Accuracy of the Electronic Nose Breath Tests in Clinical Application: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
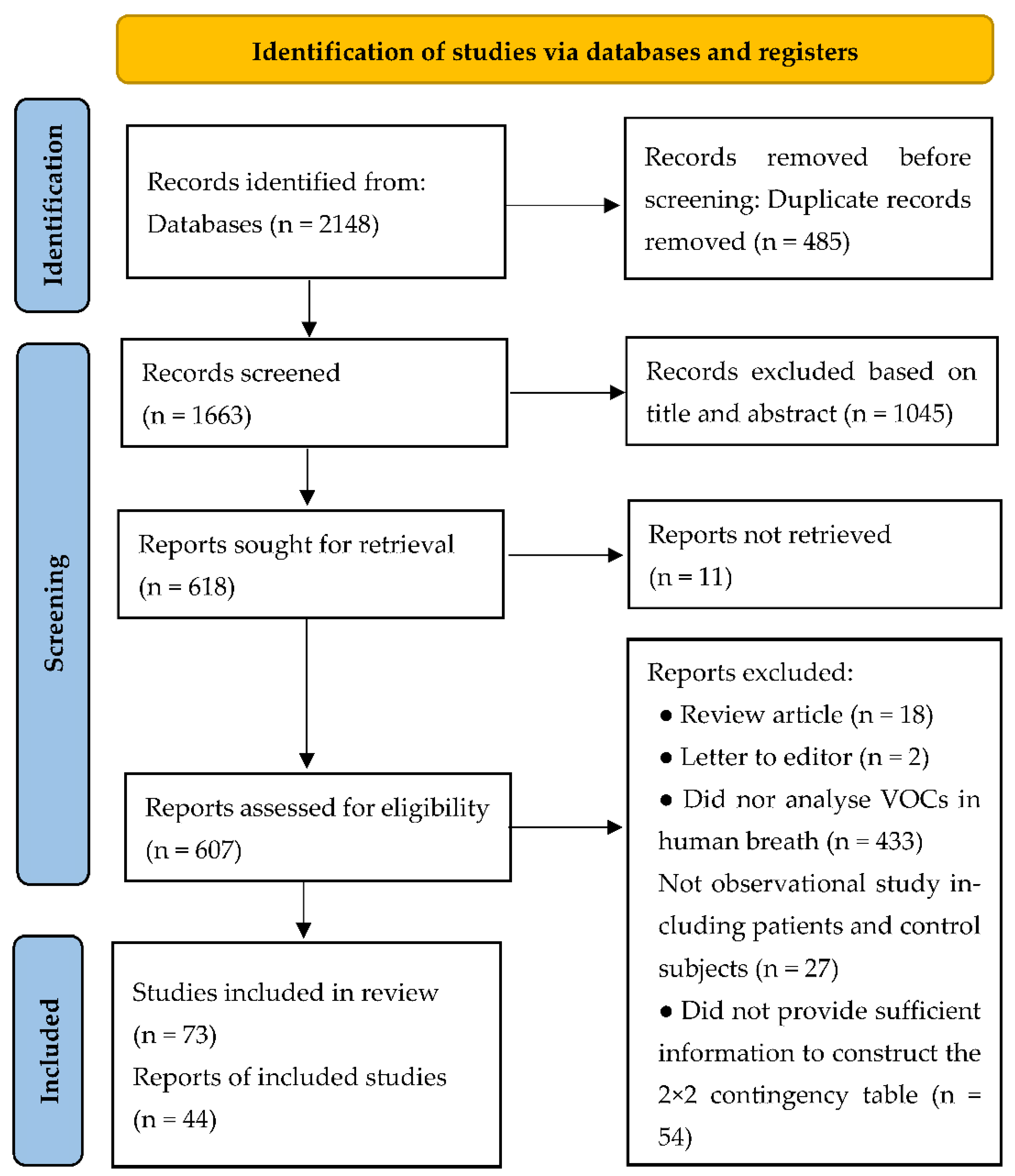
2.4. Selection Process
2.5. Data Items
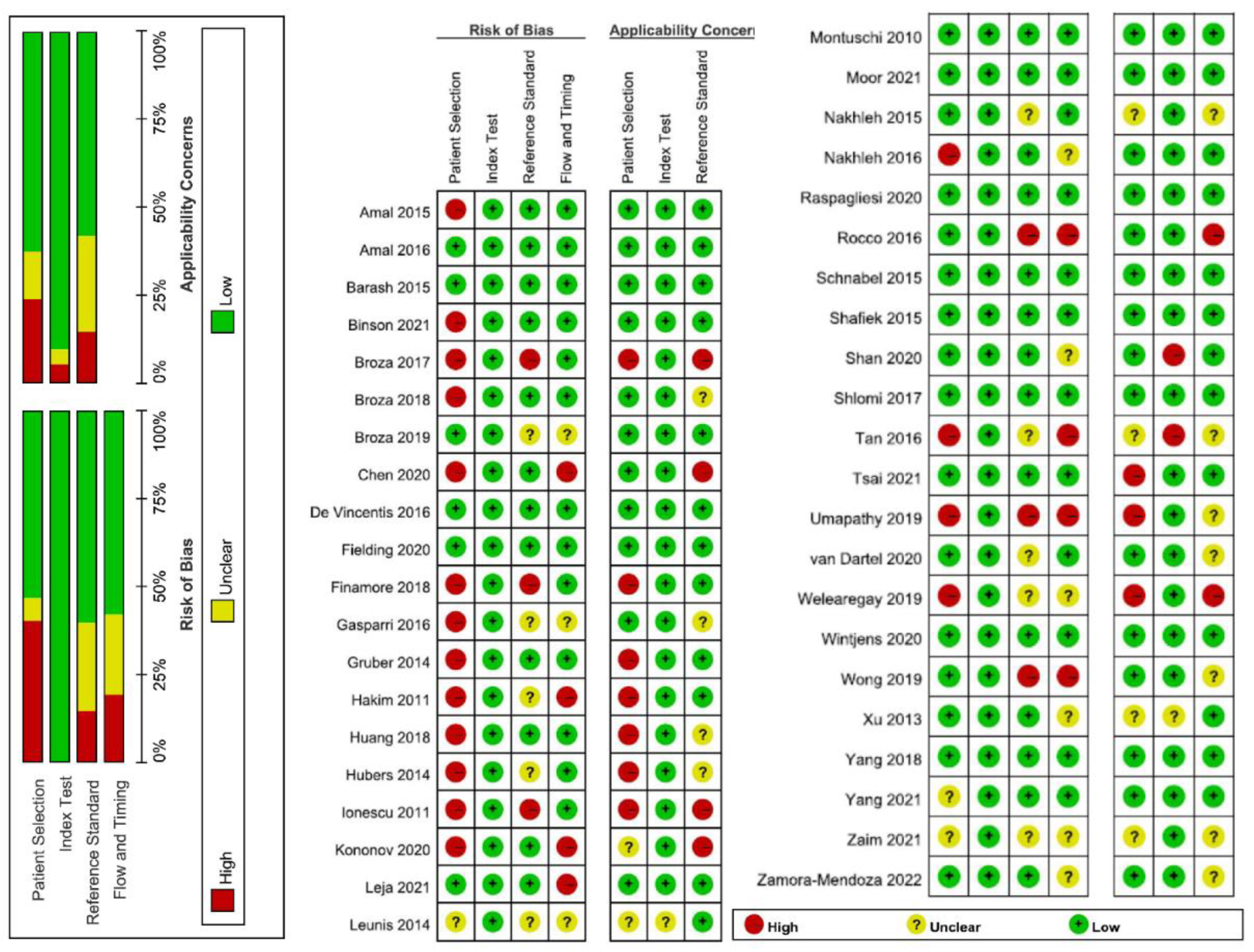
2.6. Quality Assessment
2.7. Statistical Analysis
2.8. Sensitivity Analysis
2.9. Subgroup Analysis
3. Results
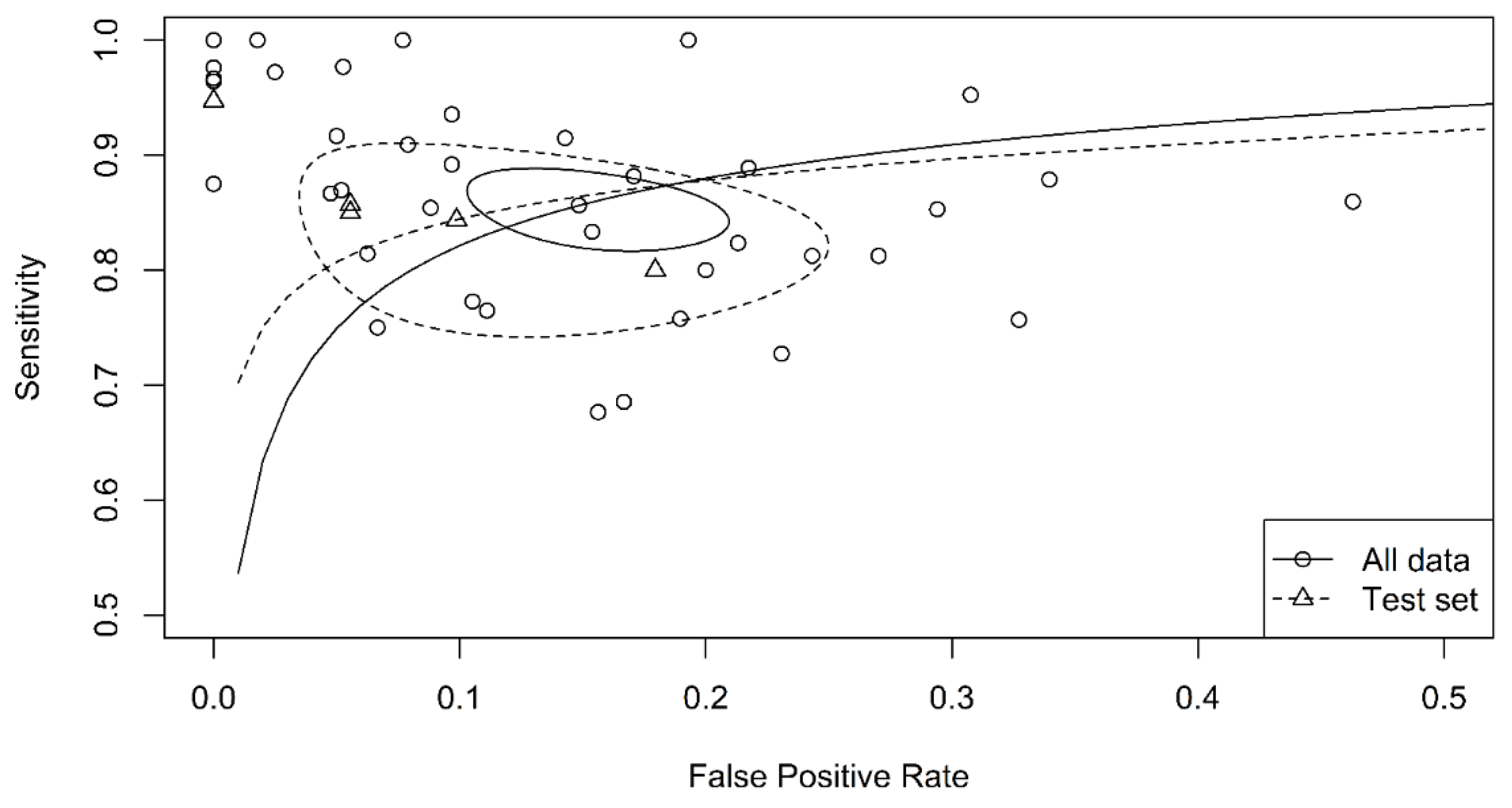
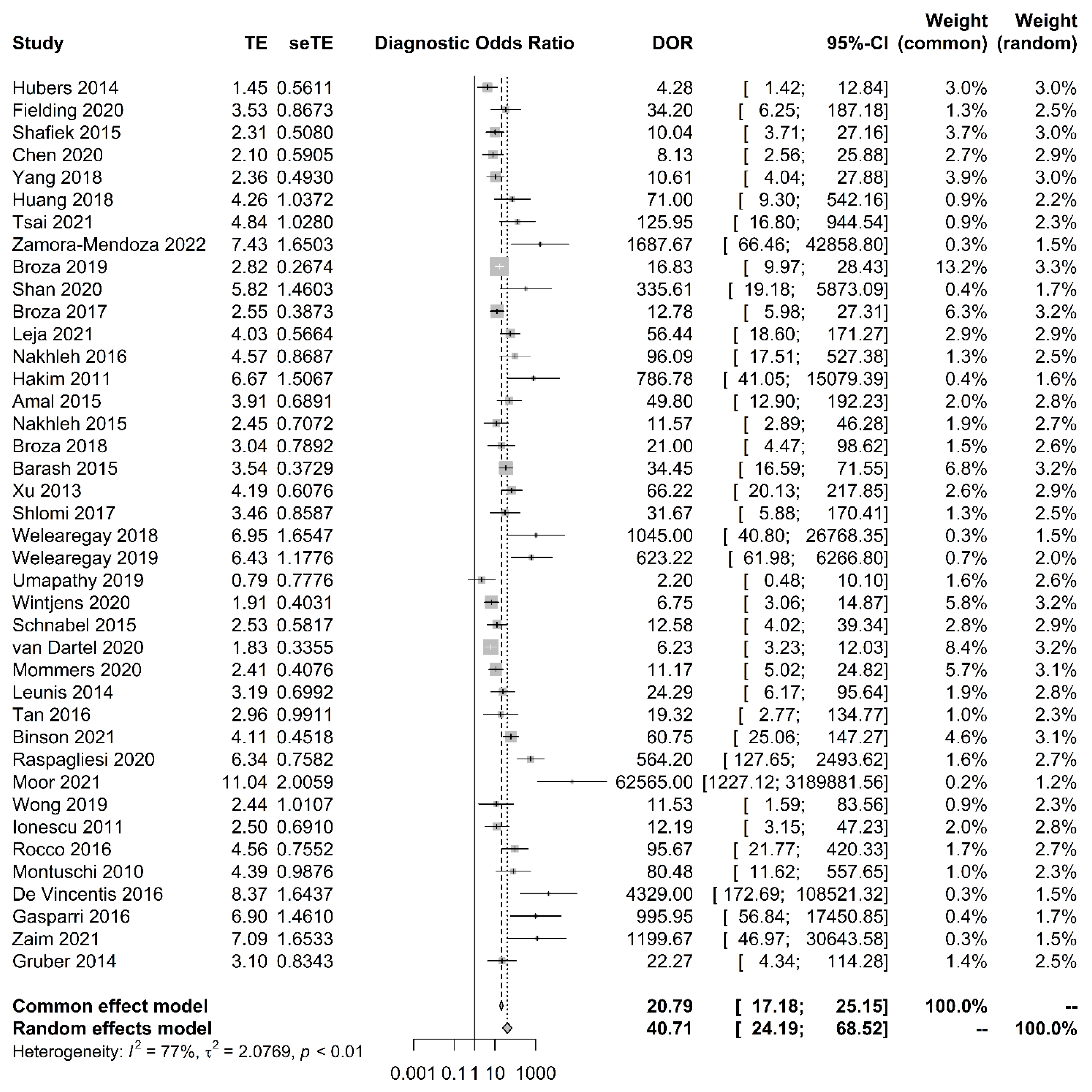
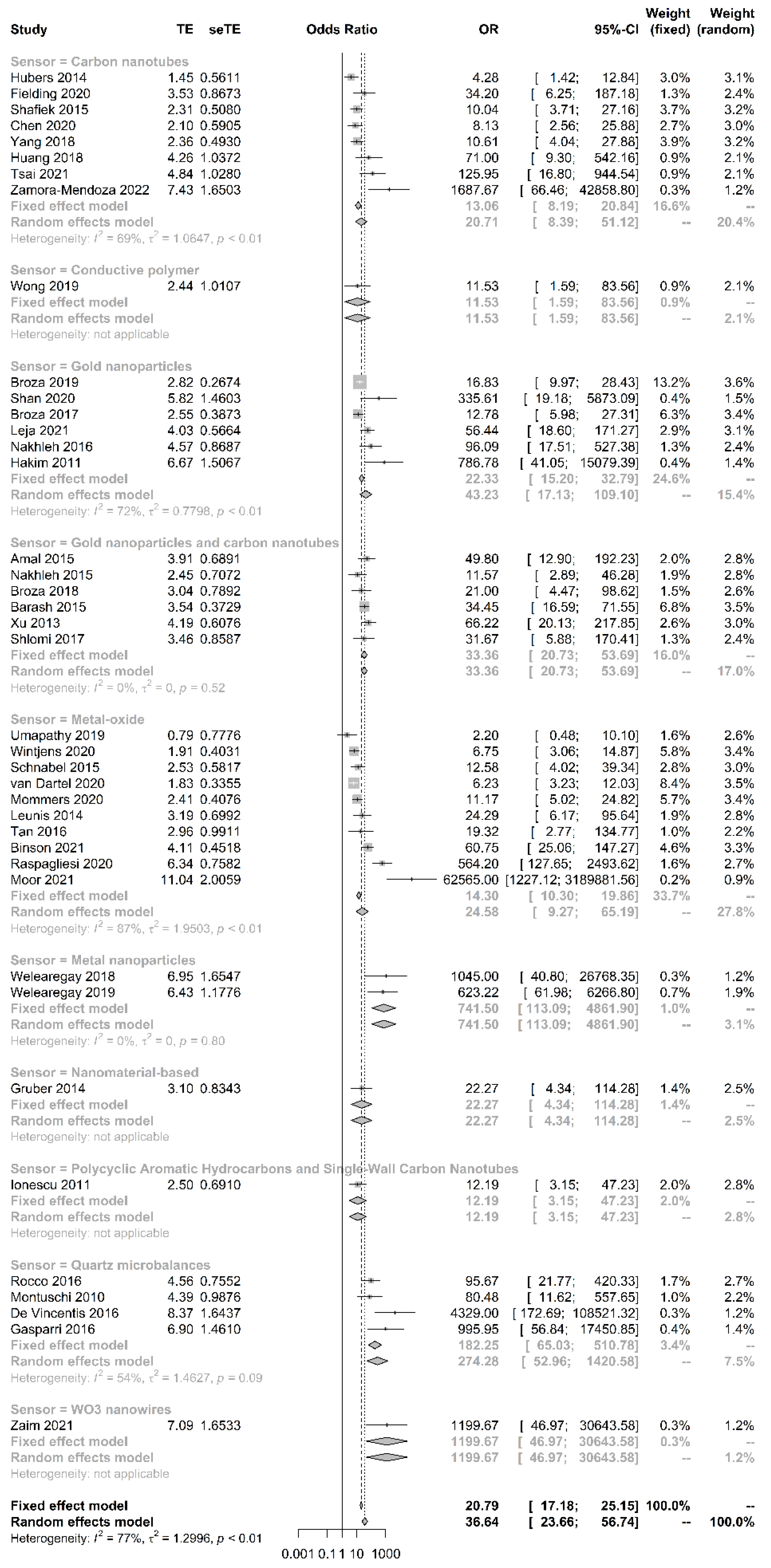
3.1. Pooled Sensitivity, Specificity, ROC and DOR
3.2. Quality Assessment
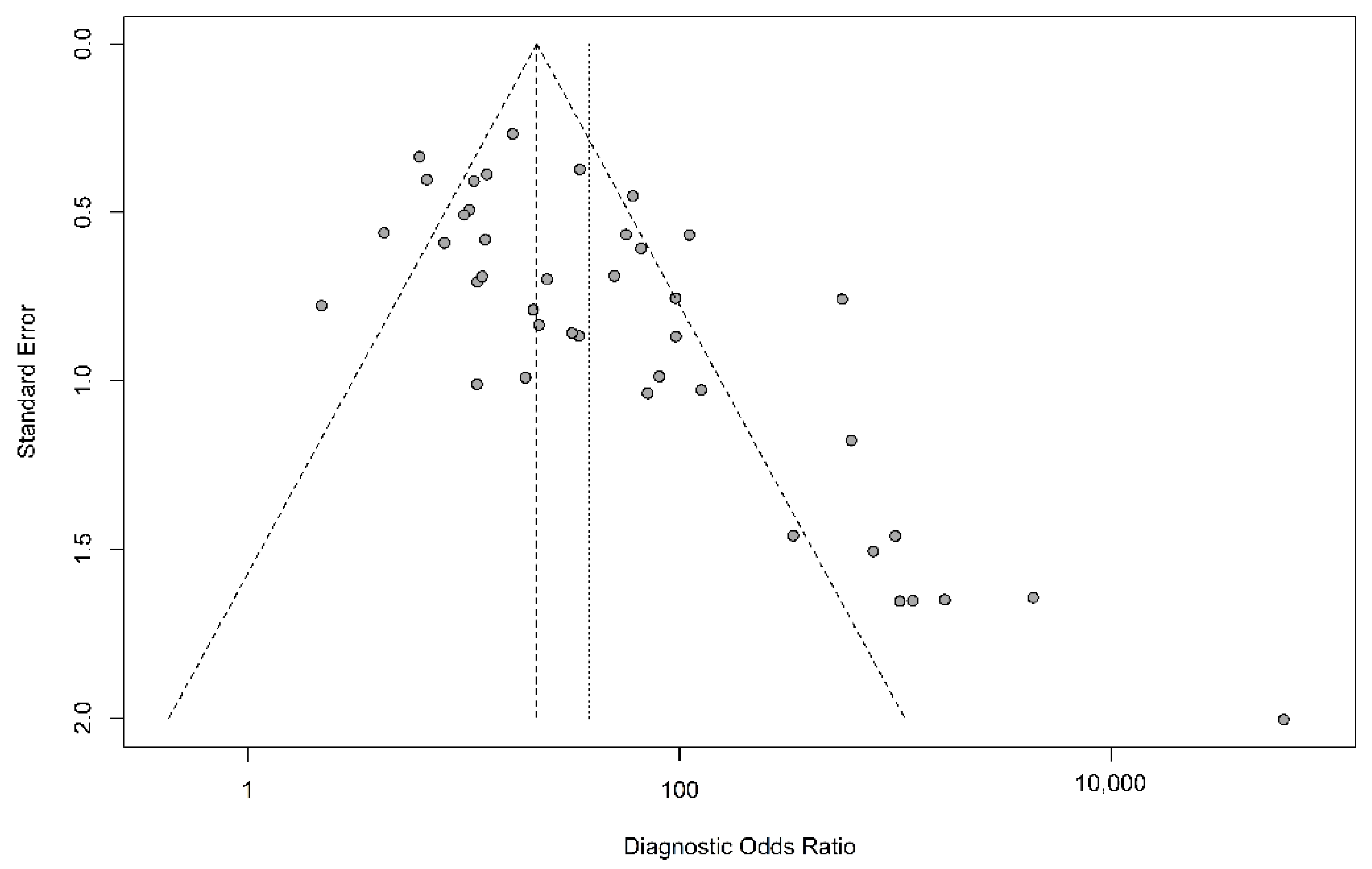
3.3. Sensitivity Analysis
3.4. Subgroup Analysis
4. Discussion
4.1. Summary of Main Results
4.2. Strengths of the Review
4.3. Applicability of Findings to the Review Question
4.4. Limitations
4.5. Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Van der Schee, M.P.; Paff, T.; Brinkman, P.; van Aalderen, W.M.; Haarman, E.G.; Sterk, P.J. Breathomics in lung disease. Chest 2015, 147, 224–231. [Google Scholar] [CrossRef]
- Hakim, M.; Broza, Y.Y.; Barash, O.; Peled, N.; Phillips, M.; Amann, A.; Haick, H. Volatile organic compounds of lung cancer and possible biochemical pathways. Chem. Rev. 2012, 112, 5949–5966. [Google Scholar] [CrossRef] [PubMed]
- Queralto, N.; Berliner, A.N.; Goldsmith, B.; Martino, R.; Rhodes, P.; Lim, S.H. Detecting cancer by breath volatile organic compound analysis: A review of array-based sensors. J. Breath Res. 2014, 8, 027112. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Zeng, C.; Wang, Y.C.; Peng, H.Y.; Lin, C.S.; Chang, C.J.; Yang, H.Y. A Study of diagnostic accuracy using a chemical sensor array and a machine learning technique to detect lung cancer. Sensors 2018, 18, 2845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.Y.; Wang, Y.C.; Peng, H.Y.; Huang, C.H. Breath biopsy of breast cancer using sensor array signals and machine learning analysis. Sci. Rep. 2021, 11, 9. [Google Scholar] [CrossRef]
- Amal, H.; Leja, M.; Funka, K.; Lasina, I.; Skapars, R.; Sivins, A.; Ancans, G.; Kikuste, I.; Vanags, A.; Tolmanis, I.; et al. Breath testing as potential colorectal cancer screening tool. Int. J. Cancer 2016, 138, 229–236. [Google Scholar] [CrossRef]
- Raspagliesi, F.; Bogani, G.; Benedetti, S.; Grassi, S.; Ferla, S.; Buratti, S. Detection of ovarian cancer through exhaled breath by electronic nose: A prospective study. Cancers 2020, 12, 2408. [Google Scholar] [CrossRef] [PubMed]
- Broza, Y.Y.; Khatib, S.; Gharra, A.; Krilaviciute, A.; Amal, H.; Polaka, I.; Parshutin, S.; Kikuste, I.; Gasenko, E.; Skapars, R.; et al. Screening for gastric cancer using exhaled breath samples. Br. J. Surg. 2019, 106, 1122–1125. [Google Scholar] [CrossRef] [PubMed]
