A High Accuracy & Ultra-Low Power ECG-Derived Respiration Estimation Processor for Wearable Respiration Monitoring Sensor †

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Existing Work
2.1. ECG-Derived Respiration Methods
2.2. QRS Detection Methods
3. Proposed EDR Estimation Method
3.1. Proposed QRS Detection Using Refractory Period Refreshing
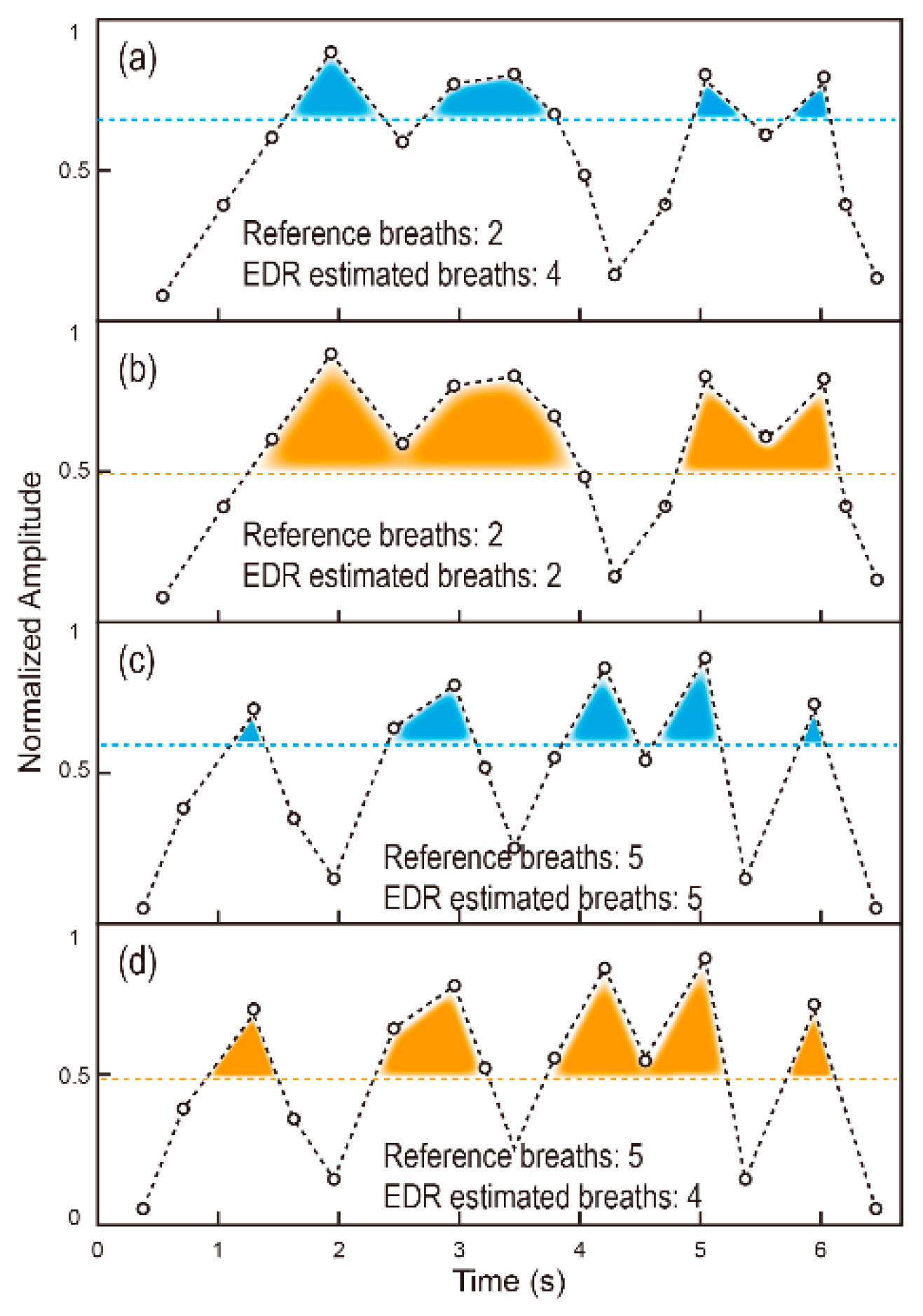
3.2. Proposed Adaptive Threshold Based EDR Estimation
4. Processor Implementation
4.1. Implementation of QRS Detection Module
4.2. Implementation of EDR Estimation Module
5. Experimental Results
5.1. Performance of QRS Detection and EDR Estimation
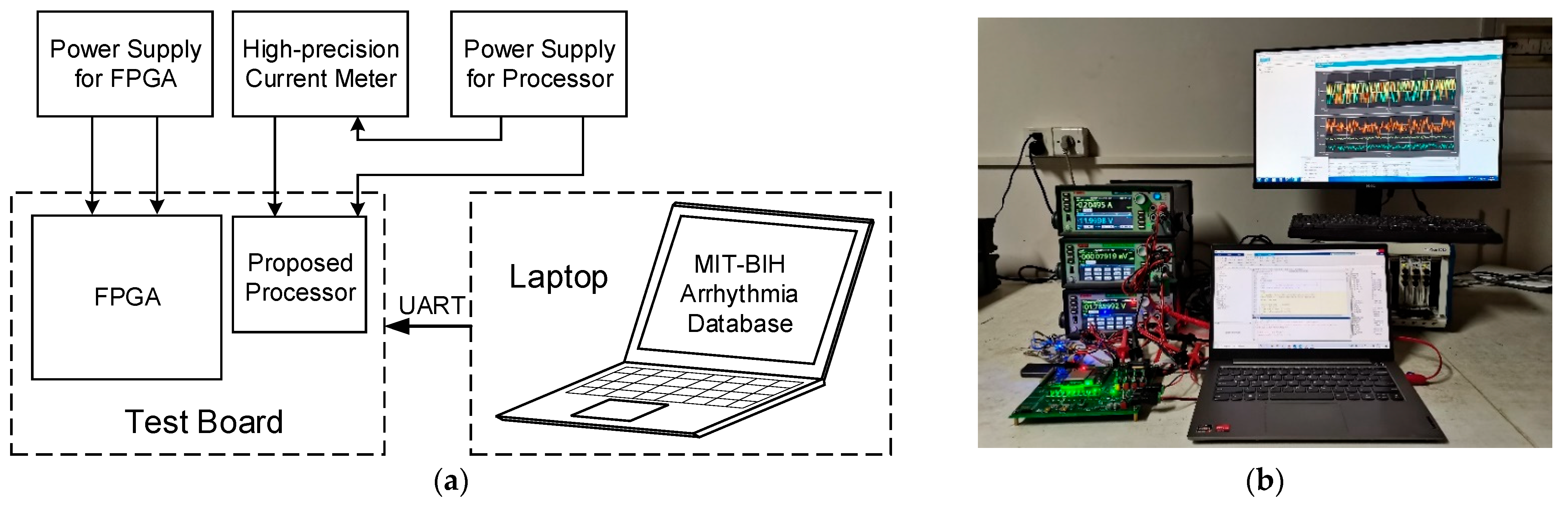
5.2. Performance of Proposed Processor
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Yang, S.; Fan, J.; Liu, J.; Chang, L.; Lin, S.; Zhou, J. A High Accuracy & Low Power EDR Estimation Processor for Wearable Devices. In Proceedings of the 2021 IEEE International Conference on Integrated Circuits, Technologies and Applications (ICTA), Zhuhai, China, 24–26 November 2021. [Google Scholar]
- Cretikos, M.; Chen, J.; Hillman, K.; Bellomo, R.; Finfer, S.; Flabouris, A. The objective medical emergency team activation criteria: A case–control study. Resuscitation 2007, 73, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Fieselmann, J.F.; Hendryx, M.S.; Helms, C.M.; Wakefield, D.S. Respiratory rate predicts cardiopulmonary arrest for internal medicine inpatients. J. Gen. Intern. Med. 1993, 8, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Cretikos, M.A.; Bellomo, R.; Hillman, K.; Chen, J.; Finfer, S.; Flabouris, V. Respiratory rate: The neglected vital sign. Med. J. Aust. 2008, 188, 657–659. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Kelen, G.; Rothman, R.E. A simple screening tool for identification of community-acquired pneumonia in an inner city emergency department. Emerg. Med. J. 2007, 24, 336–338. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, I.; Van Leuvan, C.H. Missed opportunities? An observational study of vital sign measurements. Crit. Care Resusc. 2008, 10, 111. [Google Scholar]
- Hogan, J. Why don’t nurses monitor the respiratory rates of patients? Br. J. Nurs. 2006, 15, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Charlton, P.H.; Birrenkott, D.A.; Bonnici, T.; Pimentel, M.A.F.; Johnson, A.E.W.; Alastruey, J.; Tarassenko, L.; Watkinson, P.J.; Beale, R.; Clifton, D.A. Breathing rate estimation from the electrocardiogram and photoplethysmogram: A review. IEEE Rev. Biomed. Eng. 2017, 11, 2–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzanti, B.; Lamberti, C.; De Bie, J. Validation of an ECG-derived respiration monitoring method. In Proceedings of the Computers in Cardiology, Piscataway, NJ, USA, 21–24 September 2003; pp. 613–616. [Google Scholar]
