Niosomal Drug Delivery Systems for Ocular Disease—Recent Advances and Future Prospects

 , , and
, , and 
Abstract
1. Introduction
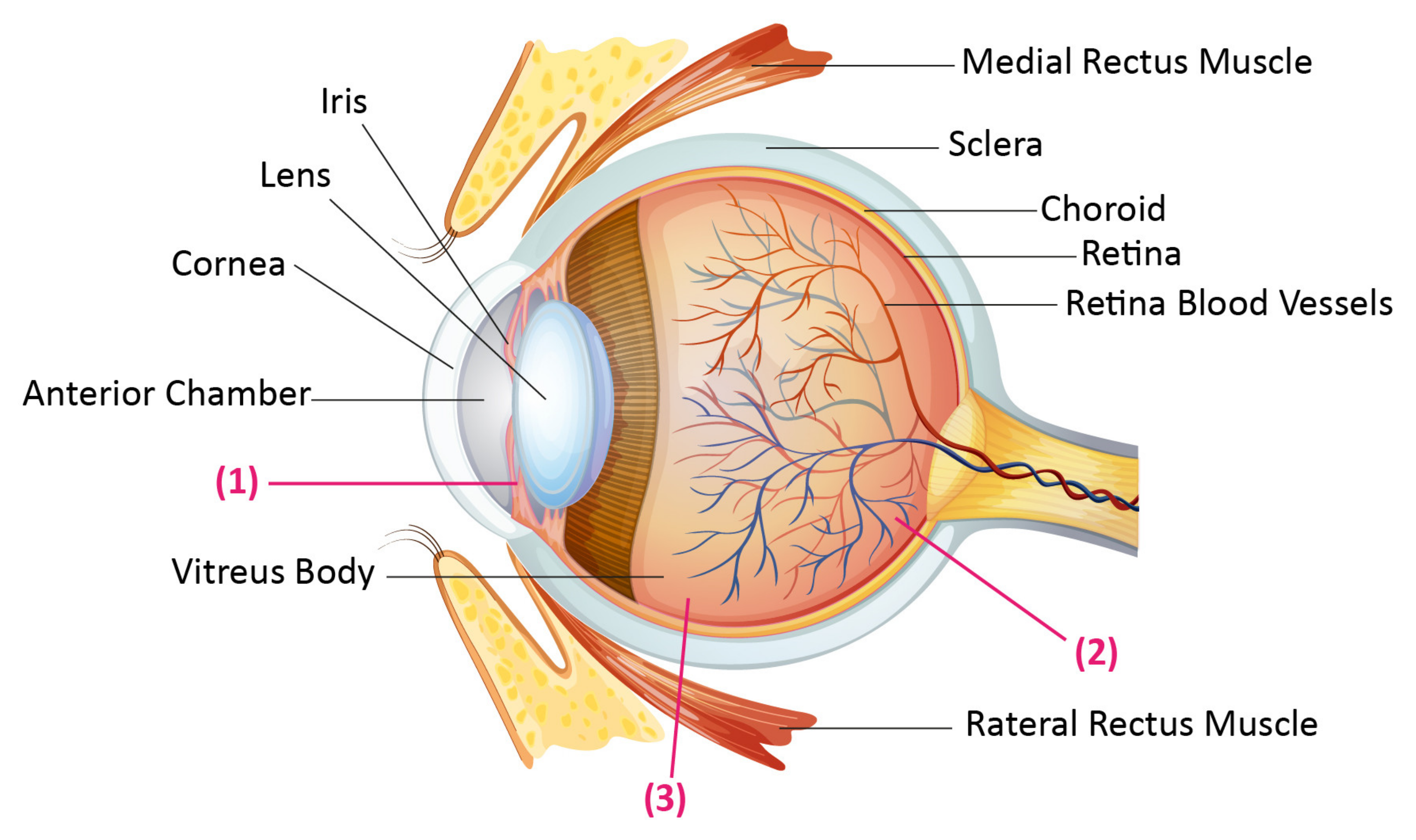
2. Anatomy of Eye and the Challenges of Drug Delivery to Eye
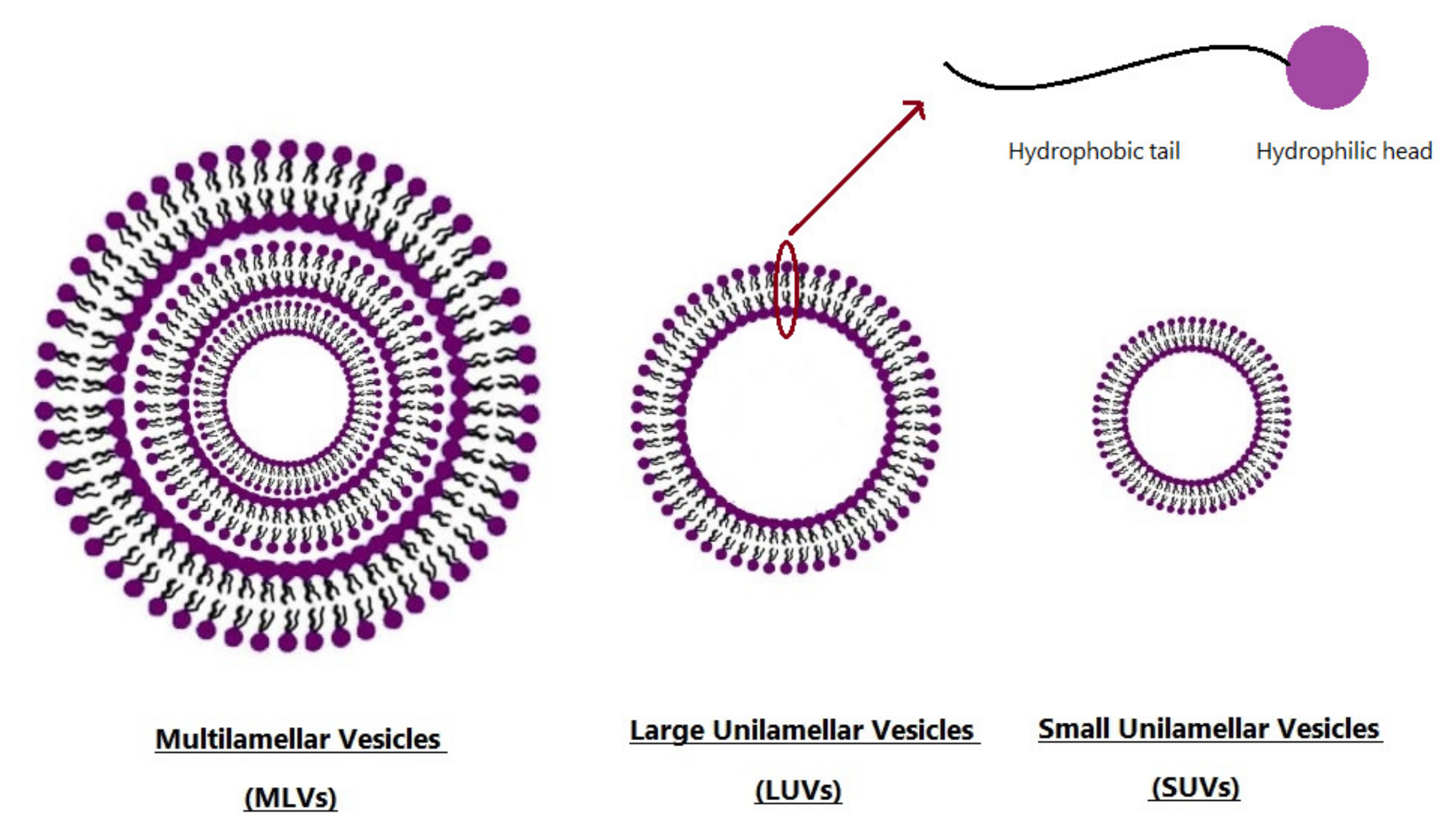
3. Niosomes as New Drug Delivery Systems
3.1. Preparation of Niosomes
3.1.1. Thin-Film Hydration (TFH) Method
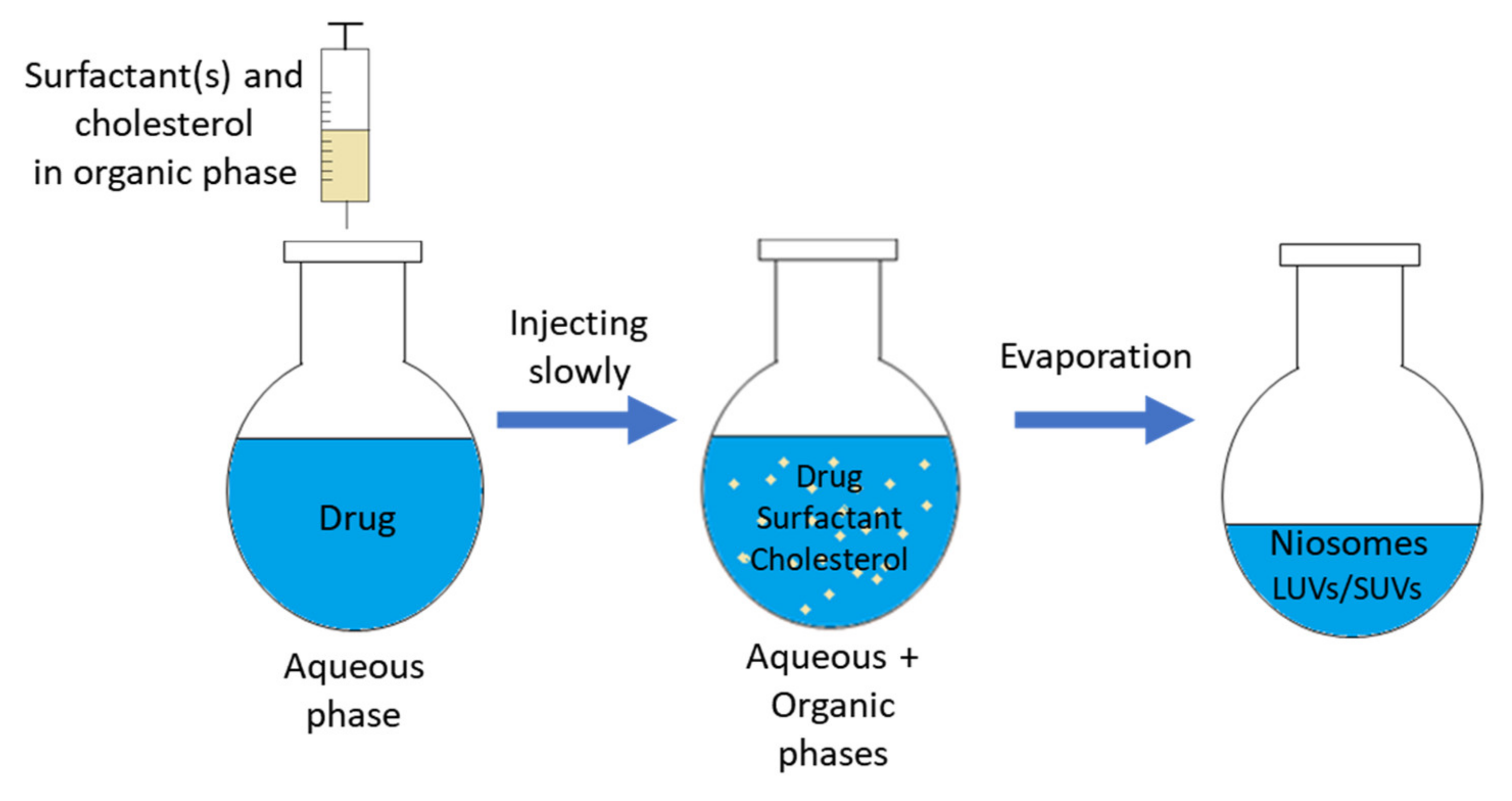
3.1.2. Solvent Injection (SI) Method
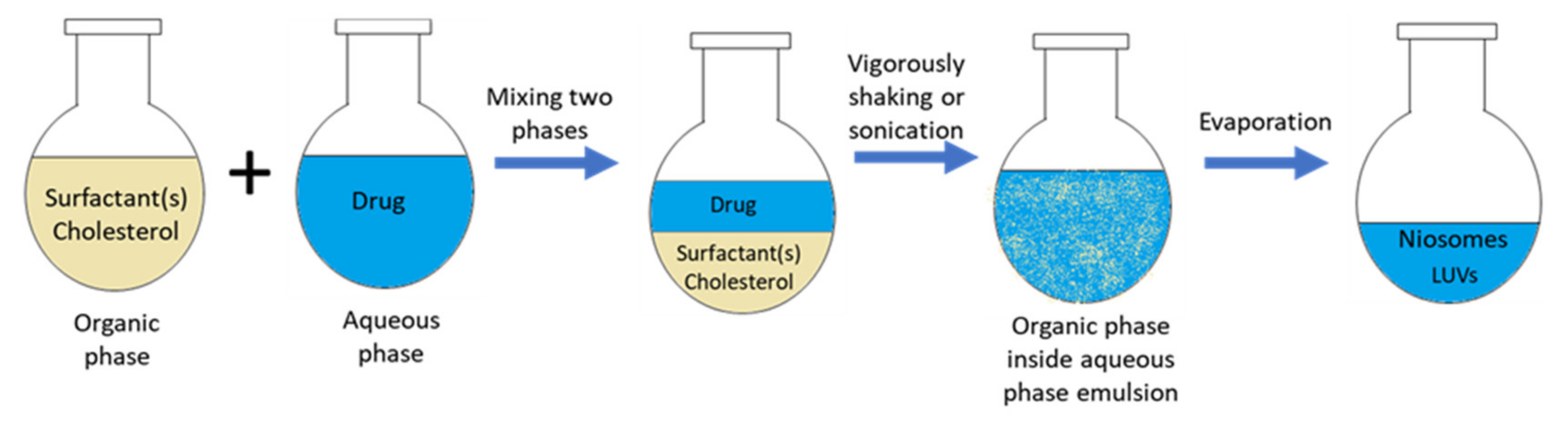
3.1.3. Reverse Phase Evaporation (REV) Method
3.1.4. The Bubble Method
3.1.5. Freeze and Thaw Method
3.1.6. Dehydration–Rehydration Vesicles (DRV) Method
3.1.7. Microfluidization Method
3.1.8. Supercritical Carbon Dioxide Fluid (scCO2) Method
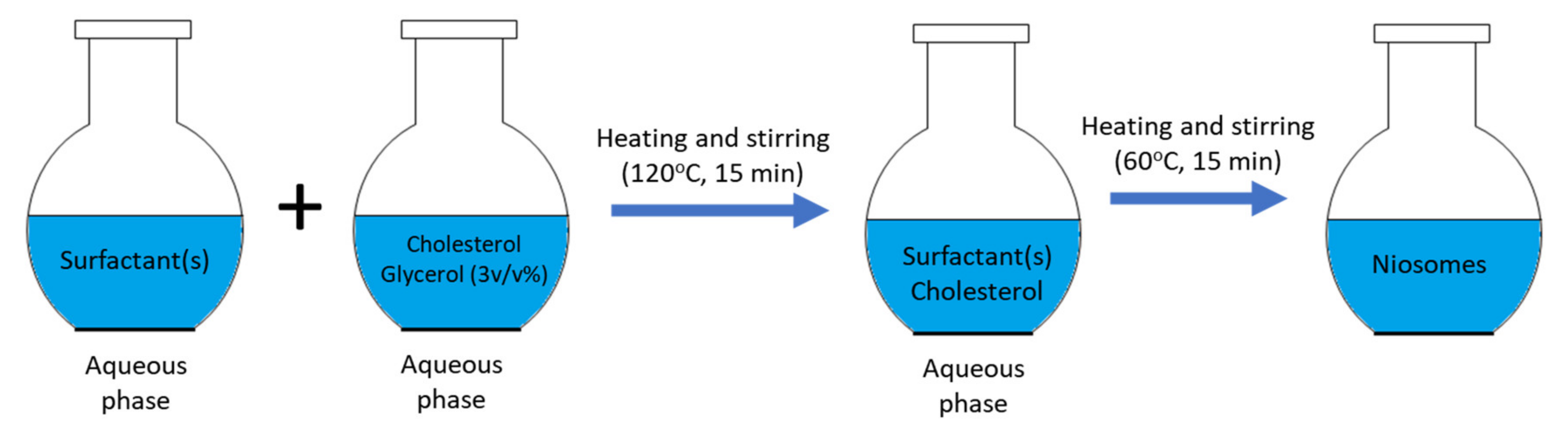
3.1.9. Heating Method (HM)
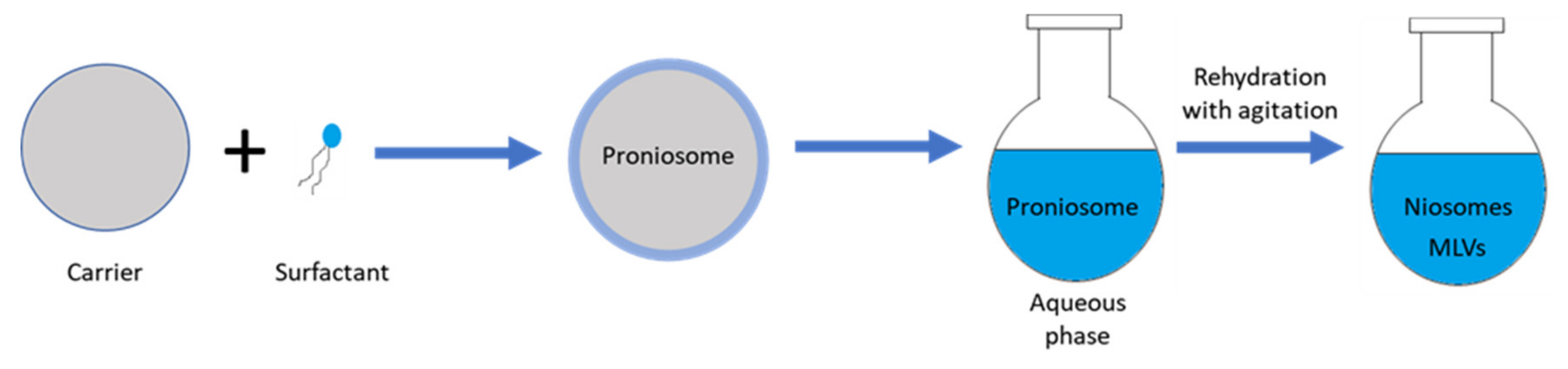
3.1.10. Pronisome Method
3.2. Niosome Drug Loading Methods
3.2.1. Passive Loading
3.2.2. Active Loading (Remote Loading)
3.3. Characterization of Niosomes
3.3.1. Average Size, Size Distribution, and Morphology
3.3.2. Charge of Niosomes
3.3.3. Entrapment Efficiency
3.3.4. Stability of Niosomes
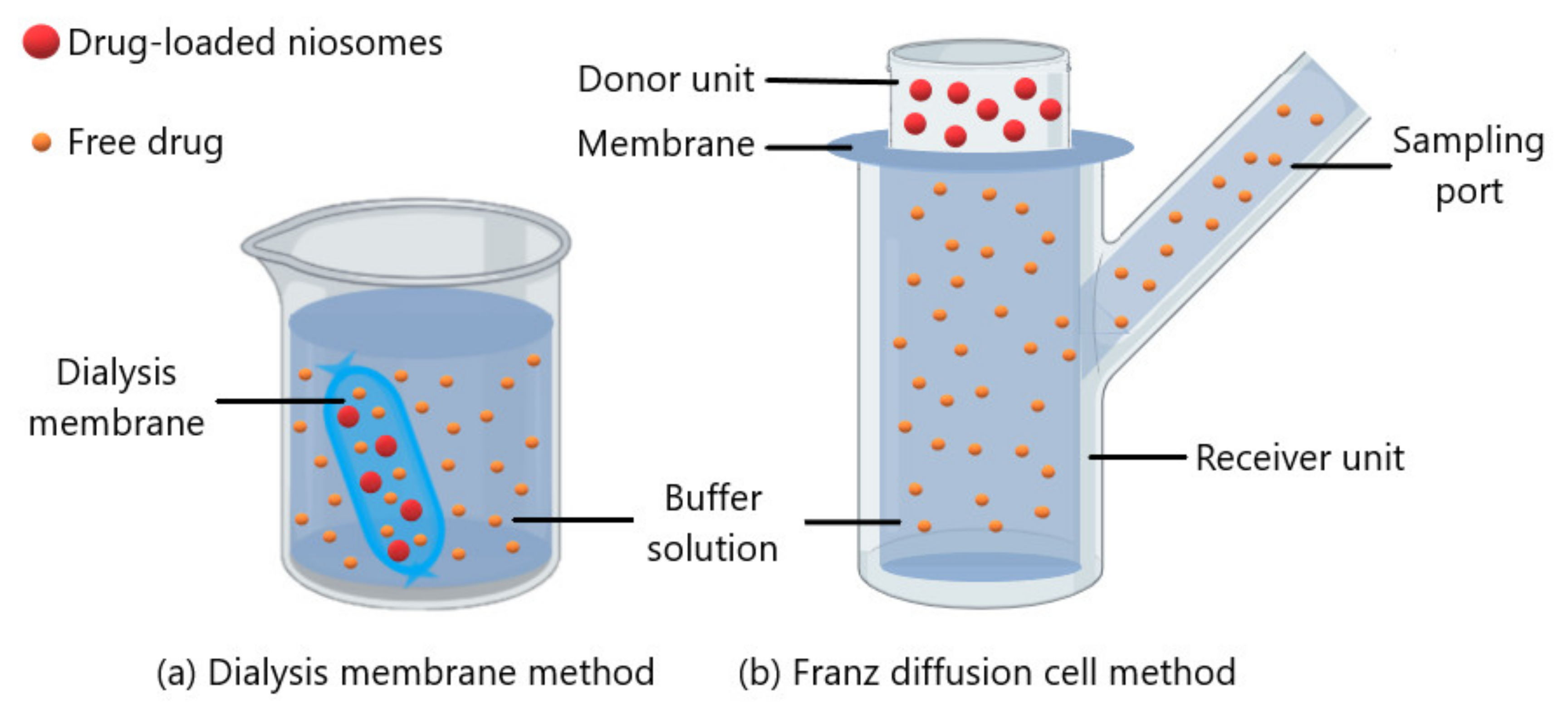
3.3.5. In Vitro Release
4. Niosome Based Treatment Strategies in Ocular Diseases
4.1. Glaucoma
4.2. Conjunctivitis
4.3. Retinal Diseases
4.4. Keratitis
5. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Urtti, A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Lajunen, T.; Nurmi, R.; Kontturi, L.; Viitala, L.; Yliperttula, M.; Murtomaki, L.; Urtti, A. Light activated liposomes: Functionality and prospects in ocular drug delivery. J. Control. Release 2016, 244, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Del Amo, E.M.; Urtti, A. Current and future ophthalmic drug delivery systems. A shift to the posterior segment. Drug Discov. Today 2008, 13, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Yetisgin, A.A.; Cetinel, S.; Zuvin, M.; Kosar, A.; Kutlu, O. Therapeutic Nanoparticles and Their Targeted Delivery Applications. Molecules 2020, 25, 2193. [Google Scholar] [CrossRef]
- Sharaf, M.G.; Cetinel, S.; Heckler, L.; Damji, K.; Unsworth, L.; Montemagno, C. Nanotechnology-Based Approaches for Ophthalmology Applications: Therapeutic and Diagnostic Strategies. Asia Pac. J. Ophthalmol. (Phila) 2014, 3, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Tagalakis, A.D.; Madaan, S.; Larsen, S.D.; Neubig, R.R.; Khaw, P.T.; Rodrigues, I.; Goyal, S.; Lim, K.S.; Yu-Wai-Man, C. In vitro and in vivo delivery of a sustained release nanocarrier-based formulation of an MRTF/SRF inhibitor in conjunctival fibrosis. J. Nanobiotechnol. 2018, 16, 97. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, J.V.; Darwitan, A.; Barathi, V.A.; Ang, M.; Htoon, H.M.; Boey, F.; Tam, K.C.; Wong, T.T.; Venkatraman, S.S. Sustained drug release in nanomedicine: A long-acting nanocarrier-based formulation for glaucoma. ACS Nano 2014, 8, 419–429. [Google Scholar] [CrossRef]
- Vaishya, R.D.; Khurana, V.; Patel, S.; Mitra, A.K. Controlled ocular drug delivery with nanomicelles. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2014, 6, 422–437. [Google Scholar] [CrossRef]
- Juliana, F.R.; Kesse, S.; Boakye-Yiadom, K.O.; Veroniaina, H.; Wang, H.; Sun, M. Promising Approach in the Treatment of Glaucoma Using Nanotechnology and Nanomedicine-Based Systems. Molecules 2019, 24, 3805. [Google Scholar] [CrossRef]
- Wakshull, E.; Quarmby, V.; Mahler, H.C.; Rivers, H.; Jere, D.; Ramos, M.; Szczesny, P.; Bechtold-Peters, K.; Masli, S.; Gupta, S. Advancements in Understanding Immunogenicity of Biotherapeutics in the Intraocular Space. AAPS J. 2017, 19, 1656–1668. [Google Scholar] [CrossRef]
- Willoughby, C.E.; Ponzin, D.; Ferrari, S.; Lobo, A.; Landau, K.; Omidi, Y. Anatomy and physiology of the human eye: Effects of mucopolysaccharidoses disease on structure and function-a review. Clin. Exp. Ophthalmol. 2010, 38, 2–11. [Google Scholar] [CrossRef]
- Rodrigues, G.A.; Lutz, D.; Shen, J.; Yuan, X.; Shen, H.; Cunningham, J.; Rivers, H.M. Topical Drug Delivery to the Posterior Segment of the Eye: Addressing the Challenge of Preclinical to Clinical Translation. Pharm. Res. 2018, 35, 245. [Google Scholar] [CrossRef] [PubMed]
- Weng, Y.; Liu, J.; Jin, S.; Guo, W.; Liang, X.; Hu, Z. Nanotechnology-based strategies for treatment of ocular disease. Acta Pharm. Sin. B 2017, 7, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Mahale, N.B.; Thakkar, P.D.; Mali, R.G.; Walunj, D.R.; Chaudhari, S.R. Niosomes: Novel sustained release nonionic stable vesicular systems–an overview. Adv. Colloid Interface Sci. 2012, 183–184, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Bidram, E.; Esmaeili, Y.; Ranji-Burachaloo, H.; Al-Zaubai, N.; Zarrabi, A.; Stewart, A.; Dunstan, D.E. A concise review on cancer treatment methods and delivery systems. J. Drug Deliv. Sci. Technol. 2019, 54, 101350. [Google Scholar] [CrossRef]
- Uchegbu, I.F.; Vyas, S.P. Non-ionic surfactant based vesicles (niosomes) in drug delivery. J. Int. Pharm. 1998, 172, 33–70. [Google Scholar] [CrossRef]
