
The Impact of Different Fiber Placement Techniques on the Fracture Resistance of Premolars Restored with Direct Resin Composite, In Vitro Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
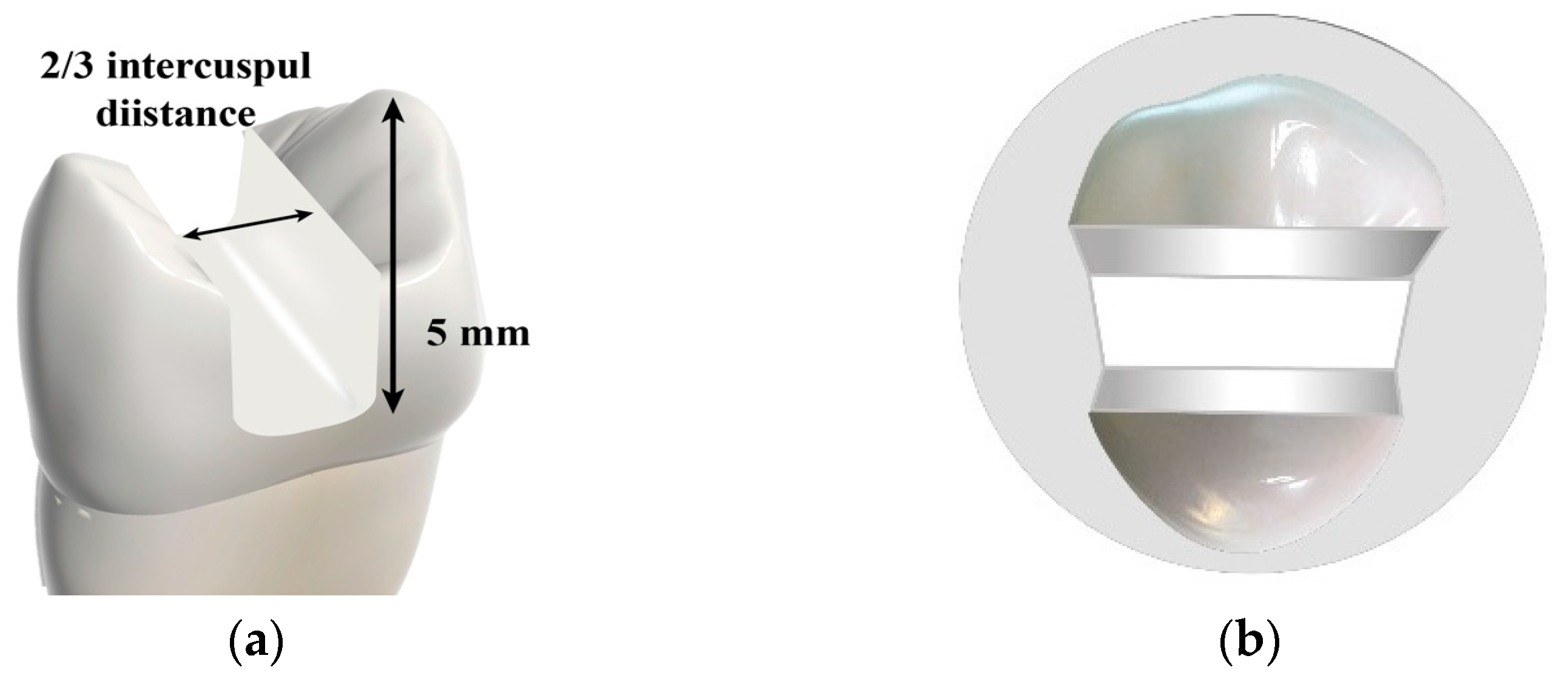
2.1. Cavity Preparation
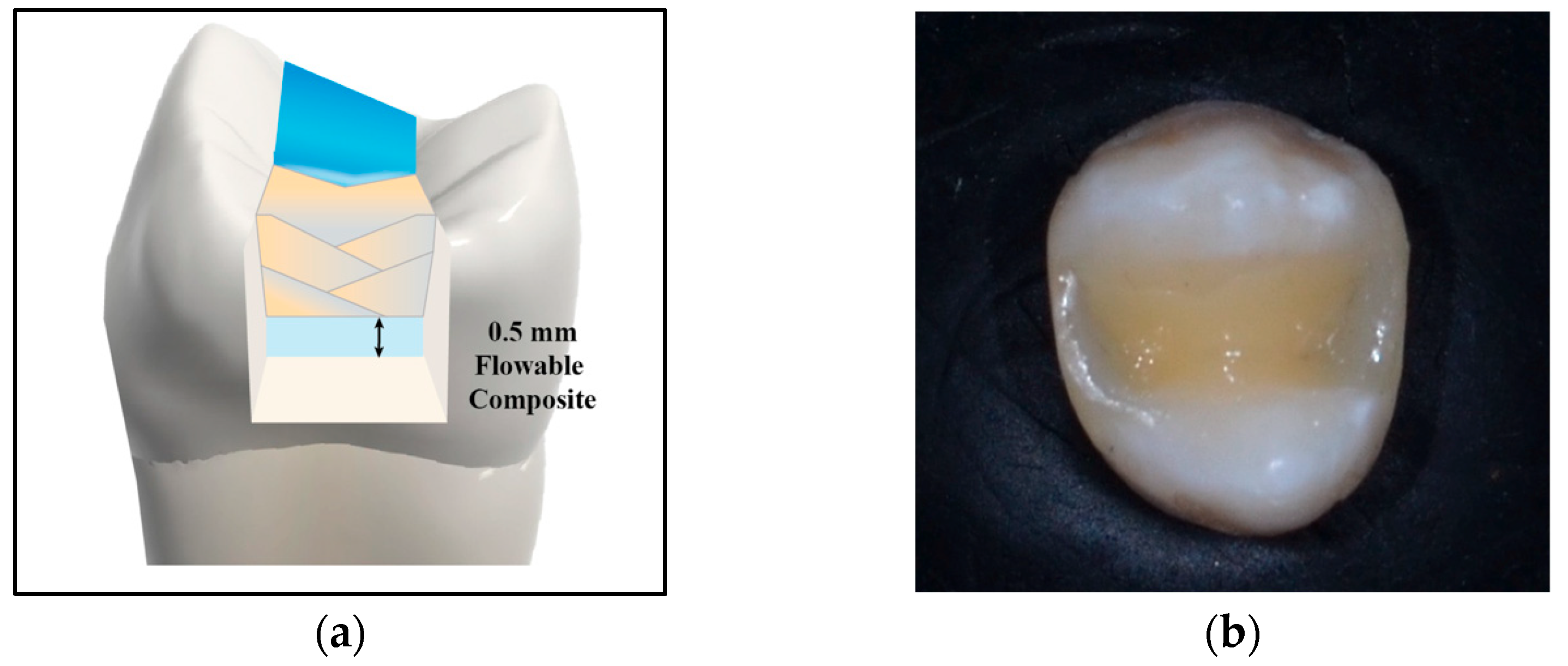
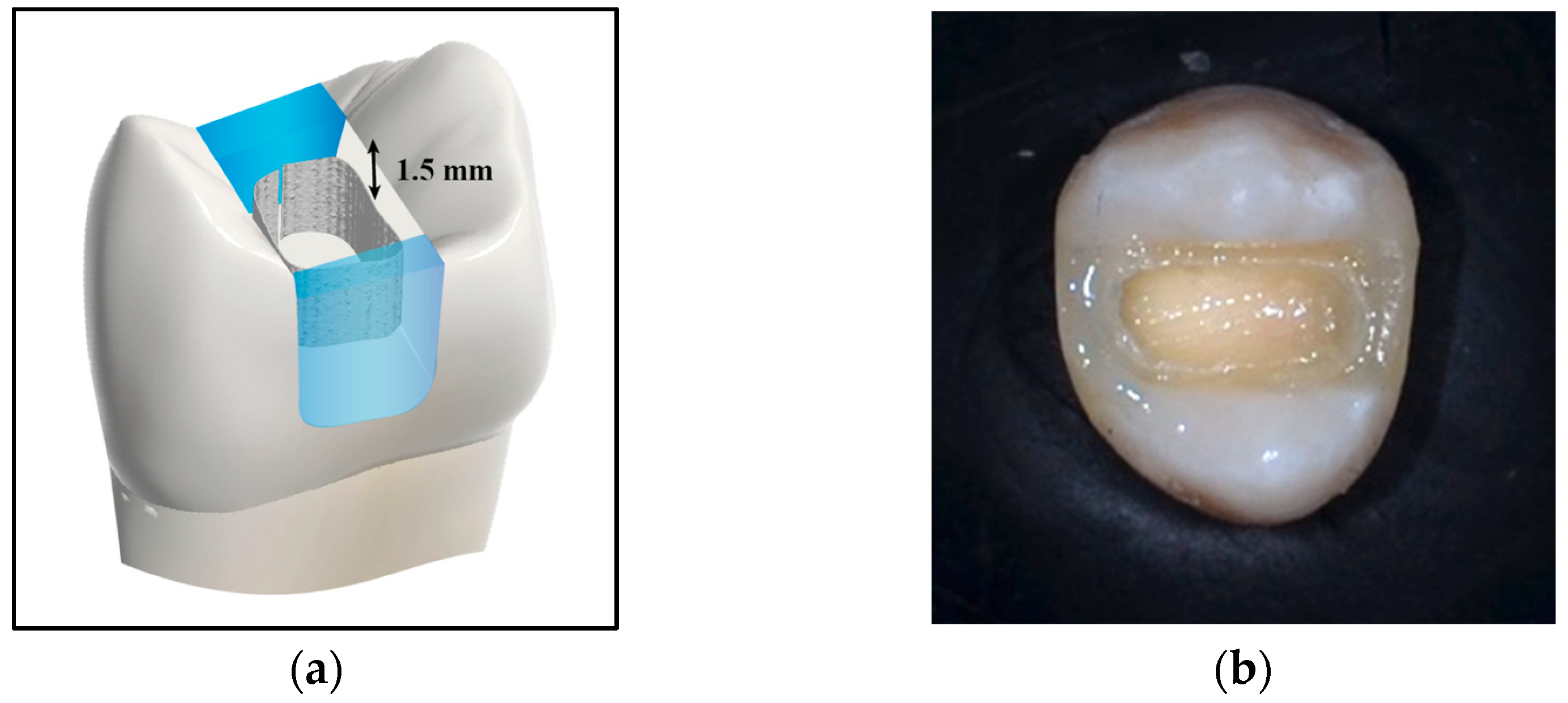
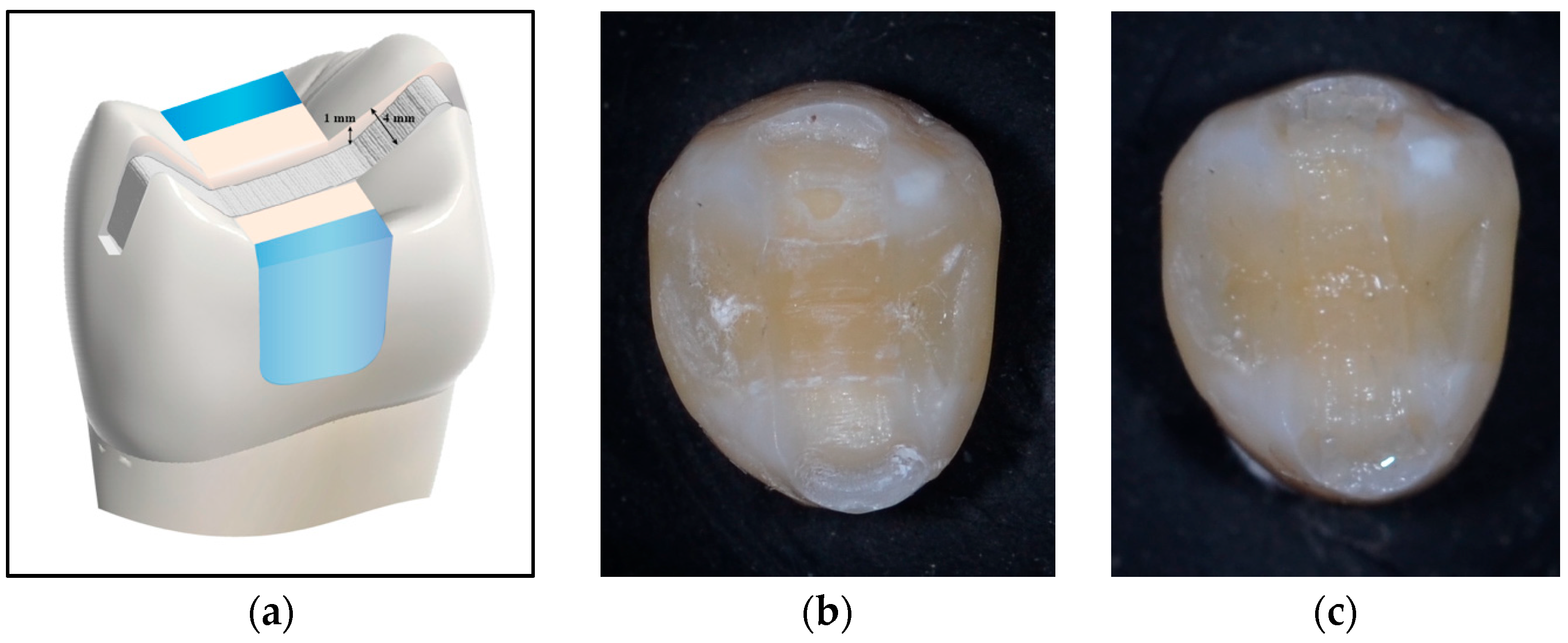
2.2. Restorative Procedures
2.3. Thermocycling Procedure
2.4. Embedding of Teeth
2.5. Fracture Resistance Test
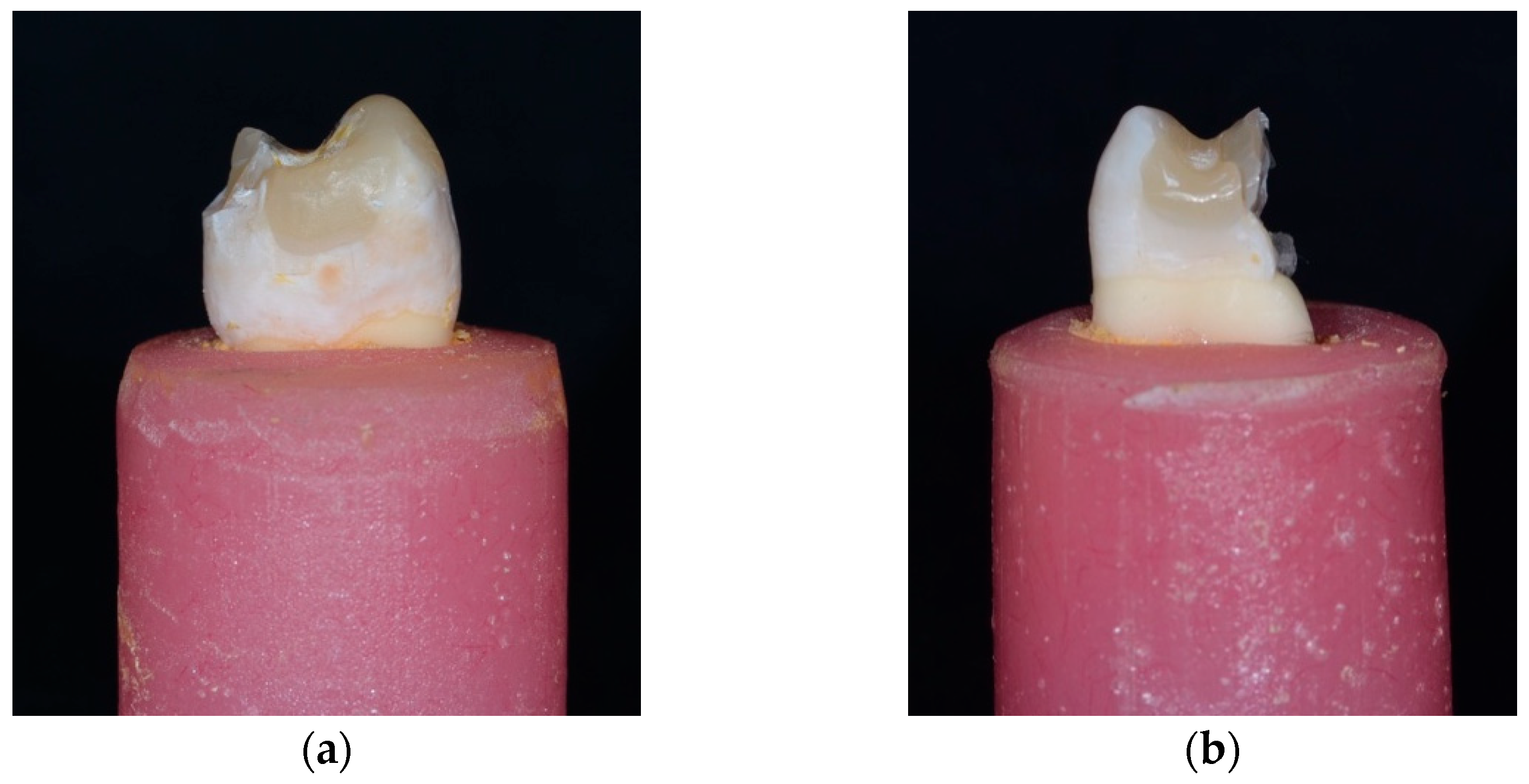
2.6. Failure Mode Analysis
2.7. Statistical Analysis
3. Results
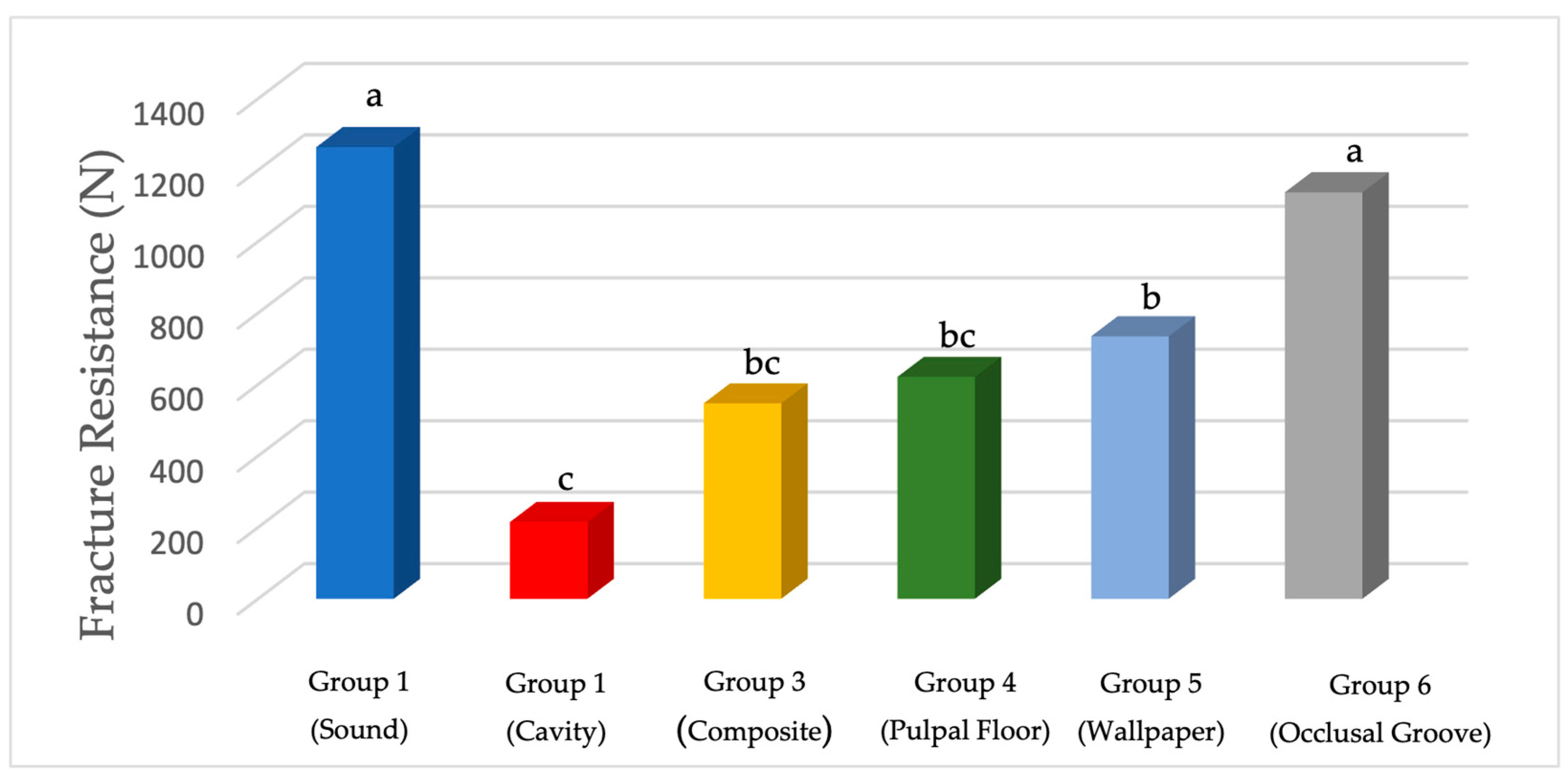
3.1. Fracture Resistance (N)
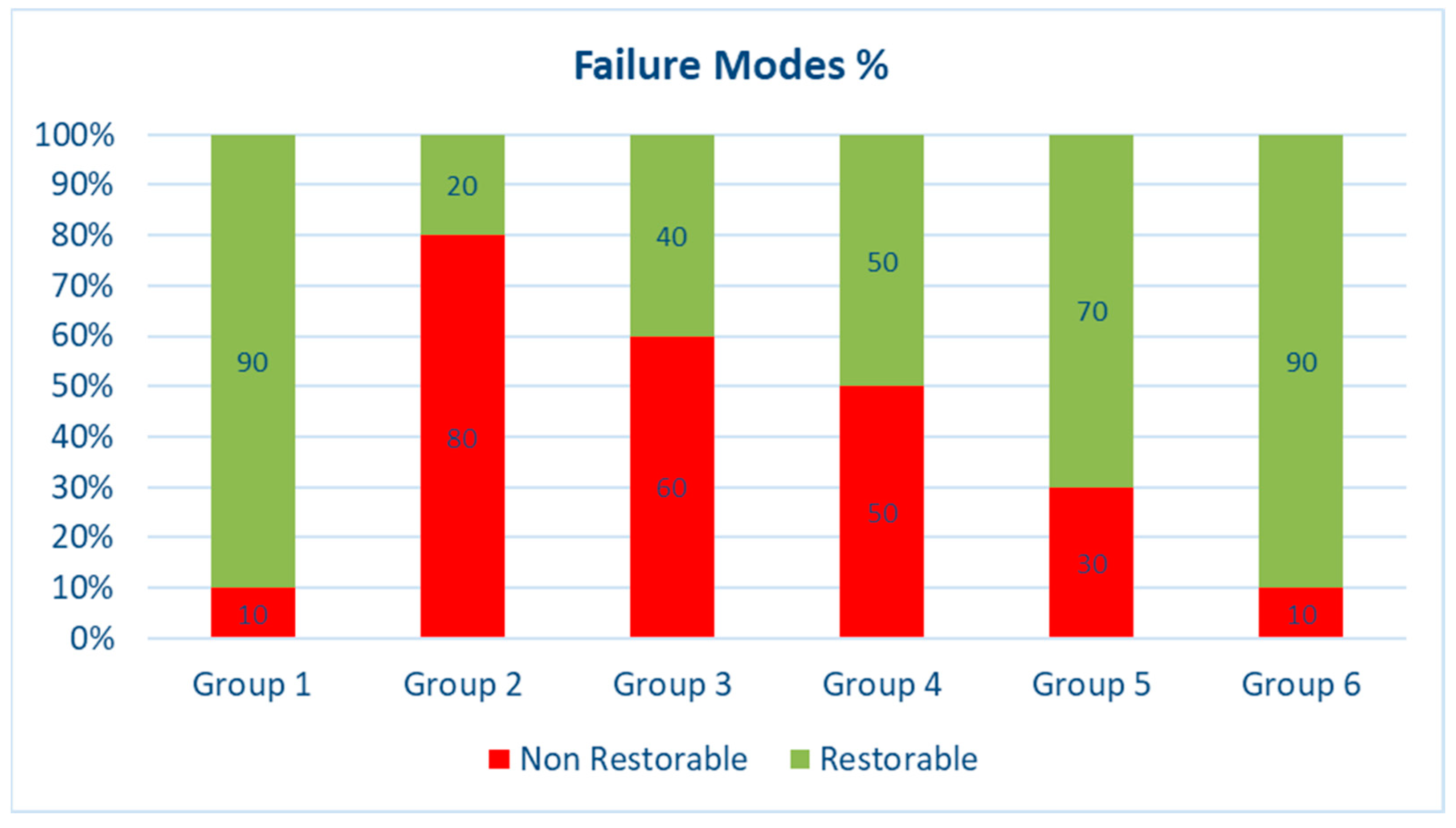
3.2. Failure Mode Results
4. Discussion
5. Conclusions
- Strategic placement of long polyethylene fibers—particularly in an occlusal splinting configuration—can significantly enhance the fracture resistance of restored teeth, achieving performance levels comparable to those of sound teeth.
- Placing fibers on the pulpal floor or in a circumferential orientation does not improve fracture resistance relative to conventional composite layering without reinforcement.
- Both occlusal splinting and circumferential placement of fibers were associated with more restorable fracture patterns, highlighting the potential of these fiber reinforcement techniques to improve the clinical manageability of structurally compromised teeth.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CEJ | Cemento-enamel junction |
| ETT | Endodontically treated teeth |
| FRC | Fiber-reinforced composite |
| LWUHMW | Leno woven ultra-high molecular weight |
| MOD | Mesio-occluso-distal |
| SFRC | Short-fiber-reinforced composite |
References
- Sfeikos, T.; Dionysopoulos, D.; Kouros, P.; Naka, O.; Tolidis, K. Effect of a fiber-reinforcing technique for direct composite restorations of structurally compromised teeth on marginal microleakage. J. Esthet. Restor. Dent. 2022, 34, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Albar, N.H.M.; Khayat, W.F. Evaluation of Fracture Strength of Fiber-Reinforced Direct Composite Resin Restorations: An In Vitro Study. Polymers 2022, 14, 4339. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Hilton, T.J.; Heintze, S.D.; Hickel, R.; Watts, D.C.; Silikas, N.; Stansbury, J.W.; Cadenaroi, M.; Ferracane, J.L. Academy of Dental Materials guidance—Resin composites: Part I—Mechanical properties. Dent. Mater. 2017, 33, 880–894. [Google Scholar] [CrossRef]