- Hakim, M.; Billan, S.; Tisch, U.; Peng, G.; Dvrokind, I.; Marom, O.; Abdah-Bortnyak, R.; Kuten, A.; Haick, H. Diagnosis of head-and-neck cancer from exhaled breath. Br. J. Cancer 2011, 104, 1649–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binson, V.A.; Subramoniam, M.; Mathew, L. Discrimination of COPD and lung cancer from controls through breath analysis using a self-developed e-nose. J. Breath Res. 2021, 15, 10. [Google Scholar] [CrossRef]
- Moor, C.C.; Oppenheimer, J.C.; Nakshbandi, G.; Aerts, J.; Brinkman, P.; Maitland-van der Zee, A.H.; Wijsenbeek, M.S. Exhaled breath analysis by use of eNose technology: A novel diagnostic tool for interstitial Lung disease. Eur. Resp. J. 2021, 57, 8. [Google Scholar] [CrossRef] [PubMed]
- De Vincentis, A.; Pennazza, G.; Santonico, M.; Vespasiani-Gentilucci, U.; Galati, G.; Gallo, P.; Vernile, C.; Pedone, C.; Incalzi, R.A.; Picardi, A. Breath-print analysis by e-nose for classifying and monitoring chronic liver disease: A proof-of-concept study. Sci. Rep. 2016, 6, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.Y.; Lin, W.C.; Yang, H.Y. Diagnosis of ventilator-associated pneumonia using electronic nose sensor array signals: Solutions to improve the application of machine learning in respiratory research. Respir. Res. 2020, 21, 12. [Google Scholar] [CrossRef]
- Shan, B.J.; Broza, Y.Y.; Li, W.J.; Wang, Y.; Wu, S.H.; Liu, Z.Z.; Wang, J.; Gui, S.Y.; Wang, L.; Zhang, Z.H.; et al. Multiplexed nanomaterial-based sensor array for detection of COVID-19 in exhaled breath. ACS Nano 2020, 14, 12125–12132. [Google Scholar] [CrossRef] [PubMed]
- Haick, H.; Broza, Y.Y.; Mochalski, P.; Ruzsanyi, V.; Amann, A. Assessment, origin, and implementation of breath volatile cancer markers. Chem. Soc. Rev. 2014, 43, 1423–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Sar, I.G.; Wijbenga, N.; Nakshbandi, G.; Aerts, J.; Manintveld, O.C.; Wijsenbeek, M.S.; Hellemons, M.E.; Moor, C.C. The smell of lung disease: A review of the current status of electronic nose technology. Respir. Res. 2021, 22, 246. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; Group, Q. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Review Manager (RevMan) [Computer Program]. Version 5.4, The Cochrane Collaboration, 2020. Available online: https://training.cochrane.org/ (accessed on 19 November 2021).
- Harbord, R.M.; Whiting, P.; Sterne, J.A.; Egger, M.; Deeks, J.J.; Shang, A.; Bachmann, L.M. An empirical comparison of methods for meta-analysis of diagnostic accuracy showed hierarchical models are necessary. J. Clin. Epidemiol. 2008, 61, 1095–1103. [Google Scholar] [CrossRef]