- Moghassemi, S.; Hadjizadeh, A.; Omidfar, K. Formulation and Characterization of Bovine Serum Albumin-Loaded Niosome. AAPS PharmSciTech 2017, 18, 27–33. [Google Scholar] [CrossRef]
- Farmoudeh, A.; Akbari, J.; Saeedi, M.; Ghasemi, M.; Asemi, N.; Nokhodchi, A. Methylene blue-loaded niosome: Preparation, physicochemical characterization, and in vivo wound healing assessment. Drug Deliv. Transl. Res. 2020. [Google Scholar] [CrossRef]
- Gharbavi, M.; Amani, J.; Kheiri-Manjili, H.; Danafar, H.; Sharafi, A. Niosome: A Promising Nanocarrier for Natural Drug Delivery through Blood-Brain Barrier. Adv. Pharmacol. Sci. 2018, 2018, 6847971. [Google Scholar] [CrossRef]
- Uchegbu, I.F.; Florence, A.T. Non-ionic surfactant vesicles (niosomes): Physical and pharmaceutical chemistry. Adv. Colloid Interface Sci. 1995, 58, 1–55. [Google Scholar] [CrossRef]
- Amoabediny, G.; Haghiralsadat, F.; Naderinezhad, S.; Helder, M.N.; Akhoundi Kharanaghi, E.; Mohammadnejad Arough, J.; Zandieh-Doulabi, B. Overview of preparation methods of polymeric and lipid-based (niosome, solid lipid, liposome) nanoparticles: A comprehensive review. Int. J. Polym. Mater. Polym. Biomater. 2017, 67, 383–400. [Google Scholar] [CrossRef]
- Rinaldi, F.; del Favero, E.; Moeller, J.; Hanieh, N.P.; Passeri, D.; Rossi, M.; Angeloni, L.; Venditti, I.; Marianecci, C.; Carafa, M.; et al. Hydrophilic Silver Nanoparticles Loaded into Niosomes: Physical–Chemical Characterization in View of Biological Applications. Nanomaterials 2019, 9, 1177. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, H.; Ismail, S.; Kamal, A.; Alany, R.G. Preparation of niosomes as an ocular delivery system for naltrexone hydrochloride: Physicochemical characterization. Pharmazie 2010, 65, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Ge, X.; Wei, M.; He, S.; Yuan, W.E. Advances of Non-Ionic Surfactant Vesicles (Niosomes) and Their Application in Drug Delivery. Pharmaceutics 2019, 11, 55. [Google Scholar] [CrossRef]
- Bangham, A.D.; Standish, M.M.; Watkins, J.C. Diffusion of univalent ions across the lamellae of swollen phospholipids. J. Mol. Biol. 1965, 13, 238–252. [Google Scholar] [CrossRef]
- Balakrishnan, P.; Shanmugam, S.; Lee, W.S.; Lee, W.M.; Kim, J.O.; Oh, D.H.; Kim, D.D.; Kim, J.S.; Yoo, B.K.; Choi, H.G.; et al. Formulation and in vitro assessment of minoxidil niosomes for enhanced skin delivery. Int. J. Pharm. 2009, 377, 1–8. [Google Scholar] [CrossRef]
- Mishra, J.; Swain, J.; Mishra, A.K. Probing the temperature-dependent changes of the interfacial hydration and viscosity of Tween20: Cholesterol (1:1) niosome membrane using fisetin as a fluorescent molecular probe. Phys. Chem. Chem. Phys. 2018, 20, 13279–13289. [Google Scholar] [CrossRef]
- Ramadan, A.A.; Eladawy, S.A.; El-Enin, A.S.M.A.; Hussein, Z.M. Development and investigation of timolol maleate niosomal formulations for the treatment of glaucoma. J. Pharm. Investig. 2020, 50, 59–70. [Google Scholar] [CrossRef]
- Baillie, A.; Coombs, G.; Dolan, T.; Laurie, J. Non-ionic surfactant vesicles, niosomes, as a delivery system for the anti-leishmanial drug, sodium stibogluconate. J. Pharm. Pharmacol. 1986, 38, 502–505. [Google Scholar] [CrossRef]
- Pando, D.; Matos, M.; Gutiérrez, G.; Pazos, C. Formulation of resveratrol entrapped niosomes for topical use. Colloids Surf. B Biointerfaces 2015, 128, 398–404. [Google Scholar] [CrossRef]
- Jain, C.P.; Vyas, S.P. Preparation and characterization of niosomes containing rifampicin for lung targeting. J. Microencapsul. 1995, 12, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Sharma, Y.; Kumar, K.; Padhy, S.K. Formulation and evaluation of Atorvastatin calcium Niosomes. Int. J. Life Sci. Sci. Res. 2016, 2, 1–4. [Google Scholar] [CrossRef]
- Kakkar, S.; Kaur, I.P. Spanlastics–a novel nanovesicular carrier system for ocular delivery. Int. J. Pharm. 2011, 413, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Szoka, F., Jr.; Papahadjopoulos, D. Procedure for preparation of liposomes with large internal aqueous space and high capture by reverse-phase evaporation. Proc. Natl. Acad. Sci. USA 1978, 75, 4194–4198. [Google Scholar] [CrossRef]
- Jain, S.; Singh, P.; Mishra, V.; Vyas, S. Mannosylated niosomes as adjuvant–carrier system for oral genetic immunization against Hepatitis B. Immunol. Lett. 2005, 101, 41–49. [Google Scholar] [CrossRef]
- Guinedi, A.S.; Mortada, N.D.; Mansour, S.; Hathout, R.M. Preparation and evaluation of reverse-phase evaporation and multilamellar niosomes as ophthalmic carriers of acetazolamide. Int. J. Pharm. 2005, 306, 71–82. [Google Scholar] [CrossRef]
- Bendas, E.R.; Abdullah, H.; El-Komy, M.H.; Kassem, M.A. Hydroxychloroquine niosomes: A new trend in topical management of oral lichen planus. Int. J. Pharm. 2013, 458, 287–295. [Google Scholar] [CrossRef]
- Villate-Beitia, I.; Gallego, I.; Martinez-Navarrete, G.; Zarate, J.; Lopez-Mendez, T.; Soto-Sanchez, C.; Santos-Vizcaino, E.; Puras, G.; Fernandez, E.; Pedraz, J.L. Polysorbate 20 non-ionic surfactant enhances retinal gene delivery efficiency of cationic niosomes after intravitreal and subretinal administration. Int. J. Pharm. 2018, 550, 388–397. [Google Scholar] [CrossRef]
