A Computational Modeling and Simulation Workflow to Investigate the Impact of Patient-Specific and Device Factors on Hemodynamic Measurements from Non-Invasive Photoplethysmography


Abstract
:1. Introduction
2. Materials and Methods
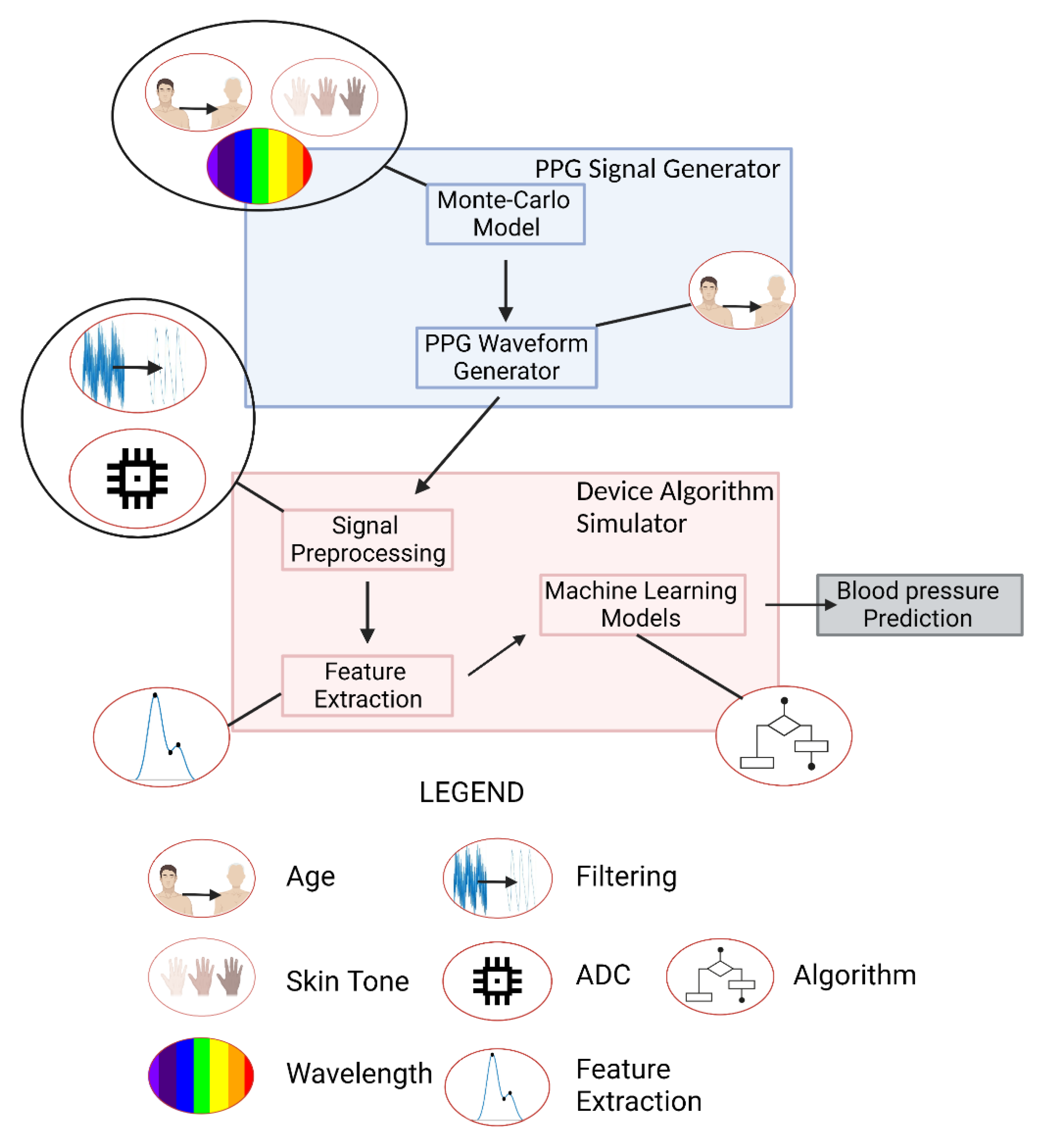
2.1. Schema Overview
2.2. PPG Signal Generator
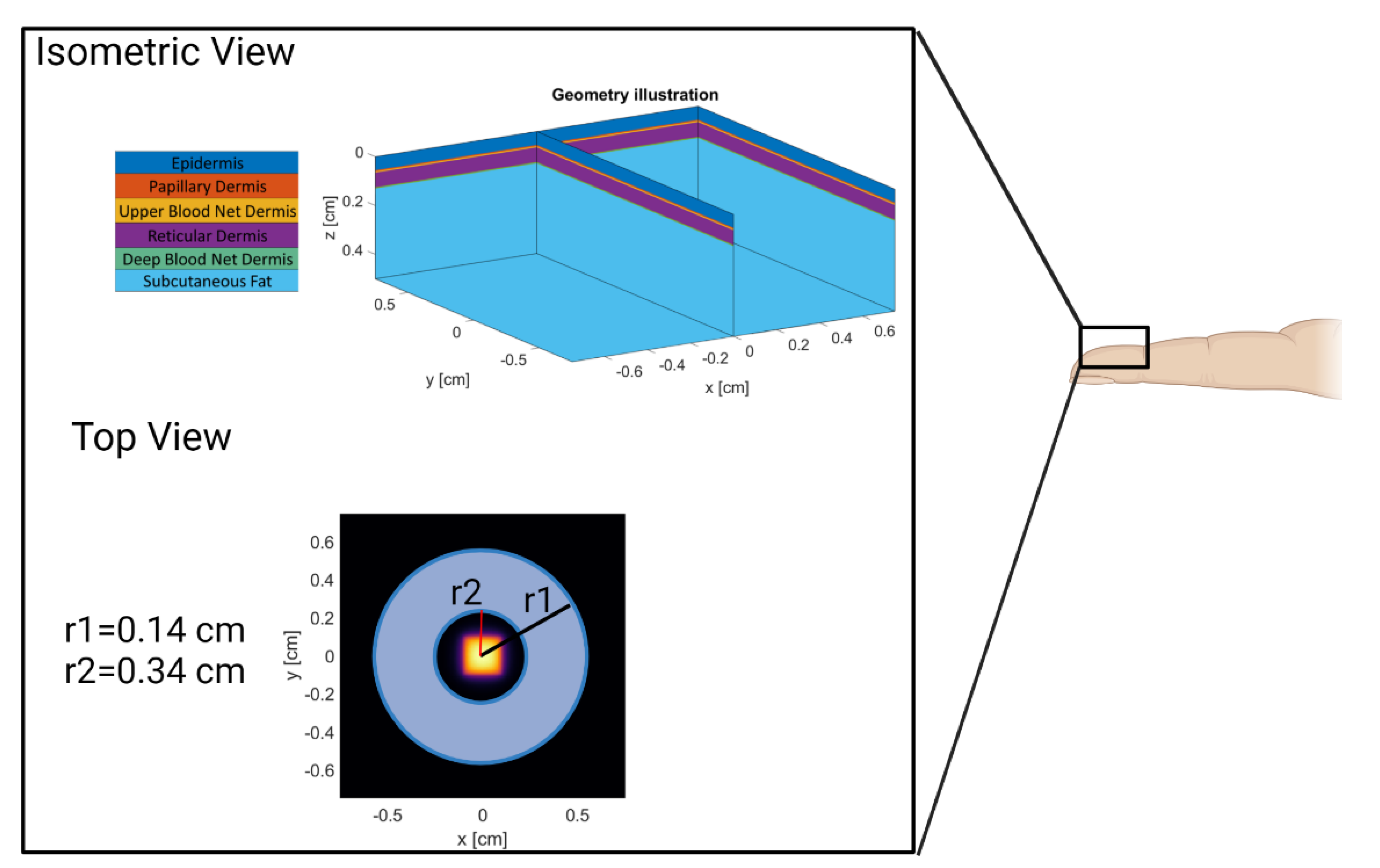
2.2.1. Monte Carlo Model
2.2.2. PPG Waveform Generator
2.3. Device Algorithm Simulator
2.3.1. Signal Preprocessing
2.3.2. Feature Extraction
2.3.3. Machine Learning Algorithms
3. Results and Discussion
3.1. PPG Signal Generator Verification
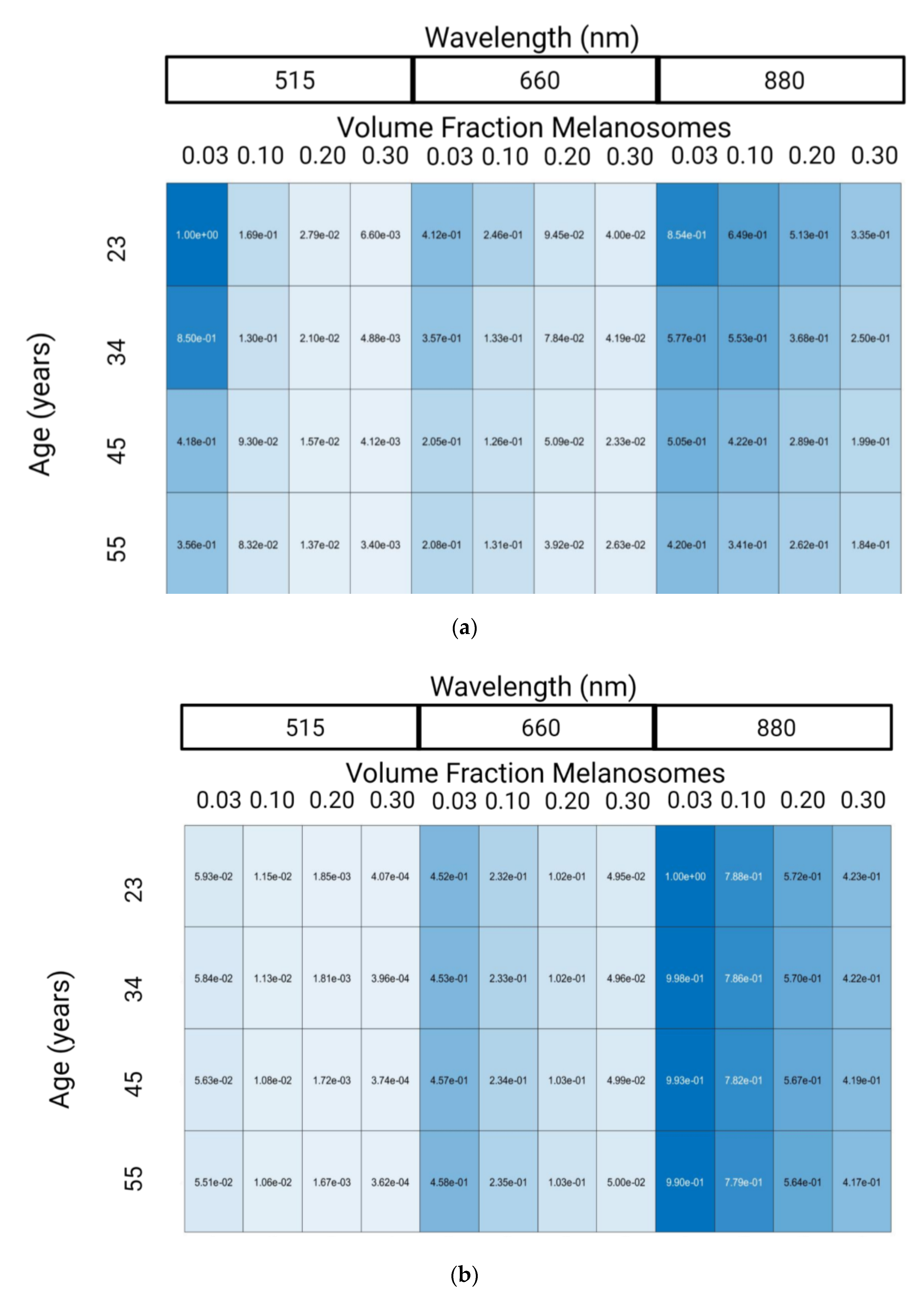
3.1.1. Monte Carlo Model
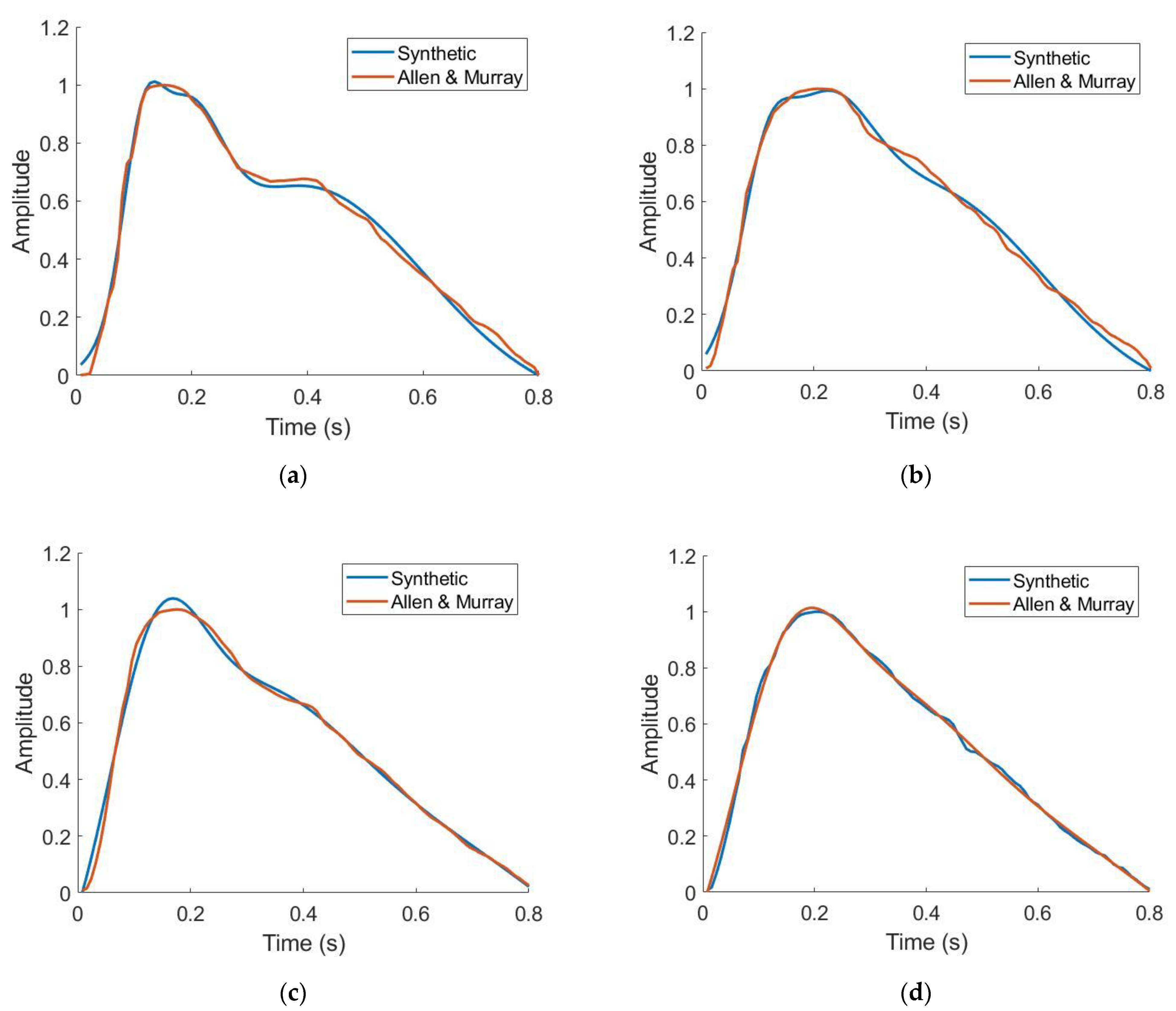
3.1.2. PPG Waveform Generator
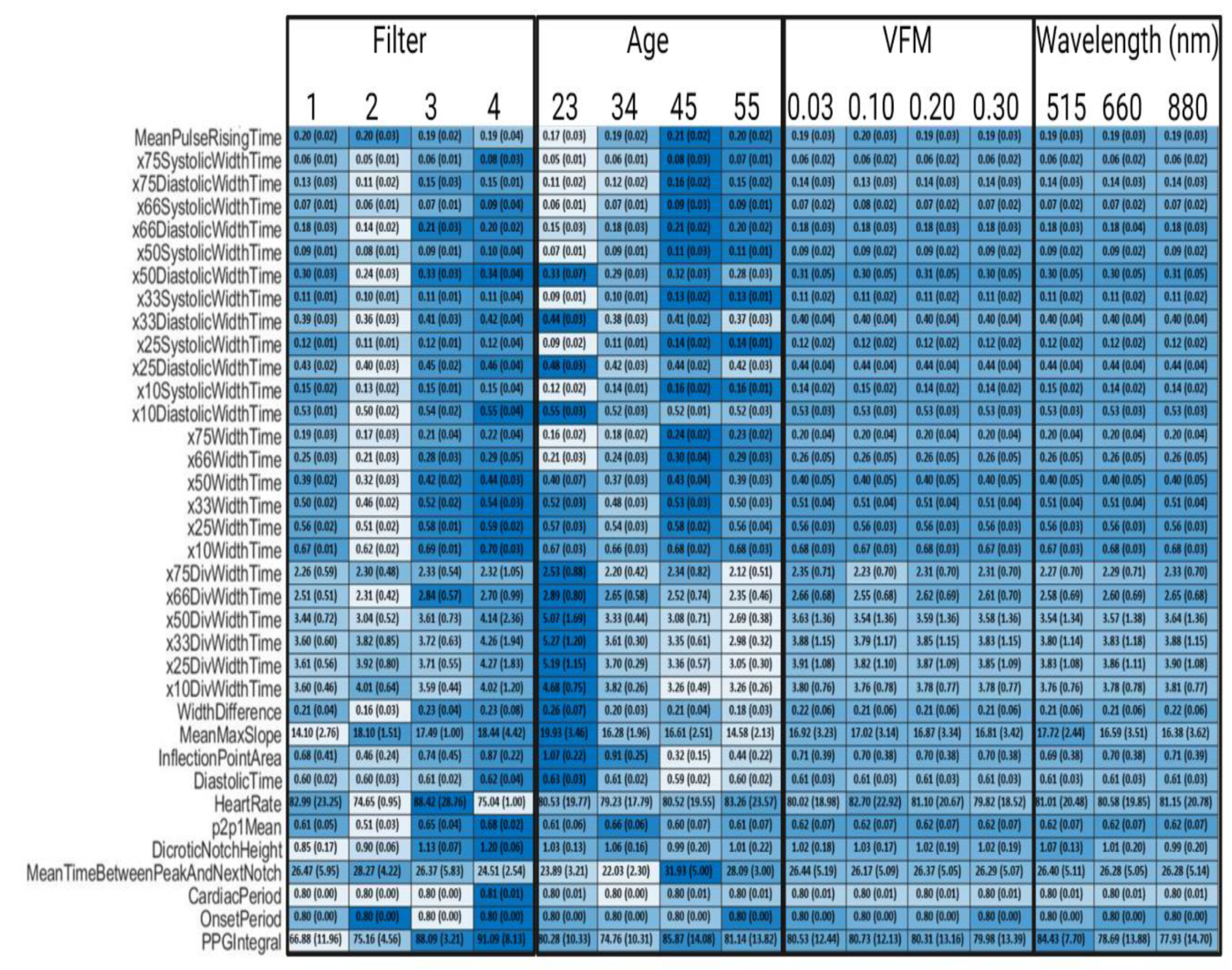
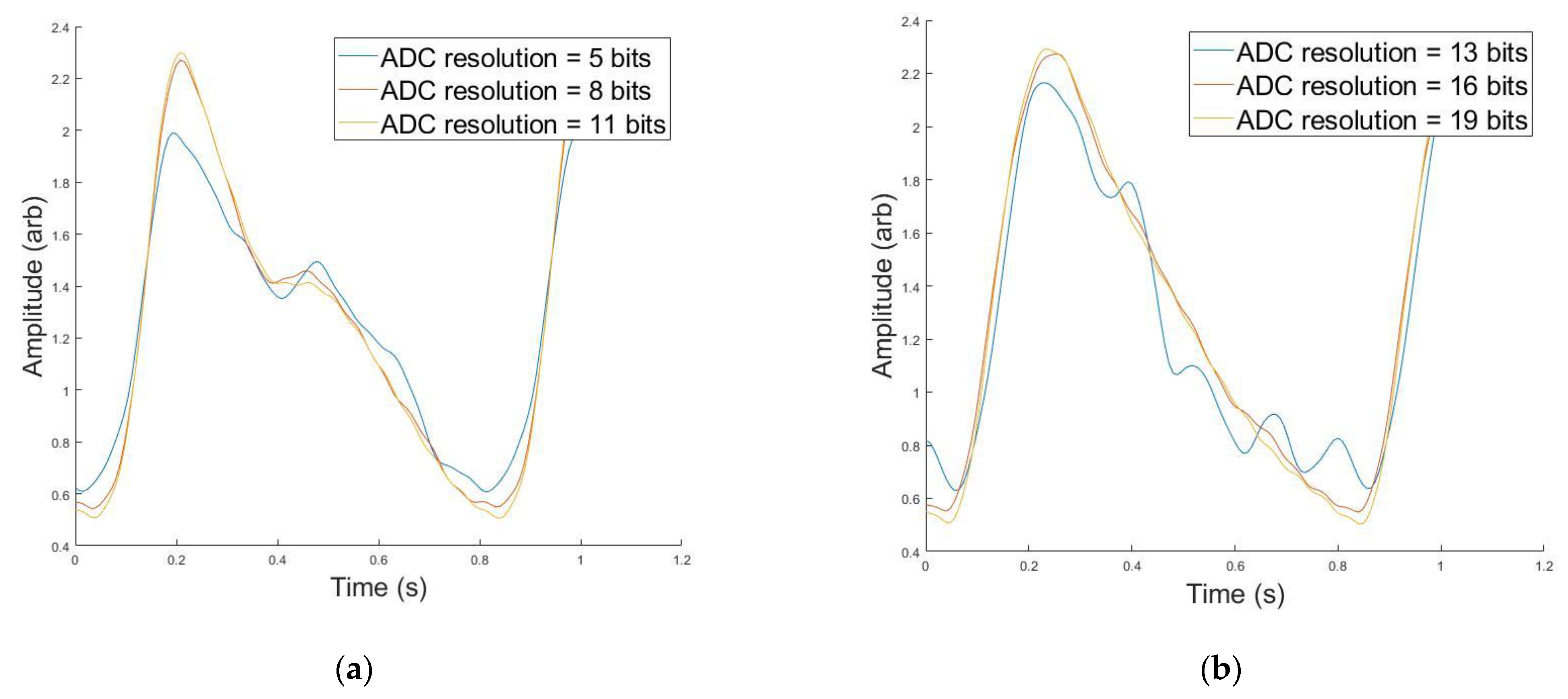
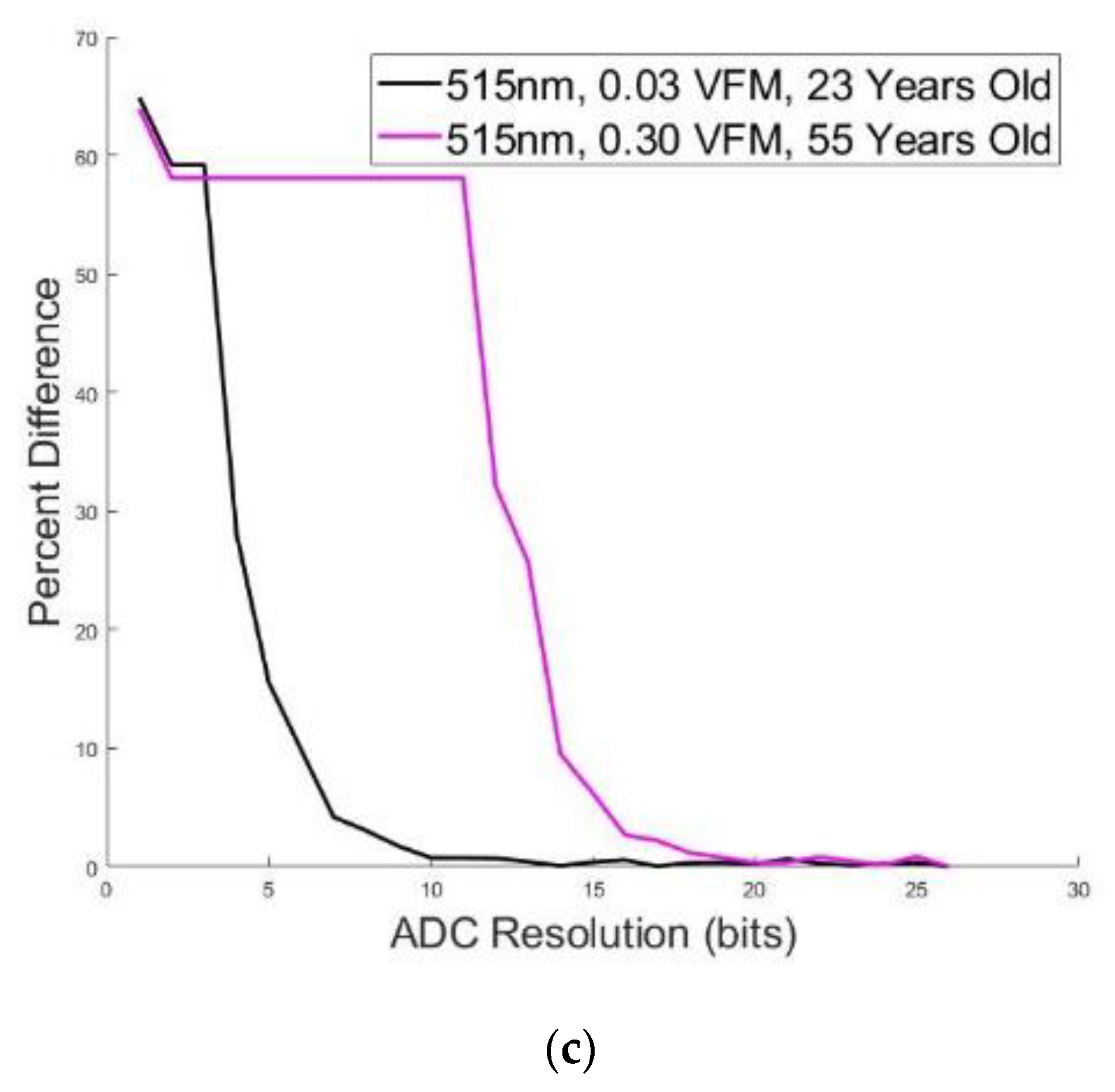
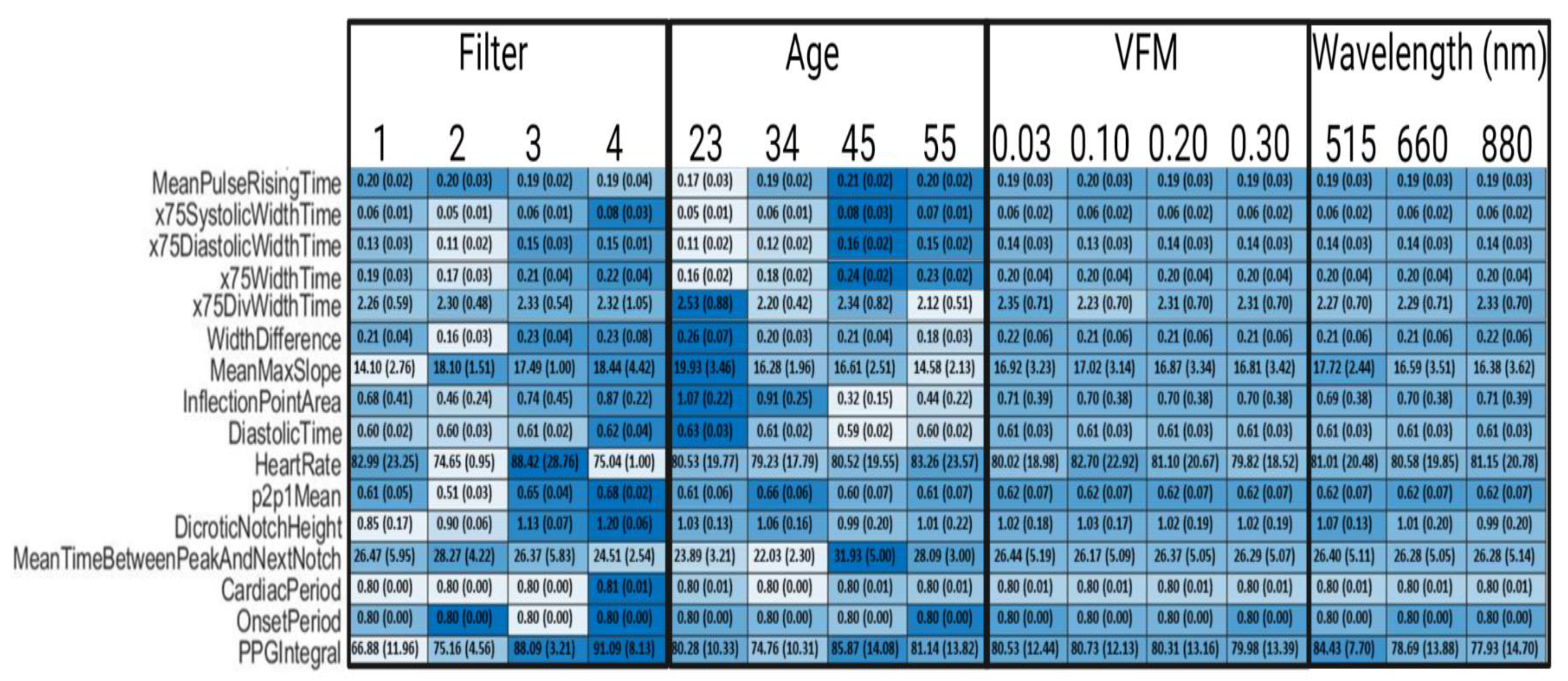
3.2. Impact on PPG Morphology and Features
3.3. Blood Pressure Estimation from Synthetic PPG Features
