A Non-Invasive Hemoglobin Detection Device Based on Multispectral Photoplethysmography

 ,
,
Abstract
:1. Introduction
2. Principles and Methods
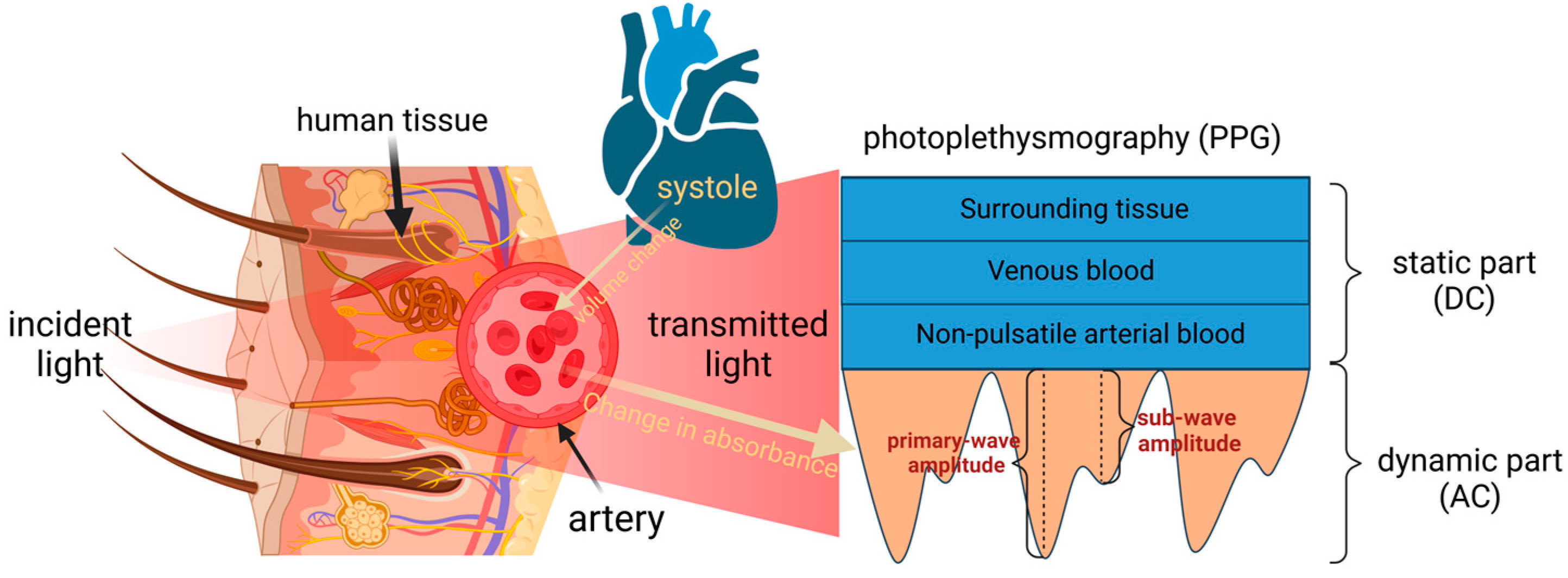
2.1. Theory of PPG
2.2. Lambert–Beer Law and Its Corollaries
3. System Composition
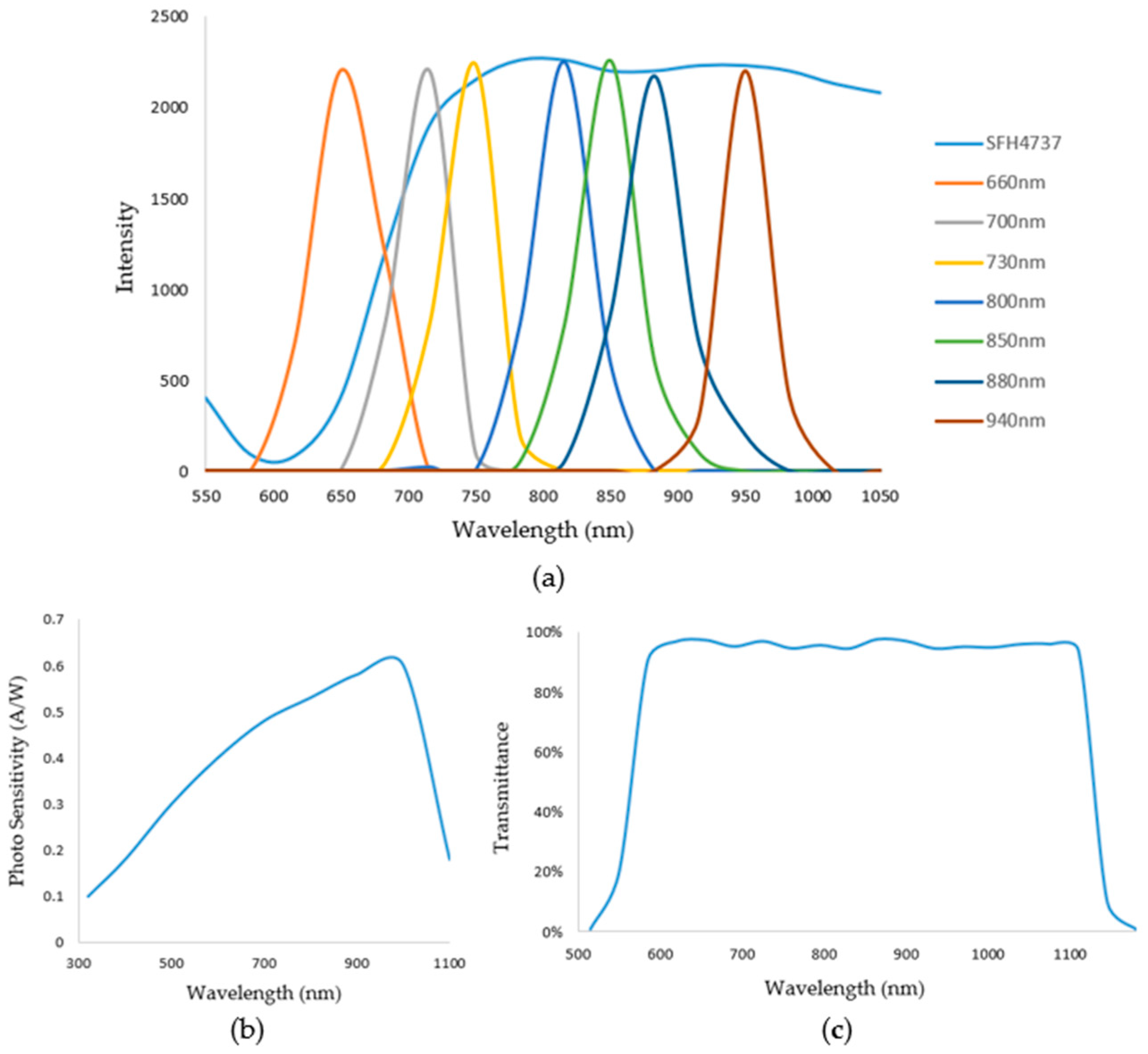
3.1. Hardware Component
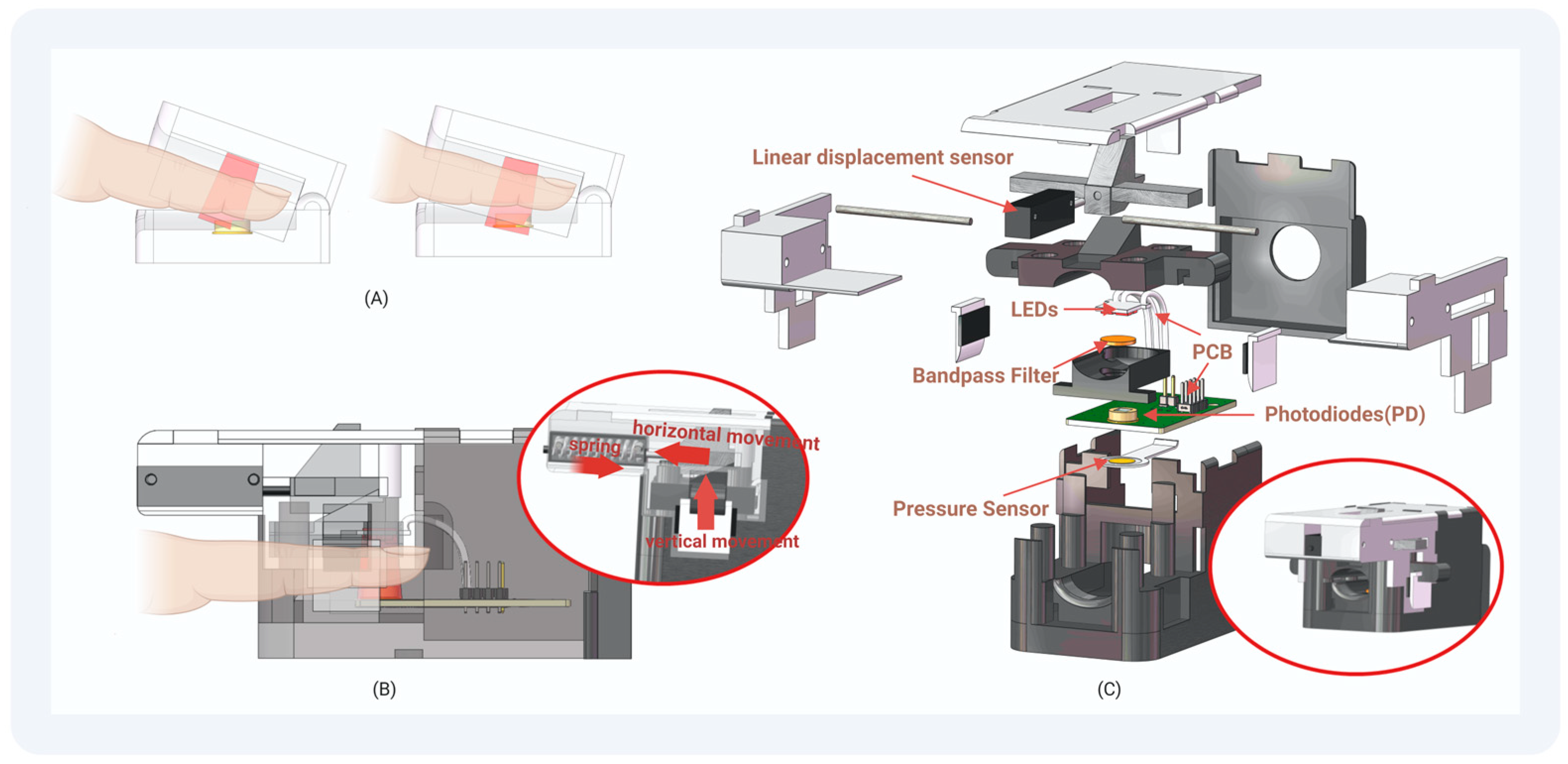
3.2. Design of Finger Clip
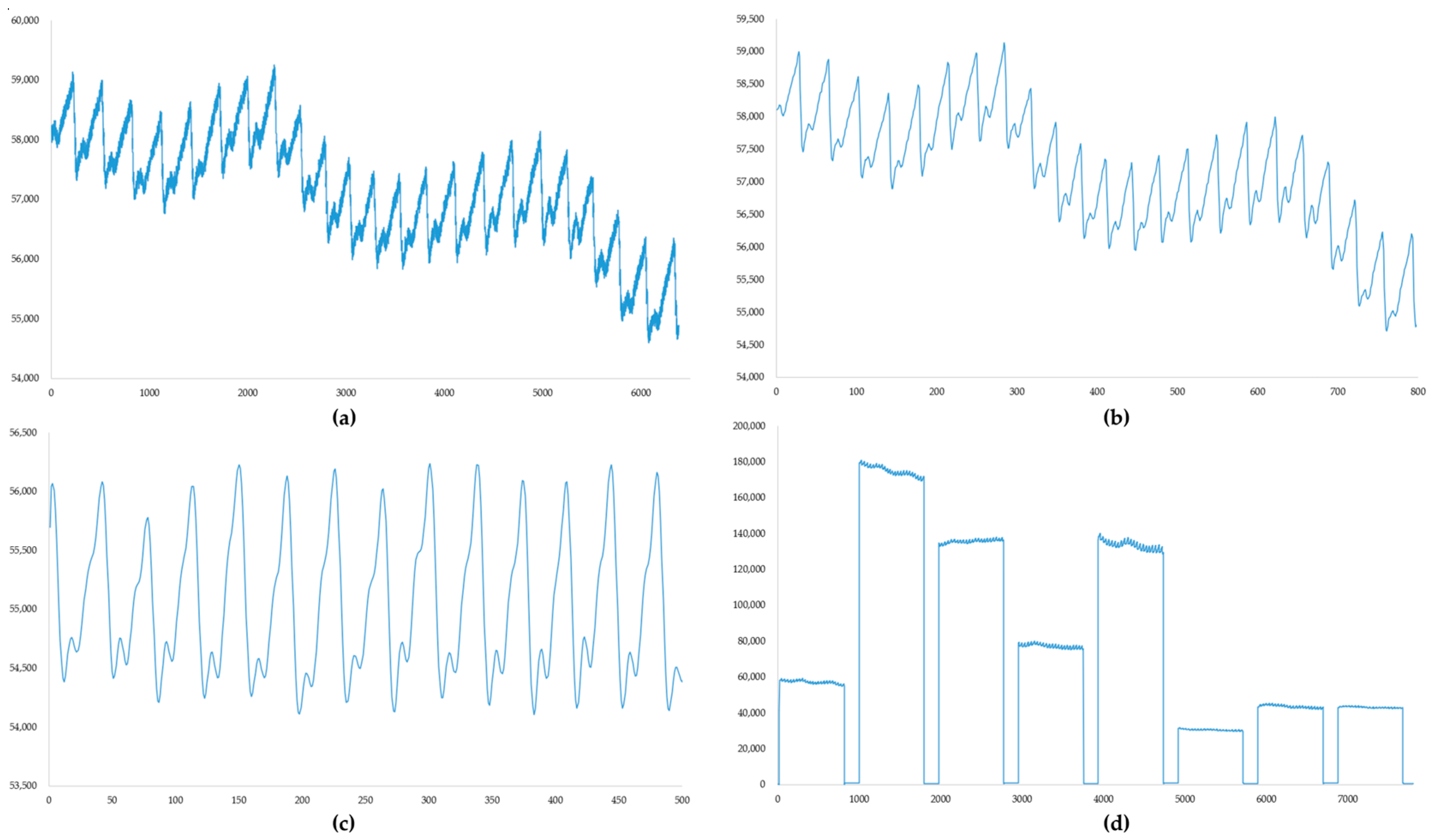
4. PPG Signal Processing and Indicators for Signal Quality Evaluation
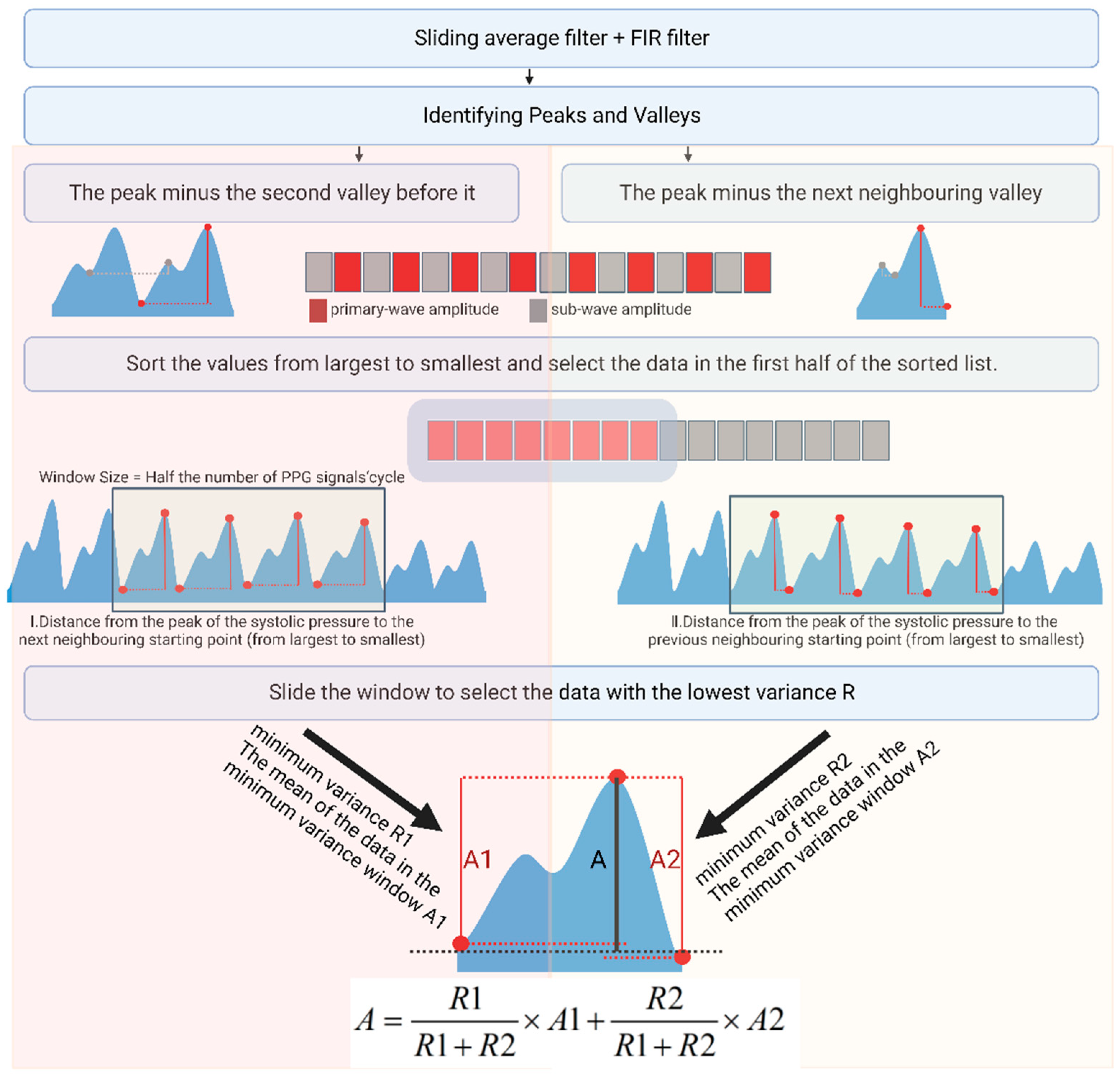
4.1. The Extraction Method for the PPG Signal Features
4.2. Signal Quality Evaluation Methods
5. Data Collection and Correlation Analysis
Data Collection
6. Results
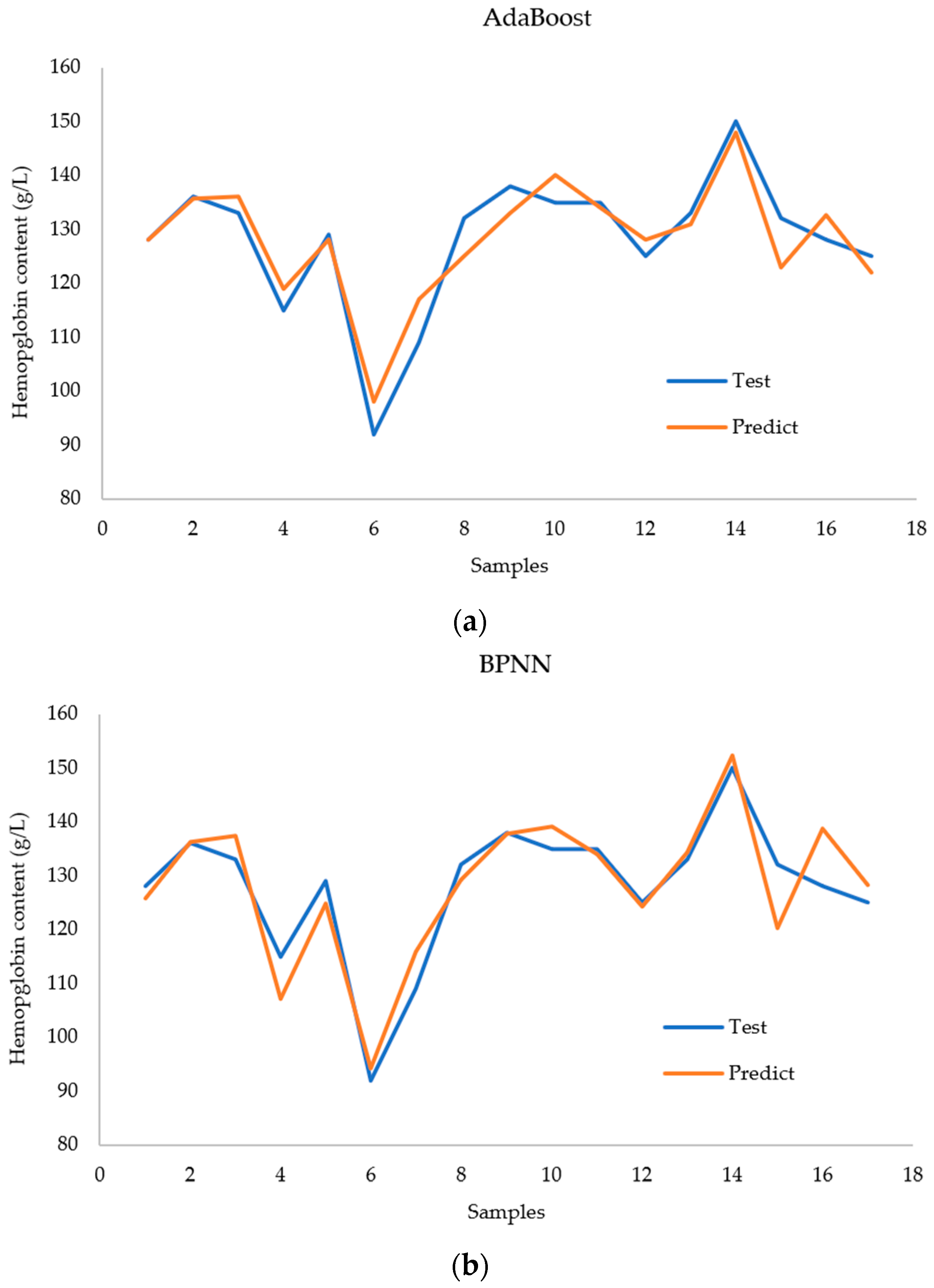
6.1. Models for Hemoglobin Level Predictions
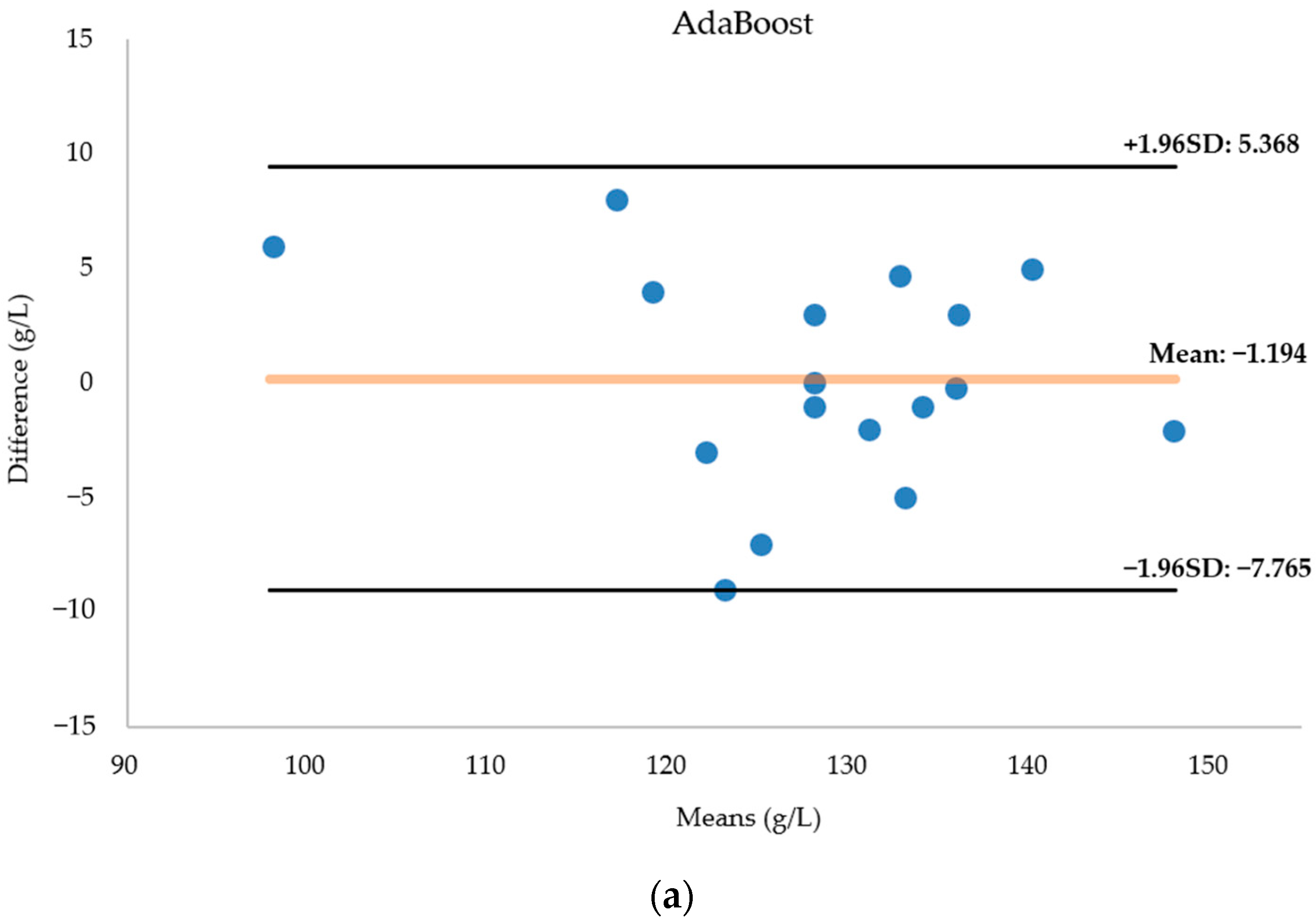
6.1.1. AdaBoost Regression
6.1.2. BP Neural Network
6.1.3. Random Forest Regression
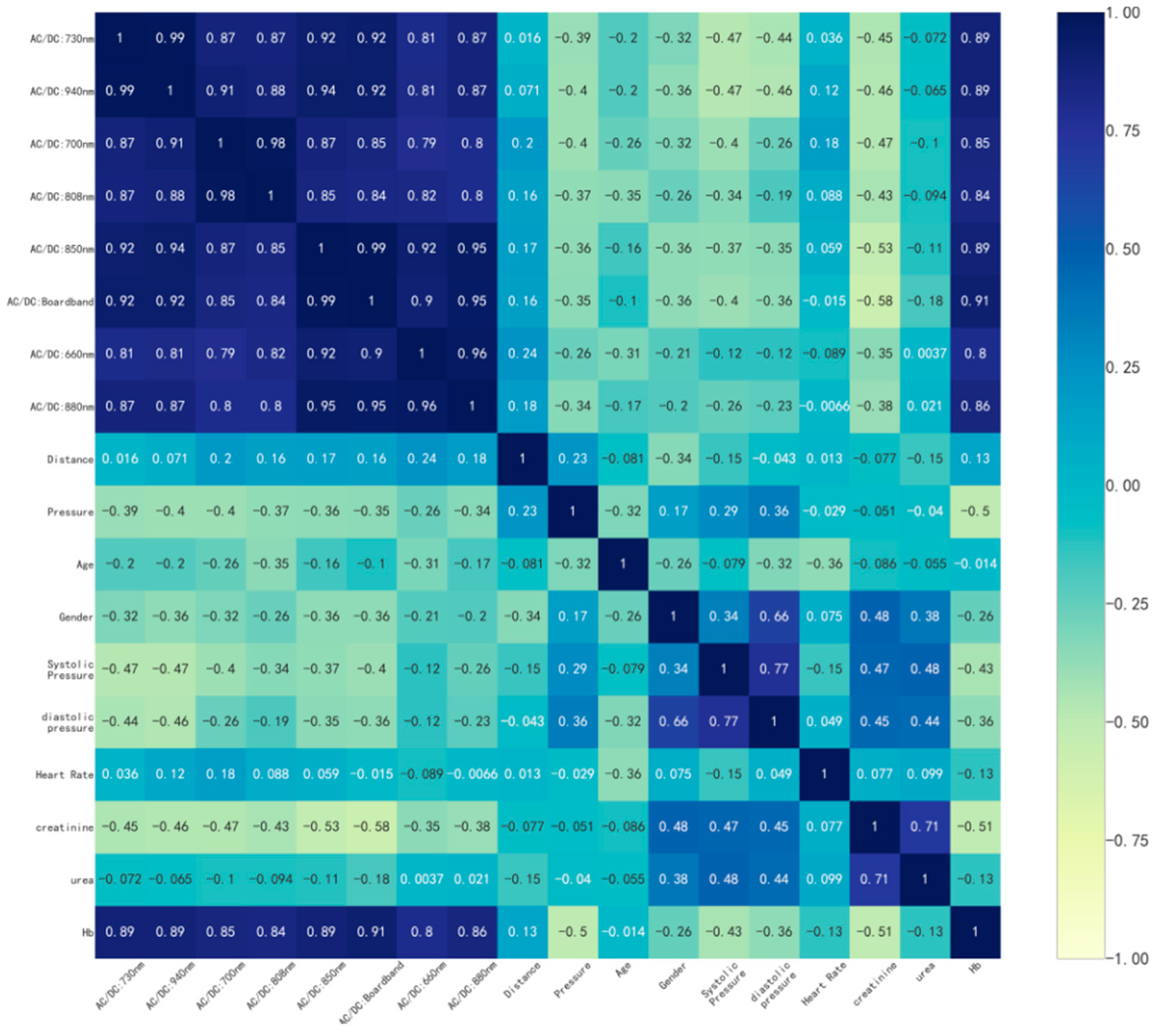
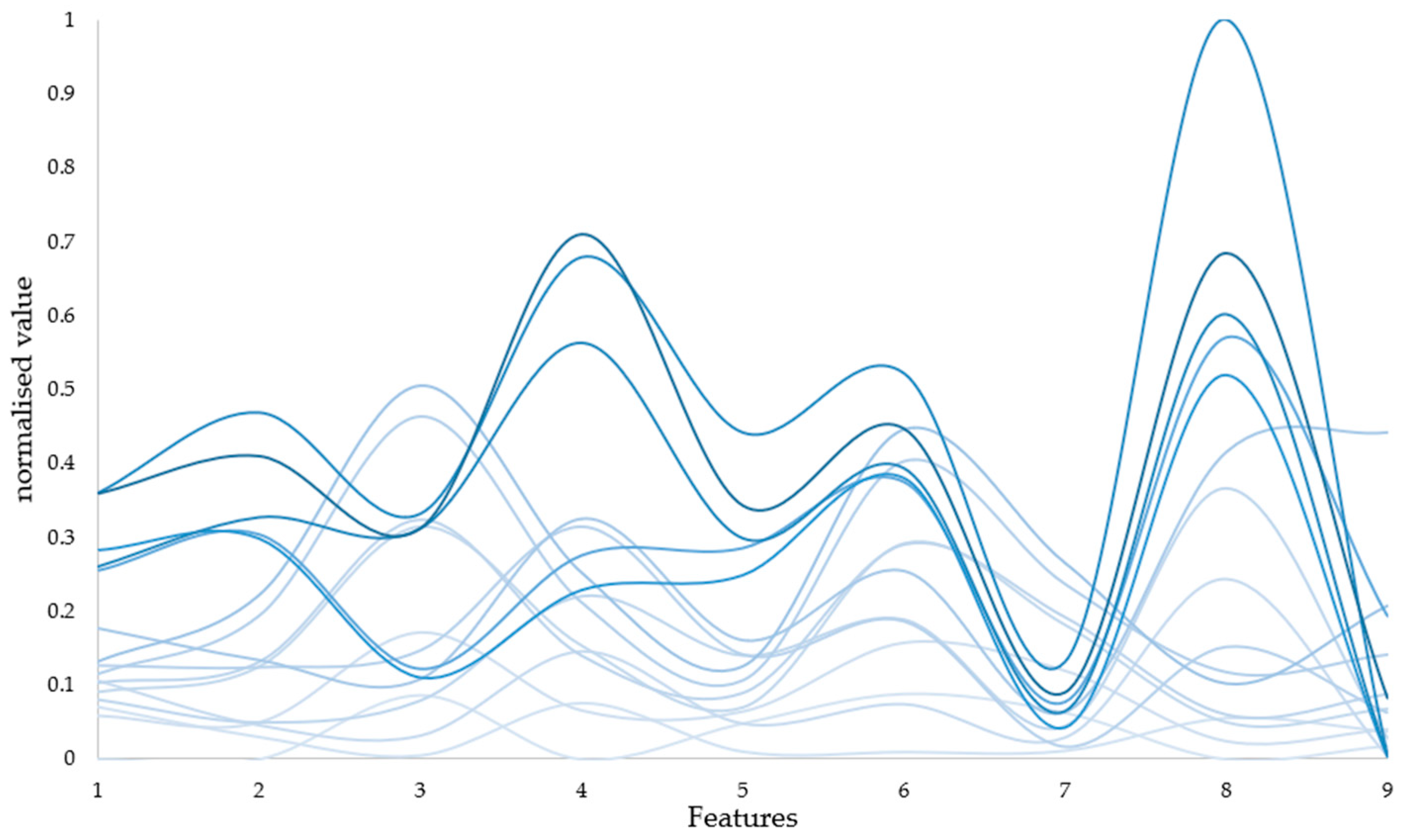
6.2. Correlation Analysis
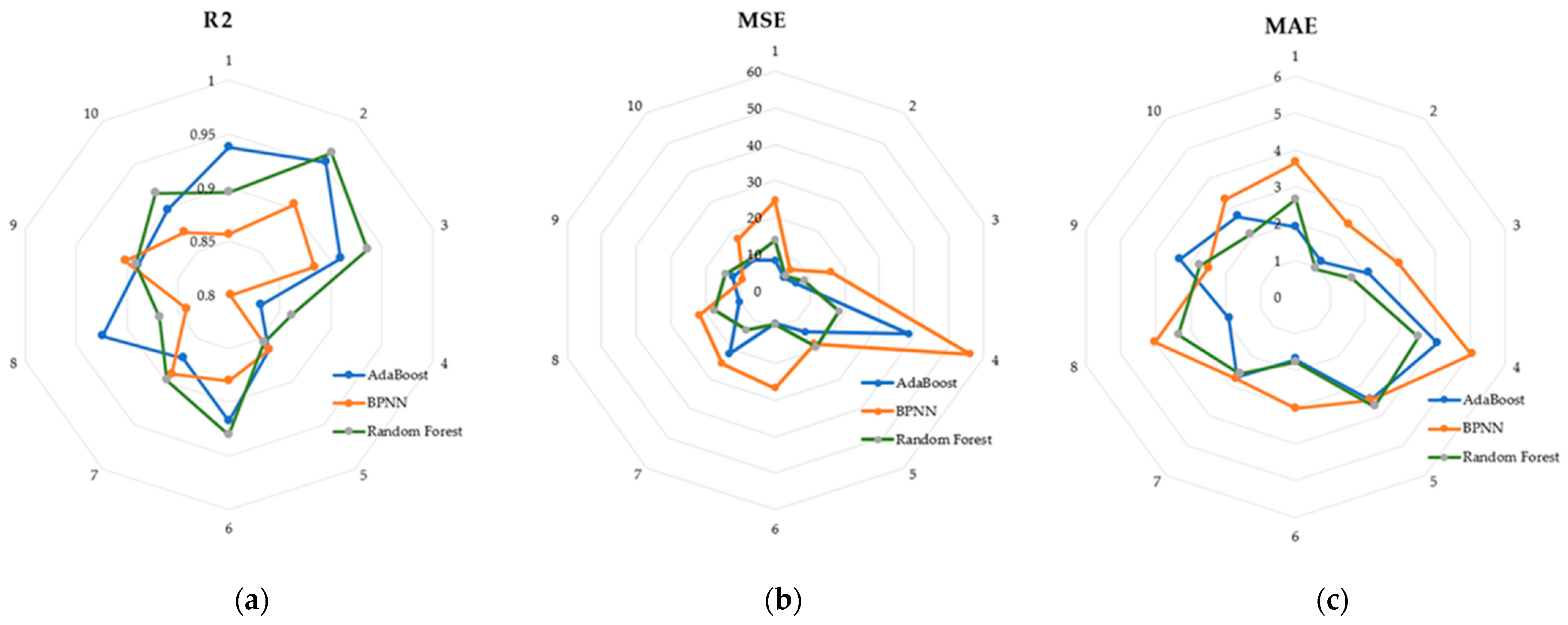
6.3. Performance Comparisons of the Models
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bell, S.G. An introduction to hemoglobin physiology. Neonatal Netw. 1999, 18, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Topal, M.; Guney, I. The association of soluble Klotho levels with anemia and hemoglobin variability in hemodialysis patients. Semin. Dial. 2023, 36, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Mutonhodza, B.; Dembedza, M.P.; Lark, M.R.; Joy, E.J.M.; Manzeke-Kangara, M.G.; Njovo, H.; Nyadzayo, T.K.; Kalimbira, A.A.; Bailey, E.H.; Broadley, M.R.; et al. Anemia in children aged 6-59 months was significantly associated with maternal anemia status in rural Zimbabwe. Food Sci. Nutr. 2023, 11, 1232–1246. [Google Scholar] [CrossRef] [PubMed]