- Moghassemi, S.; Hadjizadeh, A. Nano-niosomes as nanoscale drug delivery systems: An illustrated review. J. Control. Release 2014, 185, 22–36. [Google Scholar] [CrossRef]
- More, V.V.; Gilhotra, R.M.; Nitalikar, M.M.; Khule, P.K. Niosomal Drug Delivery-A Comprehensive Review. Asian J. Pharm. 2019, 12, S1159–S1164. [Google Scholar]
- Talsma, H.; van Steenbergen, M.J.; Borchert, J.C.; Crommelin, D.J. A novel technique for the one-step preparation of liposomes and nonionic surfactant vesicles without the use of organic solvents. Liposome formation in a continuous gas stream: The ‘bubble’ method. J. Pharm. Sci. 1994, 83, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, H.; Ismail, S.; Kamal, A.; Alany, R.G. Design and evaluation of controlled-release niosomes and discomes for naltrexone hydrochloride ocular delivery. J. Pharm. Sci. 2011, 100, 1833–1846. [Google Scholar] [CrossRef] [PubMed]
- Kirby, C.; Gregoriadis, G. dehydration–rehydration vesicles: A simple method for high yield drug entrapment in liposomes. Bio. Technol. 1984, 2, 979–984. [Google Scholar] [CrossRef]
- Kallinteri, P.; Fatouros, D.; Klepetsanis, P.; Antimisiaris, S.G. Arsenic trioxide liposomes: Encapsulation efficiency and in vitro stability. J. Liposome Res. 2004, 14, 27–38. [Google Scholar] [CrossRef]
- Khandare, J.; Madhavi, G.; Tamhankar, B. Niosomes-Novel Drug Delivery System. East. Pharm. 1994, 37, 61. [Google Scholar]
- Kazi, K.M.; Mandal, A.S.; Biswas, N.; Guha, A.; Chatterjee, S.; Behera, M.; Kuotsu, K. Niosome: A future of targeted drug delivery systems. J. Adv. Pharm. Technol. Res. 2010, 1, 374–380. [Google Scholar] [CrossRef]
- Ag Seleci, D.; Maurer, V.; Stahl, F.; Scheper, T.; Garnweitner, G. Rapid Microfluidic Preparation of Niosomes for Targeted Drug Delivery. Int. J. Mol. Sci. 2019, 20, 4696. [Google Scholar] [CrossRef]
- Manosroi, A.; Chutoprapat, R.; Abe, M.; Manosroi, J. Characteristics of niosomes prepared by supercritical carbon dioxide (scCO2) fluid. Int. J. Pharm. 2008, 352, 248–255. [Google Scholar] [CrossRef]
- Marianecci, C.; Di Marzio, L.; Rinaldi, F.; Celia, C.; Paolino, D.; Alhaique, F.; Esposito, S.; Carafa, M. Niosomes from 80 s to present: The state of the art. Adv. Colloid Interface Sci. 2014, 205, 187–206. [Google Scholar] [CrossRef]
- Mozafari, M.R. Method for the Preparation of Micro-and Nano-Sized Carrier Systems for the Encapsulation of Bioactive Substances. U.S. Patent 20100239521A1, 23 September 2010. [Google Scholar]
- Mortazavi, S.M.; Mohammadabadi, M.R.; Khosravi-Darani, K.; Mozafari, M.R. Preparation of liposomal gene therapy vectors by a scalable method without using volatile solvents or detergents. J. Biotechnol. 2007, 129, 604–613. [Google Scholar] [CrossRef]
- Hu, C.; Rhodes, D.G. Proniosomes: A novel drug carrier preparation. Int. J. Pharm. 1999, 185, 23–35. [Google Scholar] [CrossRef]
- Yasam, V.R.; Jakki, S.L.; Natarajan, J.; Kuppusamy, G. A review on novel vesicular drug delivery: Proniosomes. Drug Deliv. 2014, 21, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Li, Q.; Wan, T.; Liu, C.; Pan, W.; Wu, Z.; Zhang, G.; Pan, J.; Qin, M.; Lin, Y.; et al. Hyaluronic acid-coated niosomes facilitate tacrolimus ocular delivery: Mucoadhesion, precorneal retention, aqueous humor pharmacokinetics, and transcorneal permeability. Colloids Surf. B Biointerfaces 2016, 141, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Emad Eldeeb, A.; Salah, S.; Ghorab, M. Proniosomal gel-derived niosomes: An approach to sustain and improve the ocular delivery of brimonidine tartrate; formulation, in-vitro characterization, and in-vivo pharmacodynamic study. Drug Deliv. 2019, 26, 509–521. [Google Scholar] [CrossRef]
- Hashemi Dehaghi, M.; Haeri, A.; Keshvari, H.; Abbasian, Z.; Dadashzadeh, S. Dorzolamide Loaded Niosomal Vesicles: Comparison of Passive and Remote Loading Methods. Iran. J. Pharm. Res. 2017, 16, 413–422. [Google Scholar]
- Abu, H., II.; El-Dahan, M.S.; Yusif, R.M.; Abd-Elgawad, A.E.; Arima, H. Potential use of niosomal hydrogel as an ocular delivery system for atenolol. Biol. Pharm. Bull. 2014, 37, 541–551. [Google Scholar] [CrossRef]
- Prabhu, P.; Nitish, K.R.; Koland, M.; Harish, N.; Vijayanarayan, K.; Dhondge, G.; Charyulu, R. Preparation and Evaluation of Nano-vesicles of Brimonidine Tartrate as an Ocular Drug Delivery System. J. Young Pharm. 2010, 2, 356–361. [Google Scholar] [CrossRef]
- Kaur, I.P.; Aggarwal, D.; Singh, H.; Kakkar, S. Improved ocular absorption kinetics of timolol maleate loaded into a bioadhesive niosomal delivery system. Graefes Arch. Clin. Exp. Ophthalmol. 2010, 248, 1467–1472. [Google Scholar] [CrossRef]
- Kaur, I.P.; Mitra, A.K.; Aggarwal, D. Development of a vesicular system for effective ocular delivery of acetazolamide a comprehensive approach and successful venture. J. Drug Deliv. Sci. Technol. 2007, 17, 33–41. [Google Scholar] [CrossRef]