- Moosavi, H.; Zeynali, M.; Pour, Z.H. Fracture resistance of premolars restored by various types and placement techniques of resin composites. Int. J. Dent. 2012, 2012, 973641. [Google Scholar] [CrossRef]
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J.M. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Ástvaldsdóttir, Á.; Dagerhamn, J.; van Dijken, J.W.; Naimi-Akbar, A.; Sandborgh-Englund, G.; Tranæus, S.; Nilsson, M. Longevity of posterior resin composite restorations in adults–A systematic review. J. Dent. 2015, 43, 934–954. [Google Scholar] [CrossRef]
- Peumans, M.; Politano, G.; Van Meerbeek, B.; Leuven, K.U. Effective Protocol for Daily High-quality Direct Posterior Composite Restorations. Cavity Preparation and Design. J. Adhes. Dent. 2020, 22, 581–596. [Google Scholar]
- Agrawal, V.; Shah, A.; Kapoor, S. Effect of fiber orientation and placement on fracture resistance of large class II mesio-occluso-distal cavities in maxillary premolars: An in vitro study. J. Conserv. Dent. 2022, 25, 122–127. [Google Scholar] [CrossRef]
- Scotti, N.; Michelotto Tempesta, R.; Pasqualini, D.; Baldi, A.; Vergano, E.A.; Baldissara, P.; Alovisi, M.; Comba, A. 3D interfacial gap and fracture resistance of endodontically treated premolars restored with fiber-reinforced composites. J. Adhes. Dent. 2020, 22, 215–224. [Google Scholar]
- Zhang, X.; Zhang, Q.; Meng, X.; Ye, Y.; Feng, D.; Xue, J.; Wang, H.; Huang, H.; Wang, M.; Wang, J. Rheological and mechanical properties of resin-based materials applied in dental restorations. Polymers 2021, 13, 2975. [Google Scholar] [CrossRef]
- Jakab, A.; Volom, A.; Sáry, T.; Vincze-Bandi, E.; Braunitzer, G.; Alleman, D.; Garoushi, S.; Fráter, M. Mechanical Performance of Direct Restorative Techniques Utilizing Long Fibers for “Horizontal Splinting” to Reinforce Deep MOD Cavities—An Updated Literature Review. Polymers 2022, 14, 1438. [Google Scholar] [CrossRef]
- Mangoush, E.; Garoushi, S.; Lassila, L.; Vallittu, P.K.; Säilynoja, E. Effect of fiber reinforcement type on the performance of large posterior restorations: A review of in vitro studies. Polymers 2021, 13, 3682. [Google Scholar] [CrossRef]