- Simundic, A.M. Measures of diagnostic accuracy: Basic definitions. EJIFCC 2009, 19, 203–211. [Google Scholar] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Jackson, D.; White, I.R.; Thompson, S.G. Extending DerSimonian and Laird’s methodology to perform multivariate random effects meta-analyses. Stat. Med. 2010, 29, 1282–1297. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Comparison of two methods to detect publication bias in meta-analysis. JAMA 2006, 295, 676–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- Mommers, E.H.H.; van Kooten, L.; Nienhuijs, S.W.; de Vries Reilingh, T.S.; Lubbers, T.; Mees, B.M.E.; Schurink, G.W.H.; Bouvy, N.D. Can electric nose breath analysis identify abdominal wall hernia recurrence and aortic aneurysms? A proof-of-concept study. Surg. Innov. 2020, 27, 366–372. [Google Scholar] [CrossRef]
- Wong, D.C.; Relton, S.D.; Lane, V.; Ismail, M.; Goss, V.; Bytheway, J.; West, R.M.; Deuchars, J.; Sutcliffe, J. Bedside breath tests in children with abdominal pain: A prospective pilot feasibility study. Pilot Feasibility Stud. 2019, 5, 121. [Google Scholar] [CrossRef] [Green Version]
- Montuschi, P.; Santonico, M.; Mondino, C.; Pennazza, G.; Mantini, G.; Martinelli, E.; Capuano, R.; Ciabattoni, G.; Paolesse, R.; Di Natale, C.; et al. Diagnostic performance of an electronic nose, fractional exhaled nitric oxide, and lung function testing in asthma. Chest 2010, 137, 790–796. [Google Scholar] [CrossRef]
- Barash, O.; Zhang, W.; Halpern, J.M.; Hua, Q.L.; Pan, Y.Y.; Kayal, H.; Khoury, K.; Liu, H.; Davies, M.P.; Haick, H. Differentiation between genetic mutations of breast cancer by breath volatolomics. Oncotarget 2015, 6, 44864–44876. [Google Scholar] [CrossRef] [Green Version]
- Fielding, D.; Hartel, G.; Pass, D.; Davis, M.; Brown, M.; Dent, A.; Agnew, J.; Dickie, G.; Ware, R.S.; Hodge, R. Volatile organic compound breath testing detects in-situ squamous cell carcinoma of bronchial and laryngeal regions and shows distinct profiles of each tumour. J. Breath Res. 2020, 14, 13. [Google Scholar] [CrossRef]
- Shafiek, H.; Fiorentino, F.; Merino, J.L.; López, C.; Oliver, A.; Segura, J.; de Paul, I.; Sibila, O.; Agustí, A.; Cosío, B.G. Using the electronic nose to identify airway infection during COPD exacerbations. PLoS ONE 2015, 10, e0135199. [Google Scholar] [CrossRef] [Green Version]
- Welearegay, T.G.; Diouani, M.F.; Osterlund, L.; Ionescu, F.; Belgacem, K.; Smadhi, H.; Khaled, S.; Kidar, A.; Cindemir, U.; Laouini, D.; et al. Ligand-Capped Ultrapure Metal nanoparticle sensors for the detection of cutaneous Leishmaniasis disease in exhaled breath. ACS Sens. 2018, 3, 2532–2540. [Google Scholar] [CrossRef]
