Large Animal Studies to Reduce the Foreign Body Reaction in Brain–Computer Interfaces: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
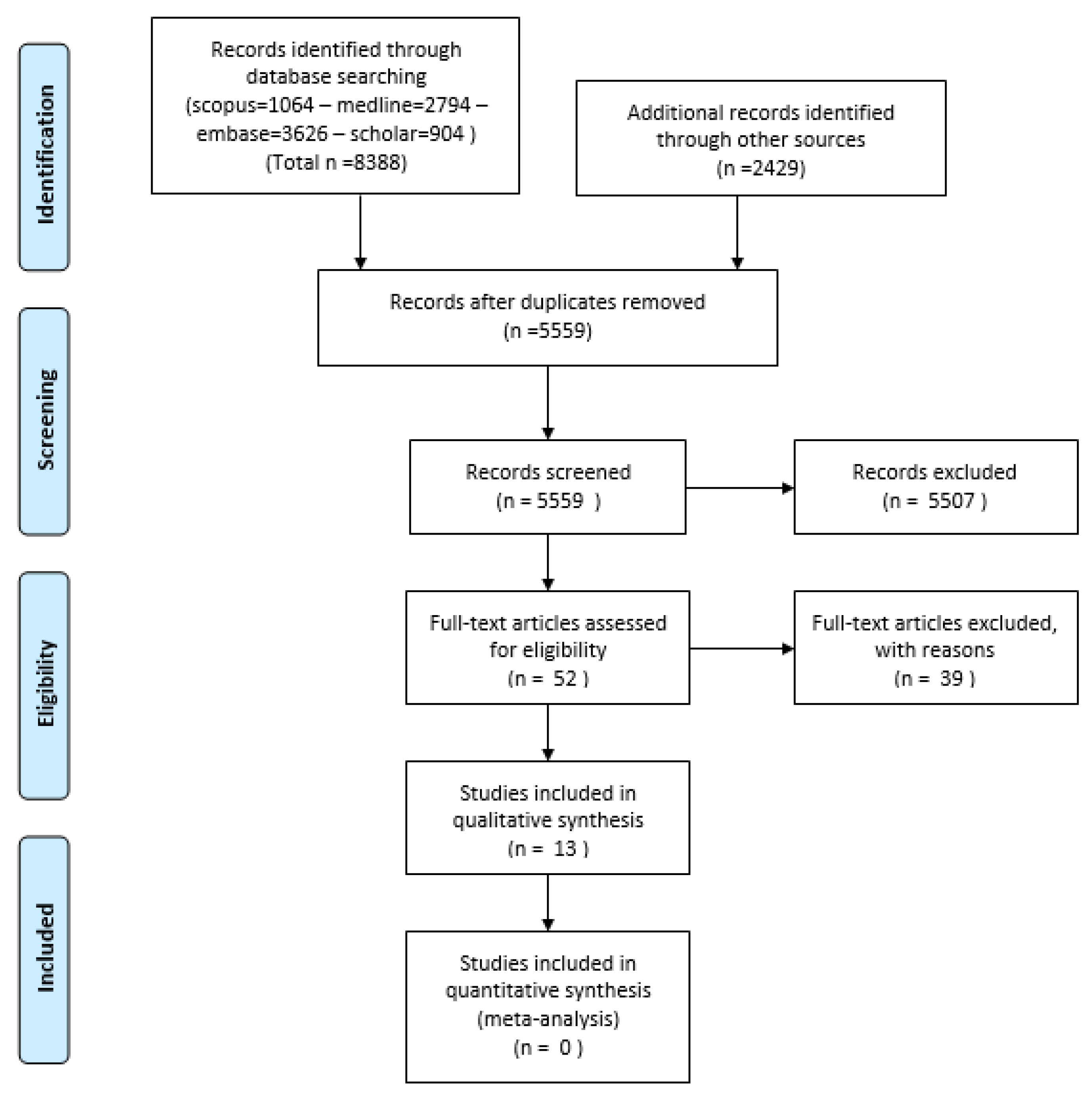
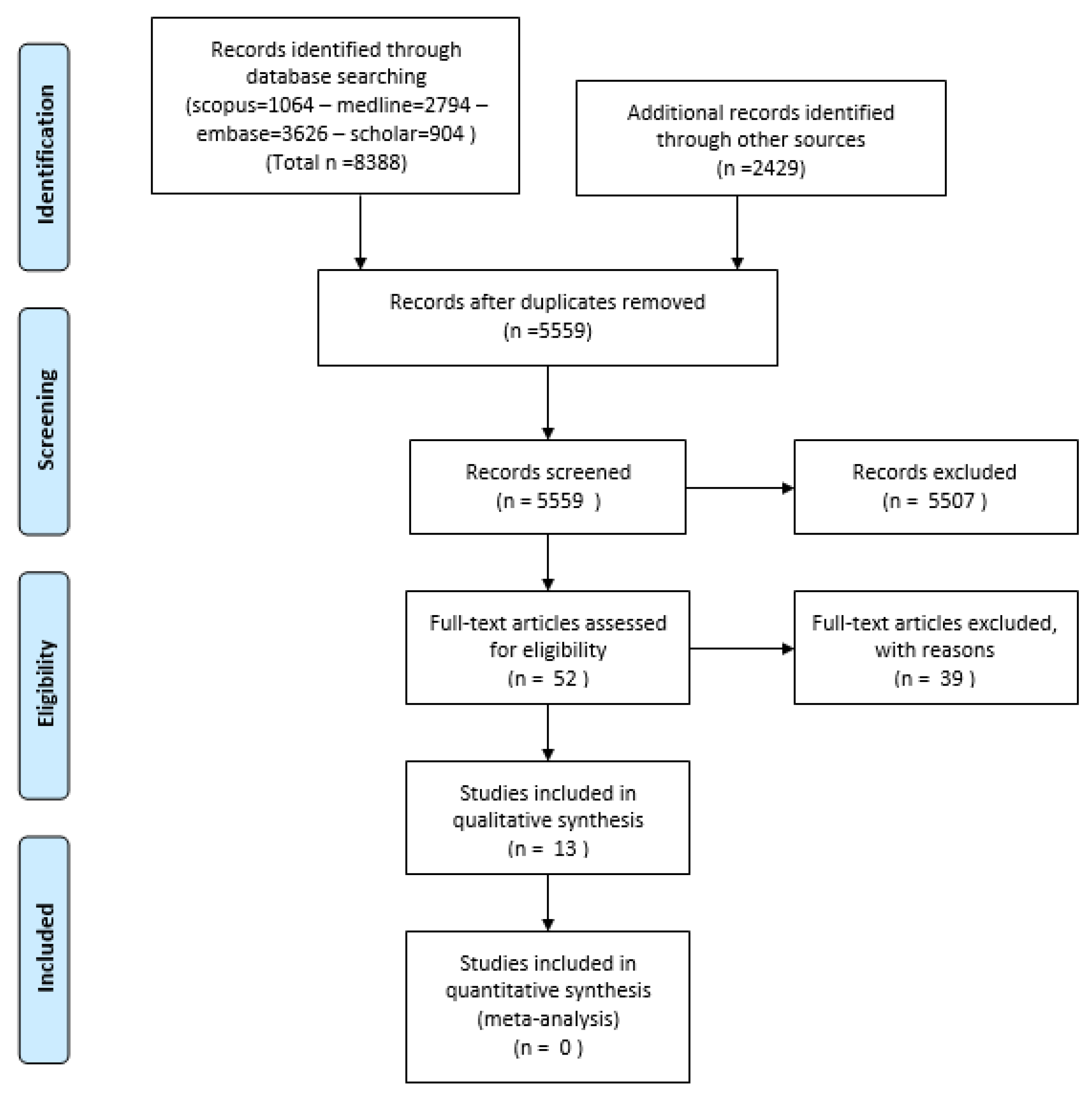
2. Methods
3. Results
- (a)
- Evaluating the FBR
- (b)
- The animals tested
- (c)
- The anatomical location of the neural interface, subdivided into the electrodes’ morphology and coating
- (d)
- The mechanics of electrode insertion
- (e)
- Pharmacological intervention
4. Discussion
4.1. Evaluation of the FBR and Animal Size
4.2. Methods to Reduce the FBR in the CNS—Physiological
4.3. Methods to Reduce the FBR in the CNS—Mechanical
4.4. Methods to Reduce the FBR in the CNS—Coatings
4.5. Methods to Reduce the FBR in the PNS—Mechanical
4.6. Methods to Reduce the FBR in the PNS—Coating and Summary
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Abdulkader, S.N.; Atia, A.; Mostafa, M.S.M. Brain computer interfacing: Applications and challenges. Egypt. Inform. J. 2015, 16, 213–230. [Google Scholar] [CrossRef] [Green Version]
- Alkawadri, R. Brain–Computer Interface (BCI) Applications in Mapping of Epileptic Brain Networks Based on Intracranial-EEG: An Update. Front. Neurosci. 2019, 13, 191. [Google Scholar] [CrossRef] [Green Version]
- Perlmutter, J.S.; Mink, J.W. DEEP BRAIN STIMULATION. Annu. Rev. Neurosci. 2006, 29, 229–257. [Google Scholar] [CrossRef] [Green Version]
- Chuang, A.T.; Margo, C.E.; Greenberg, P.B. Retinal implants: A systematic review. Br. J. Ophthalmol. 2014, 98, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.G.; Rebscher, S.; Harrison, W.; Sun, X.; Feng, H. Cochlear Implants: System Design, Integration, and Evaluation. IEEE Rev. Biomed. Eng. 2008, 1, 115–142. [Google Scholar] [CrossRef] [Green Version]
