
Tomographic Assessment of Bone Regeneration in Osteochondral Lesion Treated with Various Biomaterials in a Sheep Model Study
 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Animals
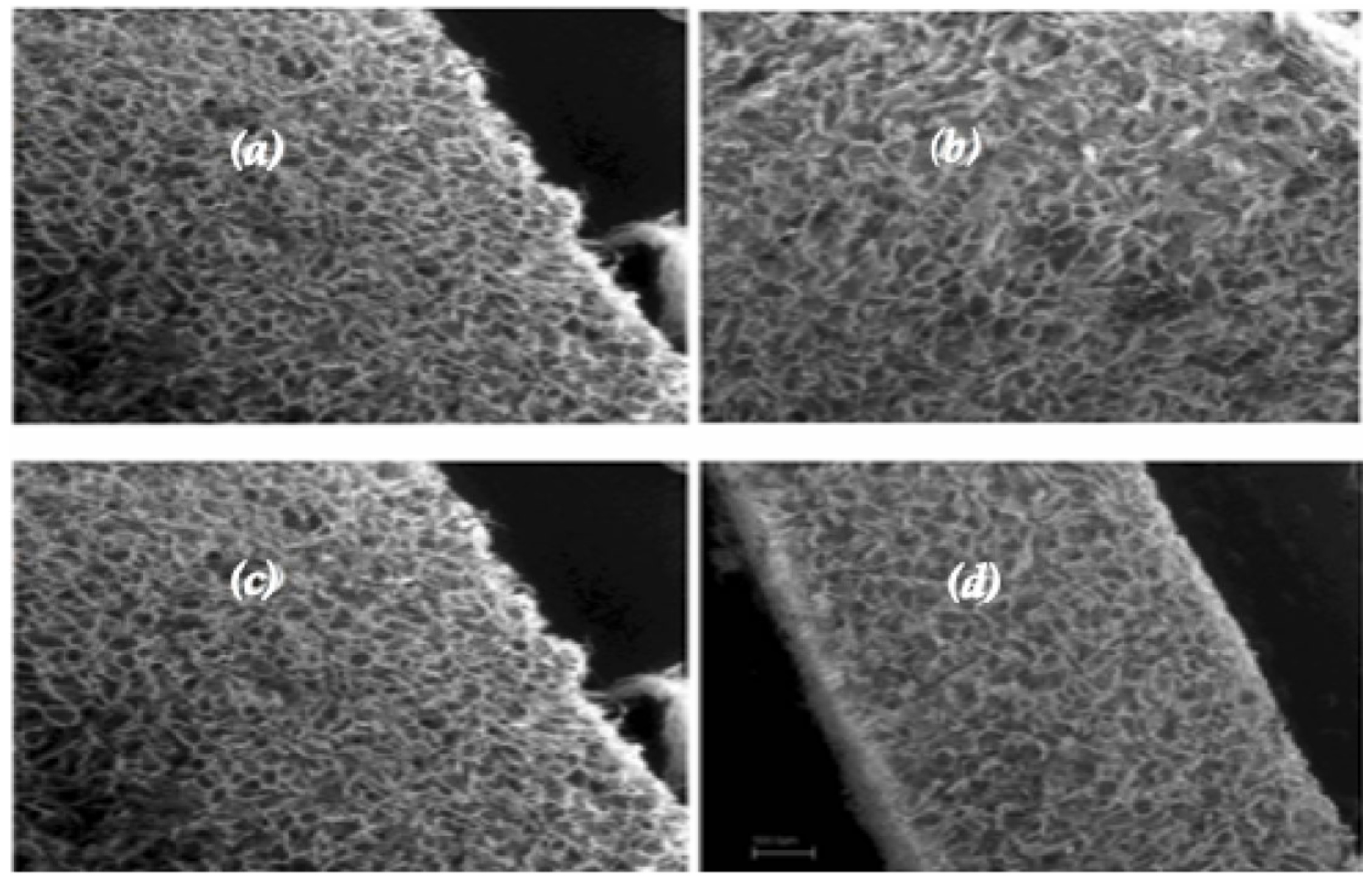
2.3. Scaffolds
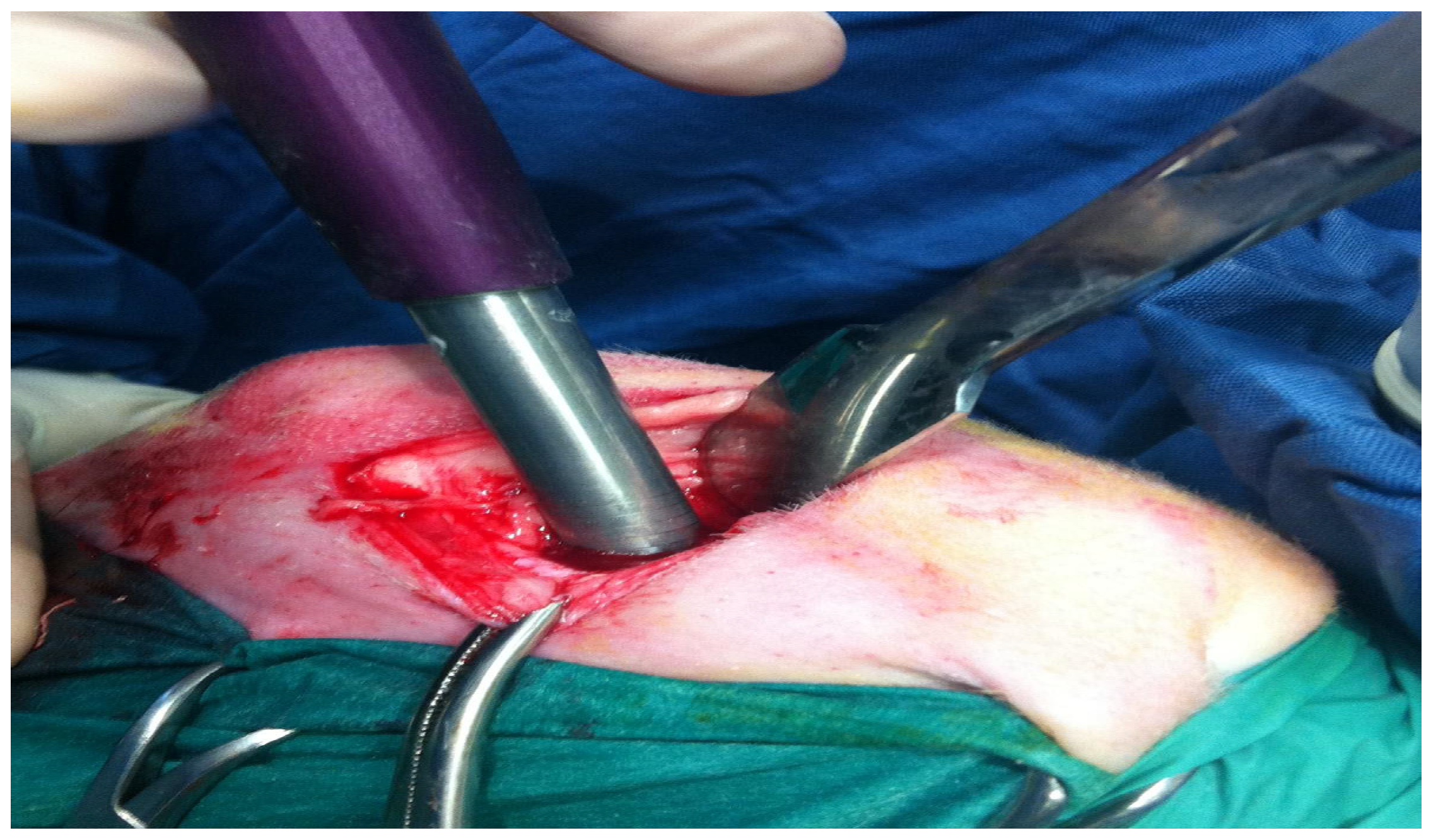
2.4. Anesthesia and Surgical Procedures
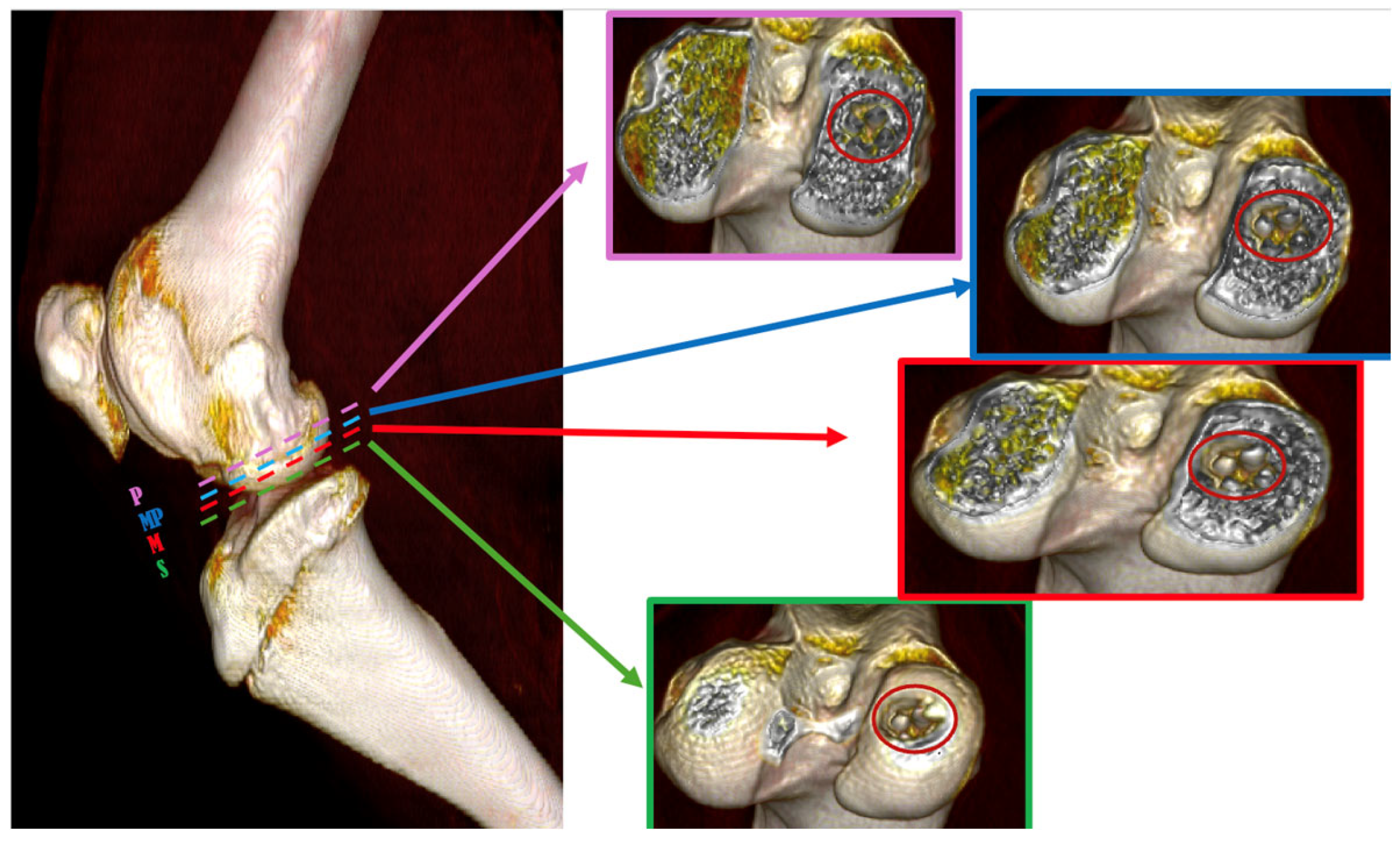
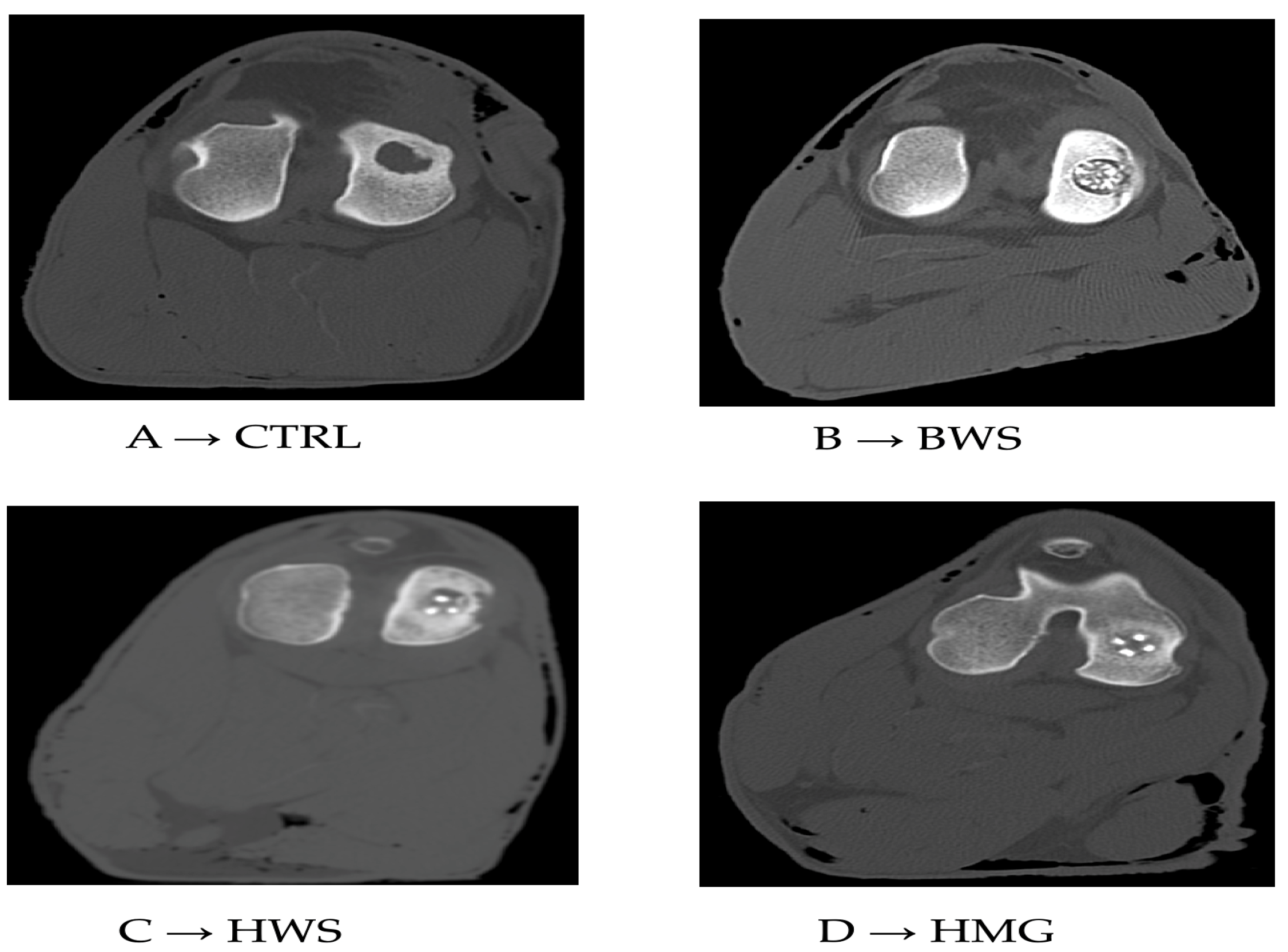
2.5. CT Evaluation
2.6. Statistical Analyzes
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lesage, C.; Lafont, M.; Guihard, P.; Weiss, P.; Guicheux, J.; Delplace, V. Material-Assisted Strategies for Osteochondral Defect Repair. Adv. Sci. 2022, 9, 2200050. [Google Scholar] [CrossRef]
- Bader, D.L.; Salter, D.M.; Chowdhury, T.T. Biomechanical Influence of Cartilage Homeostasis in Health and Disease. Arthritis 2011, 2011, 979032. [Google Scholar] [CrossRef]
- Crovace, A.M.; Giancamillo, A.D.; Gervaso, F.; Mangiavini, L.; Zani, D.; Scalera, F.; Palazzo, B.; Izzo, D.; Agnoletto, M.; Domenicucci, M.; et al. Evaluation of in Vivo Response of Three Biphasic Scaffolds for Osteochondral Tissue Regeneration in a Sheep Model. Vet. Sci. 2019, 6, 90. [Google Scholar] [CrossRef]
- Jacob, G.; Shimomura, K.; Nakamura, N. Osteochondral Injury, Management and Tissue Engineering Approaches. Front. Cell Dev. Biol. 2020, 8, 14. [Google Scholar] [CrossRef]
- Verhagen, R.A.; Struijs, P.; Bossuyt, P.; van Dijk, C. Systematic Review of Treatment Strategies for Osteochondral Defects of the Talar Dome. Foot Ankle Clin. 2003, 8, 233–242. [Google Scholar] [CrossRef]