- Welearegay, T.G.; Diouani, M.F.; Osterlund, L.; Borys, S.; Khaled, S.; Smadhi, H.; Ionescu, F.; Bouchekoua, M.; Aloui, D.; Laouini, D.; et al. Diagnosis of human echinococcosis via exhaled breath analysis: A promise for rapid diagnosis of infectious diseases caused by Helminths. J. Infect. Dis. 2019, 219, 101–109. [Google Scholar] [CrossRef]
- Van Dartel, D.; Schelhaas, H.J.; Colon, A.J.; Kho, K.H.; de Vos, C.C. Breath analysis in detecting epilepsy. J. Breath Res. 2020, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.Q.; Broza, Y.Y.; Ionsecu, R.; Tisch, U.; Ding, L.; Liu, H.; Song, Q.; Pan, Y.Y.; Xiong, F.X.; Gu, K.S.; et al. A nanomaterial-based breath test for distinguishing gastric cancer from benign gastric conditions. Br. J. Cancer 2013, 108, 941–950. [Google Scholar] [CrossRef] [Green Version]
- Leja, M.; Kortelainen, J.M.; Polaka, I.; Turppa, E.; Mitrovics, J.; Padilla, M.; Mochalski, P.; Shuster, G.; Pohle, R.; Kashanin, D.; et al. Sensing gastric cancer via point-of-care sensor breath analyzer. Cancer 2021, 127, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Umapathy, S.; Nasimsha, N.; Kumar, M.; Kalidoss, R.; Thomas, A.C.; Lakshmi, M.; Gafoor, E.R. Design and development of portable prototype for human breath analysis: A comparative study between haemodialysis patients and healthy subjects. Biomed. Phys. Eng. Express 2019, 5, 9. [Google Scholar] [CrossRef]
- Gruber, M.; Tisch, U.; Jeries, R.; Amal, H.; Hakim, M.; Ronen, O.; Marshak, T.; Zimmerman, D.; Israel, O.; Amiga, E.; et al. Analysis of exhaled breath for diagnosing head and neck squamous cell carcinoma: A feasibility study. Br. J. Cancer 2014, 111, 790–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leunis, N.; Boumans, M.L.; Kremer, B.; Din, S.; Stobberingh, E.; Kessels, A.G.H.; Kross, K.W. Application of an electronic nose in the diagnosis of head and neck cancer. Laryngoscope 2014, 124, 1377–1381. [Google Scholar] [CrossRef] [Green Version]
- Finamore, P.; Pedone, C.; Lelli, D.; Costanzo, L.; Bartoli, I.R.; De Vincentis, A.; Grasso, S.; Parente, F.R.; Pennazza, G.; Santonico, M.; et al. Analysis of volatile organic compounds: An innovative approach to heart failure characterization in older patients. J. Breath Res. 2018, 12, 8. [Google Scholar] [CrossRef]
- Zaim, O.; Diouf, A.; El Bari, N.; Lagdali, N.; Benelbarhdadi, I.; Ajana, F.Z.; Llobet, E.; Bouchikhi, B. Comparative analysis of volatile organic compounds of breath and urine for distinguishing patients with liver cirrhosis from healthy controls by using electronic nose and voltammetric electronic tongue. Anal. Chim. Acta 2021, 1184, 339028. [Google Scholar] [CrossRef]