- Aggarwal, D.; Kaur, I.P. Improved pharmacodynamics of timolol maleate from a mucoadhesive niosomal ophthalmic drug delivery system. Int. J. Pharm. 2005, 290, 155–159. [Google Scholar] [CrossRef]
- Akhtar, N.; Kumar Singh, R.; Pathak, K. Exploring the potential of complex-vesicle based niosomal ocular system loaded with azithromycin: Development of in situ gel and ex vivo characterization. Pharm. Biomed. Res. 2017, 3, 22–33. [Google Scholar] [CrossRef][Green Version]
- Khalil, R.M.; Abdelbary, G.A.; Basha, M.; Awad, G.E.A.; El-Hashemy, H.A. Enhancement of lomefloxacin Hcl ocular efficacy via niosomal encapsulation: In vitro characterization and in vivo evaluation. J. Liposome Res. 2017, 27, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Yasin, M.N.; Hussain, S.; Malik, F.; Hameed, A.; Sultan, T.; Qureshi, F.; Riaz, H.; Perveen, G.; Wajid, A. Preparation and characterization of chloramphenicol niosomes and comparison with chloramphenicol eye drops (0.5% w/v) in experimental conjunctivitis in albino rabbits. Pak. J. Pharm. Sci. 2012, 25, 117–121. [Google Scholar] [PubMed]
- Verma, A.; Sharma, G.; Jain, A.; Tiwari, A.; Saraf, S.; Panda, P.K.; Katare, O.P.; Jain, S.K. Systematic optimization of cationic surface engineered mucoadhesive vesicles employing Design of Experiment (DoE): A preclinical investigation. Int. J. Biol. Macromol. 2019, 133, 1142–1155. [Google Scholar] [CrossRef]
- Elmotasem, H.; Awad, G.E.A. A stepwise optimization strategy to formulate in situ gelling formulations comprising fluconazole-hydroxypropyl-beta-cyclodextrin complex loaded niosomal vesicles and Eudragit nanoparticles for enhanced antifungal activity and prolonged ocular delivery. Asian J. Pharm. Sci. 2019, in press. [Google Scholar] [CrossRef]
- Paradkar, M.U.; Parmar, M. Formulation development and evaluation of Natamycin niosomal in-situ gel for ophthalmic drug delivery. J. Drug Deliv. Sci. Technol. 2017, 39, 113–122. [Google Scholar] [CrossRef]
- Shukr, M.H. Novel in situ gelling ocular inserts for voriconazole-loaded niosomes: Design, in vitro characterisation and in vivo evaluation of the ocular irritation and drug pharmacokinetics. J. Microencapsul. 2016, 33, 71–79. [Google Scholar] [CrossRef]
- Fetih, G. Fluconazole-loaded niosomal gels as a topical ocular drug delivery system for corneal fungal infections. J. Drug Deliv. Sci. Technol. 2016, 35, 8–15. [Google Scholar] [CrossRef]
- Abdelbary, A.A.; Abd-Elsalam, W.H.; Al-Mahallawi, A.M. Fabrication of novel ultradeformable bilosomes for enhanced ocular delivery of terconazole: In vitro characterization, ex vivo permeation and in vivo safety assessment. Int. J. Pharm. 2016, 513, 688–696. [Google Scholar] [CrossRef]
- Kaur, I.P.; Rana, C.; Singh, M.; Bhushan, S.; Singh, H.; Kakkar, S. Development and evaluation of novel surfactant-based elastic vesicular system for ocular delivery of fluconazole. J. Ocul. Pharmacol. Ther. 2012, 28, 484–496. [Google Scholar] [CrossRef]
- Mashal, M.; Attia, N.; Martinez-Navarrete, G.; Soto-Sanchez, C.; Fernandez, E.; Grijalvo, S.; Eritja, R.; Puras, G.; Pedraz, J.L. Gene delivery to the rat retina by non-viral vectors based on chloroquine-containing cationic niosomes. J. Control. Release 2019, 304, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Mashal, M.; Attia, N.; Puras, G.; Martinez-Navarrete, G.; Fernandez, E.; Pedraz, J.L. Retinal gene delivery enhancement by lycopene incorporation into cationic niosomes based on DOTMA and polysorbate 60. J. Control. Release 2017, 254, 55–64. [Google Scholar] [CrossRef]
- Puras, G.; Mashal, M.; Zarate, J.; Agirre, M.; Ojeda, E.; Grijalvo, S.; Eritja, R.; Diaz-Tahoces, A.; Martinez Navarrete, G.; Aviles-Trigueros, M.; et al. A novel cationic niosome formulation for gene delivery to the retina. J. Control. Release 2014, 174, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Y.; Yang, J.; Zhang, H.; Gan, L. Cationized hyaluronic acid coated spanlastics for cyclosporine A ocular delivery: Prolonged ocular retention, enhanced corneal permeation and improved tear production. Int. J. Pharm. 2019, 565, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Li, Z.; Zeng, W.; Ge, S.; Lu, H.; Wu, C.; Ge, L.; Liang, D.; Xu, Y. Proniosome-derived niosomes for tacrolimus topical ocular delivery: In vitro cornea permeation, ocular irritation, and in vivo anti-allograft rejection. Eur. J. Pharm. Sci. 2014, 62, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Allam, A.; El-Mokhtar, M.A.; Elsabahy, M. Vancomycin-loaded niosomes integrated within pH-sensitive in-situ forming gel for treatment of ocular infections while minimizing drug irritation. J. Pharm. Pharmacol. 2019, 71, 1209–1221. [Google Scholar] [CrossRef] [PubMed]
- Abdelbary, A.; Salem, H.F.; Khallaf, R.A.; Ali, A.M. Mucoadhesive niosomal in situ gel for ocular tissue targeting: In vitro and in vivo evaluation of lomefloxacin hydrochloride. Pharm. Dev. Technol. 2017, 22, 409–417. [Google Scholar] [CrossRef]
- Zubairu, Y.; Negi, L.M.; Iqbal, Z.; Talegaonkar, S. Design and development of novel bioadhesive niosomal formulation for the transcorneal delivery of anti-infective agent: In-vitro and ex-vivo investigations. Asian J. Pharm. Sci. 2015, 10, 322–330. [Google Scholar] [CrossRef]
