Wu, Y.; Feng, J.; Hu, G.; Zhang, E.; Yu, H.-H. Colorimetric Sensors for Chemical and Biological Sensing Applications. Sensors 2023, 23, 2749. [Google Scholar] [CrossRef]
- Wang, D.; Zhang, F.; Prabhakar, A.; Qin, X.; Forzani, E.S.; Tao, N. Colorimetric Sensor for Online Accurate Detection of Breath Acetone. ACS Sensors 2021, 6, 450–453. [Google Scholar] [CrossRef]
- Mazzone, P.J.; Wang, X.-F.; Xu, Y.; Mekhail, T.; Beukemann, M.C.; Na, J.; Kemling, J.W.; Suslick, K.S.; Sasidhar, M. Exhaled Breath Analysis with a Colorimetric Sensor Array for the Identification and Characterization of Lung Cancer. J. Thorac. Oncol. 2012, 7, 137–142. [Google Scholar] [CrossRef]
- Mazzone, P.J.; Hammel, J.; Dweik, R.; Na, J.; Czich, C.; Laskowski, D.; Mekhail, T. Diagnosis of Lung Cancer by the Analysis of Exhaled Breath with a Colorimetric Sensor Array. Thorax 2007, 62, 565–568. [Google Scholar] [CrossRef]
- Maurya, M.R.; Onthath, H.; Morsy, H.; Riyaz, N.-U.-S.; Ibrahim, M.; Ahmed, A.E.; Abuznad, R.; Alruwaili, A.; Alsaedi, F.; Kasak, P.; et al. Colorimetry-Based Detection of Nitric Oxide from Exhaled Breath for Quantification of Oxidative Stress in Human Body. Healthcare 2021, 9, 1055. [Google Scholar] [CrossRef]
- Shahid, S.; Geetha, M.; Sadasivuni, K.K.; Remani, D.; Muthusamy, S.; Muthalif, A.G.A.; Al-maadeed, S. Highly Sensitive and Selective Colorimetric Sensing of CO2 for Biomedical Applications. 3 Biotech 2022, 12, 334. [Google Scholar] [CrossRef] [PubMed]
- Aqueveque, P.; Díaz, M.; Gomez, B.; Osorio, R.; Pastene, F.; Radrigan, L.; Morales, A. Embedded Electronic Sensor for Monitoring of Breathing Activity, Fitting and Filter Clogging in Reusable Industrial Respirators. Biosensors 2022, 12, 991. [Google Scholar] [CrossRef] [PubMed]
- Dinh, T.; Nguyen, T.; Phan, H.-P.; Nguyen, N.-T.; Dao, D.V.; Bell, J. Stretchable Respiration Sensors: Advanced Designs and Multifunctional Platforms for Wearable Physiological Monitoring. Biosens. Bioelectron. 2020, 166, 112460. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.; Ullah, S.; Fernández-García, R.; Gil, I. Wearable Sensors for Respiration Monitoring: A Review. Sensors 2023, 23, 7518. [Google Scholar] [CrossRef] [PubMed]
- Storck, K.; Karlsson, M.; Ask, P.; Loyd, D. Heat Transfer Evaluation of the Nasal Thermistor Technique. IEEE Trans. Biomed. Eng. 1996, 43, 1187–1191. [Google Scholar] [CrossRef]
- Hurtado, D.E.; Abusleme, A.; Chávez, J.A.P. Non-Invasive Continuous Respiratory Monitoring Using Temperature-Based Sensors. J. Clin. Monit. Comput. 2020, 34, 223–231. [Google Scholar] [CrossRef]
- Agnihotri, A. Human Body Respiration Measurement Using Digital Temperature Sensor with I2c Interface. Int. J. Sci. Res. Publ. 2013, 3, 1–8. [Google Scholar]
- Basra, A.; Mukhopadhayay, B.; Kar, S. Temperature Sensor Based Ultra Low Cost Respiration Monitoring System. In Proceedings of the 9th International Conference on Communication Systems and Networks (COMSNETS), Bengaluru, India, 4–8 January 2017; pp. 530–535. [Google Scholar]
- Takahashi, Y.; Gu, Y.; Nakada, T.; Abe, R.; Nakaguchi, T. Estimation of Respiratory Rate from Thermography Using Respiratory Likelihood Index. Sensors 2021, 21, 4406. [Google Scholar] [CrossRef]
