Advances in Cancer Research: Current and Future Diagnostic and Therapeutic Strategies




Abstract
1. Introduction
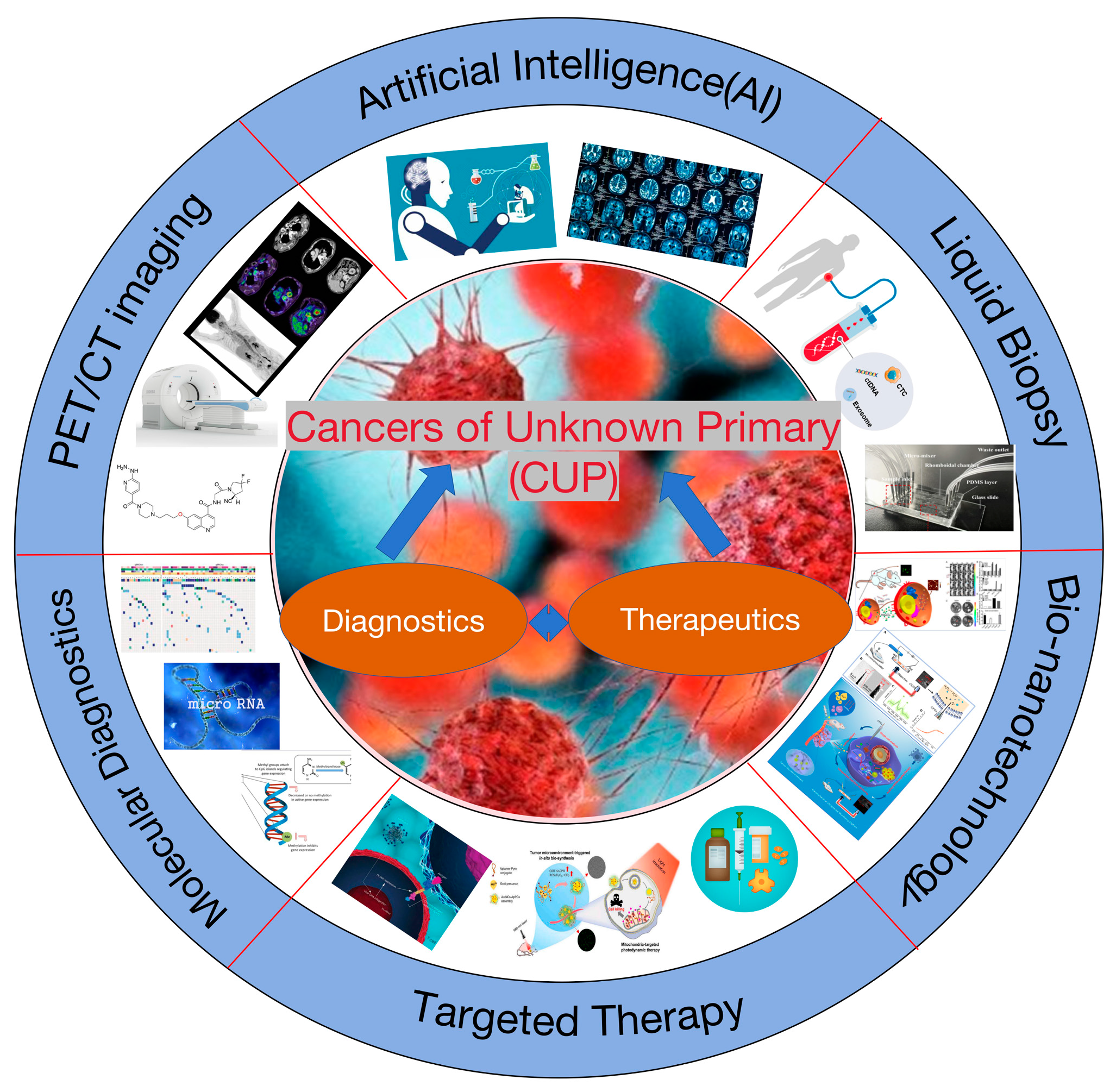
2. Diagnostic Techniques for Cancers of Unknown Primary (CUP)
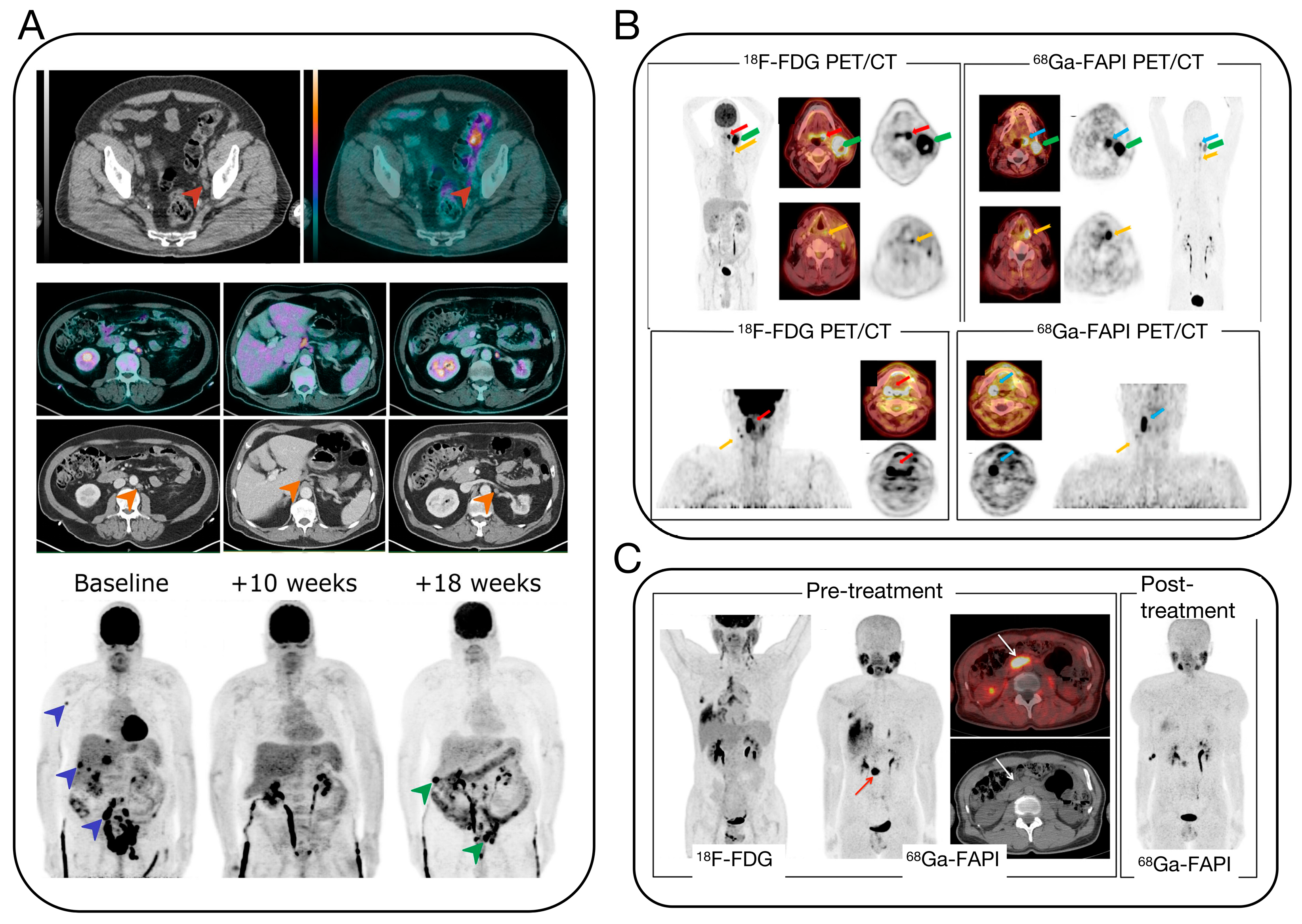
2.1. PET/CT Imaging
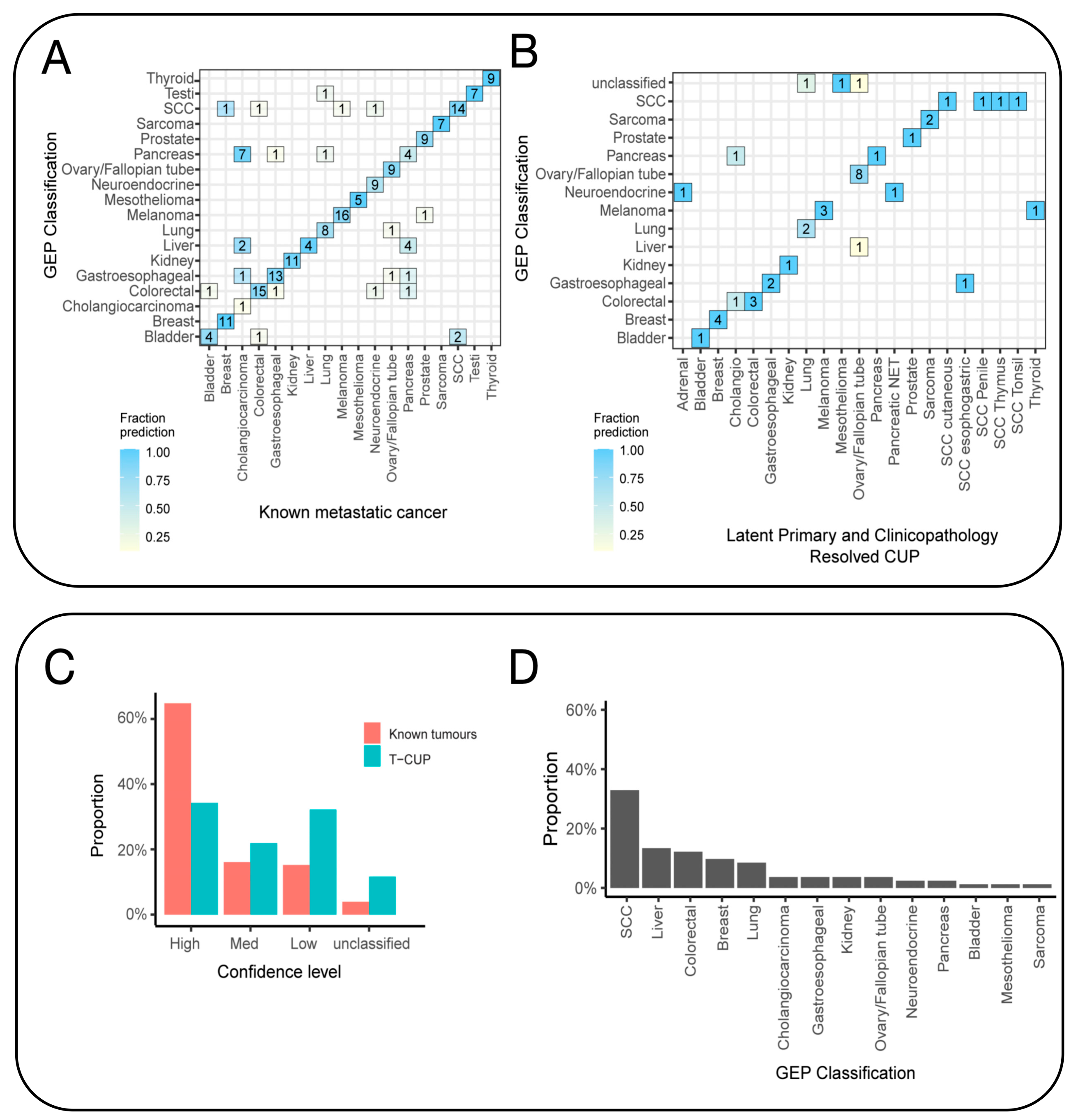
2.2. Molecular Diagnostics
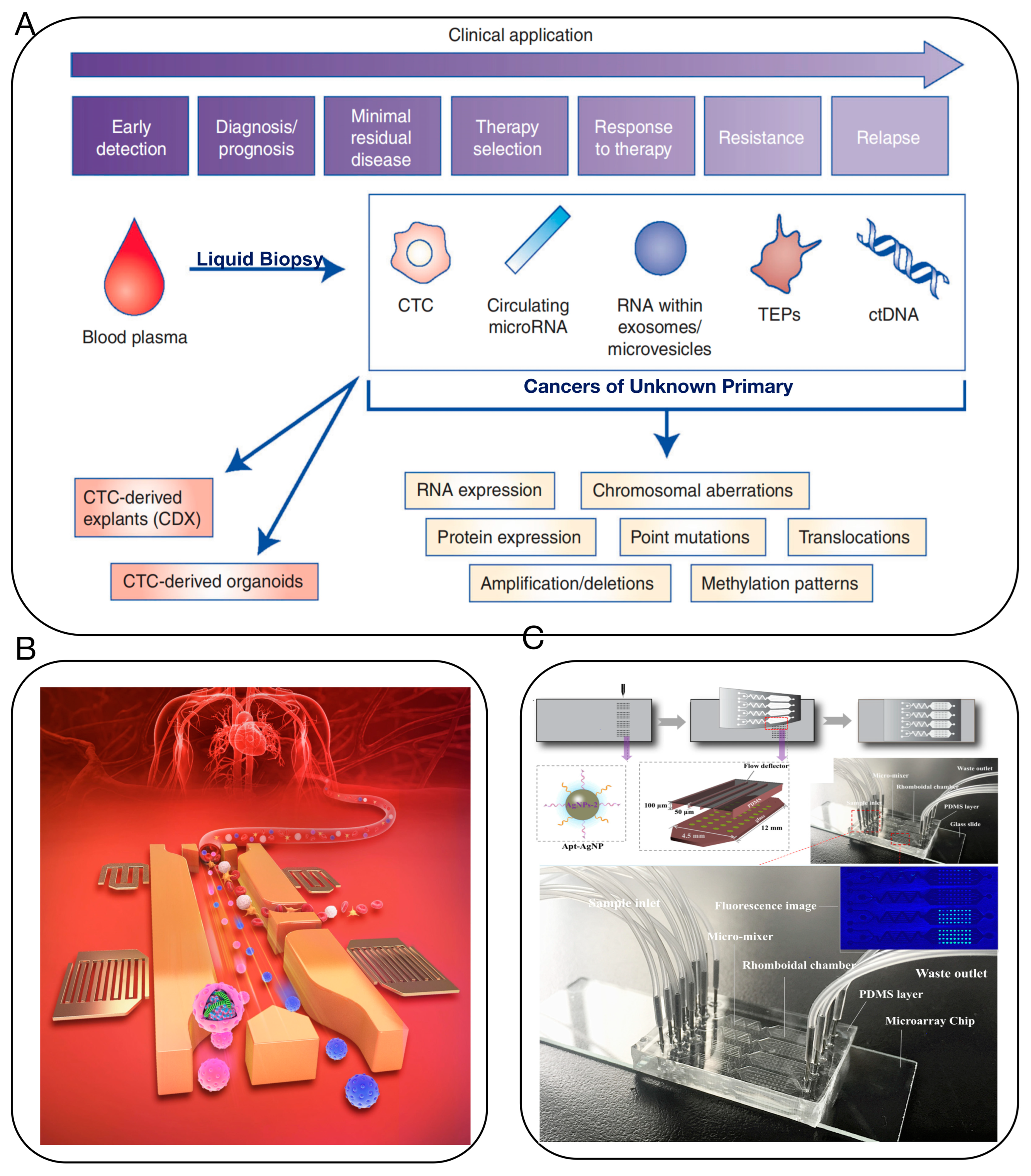
2.2.1. Liquid Biopsy
2.2.2. Artificial Intelligence (AI)
2.3. In Situ Targeting Self-Assembling Probe Technology
3. Targeted Treatment Strategies for CUP
3.1. Molecular Targeted Therapy
3.2. Immunotherapy
3.3. Self-Assembling Biological Nanotechnology
4. Challenges and Future Perspectives
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Pavlidis, N.; Pentheroudakis, G. Cancer of unknown primary site. Lancet 2012, 379, 1428–1435. [Google Scholar] [CrossRef]
- Massard, C.; Loriot, Y.; Fizazi, K. Carcinomas of an unknown primary origin—Diagnosis and treatment. Nat. Rev. Clin. Oncol. 2011, 8, 701–710. [Google Scholar] [CrossRef]
- Pavlidis, N.; Fizazi, K. Cancer of unknown primary (CUP). Crit. Rev. Oncol. Hematol. 2005, 54, 243–250. [Google Scholar] [CrossRef]
- Pavlidis, N.; Briasoulis, E.; Hainsworth, J.; Greco, F.A. Diagnostic and therapeutic management of cancer of an unknown primary. Eur. J. Cancer 2003, 39, 1990–2005. [Google Scholar] [CrossRef]
- Rassy, E.; Pavlidis, N. The currently declining incidence of cancer of unknown primary. Cancer Epidemiol. 2019, 61, 139–141. [Google Scholar] [CrossRef]
- Hemminki, K.; Bevier, M.; Hemminki, A.; Sundquist, J. Survival in cancer of unknown primary site: Population-based analysis by site and histology. Ann. Oncol. 2012, 23, 1854–1863. [Google Scholar] [CrossRef]
- Rassy, E.; Assi, T.; Pavlidis, N. Exploring the biological hallmarks of cancer of unknown primary: Where do we stand today? Br. J. Cancer 2020, 122, 1124–1132. [Google Scholar] [CrossRef] [PubMed]
- Greco, F.A.; Oien, K.; Erlander, M.; Osborne, R.; Varadhachary, G.; Bridgewater, J.; Cohen, D.; Wasan, H. Cancer of unknown primary: Progress in the search for improved and rapid diagnosis leading toward superior patient outcomes. Ann. Oncol. 2012, 23, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Rassy, E.; Kattan, J.; Pavlidis, N. Familial cancer of unknown primary. Int. J. Clin. Oncol. 2019, 24, 1328–1331. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, N.; Khaled, H.; Gaafar, R. A mini review on cancer of unknown primary site: A clinical puzzle for the oncologists. J. Adv. Res. 2015, 6, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Tanizaki, J.; Yonemori, K.; Akiyoshi, K.; Minami, H.; Ueda, H.; Takiguchi, Y.; Miura, Y.; Segawa, Y.; Takahashi, S.; Iwamoto, Y.; et al. Open-label phase II study of the efficacy of nivolumab for cancer of unknown primary. Ann. Oncol. 