- Noshiro, K.; Umazume, T.; Hattori, R.; Kataoka, S.; Yamada, T.; Watari, H. Hemoglobin Concentration during Early Pregnancy as an Accurate Predictor of Anemia during Late Pregnancy. Nutrients 2022, 14, 839. [Google Scholar] [CrossRef] [PubMed]
- Mannucci Tragodara, S.M.; Del Aguila Villar, C.M.; Rojas Gabulli, M.I.; Falen Boggio, J.M.; Lu de lama, L.R.; Nunez Almache, O.; Chavez Tejada, E.M.D.J.; Espinoza Robles, O.A.; Pinto Ibarcena, P.M.; Calagua Quispe, M.R.; et al. Anemia due to Iron Deficiency and Relationship with Glycosylated Hemoglobin Levels in Diabetic Children. Horm. Res. Paediatr. 2021, 93, 41. [Google Scholar]
- Napolitano, L.M. Vitamin D supplementation and hemoglobin: Dosing matters in prevention/treatment of anemia. Nutr. J. 2021, 20, 23. [Google Scholar] [CrossRef]
- Joseph, B.; Haider, A.; Rhee, P. Non-invasive hemoglobin monitoring. Int. J. Surg. 2016, 33, 254–257. [Google Scholar] [CrossRef]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1–R39. [Google Scholar] [CrossRef]
- Liu, A.; Li, G.; Yan, W.; Lin, L. Combined effects of PPG preprocess and dynamic spectrum extraction on predictive performance of non-invasive detection of blood components based on dynamic spectrum. Infrared Phys. Technol. 2018, 92, 436–442. [Google Scholar] [CrossRef]
- Conley, C.L. Pathophysiological Effects of Some Abnormal Hemoglobins. Medicine 1964, 43, 785–787. [Google Scholar] [CrossRef]