- Butterworth, C.; Ellakwa, A.E.; Shortall, A. Fibre-reinforced composites in restorative dentistry. Dent. Update 2003, 30, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Avcılar, İ.H.; Bakır, Ş. Use of fiber-containing materials in restorative dentistry. J. Dent. Sci. Educ. 2023, 1, 49–54. [Google Scholar] [CrossRef]
- Rajak, D.K.; Pagar, D.D.; Menezes, P.L.; Linul, E. Fiber-reinforced polymer composites: Manufacturing, properties, and applications. Polymers 2019, 11, 1667. [Google Scholar] [CrossRef]
- Vallittu, P.; Özcan, M. Clinical Guide to Principles of Fiber-Reinforced Composites in Dentistry, 1st ed.; Woodhead Publishing: Sawston, UK, 2017; pp. 100–120. [Google Scholar]
- Dyer, S.R.; Lassila, L.V.J.; Jokinen, M.; Vallittu, P.K. Effect of fiber position and orientation on fracture load of fiber-reinforced composite. Dent. Mater. 2004, 20, 947–955. [Google Scholar] [CrossRef]
- Belli, S.; Erdemir, A.; Yildirim, C. Reinforcement effect of polyethylene fibre in root-filled teeth: Comparison of two restoration techniques. Int. Endod. J. 2006, 39, 136–142. [Google Scholar] [CrossRef]
- Belli, S.; Cobankara, F.K.; Eraslan, O.; Eskitascioglu, G.; Karbhari, V. The effect of fiber insertion on fracture resistance of endodontically treated molars with MOD cavity and reattached fractured lingual cusps. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 79, 35–41. [Google Scholar] [CrossRef]
- Belli, S.; Erdemir, A.; Ozcopur, M.; Eskitascioglu, G. The effect of fibre insertion on fracture resistance of root filled molar teeth with MOD preparations restored with composite. Int. Endod. J. 2005, 38, 73–80. [Google Scholar] [CrossRef]
- Bijelic-Donova, J.; Bath, A.K.; Rocca, G.T.; Bella, E.D.; Saratti, C.M. Can Fiber-reinforced Composites Increase the Fracture Resistance of Direct Composite Restorations in Structurally Compromised Teeth? A Systematic Review and Meta-analysis of Laboratory Studies. Oper. Dent. 2025, 50, E1–E29. [Google Scholar] [CrossRef]
- Ferrando Cascales, Á.; Andreu Murillo, A.; Ferrando Cascales, R.; Agustín-Panadero, R.; Sauro, S.; Carreras-Presas, C.M.; Hirata, R.; Lijnev, A. Revolutionizing Restorative Dentistry: The Role of Polyethylene Fiber in Biomimetic Dentin Reinforcement—Insights from In Vitro Research. J. Funct. Biomater. 2025, 16, 38. [Google Scholar] [CrossRef] [PubMed]