2022, 33, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Greco, F.A. Improved diagnosis, therapy and outcomes for patients with CUP. Nat. Rev. Clin. Oncol. 2017, 14, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Alshareeda, A.T.; Al-Sowayan, B.S.; Alkhani, R.R.; Aldosari, S.M.; Al Subayyil, A.M.; Alghuwainem, A. Cancer of unknown primary site: Real entity or misdiagnosed disease? J. Cancer 2020, 11, 3919–3931. [Google Scholar] [CrossRef] [PubMed]
- Michuda, J.; Breschi, A.; Kapilivsky, J.; Manghnani, K.; McCarter, C.; Hockenberry, A.J.; Mineo, B.; Igartua, C.; Dudley, J.T.; Stumpe, M.C.; et al. Validation of a transcriptome-based assay for classifying cancers of unknown primary origin. Mol. Diagn. Ther. 2023, 27, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Zaun, G.; Weber, M.; Metzenmacher, M.; Wiesweg, M.; Hilser, T.; Zaun, Y.; Liffers, S.; Pogorzelski, M.; Virchow, I.; Eberhardt, W.; et al. SUVmax Above 20 in 18F-FDG PET/CT at Initial Diagnostic Workup Associates with Favorable Survival in Patients with Cancer of Unknown Primary. J. Nucl. Med. 2023, 64, 1191–1194. [Google Scholar] [CrossRef] [PubMed]
- Cavo, M.; Terpos, E.; Nanni, C.; Moreau, P.; Lentzsch, S.; Zweegman, S.; Hillengass, J.; Engelhardt, M.; Usmani, S.Z.; Vesole, D.H.; et al. Role of 18F-FDG PET/CT in the diagnosis and management of multiple myeloma and other plasma cell disorders: A consensus statement by the International Myeloma Working Group. Lancet Oncol. 2017, 18, E206–E217. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Becker, A.S.; Do, R.K.G.; Schöder, H.; Hricak, H.; Vargas, H.A. Impact of 18F-Fluorodeoxyglucose positron emission tomography on management of cancer of unknown primary: Systematic review and meta-analysis. Eur. J. Cancer 2021, 159, 60–77. [Google Scholar] [CrossRef]
- Girard, A.; Reyes, H.V.; Shaish, H.; Grellier, J.F.; Dercle, L.; Salaun, P.Y.; Delcroix, O.; Rouanne, M. The Role of 18F-FDG PET/CT in Guiding Precision Medicine for Invasive Bladder Carcinoma. Front. Oncol. 2020, 10, 565086. [Google Scholar] [CrossRef]
- Witjes, J.A.; Babjuk, M.; Bellmunt, J.; Bruins, H.M.; De Reijke, T.M.; De Santis, M.; Gillessen, S.; James, N.; Maclennan, S.; Palou, J.; et al. Corrigendum to ‘EAU-ESMO Consensus statements on the management of advanced and variant bladder cancer-an international collaborative multistakeholder effort under the auspices of the EAU-ESMO Guidelines Committees’. Eur. Urol. 2020, 78, E48–E50. [Google Scholar] [CrossRef]