- Gasparri, R.; Santonico, M.; Valentini, C.; Sedda, G.; Borri, A.; Petrella, F.; Maisonneuve, P.; Pennazza, G.; D’Amico, A.; Di Natale, C.; et al. Volatile signature for the early diagnosis of lung cancer. J. Breath Res. 2016, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Hubers, A.J.; Brinkman, P.; Boksem, R.J.; Rhodius, R.J.; Witte, B.I.; Zwinderman, A.H.; Heideman, D.A.M.; Duin, S.; Koning, R.; Steenbergen, R.D.M.; et al. Combined sputum hypermethylation and eNose analysis for lung cancer diagnosis. J. Clin. Pathol. 2014, 67, 707–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kononov, A.; Korotetsky, B.; Jahatspanian, I.; Gubal, A.; Vasiliev, A.; Arsenjev, A.; Nefedov, A.; Barchuk, A.; Gorbunov, I.; Kozyrev, K.; et al. Online breath analysis using metal oxide semiconductor sensors (electronic nose) for diagnosis of lung cancer. J. Breath Res. 2020, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Rocco, R.; Incalzi, R.A.; Pennazza, G.; Santonico, M.; Pedone, C.; Bartoli, I.R.; Vernile, C.; Mangiameli, G.; La Rocca, A.; De Luca, G.; et al. BIONOTE e-nose technology may reduce false positives in lung cancer screening programmes. Eur. J. Cardio-Thorac. Surg. 2016, 49, 1112–1117; discussion 1117. [Google Scholar] [CrossRef] [Green Version]
- Shlomi, D.; Abud, M.; Liran, O.; Bar, J.; Gai-Mor, N.; Ilouze, M.; Onn, A.; Ben-Nun, A.; Haick, H.; Peled, N. Detection of Lung Cancer and EGFR Mutation by Electronic Nose System. J. Thorac. Oncol. 2017, 12, 1544–1551. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.L.; Yong, Z.X.; Liam, C.K. Using a chemiresistor-based alkane sensor to distinguish exhaled breaths of lung cancer patients from subjects with no lung cancer. J. Thorac. Dis. 2016, 8, 2772–2783. [Google Scholar] [CrossRef] [Green Version]
- Broza, Y.Y.; Har-Shai, L.; Jeries, R.; Cancilla, J.C.; Glass-Marmor, L.; Lejbkowicz, I.; Torrecilla, J.S.; Yao, X.L.; Feng, X.L.; Narita, A.; et al. Exhaled Breath Markers for Nonimaging and Noninvasive Measures for Detection of Multiple Sclerosis. ACS Chem. Neurosci. 2017, 8, 2402–2413. [Google Scholar] [CrossRef]
- Nakhleh, M.K.; Badarny, S.; Winer, R.; Jeries, R.; Finberg, J.; Haick, H. Distinguishing idiopathic Parkinson’s disease from other parkinsonian syndromes by breath test. Parkinsonism Relat. Disord. 2015, 21, 150–153. [Google Scholar] [CrossRef]
- Ionescu, R.; Broza, Y.; Shaltieli, H.; Sadeh, D.; Zilberman, Y.; Feng, X.; Glass-Marmor, L.; Lejbkowicz, I.; Müllen, K.; Miller, A.; et al. Detection of multiple sclerosis from exhaled breath using bilayers of polycyclic aromatic hydrocarbons and single-wall carbon nanotubes. ACS Chem. Neurosci. 2011, 2, 687–693. [Google Scholar] [CrossRef] [Green Version]
- Amal, H.; Shi, D.Y.; Ionescu, R.; Zhang, W.; Hua, Q.L.; Pan, Y.Y.; Tao, L.; Liu, H.; Haick, H. Assessment of ovarian cancer conditions from exhaled breath. Int. J. Cancer 2015, 136, E614–E622. [Google Scholar] [CrossRef]