- Hsu, C.H.; Chow, J.C. Design and clinic monitoring of a newly developed non-attached infant apnea monitor. Biomed. Eng. Appl. Basis Commun. 2005, 17, 126–134. [Google Scholar] [CrossRef]
- Yu, Y.; Zhu, W.; Zhou, J.; Guo, Z.; Liu, Y.; Deng, Y. Wearable Respiration Sensor for Continuous Healthcare Monitoring Using a Micro-Thermoelectric Generator with Rapid Response Time and Chip-Level Design. Adv. Mater. Technol. 2022, 7, 2101416. [Google Scholar] [CrossRef]
- Zhao, C.; Liu, D.; Cai, Z.; Du, B.; Zou, M.; Tang, S.; Li, B.; Xiong, C.; Ji, P.; Zhang, L.; et al. A Wearable Breath Sensor Based on Fiber-Tip Microcantilever. Biosensors 2022, 12, 168. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Y.; Yang, H.; Wang, W.; Dai, Y.-Z.; Niu, L.-G.; Lv, C.; Xia, H.; Liu, T. Fast-Response Humidity Sensor Based on Laser Printing for Respiration Monitoring. RSC Adv. 2020, 10, 8910–8916. [Google Scholar] [CrossRef]
- Zhou, C.; Zhang, X.; Tang, N.; Fang, Y.; Zhang, H.; Duan, X. Rapid Response Flexible Humidity Sensor for Respiration Monitoring Using Nano-Confined Strategy. Nanotechnology 2020, 31, 125302. [Google Scholar] [CrossRef]
- Güder, F.; Ainla, A.; Redston, J.; Mosadegh, B.; Glavan, A.; Martin, T.J.; Whitesides, G.M. Paper-Based Electrical Respiration Sensor. Angew. Chem. Int. Ed. 2016, 55, 5727–5732. [Google Scholar] [CrossRef]
- Tekcin, M.; Kuzubasoglu, B.A.; Sayar, E.; Yalcin, M.K.; Bahadir, S.K. Performance Analysis of Wearable and Flexible Humidity Sensor Integrated to Face Mask for Respiration Monitoring. In Proceedings of the IEEE 3rd Eurasia Conference on IOT, Communication and Engineering (ECICE), Yunlin, Taiwan, 29–31 October 2021; pp. 663–666. [Google Scholar]
- Pang, Y.; Jian, J.; Tu, T.; Yang, Z.; Ling, J.; Li, Y.; Wang, X.; Qiao, Y.; Tian, H.; Yang, Y.; et al. Wearable Humidity Sensor Based on Porous Graphene Network for Respiration Monitoring. Biosens. Bioelectron. 2018, 116, 123–129. [Google Scholar] [CrossRef]
- Shneerson, J.M. Sleep Medicine: A Guide to Sleep and Its Disorders, 2nd ed.; Blackwell Publishing Ltd.: Oxford, UK, 2005; ISBN 978-1-405-17851-8. [Google Scholar]
- Lee-Chiong, L. Sleep: A Comprehensive Handbook; Lee-Chiong, T., Ed.; Wiley: New York, NY, USA, 2005; ISBN 978-0-471-68371-1. [Google Scholar]
- Tobin, M.J. Respiratory Monitoring in the Intensive Care Unit. Am. Rev. Respir. Dis. 1988, 138, 1625–1642. [Google Scholar] [CrossRef] [PubMed]
- Ionescu, C.M.; Copot, D. Monitoring Respiratory Impedance by Wearable Sensor Device: Protocol and Methodology. Biomed. Signal Process. Control 2017, 36, 57–62. [Google Scholar] [CrossRef]
- Manoni, A.; Loreti, F.; Radicioni, V.; Pellegrino, D.; Della Torre, L.; Gumiero, A.; Halicki, D.; Palange, P.; Irrera, F. A New Wearable System for Home Sleep Apnea Testing, Screening, and Classification. Sensors 2020, 20, 7014. [Google Scholar] [CrossRef] [PubMed]
- Liou, T.G.; Kanner, R.E. Spirometry. Clin. Rev. Allergy Immunol. 2009, 37, 137–152. [Google Scholar] [CrossRef]