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Software and Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature Name | Definition |
|---|---|
| Mean Peak Amplitude | distance from systolic onset to systolic peak over 30 s window |
| Mean Pulse Rising Time | time from systolic onset to systolic peak over 30 s window |
| x75 Systolic Width Time | Time from systolic peak to the point before the systolic peak with amplitude of 75% of peak amplitude |
| X75 Diastolic Width Time | Time from systolic peak to the point after the systolic peak with amplitude of 75% of peak amplitude |
| X66 Systolic Width Time | Time from systolic peak to the point before the systolic peak with amplitude of 66% of peak amplitude |
| X66 Diastolic Width Time | Time from systolic peak to the point after the systolic peak with amplitude of 66% of peak amplitude |
| X50 Systolic Width Time | Time from systolic peak to the point before the systolic peak with amplitude of 50% of peak amplitude |
| X50 Diastolic Width Time | Time from systolic peak to the point after the systolic peak with amplitude of 50% of peak amplitude |
| X33 Systolic Width Time | Time from systolic peak to the point before the systolic peak with amplitude of 33% of peak amplitude |
| X33 Diastolic Width Time | Time from systolic peak to the point after the systolic peak with amplitude of 33% of peak amplitude |
| X25 Systolic Width Time | Time from systolic peak to the point before the systolic peak with amplitude of 25% of peak amplitude |
| X25 Diastolic Width Time | Time from systolic peak to the point after the systolic peak with amplitude of 25% of peak amplitude |
| X10 Systolic Width Time | Time from systolic peak to the point before the systolic peak with amplitude of 10% of peak amplitude |
| X10 Diastolic Width Time | Time from systolic peak to the point after the systolic peak with amplitude of 10% of peak amplitude |
| X75 Width Time | Time from the point on systolic rising edge to the point after the systolic rising edge where 75% of peak amplitude occurs |
| X66 Width Time | Time from the point on systolic rising edge to the point after the systolic rising edge where 66% of peak amplitude occurs |