- Abdelbary, G.; El-Gendy, N. Niosome-encapsulated gentamicin for ophthalmic controlled delivery. AAPS PharmSciTech 2008, 9, 740–747. [Google Scholar] [CrossRef]
- Gugleva, V.; Titeva, S.; Rangelov, S.; Momekova, D. Design and in vitro evaluation of doxycycline hyclate niosomes as a potential ocular delivery system. Int. J. Pharm. 2019, 567, 118431. [Google Scholar] [CrossRef]
- El-Sayed, M.M.; Hussein, A.K.; Sarhan, H.A.; Mansour, H.F. Flurbiprofen-loaded niosomes-in-gel system improves the ocular bioavailability of flurbiprofen in the aqueous humor. Drug Dev. Ind. Pharm. 2017, 43, 902–910. [Google Scholar] [CrossRef] [PubMed]
- Gaafar, P.M.; Abdallah, O.Y.; Farid, R.M.; Abdelkader, H. Preparation, characterization and evaluation of novel elastic nano-sized niosomes (ethoniosomes) for ocular delivery of prednisolone. J. Liposome Res. 2014, 24, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, H.; Ismail, S.; Hussein, A.; Wu, Z.; Al-Kassas, R.; Alany, R.G. Conjunctival and corneal tolerability assessment of ocular naltrexone niosomes and their ingredients on the hen’s egg chorioallantoic membrane and excised bovine cornea models. Int. J. Pharm. 2012, 432, 1–10. [Google Scholar] [CrossRef]
- Fritze, A.; Hens, F.; Kimpfler, A.; Schubert, R.; Peschka-Suss, R. Remote loading of doxorubicin into liposomes driven by a transmembrane phosphate gradient. Biochim. Biophys. Acta 2006, 1758, 1633–1640. [Google Scholar] [CrossRef] [PubMed]
- Lewrick, F.; Suss, R. Remote loading of anthracyclines into liposomes. Methods Mol. Biol. 2010, 605, 139–145. [Google Scholar] [CrossRef]
- Rajera, R.; Nagpal, K.; Singh, S.K.; Mishra, D.N. Niosomes: A controlled and novel drug delivery system. Biol. Pharm. Bull. 2011, 34, 945–953. [Google Scholar] [CrossRef]
- Lakshmi, P.K.; Bhaskaran, S. Phase II study of topical niosomal urea gel-an adjuvant in the treatment of psoriasis. Int. J. Pharm. Sci. Rev. Res. 2011, 7, 1–7. [Google Scholar]
- Uchegbu, I.F.; Double, J.A.; Kelland, L.R.; Turton, J.A.; Florence, A.T. The activity of doxorubicin niosomes against an ovarian cancer cell line and three in vivo mouse tumour models. J. Drug Target. 1996, 3, 399–409. [Google Scholar] [CrossRef]
- Akbari, V.; Abedi, D.; Pardakhty, A.; Sadeghi-Aliabadi, H. Ciprofloxacin nano-niosomes for targeting intracellular infections: An in vitro evaluation. J. Nanopart. Res. 2013, 15, 1556. [Google Scholar] [CrossRef]
- Sahoo, R.K.; Biswas, N.; Guha, A.; Sahoo, N.; Kuotsu, K. Nonionic surfactant vesicles in ocular delivery: Innovative approaches and perspectives. Biomed. Res. Int. 2014, 2014, 263604. [Google Scholar] [CrossRef]
- Fitzgerald, P.; Hadgraft, J.; Kreuter, J.; Wilson, C.G. A γ-scintigraphic evaluation of microparticulate ophthalmic delivery systems: Liposomes and nanoparticles. Int. J. Pharm. 1987, 40, 81–84. [Google Scholar] [CrossRef]
- Fitzgerald, P.; Hadgraft, J.; Wilson, C.G. A gamma scintigraphic evaluation of the precorneal residence of liposomal formulations in the rabbit. J. Pharm. Pharmacol. 1987, 39, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Barza, M.; Stuart, M.; Szoka, F., Jr. Effect of size and lipid composition on the pharmacokinetics of intravitreal liposomes. Invest. Ophthalmol. Vis. Sci. 1987, 28, 893–900. [Google Scholar] [PubMed]
- Manosroi, A.; Wongtrakul, P.; Manosroi, J.; Sakai, H.; Sugawara, F.; Yuasa, M.; Abe, M. Characterization of vesicles prepared with various non-ionic surfactants mixed with cholesterol. Colloids Surf. B Biointerfaces 2003, 30, 129–138. [Google Scholar] [CrossRef]
- Danaei, M.; Dehghankhold, M.; Ataei, S.; Hasanzadeh Davarani, F.; Javanmard, R.; Dokhani, A.; Khorasani, S.; Mozafari, M.R. Impact of Particle Size and Polydispersity Index on the Clinical Applications of Lipidic Nanocarrier Systems. Pharmaceutics 2018, 10, 57. [Google Scholar] [CrossRef] [PubMed]
- Gratton, S.E.; Ropp, P.A.; Pohlhaus, P.D.; Luft, J.C.; Madden, V.J.; Napier, M.E.; DeSimone, J.M. The effect of particle design on cellular internalization pathways. Proc. Natl. Acad. Sci. USA 2008, 105, 11613–11618. [Google Scholar] [CrossRef]
- Aggarwal, D.; Garg, A.; Kaur, I.P. Development of a topical niosomal preparation of acetazolamide: Preparation and evaluation. J. Pharm. Pharmacol. 2004, 56, 1509–1517. [Google Scholar] [CrossRef]
- Arzani, G.; Haeri, A.; Daeihamed, M.; Bakhtiari-Kaboutaraki, H.; Dadashzadeh, S. Niosomal carriers enhance oral bioavailability of carvedilol: Effects of bile salt-enriched vesicles and carrier surface charge. Int. J. Nanomed. 2015, 10, 4797–4813. [Google Scholar] [CrossRef]
- Ojeda, E.; Puras, G.; Agirre, M.; Zarate, J.; Grijalvo, S.; Eritja, R.; Martinez-Navarrete, G.; Soto-Sanchez, C.; Diaz-Tahoces, A.; Aviles-Trigueros, M.; et al. The influence of the polar head-group of synthetic cationic lipids on the transfection efficiency mediated by niosomes in rat retina and brain. Biomaterials 2016, 77, 267–279. [Google Scholar] [CrossRef]