- Kumar, Y.; Dogra, A.; Kaushik, A.; Kumar, S. Progressive evaluation in spectroscopic sensors for non-invasive blood haemoglobin analysis—A review. Physiol. Meas. 2022, 43, 2. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Ding, H.; Gao, H.; Lu, Q. Research on improving the accuracy of near infrared non-invasive hemoglobin detection. Infrared Phys. Technol. 2015, 72, 117–121. [Google Scholar] [CrossRef]
- Ahsan, G.M.T.; Gani, M.O.; Hasan, M.K.; Ahamed, S.I.; Chu, W.; Adibuzzaman, M.; Field, J. A Novel Real-Time Non-Invasive Hemoglobin Level Detection Using Video Images from Smartphone Camera. In Proceedings of the 41st IEEE Annual Computer Software and Applications Conference (COMPSAC), Torino, Italy, 4–8 July 2017; pp. 967–972. [Google Scholar]
- Kesarwani, A.; Das, S.; Dalui, M.; Kisku, D.R.; Sen, B.; Roy, S.; Basu, A. Non-invasive anaemia detection by examining palm pallor: A smartphone-based approach. Biomed. Signal Process. Control 2023, 79, 104045. [Google Scholar] [CrossRef]
- Kumar, Y.; Dogra, A.; Shaw, V.; Kaushik, A.; Kumar, S. NIR-based Sensing System for Non-invasive Detection of Hemoglobin for Point-of-care Applications. Curr. Med. Imaging 2022, 18, 532–545. [Google Scholar] [CrossRef] [PubMed]
- Kavsaoglu, A.R.; Polat, K.; Hariharan, M. Non-invasive prediction of hemoglobin level using machine learning techniques with the PPG signal’s characteristics features. Appl. Soft Comput. 2015, 37, 983–991. [Google Scholar] [CrossRef]