- Yang, H.Y.; Peng, H.Y.; Chang, C.J.; Chen, P.C. Diagnostic accuracy of breath tests for pneumoconiosis using an electronic nose. J. Breath Res. 2018, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Nakhleh, M.K.; Baram, S.; Jeries, R.; Salim, R.; Haick, H.; Hakim, M. Artificially intelligent nanoarray for the detection of preeclampsia under real-world clinical conditions. Adv. Mater. Technol. 2016, 1, 1600132. [Google Scholar] [CrossRef]
- Broza, Y.Y.; Braverman, I.; Haick, H. Breath volatolomics for diagnosing chronic rhinosinusitis. Int. J. Nanomed. 2018, 13, 4661–4670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamora-Mendoza, B.N.; de Leon-Martinez, L.D.; Rodriguez-Aguilar, M.; Mizaikoff, B.; Flores-Ramirez, R. Chemometric analysis of the global pattern of volatile organic compounds in the exhaled breath of patients with COVID-19, post-COVID and healthy subjects. Proof of concept for post-COVID assessment. Talanta 2022, 236, 9. [Google Scholar] [CrossRef] [PubMed]
- Wintjens, A.; Hintzen, K.F.H.; Engelen, S.M.E.; Lubbers, T.; Savelkoul, P.H.M.; Wesseling, G.; van der Palen, J.A.M.; Bouvy, N.D. Applying the electronic nose for pre-operative SARS-CoV-2 screening. Surg. Endosc. 2020, 8. [Google Scholar] [CrossRef]
- Tsai, Y.G.; Shie, R.H.; Huang, C.H.; Chen, C.D.; Lin, W.C.; Yang, H.Y. Use of the electronic nose to screen for small airway dysfunction in schoolchildren. Sens. Actuator B Chem. 2021, 345, 8. [Google Scholar] [CrossRef]
- Schnabel, R.M.; Boumans, M.L.L.; Smolinska, A.; Stobberingh, E.E.; Kaufmann, R.; Roekaerts, P.; Bergmans, D. Electronic nose analysis of exhaled breath to diagnose ventilator-associated pneumonia. Respir. Med. 2015, 109, 1454–1459. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.; Rutjes, A.W.; Reitsma, J.B.; Glas, A.S.; Bossuyt, P.M.; Kleijnen, J. Sources of variation and bias in studies of diagnostic accuracy: A systematic review. Ann. Int. Med. 2004, 140, 189–202. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Disease | Sensor | Case | Control | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| Mommers [26], 2020 | Aneurysm and recurrent hernia | Metal-oxide | 64 a | 74 | 0.81 | 0.73 |
| Wong [27], 2019 | Appendicitis | Conductive polymer | 5 | 45 | 0.8 | 0.8 |
| Montuschi [28], 2010 | Asthma | Quartz microbalances | 30 | 21 | 0.87 | 0.95 |
| Barash [29], 2015 | Breast cancer | Gold nanoparticles and carbon nanotubes | 169 | 82 | 0.88 | 0.83 |
| Yang [5], 2021 | Breast cancer | Carbon nanotubes | 70 b | 18 a | 0.86 b | 0.97 b |
| Fielding [30], 2020 | Bronchial and laryngeal cancer | Carbon nanotubes | 42 | 13 | 0.95 | 0.69 |