- Wagner, F.B.; Mignardot, J.B.; Le Goff-Mignardot, C.G.; Demesmaeker, R.; Komi, S.; Capogrosso, M.; Rowald, A.; Seáñez, I.; Caban, M.; Pirondini, E.; et al. Targeted neurotechnology restores walking in humans with spinal cord injury. Nature 2018, 563, 65–93. [Google Scholar] [CrossRef]
- Reddy, G.D.; Lozano, A.M. Postmortem studies of deep brain stimulation for Parkinson’s disease: A systematic review of the literature. Cell Tissue Res. 2018, 373, 287–295. [Google Scholar] [CrossRef]
- Suner, S.; Fellows, M.R.; Vargas-Irwin, C.; Nakata, G.K.; Donoghue, J.P. Reliability of signals from a chronically implanted, silicon-based electrode array in non-human primate primary motor cortex. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 524–541. [Google Scholar] [CrossRef]
- Kurihara, Y.; Takei, K. LOTUS, a potent blocker of Nogo receptor-1 causing inhibition of axonal growth. Neural Regen. Res. 2015, 10, 46. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, H.; Kiritoshi, T.; Murase, K. Effect of excitatory and inhibitory agents and a glial inhibitor on optically-recorded primary-afferent excitation. Mol. Pain 2008, 4, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pekny, M.; Nilsson, M. Astrocyte activation and reactive gliosis. Glia 2005, 50, 427–434. [Google Scholar] [CrossRef]
- Eng, L.F.; Ghirnikar, R.S. GFAP and Astrogliosis. In Proceedings of the Brain Pathology; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 1994; Volume 4, pp. 229–237. [Google Scholar]