- Kraitl, J.; Timm, U.; Ewald, H. Non-invasive measurement of blood and tissue parameters based on VIS-NIR spectroscopy. In Proceedings of the Conference on Optical Diagnostics and Sensing XIII—Toward Point-of-Care Diagnostics, San Francisco, CA, USA, 6 February 2013. [Google Scholar]
- Wieringa, F.P.; Mastik, F.; van der Steen, A.F.W. Contactless multiple wavelength photoplethysmographic imaging: A first step toward “SpO(2) camera” technology. Ann. Biomed. Eng. 2005, 33, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Landsman, M.L.; Kwant, G.; Mook, G.A.; Zijlstra, W.G. Light-absorbing properties, stability, and spectral stabilization of indocyanine green. J. Appl. Physiol. 1976, 40, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Reiser, M.; Breidenassel, A.; Amft, O.; IEEE. Simulation framework for reflective PPG signal analysis depending on sensor placement and wavelength. In Proceedings of the 4th IEEE-EMBS International Conference on Wearable and Implantable Body Sensor Networks (BSN)/18th IEEE-EMBS International Conference on Biomedical and Health Informatics (BHI), Ioannina, Greece, 27–30 September 2022. [Google Scholar]
- Teng, X.F.; Zhang, Y.T. The effect of contacting force on photoplethysmographic signals. Physiol. Meas. 2004, 25, 1323–1335. [Google Scholar] [CrossRef]
- Kumar, R.D.; Guruprasad, S.; Kansara, K.; Rao, K.N.R.; Mohan, M.; Reddy, M.R.; Prabhu, U.H.; Prakash, P.; Chakraborty, S.; Das, S.; et al. A Novel Noninvasive Hemoglobin Sensing Device for Anemia Screening. IEEE Sens. J. 2021, 21, 15318–15329. [Google Scholar] [CrossRef]
- Fan, W.; Stolfo, S.J.; Zhang, J.X.; Chan, P.K. AdaCost: Misclassification cost-sensitive boosting. In Proceedings of the 16th International Conference on Machine Learning (ICML 99), Bled, Slovenia, 27–30 June 1999; pp. 97–105. [Google Scholar]