- Pambianco, B.; Sbrollini, A.; Marcantoni, I.; Morettini, M.; Fioretti, S.; Burattini, L. Electrocardiogram derived respiratory signal through the segmented-beat modulation method. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018. [Google Scholar]
- Zhao, Y.; Zhao, J.; Li, Q. Derivation of respiratory signals from single-lead ECG. In Proceedings of the 2008 International Seminar on Future BioMedical Information Engineering, Wuhan, China, 18 December 2008. [Google Scholar]
- Sarkar, S.; Bhattacherjee, S.; Pal, S. Extraction of respiration signal from ECG for respiratory rate estimation. In Proceedings of the Michael Faraday IET International Summit 2015, Kolkata, India, 12–13 September 2015. [Google Scholar]
- Sadr, N.; de Chazal, P. A fast principal component analysis method for calculating the ecg derived respiration. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018. [Google Scholar]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Hu, Q.; Tang, W. A Real-Time QRS Detection System With PR/RT Interval and ST Segment Measurements for Wearable ECG Sensors Using Parallel Delta Modulators. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Nayak, C.; Saha, S.K.; Kar, R.; Mandal, D. An Efficient and Robust Digital Fractional Order Differentiator Based ECG Pre-Processor Design for QRS Detection. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 682–696. [Google Scholar] [CrossRef] [PubMed]
- Thiamchoo, N.; Phukpattaranont, P. Application of wavelet transform and Shannon energy on R peak detection algorithm. In Proceedings of the 2016 13th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology (ECTI-CON), Chiang Mai, Thailand, 8 September 2016. [Google Scholar]
- Aqil, M.; Jbari, A.; Bourouhou, A. Adaptive ECG Wavelet analysis for R-peaks detection. In Proceedings of the 2016 International Conference on Electrical and Information Technologies (ICEIT), Tangiers, Morocco, 25 July 2016. [Google Scholar]
- Manikandan, M.; Soman, K. A novel method for detecting R-peaks in electrocardiogram (ECG) signal. Biomed. Signal Processing Control. 2012, 7, 118–128. [Google Scholar] [CrossRef]