- Carta, R.; Turgis, D.; Hermans, B.; Jourand, P.; Onclin, R.; Puers, R. A Differential Pressure Approach to Spirometry. In Proceedings of the 2007 IEEE Biomedical Circuits and Systems Conference, Montreal, QC, Canada, 27–30 November 2007; pp. 5–8. [Google Scholar]
- Moore, V.C. Spirometry: Step by Step. Breathe 2012, 8, 232–240. [Google Scholar] [CrossRef]
- Hariadi, I. Sensitivity Analysis of Silicon MEMS Thermal Flow Sensor for Spirometer Application. In Proceedings of the 2011 2nd International Conference on Instrumentation, Communications, Information Technology, and Biomedical Engineering, Bandung, Indonesia, 8–9 November 2011; pp. 249–253. [Google Scholar]
- Beyaz, M.I.; Habibiabad, S.; Yildiz, H.; Goreke, U.; Azgin, K. A Turbine-Based MEMS Sensor for Spirometry With Wearable Devices. IEEE Sens. J. 2019, 19, 8612–8617. [Google Scholar] [CrossRef]
- Baucells Costa, A.; Zhou, B.; Amiraslanov, O.; Lukowicz, P. Wearable Spirometry: Using Integrated Environment Sensor for Breath Measurement. In Proceedings of the UBICOMM 2018, The Twelfth International Conference on Mobile Ubiquitous Computing, Systems, Services and Technologies, Athens, Greece, 18–22 November 2018. [Google Scholar]
- Zhou, B.; Baucells Costa, A.; Lukowicz, P. Accurate Spirometry with Integrated Barometric Sensors in Face-Worn Garments. Sensors 2020, 20, 4234. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Costa, A.B.; Lukowicz, P. CoRSA: A Cardio-Respiratory Monitor in Sport Activities. In Proceedings of the 23rd International Symposium on Wearable Computers, London, UK, 9–13 September 2019; ACM: New York, NY, USA, 2019; pp. 254–256. [Google Scholar]
- Cortex Medical, METAMAX® 3B. Available online: https://cortex-medical.com/EN/METAMAX-3B-en.htm (accessed on 20 December 2023).
- Hafen, B.B.; Sharma, S. Oxygen Saturation. Available online: https://www.ncbi.nlm.nih.gov/books/NBK525974/ (accessed on 19 December 2023).
- Azarnoosh, M.; Doostdar, H. Assessment of Photoplethysmography Method in Extraction of Hemoglobin Concentration. J. Biomed. Phys. Eng. 2018, 9, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T. Current Progress of Photoplethysmography and SpO2 for Health Monitoring. Biomed. Eng. Lett. 2019, 9, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Koteska, B.; Bodanova, A.M.; Mitrova, H.; Sidorenko, M.; Lehocki, F. A Deep Learning Approach to Estimate SpO2 from PPG Signals. In Proceedings of the 9th International Conference on Bioinformatics Research and Applications, Berlin, Germany, 18–20 September 2022; ACM: New York, NY, USA, 2022; pp. 142–148. [Google Scholar]
- Fiorini, L.; Cavallo, F.; Martinelli, M.; Rovini, E. Characterization of a PPG Wearable Sensor to Be Embedded into an Innovative Ring-Shaped Device for Healthcare Monitoring; Springer: Berlin/Heidelberg, Germany, 2021; pp. 49–63. [Google Scholar]
- Ouraring. Available online: www.ouraring.com/ (accessed on 4 May 2023).
- Nicholls, M. Smart Ring Medical Device for 24/7 Blood Pressure Monitoring. Available online: https://healthcare-in-europe.com/en/news/smart-ring-medical-device-blood-pressure-monitoring.html (accessed on 19 December 2023).