| Amal [6], 2016 | Colorectal cancer | Gold nanoparticles and carbon nanotubes | 20 b | 36 b | 0.94 b | 0.91 b |
| Shafiek [31], 2015 | COPD | Carbon nanotubes | 124 | 30 | 0.69 | 0.75 |
| Binson [10], 2021 | COPD and lung cancer | Metal-oxide | 70 | 144 | 0.81 | 0.94 |
| Welearegay [32], 2018 | Cutaneous leishmaniasis | Metal nanoparticles | 28 a | 28 | 0.96 | 1 |
| Welearegay [33], 2019 | Echinococcosis | Metal nanoparticles | 36 | 40 | 0.97 | 0.98 |
| van Dartel [34], 2020 | Epilepsy | Metal-oxide | 74 | 110 | 0.76 | 0.67 |
| Broza [8], 2019 | Gastric cancer | Gold nanoparticles | 102 | 1065 | 0.82 | 0.79 |
| Xu [35], 2013 | Gastric cancer | Gold nanoparticles and carbon nanotubes | 37 | 93 | 0.89 | 0.9 |
| Leja [36], 2021 | Gastric cancer | Gold nanoparticles | 47 | 105 | 0.92 | 0.86 |
| Umapathy [37], 2019 | Haemodialysis | Metal-oxide | 21 | 17 | 0.86 | 0.29 |
| Gruber [38], 2014 | Head and neck cancer | Nanomaterial-based sensor | 22 | 19 | 0.77 | 0.9 |
| Leunis [39], 2014 | Head and neck cancer | Metal-oxide | 36 | 23 | 0.9 | 0.8 |
| Hakim [9], 2011 | Head-and-neck cancer and lung cancer | Gold nanoparticles | 36 a | 52 | 1 | 0.92 |
| Finamore [40], 2018 | Heart failure | Quartz microbalances | 30 b | 39 b | 0.8 b | 0.82 b |
| Moor [11], 2021 | Interstitial lung disease | Metal-oxide | 322 | 48 | 1 | 1 |
| De Vincentis [12], 2016 | Liver cirrhosis | Quartz microbalances | 58 | 56 | 1 | 0.98 |
| Zaim [41], 2021 | Liver cirrhosis | WO3 nanowires | 22 | 32 | 0.97 | 1 |
| Gasparri [42], 2016 | Lung cancer | Quartz microbalances | 72 | 74 | 0.88 | 1 |
| Huang [4], 2018 | Lung cancer | Carbon nanotubes | 56 | 188 | 0.92 | 0.93 |
| Hubers [43], 2014 | Lung cancer | Carbon nanotubes | 38 | 39 | 0.87 | 0.43 |
| Kononov [44], 2020 | Lung cancer | Metal-oxide | 19 b | 17 b | 0.95 b | 1 b |
| Rocco [45], 2016 | Lung cancer | Quartz microbalances | 23 | 77 | 0.86 | 0.95 |
| Shlomi [46], 2017 | Lung cancer | Gold nanoparticles and carbon nanotubes | 16 | 30 | 0.75 | 0.93 |
| Tan [47], 2016 | Lung cancer | Metal-oxide | 12 | 13 | 0.83 | 0.88 |
| Broza et al. [48], 2017 | Multiple sclerosis | Gold nanoparticles | 128 | 58 | 0.76 | 0.81 |
| Nakhleh et al. [49], 2015 | Parkinson’s disease | Gold nanoparticles and carbon nanotubes | 16 | 37 | 0.81 | 0.76 |
| Ionescu et al. [50], 2011 | Multiple sclerosis | Polycyclic aromatic hydrocarbons and single-wall carbon nanotubes | 34 | 17 | 0.85 | 0.71 |
| Amal et al. [51], 2015 | Ovarian cancer | Gold nanoparticles and carbon nanotubes | 48 | 48 | 0.85 | 0.65 |
| Raspagliesi et al. [7], 2020 | Ovarian cancer | Metal-oxide | 86 | 114 | 0.98 | 0.95 |
| Yang et al. [52], 2018 | Pneumoconiosis | Carbon nanotubes | 34 | 64 | 0.68 | 0.84 |