- Abdulamir, S.W.; Majeed, M.A. Fracture resistance of endodontically treated maxillary premolar teeth restored with wallpapering technique: A comparative in vitro study. Int. J. Dent. 2023, 2023, 6159338. [Google Scholar] [CrossRef]
- Sáry, T.; Garoushi, S.; Braunitzer, G.; Alleman, D.; Volom, A.; Fráter, M. Fracture behaviour of MOD restorations reinforced by various fibre-reinforced techniques—An in vitro study. J. Mech. Behav. Biomed. Mater. 2019, 98, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Taha, N.A.; Palamara, J.E.; Messer, H.H. Fracture strength and fracture patterns of root filled teeth restored with direct resin restorations. J. Dent. 2011, 39, 527–535. [Google Scholar] [CrossRef]
- Ramírez-Gómez, J.F.; Ortiz-Magdaleno, M.; Zavala-Alonso, N.V. Effect of polyethylene fiber orientation on fracture resistance of endodontically treated premolars. J. Prosthet. Dent. 2024, 131, 92.e1–92.e8. [Google Scholar] [CrossRef]
- Soto-Cadena, S.L.; Zavala-Alonso, N.V.; Cerda-Cristerna, B.I.; Ortiz-Magdaleno, M. Effect of short fiber-reinforced composite combined with polyethylene fibers on fracture resistance of endodontically treated premolars. J. Prosthet. Dent. 2023, 129, 598.e1–598.e10. [Google Scholar] [CrossRef]
- Singhal, S.; Gurtu, A.; Singhal, A.; Bansal, R.; Mohan, S. Effect of different composite restorations on the cuspal deflection of premolars restored with different insertion techniques—An in vitro study. J. Clin. Diagn. Res. 2017, 11, ZC67–ZC70. [Google Scholar] [CrossRef]
- Forster, A.; Braunitzer, G.; Tóth, M.; Szabó, B.P.; Fráter, M. In Vitro Fracture Resistance of Adhesively Restored Molar Teeth with Different MOD Cavity Dimensions. J. Prosthodont. 2019, 28, e325–e331. [Google Scholar] [CrossRef]
- Özüdoğru, S.; Tosun, G. Evaluation of Microleakage and Fatigue Behaviour of Several Fiber Application Techniques in Composite Restorations. Ann. Dent. Spec. 2022, 10, 60–66. [Google Scholar] [CrossRef]
- Deliperi, S.; Alleman, D.; Rudo, D. Stress-reduced direct composites for the restoration of structurally compromised teeth: Fiber design according to the “wallpapering” technique. Oper. Dent. 2017, 42, 233–243. [Google Scholar] [CrossRef]