- Hao, Y.; Zhao, F.; Li, N.; Yang, Y.; Li, K. Studies on a high encapsulation of colchicine by a niosome system. Int. J. Pharm. 2002, 244, 73–80. [Google Scholar] [CrossRef]
- Ojeda, E.; Puras, G.; Agirre, M.; Zarate, J.; Grijalvo, S.; Pons, R.; Eritja, R.; Martinez-Navarrete, G.; Soto-Sanchez, C.; Fernandez, E.; et al. Niosomes based on synthetic cationic lipids for gene delivery: The influence of polar head-groups on the transfection efficiency in HEK-293, ARPE-19 and MSC-D1 cells. Org. Biomol. Chem. 2015, 13, 1068–1081. [Google Scholar] [CrossRef] [PubMed]
- Jafariazar, Z.; Jamalinia, N.; Ghorbani-Bidkorbeh, F.; Mortazavi, S.A. Design and Evaluation of Ocular Controlled Delivery System for Diclofenac Sodium. Iran. J. Pharm. Res. 2015, 14, 23–31. [Google Scholar] [PubMed]
- Kamboj, S.; Saini, V.; Bala, S. Formulation and characterization of drug loaded nonionic surfactant vesicles (niosomes) for oral bioavailability enhancement. Sci. World J. 2014, 2014, 959741. [Google Scholar] [CrossRef] [PubMed]
- Subrizi, A.; Del Amo, E.M.; Korzhikov-Vlakh, V.; Tennikova, T.; Ruponen, M.; Urtti, A. Design principles of ocular drug delivery systems: Importance of drug payload, release rate, and material properties. Drug Discov. Today 2019, 24, 1446–1457. [Google Scholar] [CrossRef]
- Higuchi, T. Mechanism of Sustained-Action Medication. Theoretical Analysis of Rate of Release of Solid Drugs Dispersed in Solid Matrices. J. Pharm. Sci. 1963, 52, 1145–1149. [Google Scholar] [CrossRef]
- Attia, I.A.; El-Gizawy, S.A.; Fouda, M.A.; Donia, A.M. Influence of a niosomal formulation on the oral bioavailability of acyclovir in rabbits. AAPS PharmSciTech 2007, 8, E106. [Google Scholar] [CrossRef]
- Dorati, R.; DeTrizio, A.; Spalla, M.; Migliavacca, R.; Pagani, L.; Pisani, S.; Chiesa, E.; Conti, B.; Modena, T.; Genta, I. Gentamicin Sulfate PEG-PLGA/PLGA-H Nanoparticles: Screening Design and Antimicrobial Effect Evaluation toward Clinic Bacterial Isolates. Nanomaterials 2018, 8, 37. [Google Scholar] [CrossRef]
- Muller, R.H.; Radtke, M.; Wissing, S.A. Solid lipid nanoparticles (SLN) and nanostructured lipid carriers (NLC) in cosmetic and dermatological preparations. Adv. Drug Deliv. Rev. 2002, 54, S131–S155. [Google Scholar] [CrossRef]
- Geyer, O.; Levo, Y. Glaucoma is an autoimmune disease. Autoimmun. Rev. 2020, 19, 102535. [Google Scholar] [CrossRef]
- Cetinel, S.; Montemagno, C. Nanotechnology Applications for Glaucoma. Asia Pac. J. Ophthalmol. Phila 2016, 5, 70–78. [Google Scholar] [CrossRef]
- Gupta, N.; Yucel, Y.H. Glaucoma as a neurodegenerative disease. Curr. Opin. Ophthalmol. 2007, 18, 110–114. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, S.J. Glaucoma: Ocular Alzheimer’s disease? Front. Biosci. 2003, 8, s1140–s1156. [Google Scholar] [CrossRef] [PubMed]
- Faiq, M.A.; Wollstein, G.; Schuman, J.S.; Chan, K.C. Cholinergic nervous system and glaucoma: From basic science to clinical applications. Prog. Retin. Eye Res. 2019, 72, 100767. [Google Scholar] [CrossRef] [PubMed]
- Ma, A.; Yu, S.W.Y.; Wong, J.K.W. Micropulse laser for the treatment of glaucoma: A literature review. Surv. Ophthalmol. 2019, 64, 486–497. [Google Scholar] [CrossRef]
- Azari, A.A.; Barney, N.P. Conjunctivitis: A systematic review of diagnosis and treatment. JAMA 2013, 310, 1721–1729. [Google Scholar] [CrossRef]
- Alfonso, S.A.; Fawley, J.D.; Alexa Lu, X. Conjunctivitis. Prim. Care 2015, 42, 325–345. [Google Scholar] [CrossRef]
- La Rosa, M.; Lionetti, E.; Reibaldi, M.; Russo, A.; Longo, A.; Leonardi, S.; Tomarchio, S.; Avitabile, T.; Reibaldi, A. Allergic conjunctivitis: A comprehensive review of the literature. Ital. J. Pediatr. 2013, 39, 18. [Google Scholar] [CrossRef]
- Skevaki, C.L.; Galani, I.E.; Pararas, M.V.; Giannopoulou, K.P.; Tsakris, A. Treatment of viral conjunctivitis with antiviral drugs. Drugs 2011, 71, 331–347. [Google Scholar] [CrossRef]
- Bourcier, T.; Sauer, A.; Dory, A.; Denis, J.; Sabou, M. Fungal keratitis. J. Fr. Ophtalmol. 2017, 40, e307–e313. [Google Scholar] [CrossRef]
- McClements, M.E.; MacLaren, R.E. Gene therapy for retinal disease. Transl. Res. 2013, 161, 241–254. [Google Scholar] [CrossRef]
- Austin, A.; Lietman, T.; Rose-Nussbaumer, J. Update on the Management of Infectious Keratitis. Ophthalmology 2017, 124, 1678–1689. [Google Scholar] [CrossRef] [PubMed]
- Dart, J.K.; Stapleton, F.; Minassian, D. Contact lenses and other risk factors in microbial keratitis. Lancet 1991, 338, 650–653. [Google Scholar] [CrossRef]
- Srinivasan, M. Fungal keratitis. Curr. Opin. Ophthalmol. 2004, 15, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Lakhundi, S.; Siddiqui, R.; Khan, N.A. Pathogenesis of microbial keratitis. Microb. Pathog. 2017, 104, 97–109. [Google Scholar] [CrossRef]
- Omerović, N.; Vranić, E. Application of nanoparticles in ocular drug delivery systems. Health Technol. 2019, 10, 61–78. [Google Scholar] [CrossRef]
- Biswas, G.R.; Majee, S.B. Niosomes in ocular drug delivery. Eur. J. Pharm. Med. Res. 2017, 4, 813–819. [Google Scholar]