- Polikov, V.S.; Tresco, P.A.; Reichert, W.M. Response of brain tissue to chronically implanted neural electrodes. J. Neurosci. Methods 2005, 148, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, K.I.; Khovanov, N.; Lopes, D.M.; La Russa, F.; McMahon, S.B. Large scale in vivo recording of sensory neuron activity with GCaMP6. eNeuro 2018, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, G.A.; Ledbetter, N.M.; Warren, D.J.; Harrison, R.R. Recording sensory and motor information from peripheral nerves with Utah Slanted Electrode Arrays. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 4641–4644. [Google Scholar]
- Pekny, M.; Pekna, M. Astrocyte reactivity and reactive astrogliosis: Costs and benefits. Physiol. Rev. 2014, 94, 1077–1098. [Google Scholar] [CrossRef]
- Sofroniew, M.V. Astrogliosis. Cold Spring Harb. Perspect. Biol. 2015, 7, a020420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burda, J.E.; Bernstein, A.M.; Sofroniew, M.V. Astrocyte roles in traumatic brain injury. Exp. Neurol. 2016, 275, 305–315. [Google Scholar] [CrossRef] [Green Version]
- Begley, D.J. Structure and function of the blood-brain barrier. In Enhancement in Drug Delivery; CRC Press: Boca Raton, FL, USA, 2006; pp. 575–592. ISBN 9781420004816. [Google Scholar]
- Rubin, L.L.; Staddon, J.M. The cell biology of the blood-brain barrier. Annu. Rev. Neurosci. 1999, 22, 11–28. [Google Scholar] [CrossRef]
- Risau, W.; Wolburg, H. Trends in Neurosciences. Development of the Blood-Brain Barrier. cell.com. 1990. Available online: https://www.cell.com/trends/neurosciences/pdf/0166-2236(90)90043-A.pdf (accessed on 20 December 2020).