| X50 Width Time | Time from the point on systolic rising edge to the point after the systolic rising edge where 50% of peak amplitude occurs |
| X33 Width Time | Time from the point on systolic rising edge to the point after the systolic rising edge where 33% of peak amplitude occurs |
| X25 Width Time | Time from the point on systolic rising edge to the point after the systolic rising edge where 25% of peak amplitude occurs |
| X10 Width Time | Time from the point on systolic rising edge to the point after the systolic rising edge where 10% of peak amplitude occurs |
| X75 Div Width Time | X75 Systolic Width Time/X75 Diastolic Width Time |
| X66 Div Width Time | X66 Systolic Width Time/X66 Diastolic Width Time |
| X50 Div Width Time | X50 Systolic Width Time/X50 Diastolic Width Time |
| X33 Div Width Time | X33 Systolic Width Time/X33 Diastolic Width Time |
| X25 Div Width Time | X25 Systolic Width Time/X25 Diastolic Width Time |
| X10 Div Width Time | X10 Systolic Width Time/X10 Diastolic Width Time |
| Width Difference | The absolute difference of X50 Systolic Width Time and X50 Diastolic Width Time |
| Mean Max Slope | The maximum slope observed across 3 points in the systolic rising edge |
| Inflection Point Area | The integral of the PPG waveform from the dicrotic notch to the next systolic onset divided by the integral of the PPG waveform from the onset to the dicrotic notch |
| Diastolic Time | Time from the systolic peak to the next systolic onset |
| Heart Rate | Systolic peaks identified over 30 s × 2 |
| P2p1 Mean | The ratio of dicrotic notch amplitude to systolic peak amplitude |
| Dicrotic Notch Height | Dicrotic notch amplitude |
| Mean Time Between Peak and Next Notch | Time between the systolic peak and dicrotic notch |
| Cardiac Period | Average time between systolic peaks |
| Onset Period | Average time between systolic onsets |
| PPG Integral | Area under the PPG waveform |
Appendix B
References
- Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)#:~:text=Cardiovascular%20diseases%20(CVDs)%20are%20the,%2D%20and%20middle%2Dincome%20countries (accessed on 26 May 2022).