- Zhu, J.; Zou, H.; Rosset, S.; Hastie, T. Multi-class AdaBoost. Stat. Its Interface 2009, 2, 349–360. [Google Scholar]
- Ramakrishna, M.T.; Venkatesan, V.K.; Izonin, I.; Havryliuk, M.; Bhat, C.R. Homogeneous Adaboost Ensemble Machine Learning Algorithms with Reduced Entropy on Balanced Data. Entropy 2023, 25, 245. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, G.; Zhao, Z.; Lin, L. Dynamic Spectrum and BP Neural Network for Non-invasive Hemoglobin Measurement. In Proceedings of the International Conference on Life System Modeling and Simulation/International Conference on Intelligent Computing for Sustainable Energy and Environment (LSMS-ICSEE), Wuxi, China, 17–20 September 2010; pp. 67–74. [Google Scholar]
- Ben, S.J.; Dorner, M.; Gunther, M.P.; von Kanel, R.; Euler, S. Proof of concept: Predicting distress in cancer patients using back propagation neural network (BPNN). Heliyon 2023, 9, e18328. [Google Scholar] [CrossRef] [PubMed]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Austin, A.M.; Ramkumar, N.; Gladders, B.; Barnes, J.A.; Eid, M.A.; Moore, K.O.; Feinberg, M.W.; Creager, M.A.; Bonaca, M.; Goodney, P.P. Using a cohort study of diabetes and peripheral artery disease to compare logistic regression and machine learning via random forest modeling. Bmc Med. Res. Methodol. 2022, 22, 300. [Google Scholar] [CrossRef] [PubMed]
- Rovetta, A. Raiders of the Lost Correlation: A Guide on Using Pearson and Spearman Coefficients to Detect Hidden Correlations in Medical Sciences. Cureus 2020, 12, e11794. [Google Scholar] [CrossRef]