- Oshima, T.; Nakase, J.; Toratani, T.; Numata, H.; Takata, Y.; Nakayama, K.; Tsuchiya, H. A Scaffold-Free Allogeneic Construct from Adipose-Derived Stem Cells Regenerates an Osteochondral Defect in a Rabbit Model. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 583–593. [Google Scholar] [CrossRef]
- Shen, T.; Dai, Y.; Li, X.; Xu, S.; Gou, Z.; Gao, C. Regeneration of the Osteochondral Defect by a Wollastonite and Macroporous Fibrin Biphasic Scaffold. ACS Biomater. Sci. Eng. 2017, 4, 1942–1953. [Google Scholar] [CrossRef]
- Jia, S.; Wang, J.; Zhang, T.; Pan, W.; Li, Z.; He, X.; Yang, C.; Wu, Q.-N.; Sun, W.; Xiong, Z.; et al. Multilayered Scaffold with a Compact Interfacial Layer Enhances Osteochondral Defect Repair. ACS Appl. Mater. Interfaces 2018, 10, 20296–20305. [Google Scholar] [CrossRef]
- Choi, J.R. Applications of Biomaterials in Regenerative Medicine. J. Stem Cell Res. Med. 2019, 4, 1–3. [Google Scholar] [CrossRef]
- Hinderer, S.; Layland, S.L.; Schenke-Layland, K. ECM and ECM-like Materials—Biomaterials for Applications in Regenerative Medicine and Cancer Therapy. Adv. Drug Deliv. Rev. 2016, 97, 260–269. [Google Scholar] [CrossRef]
- Izadifar, Z.; Chen, X.; Kulyk, W. Strategic Design and Fabrication of Engineered Scaffolds for Articular Cartilage Repair. JFB 2012, 3, 799–838. [Google Scholar] [CrossRef]