- Khan, S.I.R.; Ramachandran, A.; Alfadley, A.; Baskaradoss, J.K. Ex vivo fracture resistance of teeth restored with glass and fiber reinforced composite resin. J. Mech. Behav. Biomed. Mater. 2018, 82, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Akman, S.; Akman, M.; Eskitascioglu, G.; Belli, S. Influence of several fibre-reinforced composite restoration techniques on cusp movement and fracture strength of molar teeth. Int. Endod. J. 2011, 44, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Rahman, H.; Singh, S.; Chandra, A.; Chandra, R.; Tripathi, S. Evaluation of fracture resistance of endodontically treated teeth restored with composite resin along with fibre insertion in different positions in vitro. Aust. Endod. J. 2016, 42, 60–65. [Google Scholar] [CrossRef]
- Hamouda, I.M.; Shehata, S.H. Fracture resistance of posterior teeth restored with modern restorative materials. J. Biomed. Res. 2011, 25, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Mergulhão, V.A.; De Mendonça, L.S.; De Albuquerque, M.S.; Braz, R. Fracture resistance of endodontically treated maxillary premolars restored with different methods. Oper. Dent. 2019, 44, E1–E11. [Google Scholar] [CrossRef]
- Megahed, M.S.; Zaghloul, A.I. Fracture Resistance of Maxillary Premolar Teeth Restored with Bulk Fill Resin Composite: In-vitro Study. Mansoura J. Dent. 2020, 7, 56–60. [Google Scholar]
- Gale, M.S.; Darvell, B.W. Thermal cycling procedures for laboratory testing of dental restorations. J. Dent. 1999, 27, 89–99. [Google Scholar] [CrossRef]
- Morresi, A.L.; D’Amario, M.; Capogreco, M.; Gatto, R.; Marzo, G.; D’Arcangelo, C.; Monaco, A. Thermal cycling for restorative materials: Does a standardized protocol exist in laboratory testing? A literature review. J. Mech. Behav. Biomed. Mater. 2014, 29, 295–308. [Google Scholar] [CrossRef]
- Taher, H.M.; Haridy, M. Fracture resistance of maxillary premolars restored with different fiber-reinforced composites: An in vitro study. Egypt. Dent. J. 2019, 65, 1833–1843. [Google Scholar] [CrossRef]
- Soares, C.J.; Pizi, E.C.; Fonseca, R.B.; Martins, L.R. Influence of root embedment material and periodontal ligament simulation on fracture resistance tests. Braz. Oral. Res. 2005, 19, 11–16. [Google Scholar] [CrossRef]