- Maiti, S.; Paul, S.; Mondol, R.; Ray, S.; Sa, B. Nanovesicular formulation of brimonidine tartrate for the management of glaucoma: In vitro and in vivo evaluation. AAPS PharmSciTech 2011, 12, 755–763. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polysorbates (Tweens) | Sorbitans (Spans) * | ||
|---|---|---|---|
| Tween 20 CMC~0.06 mM |  | Span 20 |  |
| Tween 40 CMC~0.027 mM |  | Span 40 |  |
| Tween 60 CMC~0.026 mM |  | Span 60 |  |
| Tween 80 CMC~0.012 mM |  | Span 80 |  |
| Tween 65 CMC~0.00018 mM |  | Span 65 |  |
| Tween 85 CMC~0.00029 mM |  | Span 85 |  |
| Disease | Surfactant(s) | Additive(s) | Drug | Production Method(s) | Results | Year, Ref. |
|---|---|---|---|---|---|---|
| Glaucoma | Span 20, 40, 60 Tween 20, 40 | Cholesterol | Timolol maleate | TFH | Highest EE% found in niosomes prepared with span60 and Tween 40 (>90%), and niosomes prolonged drug release and IOP-lowering activity up to 24 h. | 2020, [28] |
| Span 60 Brij 52 | Cholesterol Soybean α-lecithin | Brimonidine tartrate | Proniosome | Highest EE% obtained be span60 formulations (>64%) as compared to brij52 niosomes. Niosomes extended drug release up to 24 h and showed higher IOP-lowering activity than marketed drug. | 2019, [55] | |
| Span 60 | Cholesterol | Dorzolamide HCl | TFH | EE% of remote loaded niosomes was higher (>31%) than passive loaded niosomes, and prolonged drug release more than 8 h was observed. | 2017, [56] | |
| Span 60 | Cholesterol | Atenolol | TFH | Maximum EE% between formulated niosomes was 80.7%. When inside the in situ gel, niosomes prolonged drug release and IOP-lowering activity more than 8 h. | 2014, [57] | |
| Span 60 | Cholesterol | Brimonidine tartrate | TFH | EE% of the niosomes were in >32, and niosomes showed IOP-lowering activity 3 h longer than commercial drug. | 2010, [58] | |
| Span 60 | Cholesterol Chitosan | Timolol maleate | REV | EE% of niosomes was 24.3%, and niosomes extended drug release more than 10 h and IOP-lowering activity up to 8 h with peak at 3 h. | 2009, [59] | |
| Span 60 | Cholesterol Carbopol | Acetazolamide | REV | EE% of prepared niosomes was 43.75%, and carbopol coated niosomes showed more sustained and higher IOP-lowering activity than marketed drug. | 2007, [60] | |
| Span 40, 60 | Cholesterol | Acetazolamide | TFH, REV | Span60:chol (7:6) MLV niosomes are the highest entrapment efficiency (>32%), and these niosomes prolonged IOP-lowering activity compared to Span60:Chol (7:4) MLV niosomes. | 2005, [36] | |
| Span 60 | Cholesterol Chitosan Carbopol | Timolol maleate | REV | Chitosan coated niosomes formulation showed prolonged decrease in IOP compared to carbopol coated niosomes | 2005, [61] | |
| Conjunctivitis | Span 60 | Cholesterol | Azithromycin-β-CD | SI, TFH, Hand shaking | EE% of prepared niosomes (>30%) and niosomal in situ gel formulations (>63%) were high, and niosomes prolonged drug release up to 12 h with increased corneal permeation. | 2017, [62] |
| Span 20, 60, 80 Tween 40, 60, 80 | Cholesterol | Lomefloxacin HCI | TFH | EE% of the tween niosomes (>41%) and drug release rate were higher than spans niosomes (>40%), and niosomal formulation healed the infected eyes better than marketed drug. | 2017, [63] | |
| Span 60 | Cholesterol | Chloramphenicol | SI | EE% of niosomal formulations were >83%, and niosomes prolonged drug release up to 10 h. Niosomes cured disease with less administration than marketed eye drop. | 2012, [64] | |
| Fungal keratitis | Span 60 | Cholesterol Dicetyl phospate N-Trimethyl chitosan | Natamycin | TFH | Both uncoated and TMC coated niosomes extended drug release up to 12 h., and TMC coated niosomes are higher mucoadhesion and corneal permeability than uncoated niosomes. | 2019, [65] |
| Span 60 | Cholesterol Chitosan | Fluconazole-hydroxypropyl-β-CD | TFH | EE% of the chitosan-coated niosomes were 61.7%, and chitosan coated niosomes prolonged drug release up to 24 h. | 2019, [66] | |
| Span 60 | Cholesterol | Natamycin | TFH | EE% of niosome formulations were high (>65%), and niosomes extended drug release up to 24 h with increased corneal permeation. | 2017, [67] | |
| Span 40, 60 | Cholesterol Pluronic L64 Pluronic F127 | Voriconazole | TFH | EE% of the prepared formulations was >49%, also niosomes and niosomal in situ gel formulations prolonged drug release up to 8 h. | 2016, [68] | |
| Span 60, 80 | Cholesterol | Fluconazole | TFH | Span60:chol (2:1) niosomes had the highest EE% (>84%) and better release kinetics. Niosome incorporated into poloxamer gel showed better antifungal activity than niosomes incorporated into chitosan gel. | 2016, [69] | |
| Span 60 | Cholesterol Bile salts Edge activator | Tercanazole | SI | Increased edge activator concentration was decreased EE% of niosomes, and selected formulation had EE% of 95.47%. Niosomes increased corneal permeation of drug. | 2016, [70] | |
| Span 40, 60, 80 | Edge activators Cholesterol | Fluconazole | SI | In the prepared formulations highest EE% was 65.73%, and corneal permeation of niosomes were higher than marketed drug. | 2012, [71] | |