- Chandra, B.S.; Sastry, C.S.; Jana, S. Robust Heartbeat Detection from Multimodal Data via CNN-Based Generalizable Information Fusion. IEEE Trans. Biomed. Eng. 2019, 66, 710–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, R.; Gao, Y.; Duan, X.; Zhu, T.; Wang, Z.; Jiao, B. QRS Detection and Measurement Method of ECG Paper Based on Convolutional Neural Networks. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018. [Google Scholar]
- Kozia, C.; Herzallah, R.; Lowe, D. ECG-derived respiration using a real-time QRS detector based on empirical mode decomposition. In Proceedings of the 2018 12th International Conference on Signal Processing and Communication Systems (ICSPCS), Cairns, QLD, Australia, 19 December 2018. [Google Scholar]
- Lovett, P.B.; Buchwald, J.M.; Stürmann, K.; Bijur, P. The vexatious vital: Neither clinical measurements by nurses nor an electronic monitor provides accurate measurements of respiratory rate in triage. Ann. Emerg. Med. 2005, 45, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M.A.F.; Charlton, P.H.; Clifton, D.A. Probabilistic estimation of respiratory rate from wearable sensors. Wearable Electron. Sens. 2015, 15, 241–262. [Google Scholar]
- Bailón, R.; Sörnmo, L.; Laguna, P. ECG-derived respiratory frequency estimation. Adv. Methods Tools ECG Data Anal. 2006, 1, 215–243. [Google Scholar]
- Schäfer, A.; Kratky, K.W. Estimation of breathing rate from respiratory sinus arrhythmia: Comparison of various methods. Ann. Biomed. Eng. 2008, 36, 476–485. [Google Scholar] [CrossRef]
- Tekeste, T.; Saleh, H.; Mohammad, B.; Khandoker, A.; Jelinek, H.; Ismail, M. A Nanowatt Real-Time Cardiac Autonomic Neuropathy Detector. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 739–750. [Google Scholar] [CrossRef]
- García-González, M.A.; Argelagós-Palau, A.; Fernández-Chimeno, M.; Ramos-Castro, J. A comparison of heartbeat detectors for the seismocardiogram. In Proceedings of the Computing in Cardiology 2013, Zaragoza, Spain, 22–25 September 2013; pp. 461–464. [Google Scholar]
- Ichimaru, Y.; Moody, G.B. Development of the polysomnographic database on CD-ROM. Psychiatry Clin. Neurosci. 1999, 53, 175–177. [Google Scholar] [CrossRef] [Green Version]
- Negi, S.; Singh, R.K.; Anoop, C.S. Development of a real-time breathing-rate monitor using difference operation method and adaptive windowing on dry-electrode ECG signal. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017. [Google Scholar]
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH Arrhythmia Database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef]