- Bentestuen, M.; Al-Obaydi, N.; Zacho, H.D. FAPI-avid nonmalignant PET/CT findings: An expedited systematic review. Semin Nucl. Med. 2023, 53, 694–705. [Google Scholar] [CrossRef]
- Kessler, L.; Ferdinandus, J.; Hirmas, N.; Zarrad, F.; Nader, M.; Kersting, D.; Weber, M.; Kazek, S.; Sraieb, M.; Hamacher, R.; et al. Pitfalls and common findings in 68Ga-FAPI PET: A pictorial analysis. J. Nucl. Med. 2022, 63, 890–896. [Google Scholar] [CrossRef]
- Eshet, Y.; Tau, N.; Apter, S.; Nissan, N.; Levanon, K.; Bernstein-Molho, R.; Globus, O.; Itay, A.; Shapira, T.; Oedegaard, C.; et al. The role of 68Ga-FAPI PET/CT in detection of metastatic lobular breast cancer. Clin. Nucl. Med. 2023, 48, 228–232. [Google Scholar] [CrossRef]
- Serfling, S.; Zhi, Y.; Schirbel, A.; Lindner, T.; Meyer, T.; Gerhard-Hartmann, E.; Lapa, C.; Hagen, R.; Hackenberg, S.; Buck, A.K.; et al. Improved cancer detection in Waldeyer’s tonsillar ring by 68Ga-FAPI PET/CT imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.P.; Pan, Q.Q.; Zhang, W. IgG4-related disease revealed by 68Ga-FAPI and 18F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2625–2626. [Google Scholar] [CrossRef] [PubMed]
- Posner, A.; Sivakumaran, T.; Pattison, A.; Etemadmoghadam, D.; Thio, N.; Wood, C.; Fisher, K.; Webb, S.; DeFazio, A.; Wilcken, N.; et al. Immune and genomic biomarkers of immunotherapy response in cancer of unknown primary. J. Immunother. Cancer 2023, 11, e005809. [Google Scholar] [CrossRef] [PubMed]
- Clynick, B.; Dessauvagie, B.; Sterrett, G.; Harvey, N.T.; Allcock, R.J.N.; Saunders, C.; Erber, W.; Meehan, K. Genetic characterisation of molecular targets in carcinoma of unknown primary. J. Transl. Med. 2018, 16, 185. [Google Scholar] [CrossRef]
- Zhang, S.; He, S.; Zhu, X.; Wang, Y.; Xie, Q.; Song, X.; Xu, C.; Wang, W.; Xing, L.; Xia, C.; et al. DNA methylation profiling to determine the primary sites of metastatic cancers using formalin-fixed paraffin-embedded tissues. Nat. Commun. 2023, 14, 5686. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.H.; Foster, N.R.; Meyers, J.P.; Steen, P.D.; Visscher, D.W.; Pillai, R.; Prow, D.M.; Reynolds, C.M.; Marchello, B.T.; Mowat, R.B.; et al. Gene expression profiling identifies responsive patients with cancer of unknown primary treated with carboplatin, paclitaxel, and everolimus: NCCTG N0871 (alliance). Ann. Oncol. 2016, 27, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Posner, A.; Prall, O.W.; Sivakumaran, T.; Etemadamoghadam, D.; Thio, N.; Pattison, A.; Balachander, S.; Fisher, K.; Webb, S.; Wood, C.; et al. A comparison of DNA sequencing and gene expression profiling to assist tissue of origin diagnosis in cancer of unknown primary. J. Pathol. 2023, 259, 81–92. [Google Scholar] [CrossRef]