- Tessaro, I.; Nguyen, V.T.; Di Giancamillo, A.; Agnoletto, M.; Verdoni, F.; Domenicucci, M.; Scurati, R.; Peretti, G.M.; Mangiavini, L. Animal Models for Cartilage Repair. J. Biol. Regul. Homeost. Agents 2018, 32, 105–116. [Google Scholar]
- Longley, R.; Ferreira, A.M.; Gentile, P. Recent Approaches to the Manufacturing of Biomimetic Multi-Phasic Scaffolds for Osteochondral Regeneration. IJMS 2018, 19, 1755. [Google Scholar] [CrossRef]
- Maia, F.R.; Carvalho, M.R.; Oliveira, J.M.; Reis, R.L. Tissue Engineering Strategies for Osteochondral Repair. In Osteochondral Tissue Engineering; Oliveira, J.M., Pina, S., Reis, R.L., San Roman, J., Eds.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Germany, 2018; Volume 1059, pp. 353–371. ISBN 978-3-319-76734-5. [Google Scholar]
- Palazzo, B.; Scalera, F.; Soloperto, G.; Scialla, S.; Gervaso, F. Recent Strategies in Osteochondral Substitutes Design: Towards the Mimicking of a Multifaceted Anatomical Unit from the Nano to the Macro Level. J. Nanomed. Nanotechnol. 2017, 8, 7. [Google Scholar] [CrossRef]
- Gorbachova, T.; Melenevsky, Y.; Cohen, M.; Cerniglia, B.W. Osteochondral Lesions of the Knee: Differentiating the Most Common Entities at MRI. RadioGraphics 2018, 38, 1478–1495. [Google Scholar] [CrossRef]
- Hounsfield, G.N. Computed Medical Imaging. J. Comput. Assist. Tomogr. 1980, 4, 665–674. [Google Scholar] [CrossRef]
- Bolus, D.; Morgan, D.; Berland, L. Effective Use of the Hounsfield Unit in the Age of Variable Energy CT. Abdom. Radiol. 2017, 42, 766–771. [Google Scholar] [CrossRef]