- Sims, N.R.; Yew, W.P. Reactive astrogliosis in stroke: Contributions of astrocytes to recovery of neurological function. Neurochem. Int. 2017, 107, 88–103. [Google Scholar] [CrossRef]
- Moshayedi, P.; Ng, G.; Kwok, J.C.F.; Yeo, G.S.H.; Bryant, C.E.; Fawcett, J.W.; Franze, K.; Guck, J. The relationship between glial cell mechanosensitivity and foreign body reactions in the central nervous system. Biomaterials 2014, 35, 3919–3925. [Google Scholar] [CrossRef] [Green Version]
- Casanova, F.; Carney, P.R.; Sarntinoranont, M. In vivo evaluation of needle force and friction stress during insertion at varying insertion speed into the brain. J. Neurosci. Methods 2014, 237, 79–89. [Google Scholar] [CrossRef]
- Hassler, C.; von Metzen, R.P.; Ruther, P.; Stieglitz, T. Characterization of parylene C as an encapsulation material for implanted neural prostheses. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 9999B. [Google Scholar] [CrossRef]
- Vizuete, A.F.K.; Hansen, F.; Negri, E.; Leite, M.C.; de Oliveira, D.L.; Gonçalves, C.A. Effects of dexamethasone on the Li-pilocarpine model of epilepsy: Protection against hippocampal inflammation and astrogliosis. J. Neuroinflamm. 2018, 15, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kwiecien, J.M.; Jarosz, B.; Oakden, W.; Klapec, M.; Stanisz, G.J.; Delaney, K.H.; Kotlinska-Hasiec, E.; Janik, R.; Rola, R.; Dabrowski, W. An in vivo model of anti-inflammatory activity of subdural dexamethasone following the spinal cord injury. Neurol. Neurochir. Pol. 2016, 50, 7–15. [Google Scholar] [CrossRef]
- Fitzgerald, J.J. Suppression of scarring in peripheral nerve implants by drug elution. J. Neural Eng. 2016, 13, 026006. [Google Scholar] [CrossRef]
- Choy, E.H.S.; Calabrese, L.H. Neuroendocrine and neurophysiological effects of interleukin 6 in rheumatoid arthritis. Rheumatology 2018, 57, 1885–1895. [Google Scholar] [CrossRef] [Green Version]
- Veiseh, O.; Doloff, J.C.; Ma, M.; Vegas, A.J.; Tam, H.H.; Bader, A.R.; Li, J.; Langan, E.; Wyckoff, J.; Loo, W.S.; et al. Size- and shape-dependent foreign body immune response to materials implanted in rodents and non-human primates. Nat. Mater. 2015, 14, 643–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jun, J.J.; Steinmetz, N.A.; Siegle, J.H.; Denman, D.J.; Bauza, M.; Barbarits, B.; Lee, A.K.; Anastassiou, C.A.; Andrei, A.; Aydın, Ç.; et al. Fully integrated silicon probes for high-density recording of neural activity. Nature 2017, 551, 232–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bank, R.A. Implanted materials: Larger is stealthier. Nat. Mater. 2015, 14, 558–559. [Google Scholar] [CrossRef]
- Lacour, S.P.; Courtine, G.; Guck, J. Materials and technologies for soft implantable neuroprostheses. Nat. Rev. Mater. 2016, 1, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Musk, E. Neuralink An integrated brain-machine interface platform with thousands of channels. J. Med. Internet Res. 2019, 21, e16194. [Google Scholar] [CrossRef]
- Babiuk, L.A.; Pontarollo, R.; Babiuk, S.; Loehr, B.; Van Drunen Littel-van den Hurk, S. Induction of immune responses by DNA vaccines in large animals. Vaccine 2003, 21, 649–658. [Google Scholar] [CrossRef]
- Ortiz-Catalan, M.; Brånemark, R.; Håkansson, B.; Delbeke, J. On the viability of implantable electrodes for the natural control of artificial limbs: Review and discussion. Biomed. Eng. Online 2012, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Wark, H.A.C.; Sharma, R.; Mathews, K.S.; Fernandez, E.; Yoo, J.; Christensen, B.; Tresco, P.; Rieth, L.; Solzbacher, F.; Normann, R.A.; et al. A new high-density (25 electrodes/mm2) penetrating microelectrode array for recording and stimulating sub-millimeter neuroanatomical structures. J. Neural Eng. 2013, 10, 045003. [Google Scholar] [CrossRef]