- Lazaro, J.; Reljin, N.; Bailon, R.; Gil, E.; Noh, Y.; Laguna, P.; Chon, K.H. Electrocardiogram derived respiratory rate using a wearable armband. IEEE Trans. Biomed. Eng. 2020, 68, 1056–1065. [Google Scholar] [CrossRef]
- Kozia, C.; Herzallah, R. Advanced Fusion and Empirical Mode Decomposition-Based Filtering Methods for Breathing Rate Estimation from Seismocardiogram Signals. Information 2021, 12, 368. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Approach | FP | FN |
|---|---|---|---|
| M1 | High threshold with refractory period | 419 | 2103 |
| M2 | Low threshold without refractory period | 6008 | 516 |
| M3 | Low threshold with refractory period | 1013 | 887 |
| M4 | Proposed QRS detection method | 453 | 440 |
| Parameter | Meaning | Used Value |
|---|---|---|
| The number of R-S peaks in a segment | 16 | |
| Flag value of the adaptive thresholds | 4 | |
| The number of total segments | 7 |
| Method | Database | No. of Subjects | MAE | Platform |
|---|---|---|---|---|
| EMBC 2017 [30] | MIT-BIH slpdb 1 | 13 | 2 | STM32F4 |
| EMBC 2018 [10] | CEBS | 20 | 1.1 | Software |
| TBME 2020 [32] | In-house | 15 | 3.57% | Software |
| Information 2021 [33] | CEBS | 20 | 1.5 | Software |
| Proposed | MIT-BIH slpdb | 13 | 1.2 | IC |
| CEBS | 20 | 0.73 or 3.03% 2 |
| Threshold | MAE |
|---|---|
| Maximum value based | 1.62 |
| Average value based | 0.83 |
| Proposed EDR method | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, J.; Yang, S.; Liu, J.; Zhu, Z.; Xiao, J.; Chang, L.; Lin, S.; Zhou, J. A High Accuracy & Ultra-Low Power ECG-Derived Respiration Estimation Processor for Wearable Respiration Monitoring Sensor. Biosensors 2022, 12, 665. https://doi.org/10.3390/bios12080665
Fan J, Yang S, Liu J, Zhu Z, Xiao J, Chang L, Lin S, Zhou J. A High Accuracy & Ultra-Low Power ECG-Derived Respiration Estimation Processor for Wearable Respiration Monitoring Sensor. Biosensors. 2022; 12(8):665. https://doi.org/10.3390/bios12080665
Chicago/Turabian StyleFan, Jiajing, Siqi Yang, Jiahao Liu, Zhen Zhu, Jianbiao Xiao, Liang Chang, Shuisheng Lin, and Jun Zhou. 2022. "A High Accuracy & Ultra-Low Power ECG-Derived Respiration Estimation Processor for Wearable Respiration Monitoring Sensor" Biosensors 12, no. 8: 665. https://doi.org/10.3390/bios12080665
APA StyleFan, J., Yang, S., Liu, J., Zhu, Z., Xiao, J., Chang, L., Lin, S., & Zhou, J. (2022). A High Accuracy & Ultra-Low Power ECG-Derived Respiration Estimation Processor for Wearable Respiration Monitoring Sensor. Biosensors, 12(8), 665. https://doi.org/10.3390/bios12080665