- Razi, T.; Niknami, M.; Alavi Ghazani, F. Relationship between Hounsfield Unit in CT Scan and Gray Scale in CBCT. J. Dent. Res. Dent. Clin. Dent. Prospect. 2014, 8, 107–110. [Google Scholar] [CrossRef]
- Banstola, A.; Reynolds, J.N.J. The Sheep as a Large Animal Model for the Investigation and Treatment of Human Disorders. Biology 2022, 11, 1251. [Google Scholar] [CrossRef]
- Holt, J.D.S.; Cameron, D.; Dias, N.; Holding, J.; Muntendam, A.; Oostebring, F.; Dreier, P.; Rohan, L.; Nuttall, J. The Sheep as a Model of Preclinical Safety and Pharmacokinetic Evaluations of Candidate Microbicides. Antimicrob. Agents Chemother. 2015, 59, 3761–3770. [Google Scholar] [CrossRef]
- Mow, V.C.; Ratcliffe, A.; Robin Poole, A. Cartilage and Diarthrodial Joints as Paradigms for Hierarchical Materials and Structures. Biomaterials 1992, 13, 67–97. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, S.K.; Carrozzo, M.; Gervaso, F.; Scalera, F.; Sannino, A.; Licciulli, A. Mechanical Performance and In Vitro Studies of Hydroxyapatite/Wollastonite Scaffold for Bone Tissue Engineering. KEM 2011, 493–494, 855–860. [Google Scholar] [CrossRef]
- Gervaso, F.; Scalera, F.; Kunjalukkal Padmanabhan, S.; Sannino, A.; Licciulli, A. High-Performance Hydroxyapatite Scaffolds for Bone Tissue Engineering Applications. Int. J. Appl. Ceram. Tech. 2012, 9, 507–516. [Google Scholar] [CrossRef]