- Hypertension Cascade: Hypertension Prevalence, Treatment and Control Estimates among U.S. Adults Aged 18 Years and Older Applying the Criteria from the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline—NHANES 2015–2018. Available online: https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html (accessed on 26 May 2022).
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef] [PubMed]
- Group, S.R. A randomized trial of intensive versus standard blood-pressure control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-Y.; Hu, H.-Y.; Chou, Y.-J.; Huang, N.; Chou, Y.-C.; Li, C.-P. High blood pressure and all-cause and cardiovascular disease mortalities in community-dwelling older adults. Medicine 2015, 94, e2160. [Google Scholar] [CrossRef]
- Woo, S.H.; Choi, Y.Y.; Kim, D.J.; Bien, F.; Kim, J.J. Tissue-informative mechanism for wearable non-invasive continuous blood pressure monitoring. Sci. Rep. 2014, 4, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, R.; Ghosh, S.; Gupta, B.; Chakravarty, T. A literature review on current and proposed technologies of noninvasive blood pressure measurement. Telemed. e-Health 2018, 24, 185–193. [Google Scholar] [CrossRef]
- Kim, B.J.; Park, J.-M.; Park, T.H.; Kim, J.; Lee, J.; Lee, K.-J.; Lee, J.; Chae, J.E.; Thabane, L.; Lee, J. Remote blood pressure monitoring and behavioral intensification for stroke: A randomized controlled feasibility trial. PLoS ONE 2020, 15, e0229483. [Google Scholar] [CrossRef]
- Castaneda, D.; Esparza, A.; Ghamari, M.; Soltanpur, C.; Nazeran, H. A review on wearable photoplethysmography sensors and their potential future applications in health care. Int. J. Biosens. Bioelectron. 2018, 4, 195. [Google Scholar]
- Elgendi, M.; Fletcher, R.; Liang, Y.; Howard, N.; Lovell, N.H.; Abbott, D.; Lim, K.; Ward, R. The use of photoplethysmography for assessing hypertension. NPJ Digit. Med. 2019, 2, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, J.; Branan, K.L.; Rodriguez, A.J.; Boonya-Ananta, T.; Ramella-Roman, J.C.; McShane, M.J.; Coté, G.L. Sources of inaccuracy in photoplethysmography for continuous cardiovascular monitoring. Biosensors 2021, 11, 126. [Google Scholar] [CrossRef]
- Gircys, R.; Liutkevicius, A.; Kazanavicius, E.; Lesauskaite, V.; Damuleviciene, G.; Janaviciute, A. Photoplethysmography-based continuous systolic blood pressure estimation method for low processing power wearable devices. Appl. Sci. 2019, 9, 2236. [Google Scholar] [CrossRef] [Green Version]
- Fujita, D.; Suzuki, A. Evaluation of the possible use of PPG waveform features measured at low sampling rate. IEEE Access 2019, 7, 58361–58367. [Google Scholar] [CrossRef]
- Maqsood, S.; Xu, S.; Springer, M.; Mohawesh, R. A Benchmark Study of Machine Learning for Analysis of Signal Feature Extraction Techniques for Blood Pressure Estimation Using Photoplethysmography (PPG). IEEE Access 2021, 9, 138817–138833. [Google Scholar] [CrossRef]
- Bickler, P.E.; Feiner, J.R.; Severinghaus, J.W. Effects of skin pigmentation on pulse oximeter accuracy at low saturation. J. Am. Soc. Anesthesiol. 2005, 102, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Feiner, J.R.; Severinghaus, J.W.; Bickler, P.E. Dark skin decreases the accuracy of pulse oximeters at low oxygen saturation: The effects of oximeter probe type and gender. Anesth. Analg. 2007, 105, S18–S23. [Google Scholar] [CrossRef] [Green Version]
- Maeda, Y.; Sekine, M.; Tamura, T. Relationship between measurement site and motion artifacts in wearable reflected photoplethysmography. J. Med. Syst. 2011, 35, 969–976. [Google Scholar] [CrossRef]
- Elgendi, M. On the analysis of fingertip photoplethysmogram signals. Curr. Cardiol. Rev. 2012, 8, 14–25. [Google Scholar] [CrossRef]
- Kılıçkaya, S.; Güner, A.; Dal, B. Comparison of different machine learning techniques for the cuffless estimation of blood pressure using PPG signals. In Proceedings of the 2020 International Congress on Human-Computer Interaction, Optimization and Robotic Applications (HORA), Ankara, Turkey, 9–11 June 2022; pp. 1–6. [Google Scholar]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Li-Wei, H.L.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moody, B.; Moody, G.; Villarroel, M.; Clifford, G.D.; Silva, I. MIMIC-III Waveform Database Matched Subset (Version 1.0). PhysioNet. 2020. Available online: https://doi.org/10.13026/c2294b (accessed on 26 May 2022).