- Degenhart, A.D.; Eles, J.; Dum, R.; Mischel, J.L.; Smalianchuk, I.; Endler, B.; Ashmore, R.C.; Tyler-Kabara, E.C.; Hatsopoulos, N.G.; Wang, W.; et al. Histological evaluation of a chronically-implanted electrocorticographic electrode grid in a non-human primate. J. Neural Eng. 2016, 13, 046019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McConnell, G.C.; Rees, H.D.; Levey, A.I.; Gutekunst, C.A.; Gross, R.E.; Bellamkonda, R.V. Implanted neural electrodes cause chronic, local inflammation that is correlated with local neurodegeneration. J. Neural Eng. 2009, 6, 056003. [Google Scholar] [CrossRef]
- Lawson, L.J.; Perry, V.H.; Dri, P.; Gordon, S. Heterogeneity in the distribution and morphology of microglia in the normal adult mouse brain. Neuroscience 1990, 39, 151–170. [Google Scholar] [CrossRef]
- Rostworowski, M.; Balasingam, V.; Chabot, S.; Owens, T.; Yong, V.W. Astrogliosis in the neonatal and adult murine brain post-trauma: Elevation of inflammatory cytokines and the lack of requirement for endogenous interferon-γ. J. Neurosci. 1997, 17, 3664–3674. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.G.; Rao, G.; Kew, Y.; Prabhu, S.S. Laser interstitial thermal therapy for newly diagnosed and recurrent glioblastoma. Neurosurg. Focus 2016, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, J.Y.; Wu, C.; Tracy, J.; Lorenzo, M.; Evans, J.; Nei, M.; Skidmore, C.; Mintzer, S.; Sharan, A.D.; Sperling, M.R. Laser interstitial thermal therapy for medically intractable mesial temporal lobe epilepsy. Epilepsia 2016, 57, 325–334. [Google Scholar] [CrossRef]
- Mohammadi, A.M.; Schroeder, J.L. Laser interstitial thermal therapy in treatment of brain tumors-the NeuroBlate System. Expert Rev. Med. Devices 2014, 11, 109–119. [Google Scholar] [CrossRef]
- Cho, N.; Squair, J.W.; Bloch, J.; Courtine, G. Neurorestorative interventions involving bioelectronic implants after spinal cord injury. Bioelectron. Med. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, J.W.; Asher, R.A. The glial scar and central nervous system repair. Brain Res. Bull. 1999, 49, 377–391. [Google Scholar] [CrossRef]
- Frank, M.; Wolburg, H. Cellular reactions at the lesion site after crushing of the rat optic nerve. Glia 1996, 16, 227–240. [Google Scholar] [CrossRef]
- Zhang, Y.G.; Sheng, Q.S.; Wang, H.K.; Lv, L.; Zhang, J.; Chen, J.M.; Xu, H. Triptolide improves nerve regeneration and functional recovery following crush injury to rat sciatic nerve. Neurosci. Lett. 2014, 561, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Shoffstall, A.J.; Srinivasan, S.; Willis, M.; Stiller, A.M.; Ecker, M.; Voit, W.E.; Pancrazio, J.J.; Capadona, J.R. A Mosquito Inspired Strategy to Implant Microprobes into the Brain. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jensen, W.; Yoshida, K.; Hofmann, U.G. In-vivo implant mechanics of flexible, silicon-based ACREO microelectrode arrays in rat cerebral cortex. IEEE Trans. Biomed. Eng. 2006, 53, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Rochford, A.E.; Carnicer-Lombarte, A.; Curto, V.F.; Malliaras, G.G.; Barone, D.G. When Bio Meets Technology: Biohybrid Neural Interfaces. Adv. Mater. 2020, 32, 1903182. [Google Scholar] [CrossRef]
- Spinks, R.L.; Baker, S.N.; Jackson, A.; Khaw, P.T.; Lemon, R.N. Problem of Dural Scarring in Recording From Awake, Behaving Monkeys: A Solution Using 5-Fluorouracil. J. Neurophysiol. 2003, 90, 1324–1332. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.A.; Brennan, P.M.; Bunting, A.S.; Cameron, K.; Murray, A.F.; Shipston, M.J. Patterning human neuronal networks on photolithographically engineered silicon dioxide substrates functionalized with glial analogues. J. Biomed. Mater. Res. Part A 2014, 102, 1350–1360. [Google Scholar] [CrossRef]