- Mincik, J.; Urban, D.; Timkova, S.; Urban, R. Fracture resistance of endodontically treated maxillary premolars restored by various direct filling materials: An in vitro study. Int. J. Biomater. 2016, 2016, 9138945. [Google Scholar] [CrossRef] [PubMed]
- Battancs, E.; Sáry, T.; Molnár, J.; Braunitzer, G.; Skolnikovics, M.; Schindler, Á.; Szabó P., B.; Garoushi, S.; Fráter, M. Fracture Resistance and Microleakage around Direct Restorations in High C-Factor Cavities. Polymers 2022, 14, 3463. [Google Scholar] [CrossRef]
- Fráter, M.; Sáry, T.; Vincze-Bandi, E.; Volom, A.; Braunitzer, G.; Szabó P., B.; Garoushi, S.; Forster, A. Fracture behavior of short fiber-reinforced direct restorations in large MOD cavities. Polymers 2021, 13, 2040. [Google Scholar] [CrossRef]
- Scotti, N.; Coero Borga, F.A.; Alovisi, M.; Rota, R.; Pasqualini, D.; Berutti, E. Is fracture resistance of endodontically treated mandibular molars restored with indirect onlay composite restorations influenced by fibre post insertion? J. Dent. 2012, 40, 814–820. [Google Scholar] [CrossRef]
- Szabó, P.B.; Sáry, T.; Szabó, B. The key elements of conducting load-to-fracture mechanical testing on restoration-tooth units in restorative dentistry. Analecta Tech. Szeged. 2019, 13, 59–64. [Google Scholar] [CrossRef]
- Singer, L.; Fouda, A.; Bourauel, C. Biomimetic approaches and materials in restorative and regenerative dentistry. BMC Oral Health 2023, 23, 105. [Google Scholar] [CrossRef] [PubMed]
- Sengun, A.; Cobankara, F.K.; Orucoglu, H. Effect of a new restoration technique on fracture resistance of endodontically treated teeth. Dent. Traumatol. 2008, 24, 214–219. [Google Scholar] [CrossRef]
- Szabó, V.T.; Szabó, B.; Barcsayné-Tátrai, N.; Mészáros, C.; Braunitzer, G.; Szabó, B.P.; Lassila, L.; Garoushi, S.; Fráter, M. Fatigue Resistance of Dissected Lower First Molars Restored with Direct Fiber-Reinforced Bridges—An In Vitro Pilot Study. Polymers 2023, 15, 1343. [Google Scholar] [CrossRef]
- Khan, S.; Sitlani, M.; Pandey, S.; Singh, S.K.; Mishra, P.; Narang, A. To Study Fracture Resistance of InterligTM Glass Fiber Orientation and Placement on Large Class II Cavities in Maxillary Premolars: An in Vitro Study. Dent. J. 2023, 4, 48–58. [Google Scholar] [CrossRef]