- Boonya-Ananta, T.; Rodriguez, A.J.; Ajmal, A.; Du Le, V.N.; Hansen, A.K.; Hutcheson, J.D.; Ramella-Roman, J.C. Synthetic Photoplethysmography (PPG) of the radial artery through parallelized Monte Carlo and its correlation to Body Mass Index (BMI). bioRxiv 2020, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Martin-Martinez, D.; Casaseca-de-la-Higuera, P.; Martin-Fernandez, M.; Alberola-López, C. Stochastic modeling of the PPG signal: A synthesis-by-analysis approach with applications. IEEE Trans. Biomed. Eng. 2013, 60, 2432–2441. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Kyriacou, P.A. Monte Carlo analysis of optical interactions in reflectance and transmittance finger photoplethysmography. Sensors 2019, 19, 789. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Abay, T.Y.; Phillips, J.P.; Kyriacou, P.A. Investigating optical path and differential pathlength factor in reflectance photoplethysmography for the assessment of perfusion. J. Biomed. Opt. 2018, 23, 075005. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Budidha, K.; Kyriacou, P.A. Investigating the origin of photoplethysmography using a multiwavelength Monte Carlo model. Physiol. Meas. 2020, 41, 084001. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.; Chen, Z.; Allen, J.; Alian, A.; Menon, C.; Ward, R.; Elgendi, M. PPGSynth: An innovative toolbox for synthesizing regular and irregular photoplethysmography waveforms. Front. Med. 2020, 7, 735. [Google Scholar] [CrossRef] [PubMed]
- Meglinski, I.V.; Matcher, S. Computer simulation of the skin reflectance spectra. Comput. Methods Programs Biomed. 2003, 70, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Marti, D.; Aasbjerg, R.; Andersen, P.E.; Hansen, A.K. MCmatlab: An open-source user-friendly MATLAB-integrated 3D Monte Carlo light transport solver with heat diffusion and tissue damage. In Proceedings of the Optical Interactions with Tissue and Cells XXX, San Francisco, CA, USA, 2–3 February 2019; p. 108760T. [Google Scholar]
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37. [Google Scholar] [CrossRef] [PubMed]
- Shuster, S.; BLACK, M.M.; McVitie, E. The influence of age and sex on skin thickness, skin collagen and density. Br. J. Dermatol. 1975, 93, 639–643. [Google Scholar] [CrossRef]
- Lin, Y.; Li, D.; Liu, W.; Zhong, Z.; Li, Z.; He, Y.; Wu, S. A measurement of epidermal thickness of fingertip skin from OCT images using convolutional neural network. J. Innov. Opt. Health Sci. 2021, 14, 2140005. [Google Scholar] [CrossRef]
- Sulli, A.; Ruaro, B.; Alessandri, E.; Pizzorni, C.; Cimmino, M.A.; Zampogna, G.; Gallo, M.; Cutolo, M. Correlations between nailfold microangiopathy severity, finger dermal thickness and fingertip blood perfusion in systemic sclerosis patients. Ann. Rheum. Dis. 2014, 73, 247–251. [Google Scholar] [CrossRef]
- Reneman, R.S.; Van Merode, T.; Hick, P.; Muytjens, A.M.; Hoeks, A.P. Age-related changes in carotid artery wall properties in men. Ultrasound Med. Biol. 1986, 12, 465–471. [Google Scholar] [CrossRef]
- Meglinski, I.V.; Matcher, S.J. Quantitative assessment of skin layers absorption and skin reflectance spectra simulation in the visible and near-infrared spectral regions. Physiol. Meas. 2002, 23, 741. [Google Scholar] [CrossRef]
- Fine, J.; Boonya-ananta, T.; Rodriguez, A.; Ramella-Roman, J.C.; McShane, M.; Cote, G.L. Parallelized multi-layered Monte Carlo model for evaluation of a proximal phalanx photoplethysmograph. In Proceedings of the Optical Diagnostics and Sensing XX: Toward Point-of-Care Diagnostics, San Francisco, CA, USA, 3 February 2020; p. 1124702. [Google Scholar]
- Jacques, S.L. Optical Absorption of Melanin. In Oregon Medical Laser Center Monthly News and Articles on Biomedical Optics and Medical Lasers. 1998. Available online: http://omlc.ogi.edu/news/jan98/skinoptics.html (accessed on 26 May 2022).
- Anderson, R.; Parrish, J. Optical properties of human skin. In The Science of Photomedicine; Springer: Berlin/Heidelberg, Germany, 1982; pp. 147–194. [Google Scholar]
- Blanco, P.J.; Watanabe, S.M.; Passos, M.A.R.; Lemos, P.A.; Feijóo, R.A. An anatomically detailed arterial network model for one-dimensional computational hemodynamics. IEEE Trans. Biomed. Eng. 2014, 62, 736–753. [Google Scholar] [CrossRef]
- Allen, J.; O’Sullivan, J.; Stansby, G.; Murray, A. Age-related changes in pulse risetime measured by multi-site photoplethysmography. Physiol. Meas. 2020, 41, 074001. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Murray, A. Age-related changes in the characteristics of the photoplethysmographic pulse shape at various body sites. Physiol. Meas. 2003, 24, 297. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Liu, L.; Wu, J.; Tang, B.; Li, D. Comparison and noise suppression of the transmitted and reflected photoplethysmography signals. BioMed Res. Int. 2018, 2018, 4523593. [Google Scholar] [CrossRef]
- van Gent, P.; Farah, H.; van Nes, N.; van Arem, B. Analysing noisy driver physiology real-time using off-the-shelf sensors: Heart rate analysis software from the taking the fast lane project. J. Open Res. Softw. 2019, 7, 32. [Google Scholar] [CrossRef] [Green Version]
- Ab Hamid, H.; Nayan, N.A.; Suboh, M.Z.; Aminuddin, A. Second Derivatives of Photoplethysmogram for Hyperuricemia Classification using Artificial Neural Network. In Proceedings of the 2020 IEEE-EMBS Conference on Biomedical Engineering and Sciences (IECBES), Langkawi, Malaysia, 1 December 2020–3 March 2021; pp. 494–498. [Google Scholar]
- ISO 81060-2:2018; Noninvasive Sphygmomanometers—Part 2: Clinical Investigation of Intermittent Automated Measurement Type. ISO: Geneva, Switzerland, 2018.