- Bestbier, A.; Fourie, P.R. Development of a Vital Signs Monitoring Wireless Ear Probe. In Proceedings of the 2018 3rd Biennial South African Biomedical Engineering Conference (SAIBMEC), Stellenbosch, South Africa, 4–6 April 2018; pp. 1–5. [Google Scholar]
- Rodriguez-Labra, J.I.; Kosik, C.; Maddipatla, D.; Narakathu, B.B.; Atashbar, M.Z. Development of a PPG Sensor Array as a Wearable Device for Monitoring Cardiovascular Metrics. IEEE Sens. J. 2021, 21, 26320–26327. [Google Scholar] [CrossRef]
- Kim, K.B.; Baek, H.J. Photoplethysmography in Wearable Devices: A Comprehensive Review of Technological Advances, Current Challenges, and Future Directions. Electronics 2023, 12, 2923. [Google Scholar] [CrossRef]
- Xiao, S.; Lv, Z.; Zhou, X. SpO2 and Heart Rate Measurement with Wearable Watch Based on PPG. In Proceedings of the 2015 IET International Conference on Biomedical Image and Signal Processing (ICBISP 2015), Beijing, China, 19 November 2015. [Google Scholar]
- Tipparaju, V.V.; Mora, S.J.; Yu, J.; Tsow, F.; Xian, X. Wearable Transcutaneous CO₂ Monitor Based on Miniaturized Nondispersive Infrared Sensor. IEEE Sens. J. 2021, 21, 17327–17334. [Google Scholar] [CrossRef]
- Dias, D.; Paulo Silva Cunha, J. Wearable Health Devices—Vital Sign Monitoring, Systems and Technologies. Sensors 2018, 18, 2414. [Google Scholar] [CrossRef] [PubMed]
- Tufan, T.B.; Sen, D.; Guler, U. An Infra-Red-Based Prototype for a Miniaturized Transcutaneous Carbon Dioxide Monitor. In Proceedings of the 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 7132–7135. [Google Scholar]
- Vincent, T.A.; Gardner, J.W. A Low Cost MEMS Based NDIR System for the Monitoring of Carbon Dioxide in Breath Analysis at Ppm Levels. Sens. Actuators B Chem. 2016, 236, 954–964. [Google Scholar] [CrossRef]
- Tufan, T.B.; Guler, U. A Fluorescent Thin Film-Based Miniaturized Transcutaneous Carbon Dioxide Monitor. In Proceedings of the 2021 IEEE Biomedical Circuits and Systems Conference (BioCAS), Virtual, 7–9 October 2021; pp. 1–5. [Google Scholar]