| Genetic retinal disorders | Tween 80 Poloxamer 188 | Chloroquine (CQ) Cationic lipid 2,3-di(tetra decyloxy)propan-1-amine | pCMS-EGFP plasmid | REV | Transfection efficiency of pristine nioplexes was higher than CQ-nioplexes but efficiency of both nioplexes were lower compared to Lipofectamine 2000, and CQ-nioplexes transfected cells in inner layers of retina. | 2019, [72] |
| Tween 20, 80, 85 | Cationic lipid DOTMA Squalene | pCMS-EGFP reporter plasmid | REV | Cell viability was higher for nioplexes transfected cells, but transfection efficiency was lower compared to Lipofectamine 2000, and Tween 20 nioplexes was the highest transfection efficiency (>24.5%) for ARPE-19 cells | 2018, [38] | |
| Tween 60 | Lycopene Cationic lipid DOTMA | pCMS-EGFP plasmid | REV | Lycopene was increased transfection efficiency of nioplexes, but the efficiency was lower than lipofectamine 2000. Nioplexes were transfected cells in inner layers of retina. | 2017, [73] | |
| Tween 80 | Cationic lipid 2,3-di(tetradecyloxy)propan-1-amine Squalene | pCMS-EGFP plasmid | REV | Cell viability was higher for nioplexes compared to Lipofectamine 2000. in vivo transfection was depending administration route; subretinal injection transfected RPE layer cells but intravitreal injection transfected cells in inner layers of retina. | 2014, [74] | |
| Corneal graft rejection | Span 60 Tween 80 | Hyaluronic acid | Cyclosporine A | SI | HA-coated elastic niosomes had EE% of >92%, and HA-coated formulations were higher corneal permeability than drug emulsion and Span60 niosomes. | 2019, [75] |
| Poloxamer 188 Soybean phophadithylcoline | Cholesterol Hyaluronic acid | Tacrolimus (FK506) | Proniosome | HA improved the mucoadhesion niosomes, prolonged the residency of drug, and decreased clearance rate of drug in aqueous humor. | 2016, [54] | |
| Poloxamer 188 Lecithin | Cholesterol | Tacrolimus (FK506) | Proniosome | Drug loaded with EE% of 95.32%, and niosomes enhanced the precorneal permeation with prolonged corneal graft survival | 2014, [76] | |
| Ocular infections | Span 60 Tween 40 | Cholesterol | Vancomycin | TFH | EE% of niosomes was >46%, and niosomes prolonged drug release more than 24 h with increased antibacterial activity. | 2019, [77] |
| Span 20, 60, 80 | Cholesterol | Lomefloxacin HCI | TFH | Drug EE% of niosomes were >78.1%, and niosomes prolonged drug release up to 8 h with higher antimicrobial activity than free drug. | 2017, [78] | |
| Span 60 | Cholesterol Chitosan | Gatifloxacin | SI | EE% of chitosan coated niosomes was >68.9%, and chitosan coating was further improved corneal permeability of niosomes | 2015, [79] | |
| Tween 60, 80 Brij 35 | Cholesterol Dicetyl phospate | Gentamicin sulfate | TFH | Drug EE% of prepared niosomes was changed in wide range, but all of the niosomes prolonged drug release up to 8 h. | 2008, [80] | |
| Ocular surface diseases | Span 20, 60, 80 Tween 60 | Cholesterol | Doxycycline hyclate | TFH with extrusion, REV | Span60 niosomes had the highest EE% (>50%), and niosomes extended release of drug more than 20 h. | 2019, [81] |
| Ocular inflammation | Span 60 | Cholesterol | Flurbiprofen | TFH | Niosomal in situ gel formulation extended drug release more than 7 h and maintained drug concentration in the aqueous humor up to 12 h. | 2016, [82] |
| Span 60 | Cholesterol Ethanol | Prednisolone | TFH, SI | EE% of niosomes prepared by TFH was higher than SI, and niosomes extended drug release up to 8 h. Also, niosomes decreased the inflammation more than drug solution. | 2014, [83] | |
| Diabetic keratopathy | Span 60 Solulan C24 Sodium cholate | Cholesterol Dicetyl phospate | Naltrexone | REV | All of the niosomal formulations showed no irritation and have good corneal tolerability. | 2012, [84] |
| Span 60 Solulan C24 Sodium cholate | DCP Stearyl amine Cholesterol | Naltrexone | TFH, REV, DRV, Freeze/thaw | EE% of niosomes prepared from different methods compared, and Rev. niosomes showed highest EE%, and niosomes prolonged drug release up to 12 h. | 2011, [42] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durak, S.; Esmaeili Rad, M.; Alp Yetisgin, A.; Eda Sutova, H.; Kutlu, O.; Cetinel, S.; Zarrabi, A. Niosomal Drug Delivery Systems for Ocular Disease—Recent Advances and Future Prospects. Nanomaterials 2020, 10, 1191. https://doi.org/10.3390/nano10061191
Durak S, Esmaeili Rad M, Alp Yetisgin A, Eda Sutova H, Kutlu O, Cetinel S, Zarrabi A. Niosomal Drug Delivery Systems for Ocular Disease—Recent Advances and Future Prospects. Nanomaterials. 2020; 10(6):1191. https://doi.org/10.3390/nano10061191
Chicago/Turabian StyleDurak, Saliha, Monireh Esmaeili Rad, Abuzer Alp Yetisgin, Hande Eda Sutova, Ozlem Kutlu, Sibel Cetinel, and Ali Zarrabi. 2020. "Niosomal Drug Delivery Systems for Ocular Disease—Recent Advances and Future Prospects" Nanomaterials 10, no. 6: 1191. https://doi.org/10.3390/nano10061191
APA StyleDurak, S., Esmaeili Rad, M., Alp Yetisgin, A., Eda Sutova, H., Kutlu, O., Cetinel, S., & Zarrabi, A. (2020). Niosomal Drug Delivery Systems for Ocular Disease—Recent Advances and Future Prospects. Nanomaterials, 10(6), 1191. https://doi.org/10.3390/nano10061191