- Gervaso, F.; Padmanabhan, S.K.; Scalera, F.; Sannino, A.; Licciulli, A. Mechanical Stability of Highly Porous Hydroxyapatite Scaffolds during Different Stages of in Vitro Studies. Mater. Lett. 2016, 185, 239–242. [Google Scholar] [CrossRef]
- Parisi, C.; Gervaso, F.; Scalera, F.; Padmanabhan, S.K.; Nobile, C.; Cozzoli, P.D.; Di Silvio, L.; Sannino, A. Influence of the Precipitation Temperature on Properties of Nanohydroxyapatite Powder for the Fabrication of Highly Porous Bone Scaffolds. KEM 2013, 587, 27–32. [Google Scholar] [CrossRef]
- Scalera, F.; Gervaso, F.; Sanosh, K.P.; Sannino, A.; Licciulli, A. Influence of the Calcination Temperature on Morphological and Mechanical Properties of Highly Porous Hydroxyapatite Scaffolds. Ceram. Int. 2013, 39, 4839–4846. [Google Scholar] [CrossRef]
- Sosio, C.; Di Giancamillo, A.; Deponti, D.; Gervaso, F.; Scalera, F.; Melato, M.; Campagnol, M.; Boschetti, F.; Nonis, A.; Domeneghini, C.; et al. Osteochondral Repair by a Novel Interconnecting Collagen–Hydroxyapatite Substitute: A Large-Animal Study. Tissue Eng. Part. A 2015, 21, 704–715. [Google Scholar] [CrossRef]
- Deponti, D.; Giancamillo, A.D.; Gervaso, F.; Domenicucci, M.; Domeneghini, C.; Sannino, A.; Peretti, G.M. Collagen Scaffold for Cartilage Tissue Engineering: The Benefit of Fibrin Glue and the Proper Culture Time in an Infant Cartilage Model. Tissue Eng. Part. A 2014, 20, 1113–1126. [Google Scholar] [CrossRef]