- Ahmed, S.; Islam, M.T.; Biswas, S.; Samrat, R.H.; Akash, T.I.; Subhana, A.; Shahnaz, C. CapNet: A Deep Learning-Based Framework for Estimation of Capnograph Signal from PPG. In Proceedings of the 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022; pp. 3392–3395. [Google Scholar]
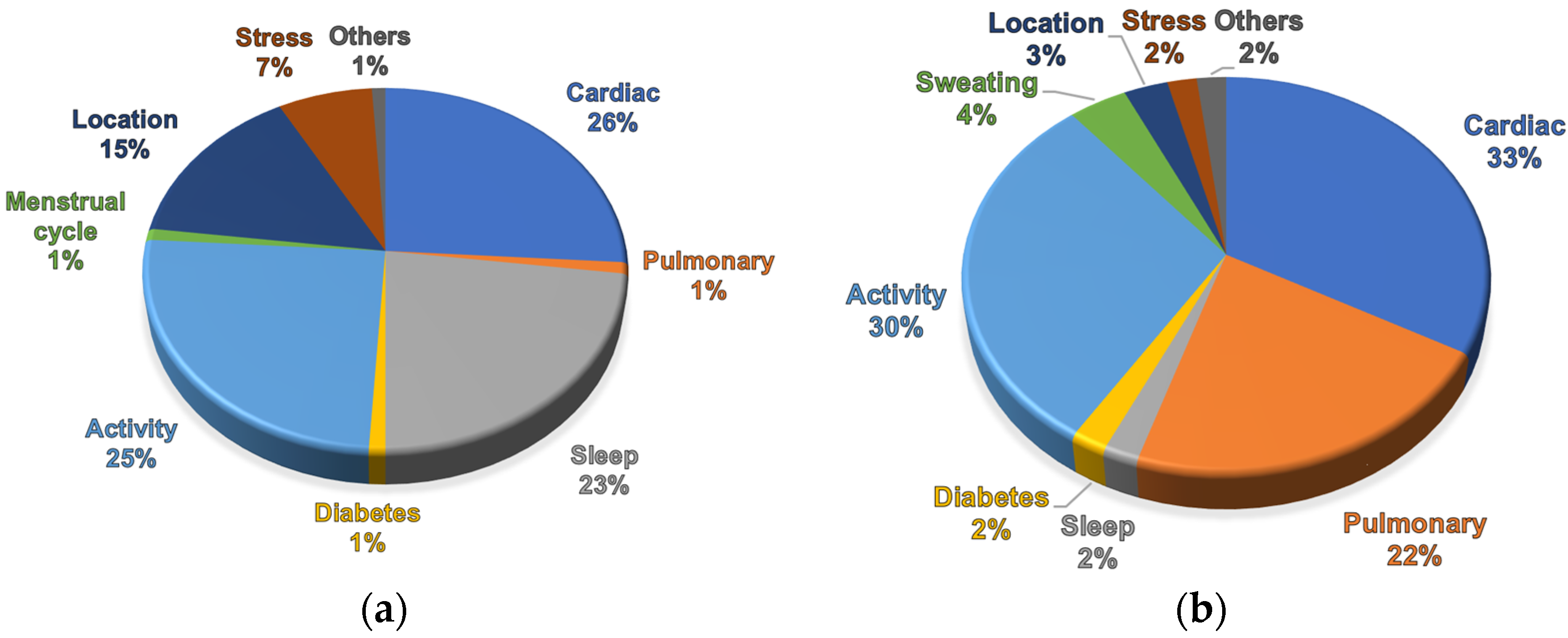
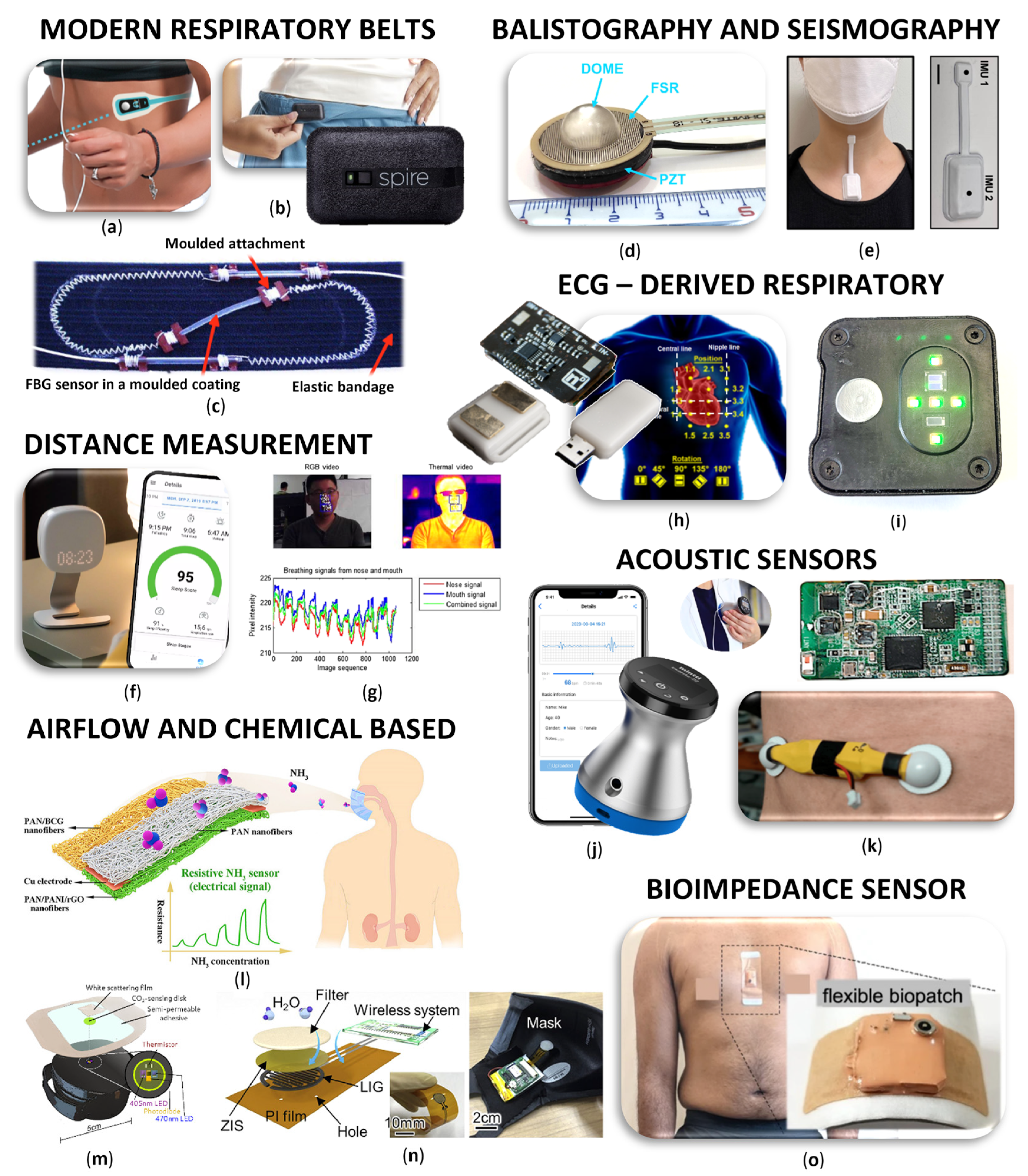
| Method | Advantages | Disadvantages | Measured Parameters | Accuracy | Application | Sampling Frequency | Convenience |
|---|---|---|---|---|---|---|---|
| Chest belt | High accuracy cost-effective, long battery life | Uncomfortable for long-term use, may not capture subtle movements | RR, RV, apnea | Generally high for basic monitoring | Well-suited for sports and fitness applications, sleep monitoring | <100 Hz | Moderate |
| Patch | Comfortable, small size, suitable for long term monitoring | Precise placement and close contact with skin is crucial | RR, RV | Generally high for basic monitoring | Well-suited for sports and fitness applications, disease progress | <100 Hz | High |
| SCG/ BCG | Capture subtle movements, patterns | Complexity in interpretation, susceptible to interference | RR, RV, respiratory patterns | Variable, may require validation for clinical use | Cardio-respiratory dynamics, Sleep monitoring | 0.1–5 kHz | Moderate |
| Impedance | Nonintrusive, low power consumption | Susceptible to interference, proper contact is crucial | RR, RV | Variable, affected by skin contact | Suitable for continuous monitoring | 0.03–32 kHz | Moderate |
| Optical fiber | Capture subtle movements, comfortable, resistant to EMG | Sophisticated signal processing, relatively expensive, fragile | RR, RV | Generally good for basic monitoring | Integrated into clothing or beds, monitoring in MRI or CT | 0.01–3 kHz | High |
| Camera | Non-contact, captures multiple parameters | Privacy concerns, limited accuracy in certain conditions | RR, RV, temperature | Moderate, affected by lighting and resolution | Continuous monitoring in controlled environments | 30–100 Hz | Remote |