- Laprovitera, N.; Riefolo, M.; Porcellini, E.; Durante, G.; Garajova, I.; Vasuri, F.; Aigelsreiter, A.; Dandachi, N.; Benvenuto, G.; Agostinis, F.; et al. MicroRNA expression profiling with a droplet digital PCR assay enables molecular diagnosis and prognosis of cancers of unknown primary. Mol. Oncol. 2021, 15, 2732–2751. [Google Scholar] [CrossRef]
- Rosenwald, S.; Gilad, S.; Benjamin, S.; Lebanony, D.; Dromi, N.; Faerman, A.; Benjamin, H.; Tamir, R.; Ezagouri, M.; Goren, E.; et al. Validation of a microRNA-based qRT-PCR test for accurate identification of tumor tissue origin. Mod. Pathol. 2010, 23, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Erlander, M.G.; Ma, X.J.; Kesty, N.C.; Bao, L.; Salunga, R.; Schnabel, C.A. Performance and clinical evaluation of the 92-gene real-time PCR assay for tumor classification. J. Mol. Diagn. 2011, 13, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Lorkowski, S.W.; Dermawan, J.K.; Rubin, B.P. The practical utility of AI-assisted molecular profiling in the diagnosis and management of cancer of unknown primary: An updated review. Virchows Arch. 2023, 177. [Google Scholar] [CrossRef]
- Li, W.; Liu, J.B.; Hou, L.K.; Yu, F.; Zhang, J.; Wu, W.; Tang, X.M.; Sun, F.; Lu, H.M.; Deng, J.; et al. Liquid biopsy in lung cancer: Significance in diagnostics, prediction, and treatment monitoring. Mol. Cancer 2022, 21, 25. [Google Scholar] [CrossRef] [PubMed]
- Lone, S.N.; Nisar, S.; Masoodi, T.; Singh, M.; Rizwan, A.; Hashem, S.; El-Rifai, W.; Bedognetti, D.; Batra, S.K.; Haris, M.; et al. Liquid biopsy: A step closer to transform diagnosis, prognosis and future of cancer treatments. Mol. Cancer 2022, 21, 79. [Google Scholar] [CrossRef]
- Conway, A.M.; Mitchell, C.; Kilgour, E.; Brady, G.; Dive, C.; Cook, N. Molecular characterisation and liquid biomarkers in Carcinoma of Unknown Primary (CUP): Taking the ‘U’ out of ‘CUP’. Br. J. Cancer 2019, 120, 141–153. [Google Scholar] [CrossRef]
- Wu, M.X.; Ouyang, Y.S.; Wang, Z.Y.; Zhang, R.; Huang, P.H.; Chen, C.Y.; Li, H.; Li, P.; Quinn, D.; Dao, M.; et al. Isolation of exosomes from whole blood by integrating acoustics and microfluidics. Proc. Natl. Acad. Sci. USA 2020, 117, 28525. [Google Scholar] [CrossRef]
- Liu, X.H.; Li, H.; Zhao, Y.J.; Yu, X.D.; Xu, D.K. Multivalent aptasensor array and silver aggregated amplification for multiplex detection in microfluidic devices. Talanta 2018, 188, 417–422. [Google Scholar] [CrossRef]