- Hegde, V.; Sali, A.V. Fracture resistance of posterior teeth restored with high-viscosity bulk-fill resin composites in comparison to the incremental placement technique. J. Conserv. Dent. 2017, 20, 360–364. [Google Scholar]
- Hood, J.A. Biomechanics of the intact, prepared and restored tooth: Some clinical implications. Int. Dent. J. 1991, 41, 25–32. [Google Scholar] [PubMed]
- Ayad, M.F.; Maghrabi, A.A.; Garcia-Godoy, F. Resin composite polyethylene fiber reinforcement: Effect on fracture resistance of weakened marginal ridges. Am. J. Dent. 2010, 23, 133–136. [Google Scholar]
- Hazar, E.; Hazar, A. Effect of Long Glass Fiber Orientations or a Short-Fiber-Reinforced Composite on the Fracture Resistance of Endodontically Treated Premolars. Polymers 2024, 16, 1289. [Google Scholar] [CrossRef]
- Oskoee, P.A.; Ajami, A.A.; Navimipour, E.J.; Oskoee, S.S.; Sadjadi, J. The Effect of Three Composite Fiber Insertion Techniques on Fracture Resistance of Root-filled Teeth. J. Endod. 2009, 35, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Küçük, Ö.; Keçeci, A.D. Strengthening effect of different fiber placement designs on root canal treated and bleached premolars. Odontology 2021, 109, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Bahari, M.; Mohammadi, N.; Kimyai, S.; Kahnamoui, M.A.; Vahedpour, H.; Torkani, M.A.M.; Oskoee, A.S. Effect of Different Fiber Reinforcement Strategies on the Fracture Strength of Composite Resin Restored Endodontically Treated Premolars. Pesqui. Bras. Odontopediatria Clin. Integr. 2019, 19, e4465. [Google Scholar] [CrossRef]
- Fráter, M.; Lassila, L.; Braunitzer, G.; Vallittu, P.K.; Garoushi, S. Fracture resistance and marginal gap formation of post-core restorations: Influence of different fiber-reinforced composites. Clin. Oral Investig. 2020, 24, 265–276. [Google Scholar] [CrossRef]
- Lee, J.J.W.; Kwon, J.Y.; Chai, H.; Lucas, P.W.; Thompson, V.P.; Lawn, B.R. Fracture modes in human teeth. J. Dent. Res. 2009, 88, 224–228. [Google Scholar] [CrossRef]
- Belli, S.E.; Eskitascioglu, G.Ü. Biomechanical properties and clinical use of a polyethylene fibre post-core material. Int. Dent. S. Afr. 2006, 8, 20–26. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | DF | Sum of Square | Mean Square | F Statistic | p-Value |
|---|---|---|---|---|---|