- Chaila, M.Z.; Viniegra, M.; Gagliardino, J.J.; Martinez, A.; Simesen de Bielke, M.G.; Frusti, M.; Monaco, L.; Salgado, P.; Buso, C.; Gonzalez, C.D.; et al. Glycated Hemoglobin Measurement: Comparison of Three Methods Versus High Performance Liquid Chromatography. J. Diabetes Sci. Technol. 2022, 16, 724–731. [Google Scholar] [CrossRef]
- Zhu, W.W.; Yu, H.X.; Pu, Z.H.; Guo, Z.J.; Zheng, H.; Li, C.C.; Zhang, X.G.; Li, J.; Li, D.C. Effect of interstitial fluid pH on transdermal glucose extraction by reverse iontophoresis. Biosens. Bioelectron. 2023, 235, 115406. [Google Scholar] [CrossRef]
- Zhang, C.; Zhang, L.; Pu, Z.H.; Bao, B.; Ouyang, W.Y.; Li, D.C. Fabricating 1D stretchable fiber-shaped electronics based on inkjet printing technology for wearable applications. Nano Energy 2023, 113, 108574. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification Model | Recall Score * | Precision Score * | F1 Score * |
|---|---|---|---|
| AdaBoost | 0.83 | 0.75 | 0.79 |
| AdaCost | 0.94 | 0.89 | 0.92 |
| NO. | Hemoglobin Content (g/L) | Gender | Age | Blood Pressure (mmHg) Diastolic/Systolic | Heart Rate (BPM) | Creatinine (μmoI/L) | Urea (mmol/L) |
|---|---|---|---|---|---|---|---|
| 1 | 135 | Male | 23 | ||||
| 2 | 128 | Female | 25 | ||||
| 3 | 130 | Male | 72 | 129/80 | 70 | 94.8 | 8.09 |
| 4 | 136 | Male | 21 | ||||
| 5 | 110 | Male | 48 | 147/97 | 79 | 67.3 | 2.91 |
| 6 | 148.5 | Male | 26 | ||||
| 7 | 147.9 | Male | 36 | ||||
| 8 | 119 | Female | 30 | 165/107 | 70 | 173.8 | 8.92 |
| 9 | 136.5 | Male | 25 | ||||
| 10 | 117 | Male | 36 | 129/102 | 93 | 229.8 | 10.34 |