- Laprovitera, N.; Salamon, I.; Gelsomino, F.; Porcellini, E.; Riefolo, M.; Garonzi, M.; Tononi, P.; Valente, S.; Sabbioni, S.; Fontana, F.; et al. Genetic characterization of cancer of unknown primary using liquid biopsy approaches. Front. Cell Dev. Biol. 2021, 9, 1346. [Google Scholar] [CrossRef]
- Kato, S.; Krishnamurthy, N.; Banks, K.C.; De, P.; Williams, K.; Williams, C.; Leyland-Jones, B.; Lippman, S.M.; Lanman, R.B.; Kurzrock, R. Utility of genomic analysis in circulating tumor DNA from patients with carcinoma of unknown primary. Cancer Res. 2017, 77, 4238–4246. [Google Scholar] [CrossRef]
- Tanaka, H.; Suzuki, M.; Takemoto, N.; Fukusumi, T.; Eguchi, H.; Takai, E.; Kanai, H.; Tatsumi, M.; Horie, M.; Takenaka, Y.; et al. Performance of oral HPV DNA, oral HPV mRNA and circulating tumor HPV DNA in the detection of HPV-related oropharyngeal cancer and cancer of unknown primary. Int. J. Cancer 2022, 150, 174–186. [Google Scholar] [CrossRef]
- Wang, Y.H.; Song, Z.; Hu, X.Y.; Wang, H.S. Circulating tumor DNA analysis for tumor diagnosis. Talanta 2021, 228, 122220. [Google Scholar] [CrossRef]
- El Rassy, E.; Khaled, H.; Pavlidis, N. Liquid biopsy: A new diagnostic, predictive and prognostic window in cancers of unknown primary. Eur. J. Cancer 2018, 105, 28–32. [Google Scholar] [CrossRef]
- Cohen, J.D.; Javed, A.A.; Thoburn, C.; Wong, F.; Tie, J.; Gibbs, P.; Schmidt, C.M.; Yip-Schneider, M.T.; Allen, P.J.; Schattner, M.; et al. Combined circulating tumor DNA and protein biomarker-based liquid biopsy for the earlier detection of pancreatic cancers. Proc. Natl. Acad. Sci. USA 2017, 114, 10202–10207. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J.; Crown, J. Circulating tumor DNA (ctDNA): Can it be used as a pan-cancer early detection test? Crit. Rev. Clin. Lab. Sci. 2023, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Liang, T.; Qin, X.; Zhang, Y.; Yang, Y.; Chen, Y.; Yuan, L.; Liu, F.; Chen, Z.; Li, X.; Yang, F. CRISPR/dCas9-Mediated Specific Molecular Assembly Facilitates Genotyping of Mutant Circulating Tumor DNA. Anal. Chem. 2023, 95, 16305–16314. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Wu, S.; Wang, Y.; Shi, D. Circulating tumor cell isolation for cancer diagnosis and prognosis. EBioMedicine 2022, 83, 104237. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhou, X.; He, M.; Shang, Y.; Tetlow, A.L.; Godwin, A.K.; Zeng, Y. Ultrasensitive detection of circulating exosomes with a 3D-nanopatterned microfluidic chip. Nat. Biomed. Eng. 2019, 3, 438–451. [Google Scholar] [CrossRef] [PubMed]
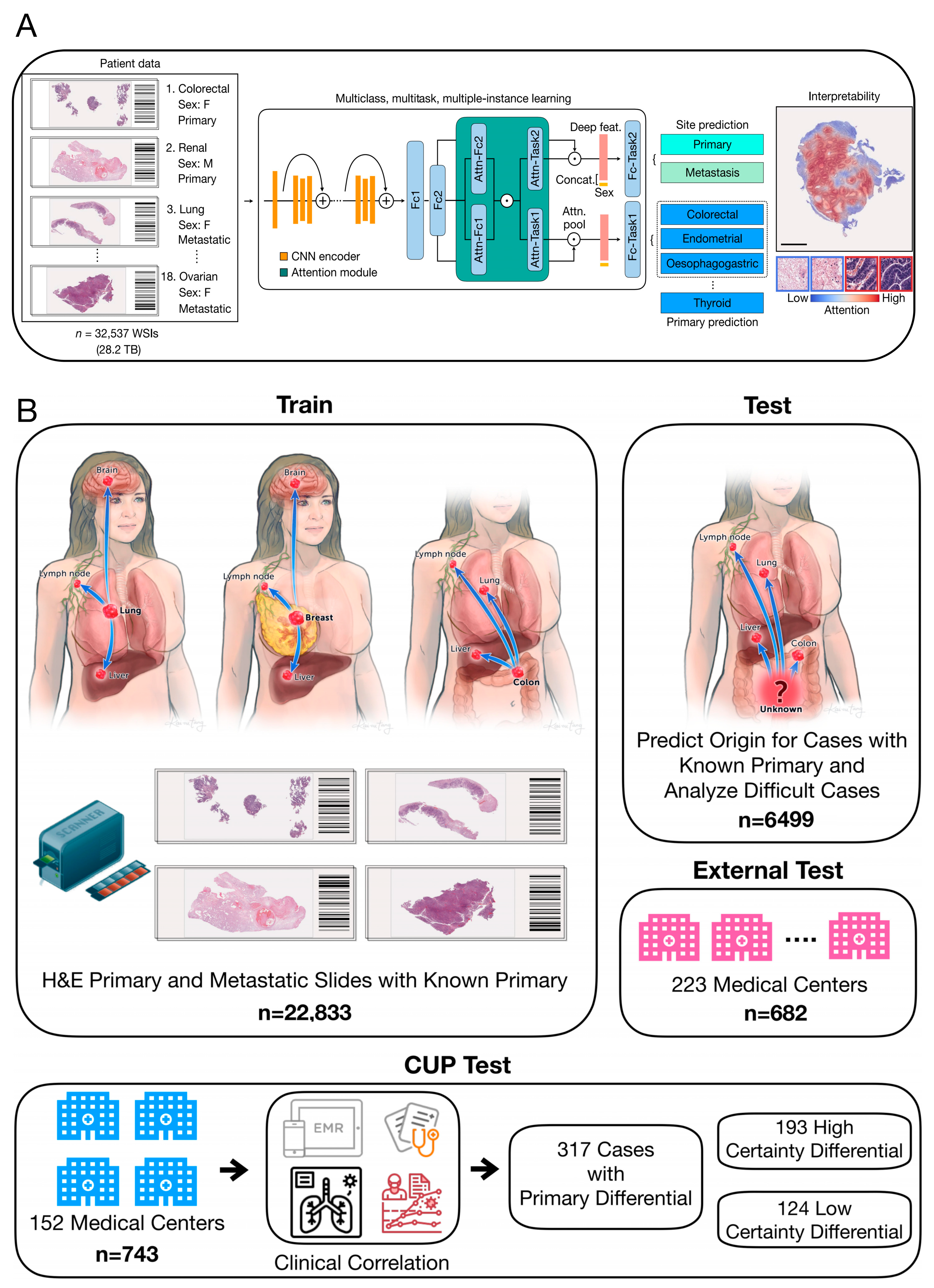
- Lu, M.Y.; Chen, T.Y.; Williamson, D.F.K.; Zhao, M.; Shady, M.; Lipkova, J.; Mahmood, F. AI-based pathology predicts origins for cancers of unknown primary. Nature 2021, 594, 106–110. [Google Scholar] [CrossRef] [PubMed]