| Groups (between groups) | 5 | 4,007,787.839 | 801,557.5678 | 12.0535 | <0.0001 |
| Error (within groups) | 34 | 2,261,006.712 | 66,500.1974 | ||
| Total | 39 | 6,268,794.551 | 160,738.3218 |
| Group | Descriptive Statistics | ||||
|---|---|---|---|---|---|
| (n) | Minimum | Maximum | Mean | SD | |
| Group 1 | 10 | 667.05 | 2008.41 | 1264.13 a | 559.74 |
| Group 2 | 10 | 184.58 | 259.91 | 214.87 c | 34.49 |
| Group 3 | 10 | 447.73 | 609.71 | 546.93 bc | 59.89 |
| Group 4 | 10 | 415.21 | 919.27 | 621.08 bc | 171.61 |
| Group 5 | 10 | 409.56 | 880.07 | 734.73 b | 154.79 |
| Group 6 | 10 | 755.90 | 1687.46 | 1137.72 a | 316.20 |
| Group | Failure Mode | Significance | |||
|---|---|---|---|---|---|
| Non-Restorable Failure | Restorable Failure | ||||
| n * | % | n | % | ||
| Sound | 1 | 10 | 9 | 90 | a |
| Cavity | 8 | 80 | 2 | 20 | b |
| Composite | 6 | 60 | 4 | 40 | bc |
| Pulpal Floor | 5 | 50 | 5 | 50 | ac |
| Wallpapering | 3 | 30 | 7 | 70 | a |
| Occlusal Groove | 1 | 10 | 9 | 90 | a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, R.H.; ElKassas, D.W.; Nabih, S.M.; Salem, M.N.; Haridy, R. The Impact of Different Fiber Placement Techniques on the Fracture Resistance of Premolars Restored with Direct Resin Composite, In Vitro Study. J. Funct. Biomater. 2025, 16, 225. https://doi.org/10.3390/jfb16060225
Ibrahim RH, ElKassas DW, Nabih SM, Salem MN, Haridy R. The Impact of Different Fiber Placement Techniques on the Fracture Resistance of Premolars Restored with Direct Resin Composite, In Vitro Study. Journal of Functional Biomaterials. 2025; 16(6):225. https://doi.org/10.3390/jfb16060225
Chicago/Turabian StyleIbrahim, Reham Hesham, Dina Wafik ElKassas, Sameh Mahmoud Nabih, Mennatallah Naguib Salem, and Rasha Haridy. 2025. "The Impact of Different Fiber Placement Techniques on the Fracture Resistance of Premolars Restored with Direct Resin Composite, In Vitro Study" Journal of Functional Biomaterials 16, no. 6: 225. https://doi.org/10.3390/jfb16060225
APA StyleIbrahim, R. H., ElKassas, D. W., Nabih, S. M., Salem, M. N., & Haridy, R. (2025). The Impact of Different Fiber Placement Techniques on the Fracture Resistance of Premolars Restored with Direct Resin Composite, In Vitro Study. Journal of Functional Biomaterials, 16(6), 225. https://doi.org/10.3390/jfb16060225