| 11 | 133 | Male | 24 | ||||
| 12 | 118 | Male | 38 | 160/98 | 75 | 360.2 | 27.17 |
| 13 | 92 | Male | 38 | ||||
| 14 | 125 | Female | 28 | ||||
| 15 | 133 | Female | 64 | 120/76 | 85 | 66.3 | 5.38 |
| 16 | 124 | Female | 55 | 155/84 | 63 | 61.1 | 5.16 |
| 17 | 106 | Male | 58 | 141/93 | 63 | 551.3 | 29.5 |
| 18 | 119 | Male | 24 | ||||
| 19 | 131 | Male | 26 | ||||
| 20 | 124 | Female | 25 | 120/80 | 86 | 90 | 4 |
| 21 | 150 | Male | 28 | ||||
| 22 | 88 | Male | 27 | 152/92 | 84 | 207.1 | 13.07 |
| 23 | 102.5 | Male | 48 | ||||
| 24 | 126 | Female | 26 | ||||
| 25 | 133 | Female | 24 | ||||
| 26 | 115 | Male | 40 | ||||
| 27 | 140 | Female | 41 | ||||
| 28 | 129.7 | Female | 30 | ||||
| 29 | 132.7 | Male | 24 | ||||
| 30 | 103 | Female | 33 | ||||
| 31 | 109 | Male | 30 | ||||
| 32 | 132 | Female | 24 | ||||
| 33 | 122 | Male | 36 | ||||
| 34 | 123 | Female | 39 | ||||
| 35 | 134.6 | Male | 25 | ||||
| 36 | 132 | Male | 26 | ||||
| 37 | 118 | Male | 35 | ||||
| 38 | 138 | Female | |||||
| 39 | 127 | Male | 26 | ||||
| 40 | 132 | Female | 23 | ||||
| 41 | 128 | Female | 39 | 117/63 | 70 | 67.3 | 2.91 |
| 42 | 129 | Female | 25 | ||||
| 43 | 128 | Female | 27 | ||||
| 44 | 138 | Male | 24 | 110/80 | 70 | 90 | 4 |
| 45 | 136 | Male | 27 | 155/110 | 60 | 178.4 | 9.04 |
| 46 | 133 | Male | 20 | 160/101 | 97 | 344.1 | 34.16 |
| 47 | 136 | Male | 36 | ||||
| 48 | 135 | Male | 24 | 110/80 | 88 | 90 | 4 |
| 49 | 125 | Female | 28 | ||||
| 50 | 125 | Female | |||||
| 51 | 134 | Male | 44 | ||||
| 52 | 127.9 | Female | 55 | 125/74 | 68 | ||
| 53 | 127 | Female | 36 | ||||