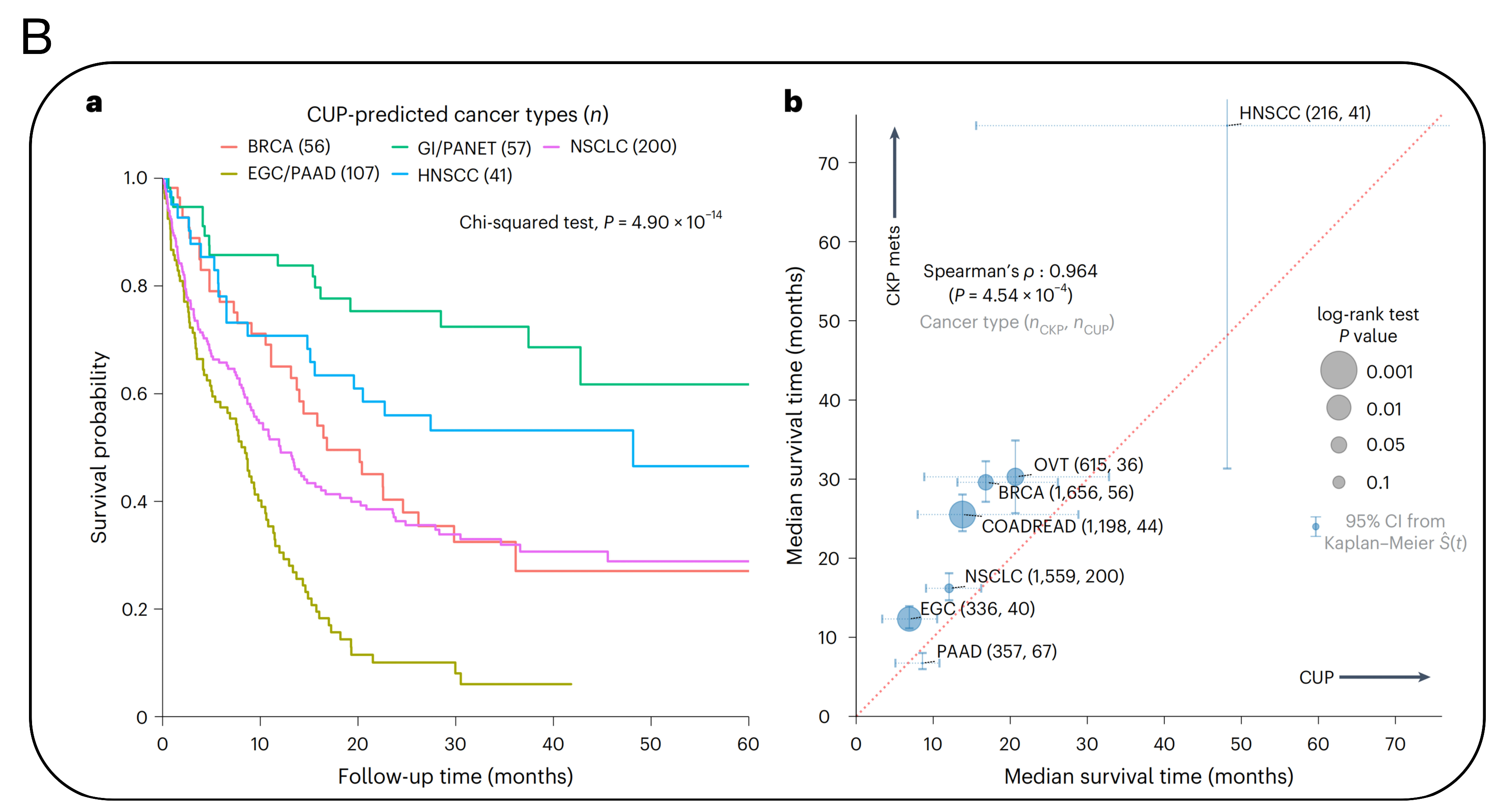
- Moon, I.; LoPiccolo, J.; Baca, S.C.; Sholl, L.M.; Kehl, K.L.; Hassett, M.J.; Liu, D.V.; Schrag, D.; Gusev, A. Machine learning for genetics-based classification and treatment response prediction in cancer of unknown primary. Nat. Med. 2023, 29, 2057–2067. [Google Scholar] [CrossRef]
- Xiao, Y.; Yu, D.H. Tumor microenvironment as a therapeutic target in cancer. Pharmacol. Ther. 2021, 221, 107753. [Google Scholar] [CrossRef] [PubMed]
- Pei, Z.F.; Lei, H.L.; Cheng, L. Bioactive inorganic nanomaterials for cancer theranostics. Chem. Soc. Rev. 2023, 52, 2031–2081. [Google Scholar] [CrossRef] [PubMed]
- Vincent, M.P.; Navidzadeh, J.O.; Bobbala, S.; Scott, E.A. Leveraging self-assembled nanobiomaterials for improved cancer immunotherapy. Cancer Cell 2022, 40, 255–276. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.H.; Huang, K.; Qin, Z.J.; Zeng, J.Y.; Zhang, Y.; Yin, L.H.; Liu, X.H.; Jiang, H.; Wang, X.M. Ultraprecise Real-Time Monitoring of Single Cells in Tumors in Response to Metal Ion-Mediated RNA Delivery. ACS Appl. Mater. Interfaces 2022, 14, 37291–37300. [Google Scholar] [CrossRef]
- Liu, H.; Liu, Z.M.; Wang, Y.H.; Xiao, J.; Liu, X.H.; Jiang, H.; Wang, X.M. Intracellular Liquid-Liquid Phase Separation Induces Tunable Anisotropic Nanocrystal Growth for Multidimensional Analysis. Adv. Funct. Mater. 2023, 33, 2302136. [Google Scholar] [CrossRef]
- Du, T.Y.; Qin, Z.J.; Zheng, Y.K.; Jiang, H.; Weizmann, Y.; Wang, X.M. The “Framework Exchange”-Strategy-Based MOF Platform for Biodegradable Multimodal Therapy. Chem 2019, 5, 2942–2954. [Google Scholar] [CrossRef]
- Wang, M.N.; Chen, Y.; Cai, W.J.; Feng, H.; Du, T.Y.; Liu, W.W.; Jiang, H.; Pasquarelli, A.; Weizmann, Y.; Wang, X.M. In situ self-assembling Au-DNA complexes for targeted cancer bioimaging and inhibition. Proc. Natl. Acad. Sci. USA 2020, 117, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Du, T.Y.; Shi, Z.W.; Qin, Z.J.; Hu, Y.W.; Zhu, Y.B.; Jiang, H.; Wang, X.M. Tailoring Photothermally Triggered Phase Transition of Multimodal Cascade Theranostics Platform by Spherical Nucleic Acids. Adv. Funct. Mater. 2022, 32, 2207410. [Google Scholar] [CrossRef]
- Kato, S.; Gumas, S.; Adashek, J.J.; Okamura, R.; Lee, S.; Sicklick, J.K.; Kurzrock, R. Multi-omic analysis in carcinoma of unknown primary (CUP): Therapeutic impact of knowing the unknown. Mol. Oncol. 2023, 14. [Google Scholar] [CrossRef]
- Kato, S.; Alsafar, A.; Walavalkar, V.; Hainsworth, J.; Kurzrock, R. Cancer of unknown primary in the molecular era. Trends Cancer 2021, 7, 465–477. [Google Scholar] [CrossRef]