- Moço, A.V.; Stuijk, S.; de Haan, G. New insights into the origin of remote PPG signals in visible light and infrared. Sci. Rep. 2018, 8, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajmal, A.; Boonya-Ananta, T.; Rodriguez, A.J.; Du Le, V.N.; Ramella-Roman, J.C. Investigation of optical heart rate sensors in wearables and the influence of skin tone and obesity on photoplethysmography (PPG) signal. In Proceedings of the Biophotonics in Exercise Science, Sports Medicine, Health Monitoring Technologies, and Wearables II; SPIE: Bellingham, DC, USA, 2021; p. 1163808. [Google Scholar]
- Asare, L.; Kviesis-Kipge, E.; Rubins, U.; Rubenis, O.; Spigulis, J. Multi-spectral photoplethysmography technique for parallel monitoring of pulse shapes at different tissue depths. In Proceedings of the European Conference on Biomedical Optics, Munich, Germany, 26–29 April 2022; p. 80872E. [Google Scholar]
- Abood, M.H.; Daood, A.S. A comparative study of the supraperiosteal and the subperiosteal dissection in the VY advancement (atasoy) flap for the management of fingertip injury. Basrah J. Surg. 2007, 13, 1–11. [Google Scholar]
- Schrumpf, F.; Frenzel, P.; Aust, C.; Osterhoff, G.; Fuchs, M. Assessment of Non-Invasive Blood Pressure Prediction from PPG and rPPG Signals Using Deep Learning. Sensors 2021, 21, 6022. [Google Scholar] [CrossRef]
- Monte-Moreno, E. Non-invasive estimate of blood glucose and blood pressure from a photoplethysmograph by means of machine learning techniques. Artif. Intell. Med. 2011, 53, 127–138. [Google Scholar] [CrossRef]
- El-Hajj, C.; Kyriacou, P.A. Cuffless blood pressure estimation from PPG signals and its derivatives using deep learning models. Biomed. Signal Process. Control. 2021, 70, 102984. [Google Scholar] [CrossRef]


| Feature Name | Definition |
|---|---|
| Pulse Rise Time | Difference in time from pulse onset to systolic peak |
| Peak Amplitude | Difference in signal amplitude between systolic peak and onset (AC component) |
| “X”% Systolic Width | Difference in time between “Y” and the systolic peak, where “Y” is the time at which “X”% of the peak amplitude is achieved before the systolic peak [19] |
| “X”% Diastolic Width | Difference in time between “Y” and the systolic peak, where “Y” is the time at which “X”% of the peak amplitude is achieved after the systolic peak [19] |
| Inflection Point Area | The ratio a2/a1, where a2 is the area under the PPG waveform from the dicrotic notch to the next onset and a1 is the area under the PPG waveform from the onset to the dicrotic notch [18] |
| Pulse Rate | The number of systolic peaks observed over 60 s |
| Age (Years) | Wavelength (nm) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 23 | 34.4 | 44.8 | 55 | 515 | 660 | 880 | |||||
| Thickness (mm)/Starting Depth (mm) | µa (cm−1) | µs (cm−1) | µa (cm−1) | µs (cm−1) | µa (cm−1) | µs (cm−1) | |||||
| Epidermis | 0.55/0.00 | 0.55/0.00 | 0.55/0.00 | 0.55/0.00 | (0.03/0.10/0.20/0.30 VFM) | 1.96/6.28/12.43/18.58 | 388.35 | 0.86/2.75/5.44/8.13 | 303.03 | 0.33/1.06/2.09/3.13 | 227.27 |
| Papillary Dermis | 0.075/0.55 | 0.071/0.55 | 0.067/0.55 | 0.064/0.55 | Rest | 1.2166 | 389.99 | 0.5249 | 208.65 | 0.2344 | 118.94 |
| Pulsed | 1.2202 | 0.5250 | 0.2346 | ||||||||
| Upper Blood Net Dermis | 0.04/0.63 | 0.038/0.62 | 0.036/0.62 | 0.033/0.61 | Rest | 1.5328 | 389.99 | 0.5398 | 208.65 | 0.2546 | 118.94 |
| Pulsed | 1.5593 | 0.5410 | 0.2558 | ||||||||
| Reticular Dermis | 0.75/0.67 | 0.71/0.66 | 0.67/0.65 | 0.64/0.65 | Rest | 1.2167 | 389.99 | 0.5256 | 208.65 | 0.2456 | 118.94 |
| Pulsed | 1.2202 | 0.5257 | 0.2458 | ||||||||
| Deep Blood Net Dermis | 0.05/1.42 | 0.05/1.37 | 0.04/1.33 | 0.04/1.28 | Rest | 1.2896 | 389.99 | 0.5288 | 208.65 | 0.2462 | 118.94 |
| Pulsed | 1.2985 | 0.5292 | 0.2466 | ||||||||
| Subcutaneous Tissue | 2.00/1.47 | 2.00/1.42 | 2.00/1.37 | 2.00/1.33 | n/a | 6.0798 | 336.18 | 0.2827 | 249.74 | 0.3195 | 191.53 |
| Age (Years) | Gaussian 1 Parameters (a1, b1, c1) | Gaussian 2 Parameters (a2, b2, c2) | Gaussian 3 Parameters (a3, b3, c3) | Median Relative Error (%) |
|---|---|---|---|---|
| 23 | 0.57,0.19,0.09 | 0.47,0.11,0.05 | 0.77,0.39,0.30 | 3.58 |
| 34.4 | 0.80,0.28,0.25 | 0.77,0.59,0.44 | 0.74,0.13,0.11 | 2.12 |
| 44.8 | 0.59,0.21,0.12 | 0.38,0.11,0.06 | 0.75,0.40,0.29 | 4.14 |
| 55.0 | 0.77,0.28,0.25 | 0.67,0.14,0.13 | 0.79,0.58,0.44 | 1.79 |
| Support Vector Machine | Bagged Trees | Neural Network | ||||
|---|---|---|---|---|---|---|
| Mean Error (mmHg) | Standard Deviation (mmHg) | Mean Error (mmHg) | Standard Deviation (mmHg) | Mean Error (mmHg) | Standard Deviation (mmHg) | |
| Systolic | 0.55 | 11.56 | −0.02 | 12.4 | −0.36 | 15.53 |
| Diastolic | −0.72 | 8.24 | −0.11 | 8.63 | −0.16 | 10.75 |
| Systolic-Synthetic | N/A | 0.12 | N/A | 3.46 | N/A | 14.53 |
| Diastolic-Synthetic | N/A | 0.10 | N/A | 4.34 | N/A | 9.44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fine, J.; McShane, M.J.; Coté, G.L.; Scully, C.G. A Computational Modeling and Simulation Workflow to Investigate the Impact of Patient-Specific and Device Factors on Hemodynamic Measurements from Non-Invasive Photoplethysmography. Biosensors 2022, 12, 598. https://doi.org/10.3390/bios12080598
Fine J, McShane MJ, Coté GL, Scully CG. A Computational Modeling and Simulation Workflow to Investigate the Impact of Patient-Specific and Device Factors on Hemodynamic Measurements from Non-Invasive Photoplethysmography. Biosensors. 2022; 12(8):598. https://doi.org/10.3390/bios12080598
Chicago/Turabian StyleFine, Jesse, Michael J. McShane, Gerard L. Coté, and Christopher G. Scully. 2022. "A Computational Modeling and Simulation Workflow to Investigate the Impact of Patient-Specific and Device Factors on Hemodynamic Measurements from Non-Invasive Photoplethysmography" Biosensors 12, no. 8: 598. https://doi.org/10.3390/bios12080598
APA StyleFine, J., McShane, M. J., Coté, G. L., & Scully, C. G. (2022). A Computational Modeling and Simulation Workflow to Investigate the Impact of Patient-Specific and Device Factors on Hemodynamic Measurements from Non-Invasive Photoplethysmography. Biosensors, 12(8), 598. https://doi.org/10.3390/bios12080598