| Nakhleh et al. [53], 2016 | Preeclampsia | Gold nanoparticles | 31 | 31 | 0.92 | 0.91 |
| Broza et al. [54], 2018 | Rhinosinusitis | Gold nanoparticles and carbon nanotubes | 17 | 30 | 0.76 | 0.8 |
| Zamora-Mendoza et al. [55], 2022 | SARS-CoV-2 | Carbon nanotubes | 42 | 30 | 0.97 | 1 |
| Shan et al. [14], 2020 | SARS-CoV-2 | Gold nanoparticles | 41 | 57 | 1 | 0.81 |
| Wintjens et al. [56], 2020 | SARS-CoV-2 | Metal-oxide | 57 | 162 | 0.86 | 0.54 |
| Tsai et al. [57], 2021 | Small airway dysfunction | Carbon nanotubes | 12 | 60 | 0.92 | 0.95 |
| Chen et al. [13], 2020 | Ventilator-associated pneumonia | Carbon nanotubes | 33 | 26 | 0.72 | 0.77 |
| Schnabel et al. [58], 2015 | Ventilator-associated pneumonia | Metal-oxide | 33 | 53 | 0.88 | 0.66 |
| Type 1 | Sensitivity (95% CI) | I2 | Specificity (95% CI) | I2 |
|---|---|---|---|---|
| Carbon nanotube (n = 8) | 0.86 (0.75, 0.93) | 69.4% | 0.86 (0.71, 0.94) | 82.1% |
| Conductive polymer (n = 1) | 0.80 (0.31, 0.97) | NA | 0.80 (0.66, 0.89) | NA |
| Gold nanoparticles (n = 6) | 0.94 (0.80, 0.98) | 39.8% | 0.83 (0.78, 0.88) | 48.5% |
| Gold nanoparticles and carbon nanotube (n = 6) | 0.86 (0.82, 0.90) | 0.0% | 0.87 (0.82, 0.91) | 32.5% |
| Metal-oxide (n = 10) | 0.91 (0.81, 0.96) | 35.2% | 0.81 (0.63, 0.91) | 89.5% |
| Metal nanoparticles (n = 2) | 0.97 (0.88, 099) | 0.0% | 0.99 (0.90, 1.00) | 0.0% |
| Nanomaterial-based (n = 1) | 0.77 (0.56, 0.90) | NA | 0.89 (0.66, 0.97) | NA |
| Polycyclic aromatic hydrocarbons and single wall carbon nanotubes (n = 1) | 0.85 (0.69, 0.94) | NA | 0.71 (0.46, 0.87) | NA |
| Quartz microbalances (n = 4) | 0.93 (0.81, 0.97) | 0.0% | 0.98 (0.93, 0.99) | 0.0% |
| WO3 nanowires (n = 1) | 0.97 (0.80, 1.00) | NA | 1.00 (0.00–1.00) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.-Y.; Chen, W.-C.; Tsai, R.-C. Accuracy of the Electronic Nose Breath Tests in Clinical Application: A Systematic Review and Meta-Analysis. Biosensors 2021, 11, 469. https://doi.org/10.3390/bios11110469
Yang H-Y, Chen W-C, Tsai R-C. Accuracy of the Electronic Nose Breath Tests in Clinical Application: A Systematic Review and Meta-Analysis. Biosensors. 2021; 11(11):469. https://doi.org/10.3390/bios11110469
Chicago/Turabian StyleYang, Hsiao-Yu, Wan-Chin Chen, and Rodger-Chen Tsai. 2021. "Accuracy of the Electronic Nose Breath Tests in Clinical Application: A Systematic Review and Meta-Analysis" Biosensors 11, no. 11: 469. https://doi.org/10.3390/bios11110469
APA StyleYang, H.-Y., Chen, W.-C., & Tsai, R.-C. (2021). Accuracy of the Electronic Nose Breath Tests in Clinical Application: A Systematic Review and Meta-Analysis. Biosensors, 11(11), 469. https://doi.org/10.3390/bios11110469