| 54 | 131 | Male | 24 | ||||
| 55 | 129 | Female | 25 | ||||
| 56 | 96 | Male | 32 | 152/92 | 86 | 474.6 | 4.29 |
| Classification Model | R2 | MSE | MAE |
|---|---|---|---|
| AdaBoost | 0.89 | 13.43 | 2.50 |
| BP neural network | 0.86 | 22.21 | 3.32 |
| Random Forest | 0.90 | 13.02 | 2.48 |
| Classification Model | R2 | MSE | MAE | |||
|---|---|---|---|---|---|---|
| Nine Inputs | Eight Inputs | Nine Inputs | Eight Inputs | Nine Inputs | Eight Inputs | |
| AdaBoost | 0.91 | 0.86 | 13.99 | 20.78 | 2.67 | 3.35 |
| BP neural network | 0.87 | 0.82 | 24.64 | 26.86 | 3.77 | 3.91 |
| Random Forest | 0.89 | 0.85 | 15.20 | 22.92 | 2.80 | 3.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, J.; Sun, R.; Liu, H.; Wang, T.; Cai, L.; Chen, Z.; Heng, B. A Non-Invasive Hemoglobin Detection Device Based on Multispectral Photoplethysmography. Biosensors 2024, 14, 22. https://doi.org/10.3390/bios14010022
Zhu J, Sun R, Liu H, Wang T, Cai L, Chen Z, Heng B. A Non-Invasive Hemoglobin Detection Device Based on Multispectral Photoplethysmography. Biosensors. 2024; 14(1):22. https://doi.org/10.3390/bios14010022
Chicago/Turabian StyleZhu, Jianming, Ruiyang Sun, Huiling Liu, Tianjiao Wang, Lijuan Cai, Zhencheng Chen, and Baoli Heng. 2024. "A Non-Invasive Hemoglobin Detection Device Based on Multispectral Photoplethysmography" Biosensors 14, no. 1: 22. https://doi.org/10.3390/bios14010022
APA StyleZhu, J., Sun, R., Liu, H., Wang, T., Cai, L., Chen, Z., & Heng, B. (2024). A Non-Invasive Hemoglobin Detection Device Based on Multispectral Photoplethysmography. Biosensors, 14(1), 22. https://doi.org/10.3390/bios14010022