- Gullotta, F.; Izzo, D.; Scalera, F.; Palazzo, B.; Martin, I.; Sannino, A.; Gervaso, F. Biomechanical Evaluation of hMSCs-Based Engineered Cartilage for Chondral Tissue Regeneration. J. Mech. Behav. Biomed. Mater. 2018, 86, 294–304. [Google Scholar] [CrossRef]
- Gervaso, F.; Mangiavini, L.; Di Giancamillo, A.; Boschetti, F.; Izzo, D.; Zani, D.D.; Di Giancamillo, M.; Tessaro, I.; Domenicucci, M.; Scalera, F.; et al. Comparison of Three Novel Biphasic Scaffolds for One-Stage Treatment of Osteochondral Defects in a Sheep Model. J. Biol. Regul. Homeost. Agents 2016, 30, 24–31. [Google Scholar]
- Roohani-Esfahani, S.-I.; Nouri-Khorasani, S.; Lu, Z.; Appleyard, R.; Zreiqat, H. The Influence Hydroxyapatite Nanoparticle Shape and Size on the Properties of Biphasic Calcium Phosphate Scaffolds Coated with Hydroxyapatite–PCL Composites. Biomaterials 2010, 31, 5498–5509. [Google Scholar] [CrossRef]
- Zhao, J.; Xiao, S.; Lu, X.; Wang, J.; Weng, J. A Study on Improving Mechanical Properties of Porous HA Tissue Engineering Scaffolds by Hot Isostatic Pressing. Biomed. Mater. 2006, 1, 188–192. [Google Scholar] [CrossRef]
- Teixeira, S.; Rodriguez, M.A.; Pena, P.; De Aza, A.H.; De Aza, S.; Ferraz, M.P.; Monteiro, F.J. Physical Characterization of Hydroxyapatite Porous Scaffolds for Tissue Engineering. Mater. Sci. Eng. C 2009, 29, 1510–1514. [Google Scholar] [CrossRef]
- Miao, X.; Tan, D.M.; Li, J.; Xiao, Y.; Crawford, R. Mechanical and Biological Properties of Hydroxyapatite/Tricalcium Phosphate Scaffolds Coated with Poly(Lactic-Co-Glycolic Acid). Acta Biomater. 2008, 4, 638–645. [Google Scholar] [CrossRef]