| Radar | Non-contact, captures motion through clothing | Limited accuracy in certain situations | RR, RV | Moderate, affected by environment | Continuous monitoring in controlled environments | Operational frequency 1.8–24 GHz | Remote |
| EDR | Continuous monitoring, additional cardio data | Indirect measurement, accuracy influenced by artifacts | RR, RV | Generally good for trends monitoring | Combined cardio and respiratory assessment | 50–500 Hz | High |
| Acoustic | Non-invasive, cost-effective | Ambient noise interference, may not be suitable for all settings | Respiratory sounds, RR, airflow | Good for certain applications (e.g., diagnosing respiratory conditions) | Cough, asthma, apnea detection, remote patient monitoring, smartphone apps | 0.01–22 kHz | Moderate |
| Gases | Comprehensive view of respiratory parameters | Limited scope, uncomfortable | SpO2, CO2, NH3, humidity, temperature | High for clinical settings | Diagnosing specific respiratory and metabolic conditions | - | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitazkova, D.; Foltan, E.; Kosnacova, H.; Micjan, M.; Donoval, M.; Kuzma, A.; Kopani, M.; Vavrinsky, E. Advances in Respiratory Monitoring: A Comprehensive Review of Wearable and Remote Technologies. Biosensors 2024, 14, 90. https://doi.org/10.3390/bios14020090
Vitazkova D, Foltan E, Kosnacova H, Micjan M, Donoval M, Kuzma A, Kopani M, Vavrinsky E. Advances in Respiratory Monitoring: A Comprehensive Review of Wearable and Remote Technologies. Biosensors. 2024; 14(2):90. https://doi.org/10.3390/bios14020090
Chicago/Turabian StyleVitazkova, Diana, Erik Foltan, Helena Kosnacova, Michal Micjan, Martin Donoval, Anton Kuzma, Martin Kopani, and Erik Vavrinsky. 2024. "Advances in Respiratory Monitoring: A Comprehensive Review of Wearable and Remote Technologies" Biosensors 14, no. 2: 90. https://doi.org/10.3390/bios14020090
APA StyleVitazkova, D., Foltan, E., Kosnacova, H., Micjan, M., Donoval, M., Kuzma, A., Kopani, M., & Vavrinsky, E. (2024). Advances in Respiratory Monitoring: A Comprehensive Review of Wearable and Remote Technologies. Biosensors, 14(2), 90. https://doi.org/10.3390/bios14020090