- Agnew, W.F.; McCreery, D.B.; Yuen, T.G.H.; Bullara, L.A. Histologic and physiologic evaluation of electrically stimulated peripheral nerve: Considerations for the selection of parameters. Ann. Biomed. Eng. 1989, 17, 39–60. [Google Scholar] [CrossRef]
- Sweeney, J.D.; Ksienski, D.A.; Mortimer, J.T. A Nerve Cuff Technique for Selective Excitation of Peripheral Nerve Trunk Regions. IEEE Trans. Biomed. Eng. 1990, 37, 706–715. [Google Scholar] [CrossRef] [PubMed]
- Badia, J.; Boretius, T.; Andreu, D.; Azevedo-Coste, C.; Stieglitz, T.; Navarro, X. Comparative analysis of transverse intrafascicular multichannel, longitudinal intrafascicular and multipolar cuff electrodes for the selective stimulation of nerve fascicles. J. Neural Eng. 2011, 8, 036023. [Google Scholar] [CrossRef]
- Zheng, X.; Zhang, J.; Chen, T.; Chen, Z. Longitudinally implanted intrafascicular electrodes for stimulating and recording fascicular physioelectrical signals in the sciatic nerve of rabbits. Microsurgery 2003, 23, 268–273. [Google Scholar] [CrossRef]
- Veraart, C.; Grill, W.M.; Mortimer, J.T. Selective Control of Muscle Activation with a Multipolar Nerve Cuff Electrode. IEEE Trans. Biomed. Eng. 1993, 40, 640–653. [Google Scholar] [CrossRef]
- Lawrence, S.M.; Dhillon, G.S.; Jensen, W.; Yoshida, K.; Horch, K.W. Acute peripheral nerve recording characteristics of polymer-based longitudinal intrafascicular electrodes. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Vomero, M.; Porto Cruz, M.F.; Zucchini, E.; Ciarpella, F.; Delfino, E.; Carli, S.; Boehler, C.; Asplund, M.; Ricci, D.; Fadiga, L.; et al. Conformable polyimide-based μECoGs: Bringing the electrodes closer to the signal source. Biomaterials 2020, 255, 120178. [Google Scholar] [CrossRef]
- Schendel, A.A.; Nonte, M.W.; Vokoun, C.; Richner, T.J.; Brodnick, S.K.; Atry, F.; Frye, S.; Bostrom, P.; Pashaie, R.; Thongpang, S.; et al. The effect of micro-ECoG substrate footprint on the meningeal tissue response. J. Neural Eng. 2014, 11, 046011. [Google Scholar] [CrossRef] [Green Version]
- Schiavone, G.; Fallegger, F.; Kang, X.; Barra, B.; Vachicouras, N.; Roussinova, E.; Furfaro, I.; Jiguet, S.; Seáñez, I.; Borgognon, S.; et al. Soft, Implantable Bioelectronic Interfaces for Translational Research. Adv. Mater. 2020, 32, 1906512. [Google Scholar] [CrossRef]
- Biran, R.; Martin, D.C.; Tresco, P.A. The brain tissue response to implanted silicon microelectrode arrays is increased when the device is tethered to the skull. J. Biomed. Mater. Res. Part A 2007, 82A, 169–178. [Google Scholar] [CrossRef]
- Kim, D.-H.; Viventi, J.; Amsden, J.J.; Xiao, J.; Vigeland, L.; Kim, Y.-S.; Blanco, J.A.; Panilaitis, B.; Frechette, E.S.; Contreras, D.; et al. Dissolvable films of silk fibroin for ultrathin conformal bio-integrated electronics. Nat. Mater. 2010, 9, 511–517. [Google Scholar] [CrossRef]
- Fisher, R.S. Intravascular stimulation of the motor cortex. Nat. Biomed. Eng. 2018, 2, 883–884. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Study | Species | Locus | Sample Size/Length of Study | Intervention | Control | Outcome(s) | Conclusion |
|---|---|---|---|---|---|---|---|
| Budoff 2019 * | Callithrix Jacchus | Cortex | 2, 7 Months | Teflon electrode coating | Comparison made to the same electrode applied in rodent | Immunohistochemistry | Mean presence of Gliosis extends to 1000 microns, as opposed to 800 in rodents |
| Edell 1992 * | Oructolagus Cuniculus | Cortex | 12, 6 Months | Chisel tip electrode | Control electrode inserted in same subject at different locus | Immunohistochemistry | All subjects showed significantly reduced Gliosis after first 30 Microns compared to control, extent of Gliosis was equivalent |