- Huey, R.W.; Shah, A.T.; Reddi, H.V.; Dasari, P.; Topham, J.T.; Hwang, H.; Dhillon, N.; Willett, A.; Smaglo, B.G.; Estrella, J.S.; et al. Feasibility and value of genomic profiling in cancer of unknown primary: Real-world evidence from prospective profiling study. JNCI-J. Natl. Cancer Inst. 2023, 115, 994–997. [Google Scholar] [CrossRef]
- Binder, C.; Matthes, K.L.; Korol, D.; Rohrmann, S.; Moch, H. Cancer of unknown primary—Epidemiological trends and relevance of comprehensive genomic profiling. Cancer Med. 2018, 7, 4814–4824. [Google Scholar] [CrossRef]
- Olivier, T.; Fernandez, E.; Labidi-Galy, I.; Dietrich, P.Y.; Rodriguez-Bravo, V.; Baciarello, G.; Fizazi, K.; Patrikidou, A. Redefining cancer of unknown primary: Is precision medicine really shifting the paradigm? Cancer Treat. Rev. 2021, 97, 102204. [Google Scholar] [CrossRef]
- Westphalen, C.B.; Federer-Gsponer, J.; Pauli, C.; Karapetyan, A.R.; Chalabi, N.; Durán-Pacheco, G.; Beringer, A.; Bochtler, T.; Cook, N.; Höeglander, E.; et al. Baseline mutational profiles of patients with carcinoma of unknown primary origin enrolled in the CUPISCO study. ESMO Open 2023, 8, 102035. [Google Scholar] [CrossRef]
- Hayashi, H.; Takiguchi, Y.; Minami, H.; Akiyoshi, K.; Segawa, Y.; Ueda, H.; Iwamoto, Y.; Kondoh, C.; Matsumoto, K.; Takahashi, S.; et al. Site-specific and targeted therapy based on molecular profiling by next-generation sequencing for cancer of unknown primary site: A nonrandomized phase 2 clinical trial. JAMA Oncol. 2020, 6, 1931–1938. [Google Scholar] [CrossRef]
- Möhrmann, L.; Werner, M.; Oles, M.; Mock, A.; Uhrig, S.; Jahn, A.; Kreutzfeldt, S.; Fröhlich, M.; Hutter, B.; Paramasivam, N.; et al. Comprehensive genomic and epigenomic analysis in cancer of unknown primary guides molecularly-informed therapies despite heterogeneity. Nat. Commun. 2022, 13, 4485. [Google Scholar] [CrossRef]
- Ross, J.S.; Wang, K.; Gay, L.; Otto, G.A.; White, E.; Iwanik, K.; Palmer, G.; Yelensky, R.; Lipson, D.M.; Chmielecki, J.; et al. Comprehensive Genomic Profiling of Carcinoma of Unknown Primary Site: New Routes to Targeted Therapies. JAMA Oncol. 2015, 1, 40–49. [Google Scholar]
- Vlachostergios, P.J. Integrin signaling gene alterations and outcomes of cancer patients receiving immune checkpoint inhibitors. Am. J. Transl. Res. 2021, 13, 12386–12394. [Google Scholar] [PubMed]
- Rassy, E.; Boussios, S.; Pavlidis, N. Genomic correlates of response and resistance to immune checkpoint inhibitors in carcinomas of unknown primary. Eur. J. Clin. Investig. 2021, 51, e13583. [Google Scholar] [CrossRef]
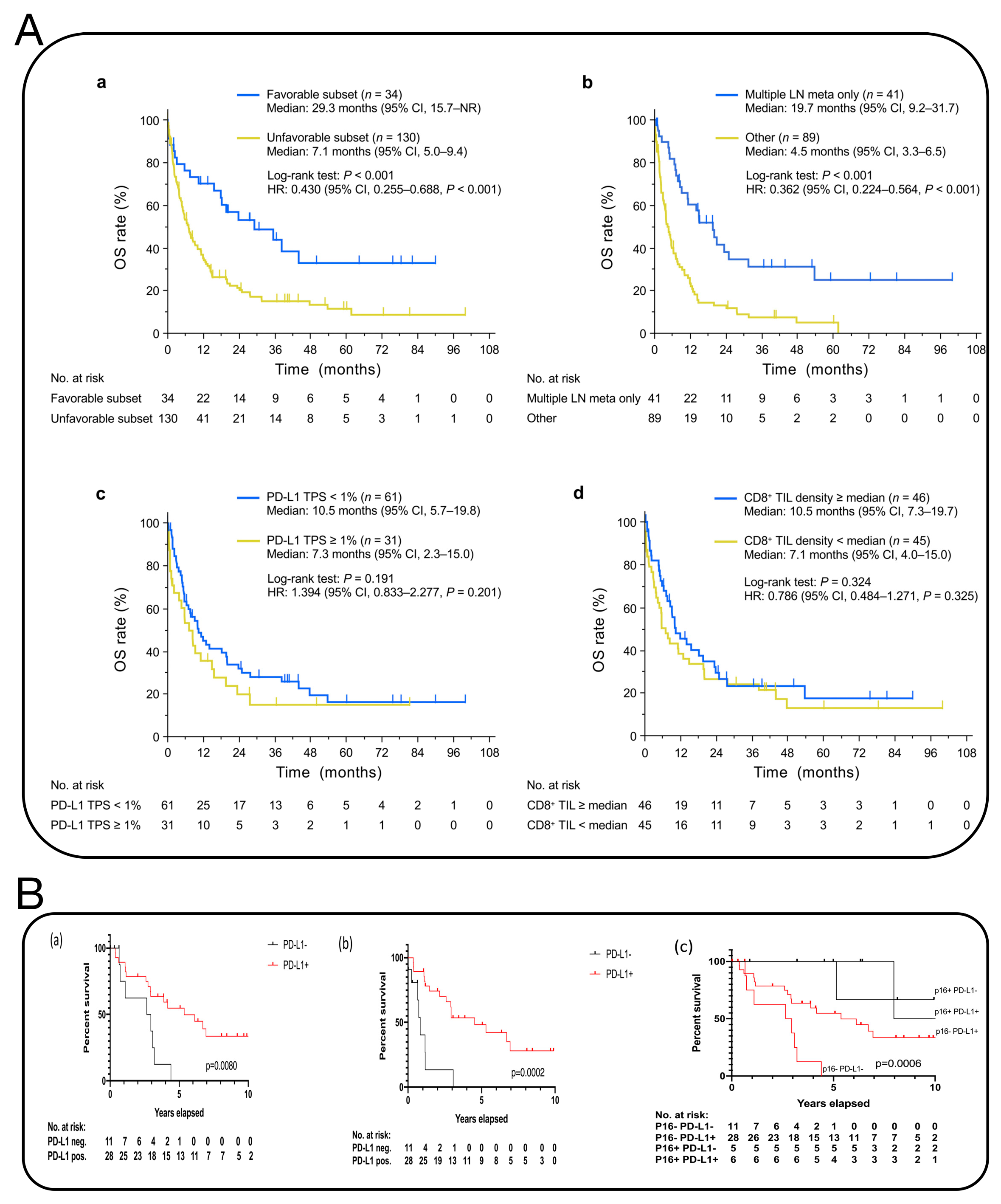