| Han 2012 * | Felis Catus/ Oructolagus Cuniculus | Cortex + VCN | 5C, 3R 18 Months | Silicon + Iridium Oxide plated electrode | Control electrodes in same subject at contralateral locus | Immunohistochemistry + Electrophysiology |
|
| Lenarz 2007 | Felis Catus | Inferior Colliculi | 8, 3 Months | 4 Hourly daily stimulation | Control group without stimulation | Immunohistochemistry |
|
| Leventhal 2006 | Felis Catus | Sciatic Nerve | 12, 3 Months | FINE Ovoid Cuff (wide, medium and narrow configurations) | Control electrode inserted at contralateral side | Immunohistochemistry | 30% increase in Gliosis in narrow cuff, medium and wide comparable |
| Meijs 2016 | Sus Scrofa Domesticus | Dorsal Genital Nerve | 2, 2 Months | Porous Tin Nitride plated electrode | Control electrode inserted at contralateral side | Immunohistochemistry | No significant change in Gliosis |
| Orlowski 2017 * | Sus Scrofa Domesticus | Cortex | 11, 12 Months | Altering depth of stimulation segment | Control inserted contralaterally, different depths activated | Immunohistochemistry | No significant changes in Gliosis with varying height, mean range was 500 microns |
| Schmidt 1993 * | Felis Catus | Cortex | 12, 6 Months | Polyamide coating of electrode | Control uncoated electrodes inserted contralaterally | Immunohistochemistry | Polyamide coating significantly increased Gliosis density, with no effect on range of around 40–80 microns |
| Smith 2012 | Felis Catus | RLGN | 12, 3 Months | Electrode effect measured in anastomosed and autografted nerves | Controlled against similar trials in the literature | Immunohistochemistry | No significant change in Gliosis, either against controls or in method of repair |
| Sohal 2016 * | Oructolagus Cuniculus | Cortex | 4, 24 Months | Sinusoidal, flexible electrode | Controlled against traditional, rigid electrode | Immunohistochemistry | Significant reduction in Gliosis up to 500 microns, no change in range of Gliosis observed between groups |
| Sohal 2014 * | Oructolagus Cuniculus | Cortex | 5, 24 Months | Sinusoidal, flexible electrode | Controlled against traditional, rigid electrode | Immunohistochemistry + Electrophysiology |
|
| Torres 2019 * | Sus Scrofa Domesticus | Cortex | 2, 3 Months | Boron/Diamond coated Carbon electrode | Controlled against traditional Platinum Iridium electrode | Immunohistochemistry + Electrophysiology |
|
| Zhen 2019 | Oructolagus Cuniculus | Sciatic Nerve | 14, 9 Months | Novel custom electrode | Controlled against traditional straight electrode, and sham cuff | Immunohistochemistry + Electrophysiology |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mian, S.Y.; Honey, J.R.; Carnicer-Lombarte, A.; Barone, D.G. Large Animal Studies to Reduce the Foreign Body Reaction in Brain–Computer Interfaces: A Systematic Review. Biosensors 2021, 11, 275. https://doi.org/10.3390/bios11080275
Mian SY, Honey JR, Carnicer-Lombarte A, Barone DG. Large Animal Studies to Reduce the Foreign Body Reaction in Brain–Computer Interfaces: A Systematic Review. Biosensors. 2021; 11(8):275. https://doi.org/10.3390/bios11080275
Chicago/Turabian StyleMian, Shan Yasin, Jonathan Roy Honey, Alejandro Carnicer-Lombarte, and Damiano Giuseppe Barone. 2021. "Large Animal Studies to Reduce the Foreign Body Reaction in Brain–Computer Interfaces: A Systematic Review" Biosensors 11, no. 8: 275. https://doi.org/10.3390/bios11080275
APA StyleMian, S. Y., Honey, J. R., Carnicer-Lombarte, A., & Barone, D. G. (2021). Large Animal Studies to Reduce the Foreign Body Reaction in Brain–Computer Interfaces: A Systematic Review. Biosensors, 11(8), 275. https://doi.org/10.3390/bios11080275