- Schmidl, B.; Vossenkämper, K.A.; Stark, L.; Boxberg, M.; Stögbauer, F.; Feigl, K.; Winter, C.; Pickhard, A.; Wollenberg, B.; Wirth, M. Comparison of PD-L1 expression in squamous cell cancer of unknown primary and oropharyngeal squamous cell carcinoma. Eur. Arch. Oto-Rhino-Laryngol. 2022, 280, 1991–1997. [Google Scholar] [CrossRef] [PubMed]
- Haratani, K.; Hayashi, H.; Takahama, T.; Nakamura, Y.; Tomida, S.; Yoshida, T.; Chiba, Y.; Sawada, T.; Sakai, K.; Fujita, Y.; et al. Clinical and immune profiling for cancer of unknown primary site. J. Immunother. Cancer 2019, 7, 251. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.J.; Zhang, X.G.; Cheng, L.L.; Liu, Y.D.; Chen, Y.; Jiang, Z.Z.; Liu, J. Multiple stimuli-responsive nanosystem for potent, ROS-amplifying, chemo-sonodynamic antitumor therapy. Bioact. Mater. 2022, 15, 355–371. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.Y.; Wang, X.W.; Li, J.X.; Hu, J.; Cheng, L.; Yang, X.L. ROS-based dynamic therapy synergy with modulating tumor cell-microenvironment mediated by inorganic nanomedicine. Coord. Chem. Rev. 2021, 437, 213828. [Google Scholar] [CrossRef]
- Zhang, H.J.; Chen, W.J.; Wang, J.; Du, W.X.; Wang, B.B.; Song, L.; Hu, Y.; Ma, X.P. A novel ROS-activable self-immolative prodrug for tumor-specific amplification of oxidative stress and enhancing chemotherapy of mitoxantrone. Biomaterials 2023, 293, 121954. [Google Scholar] [CrossRef]
- Xiong, H.J.; Ye, J.; Wang, M.N.; Wang, Y.H.; Liu, X.H.; Jiang, H.; Wang, X.M. In-situ bio-assembled specific Au NCs-Aptamer-Pyro conjugates nanoprobe for tumor imaging and mitochondria-targeted photodynamic therapy. Biosens. Bioelectron. 2022, 218, 114763. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.; Kim, Y.; Choi, M.; Lee, I.; Kim, E.; Yoon, C.G.; Pu, K.; Kang, H.M.; Kim, J.S. In situ self-assembly for cancer therapy and imaging. Nat. Rev. Mater. 2023, 8, 710–725. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Jiang, H.; Wang, X. Advances in Cancer Research: Current and Future Diagnostic and Therapeutic Strategies. Biosensors 2024, 14, 100. https://doi.org/10.3390/bios14020100
Liu X, Jiang H, Wang X. Advances in Cancer Research: Current and Future Diagnostic and Therapeutic Strategies. Biosensors. 2024; 14(2):100. https://doi.org/10.3390/bios14020100
Chicago/Turabian StyleLiu, Xiaohui, Hui Jiang, and Xuemei Wang. 2024. "Advances in Cancer Research: Current and Future Diagnostic and Therapeutic Strategies" Biosensors 14, no. 2: 100. https://doi.org/10.3390/bios14020100
APA StyleLiu, X., Jiang, H., & Wang, X. (2024). Advances in Cancer Research: Current and Future Diagnostic and Therapeutic Strategies. Biosensors, 14(2), 100. https://doi.org/10.3390/bios14020100