- Barletta, M.; Hofmeister, E.H.; Peroni, J.F.; Thoresen, M.; Scharf, A.M.; Quandt, J.E. Influence of Sedation on Onset and Quality of Euthanasia in Sheep. Res. Vet. Sci. 2018, 117, 57–59. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Corder, G.W.; Foreman, D.I. Nonparametric Statistics for Non-Statisticians: A Step-by-Step Approach; Wiley: Hoboken, NJ, USA, 2009; ISBN 978-0-470-45461-9. [Google Scholar]
- Seo, S.-J.; Mahapatra, C.; Singh, R.K.; Knowles, J.C.; Kim, H.-W. Strategies for Osteochondral Repair: Focus on Scaffolds. J. Tissue Eng. 2014, 5, 204173141454185. [Google Scholar] [CrossRef]
- Butnariu-Ephrat, M.; Robinson, D.; Mendes, D.; Halperin, N.; Nevo, Z. Resurfacing of Goat Articular Cartilage by Chondrocytes Derived from Bone Marrow. Clin. Orthop. Relat. Res. 1996, 330, 234–243. [Google Scholar] [CrossRef]
- Strauss, E.J.; Goodrich, L.R.; Chen, C.-T.; Hidaka, C.; Nixon, A.J. Biochemical and Biomechanical Properties of Lesion and Adjacent Articular Cartilage after Chondral Defect Repair in an Equine Model. Am. J. Sports Med. 2005, 33, 1647–1653. [Google Scholar] [CrossRef]
- Zhou, L.; Ho, K.-W.K.; Zheng, L.; Xu, J.; Chen, Z.; Ye, X.; Zou, L.; Li, Y.; Chang, L.; Shao, H.; et al. A Rabbit Osteochondral Defect (OCD) Model for Evaluation of Tissue Engineered Implants on Their Biosafety and Efficacy in Osteochondral Repair. Front. Bioeng. Biotechnol. 2024, 12, 1352023. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
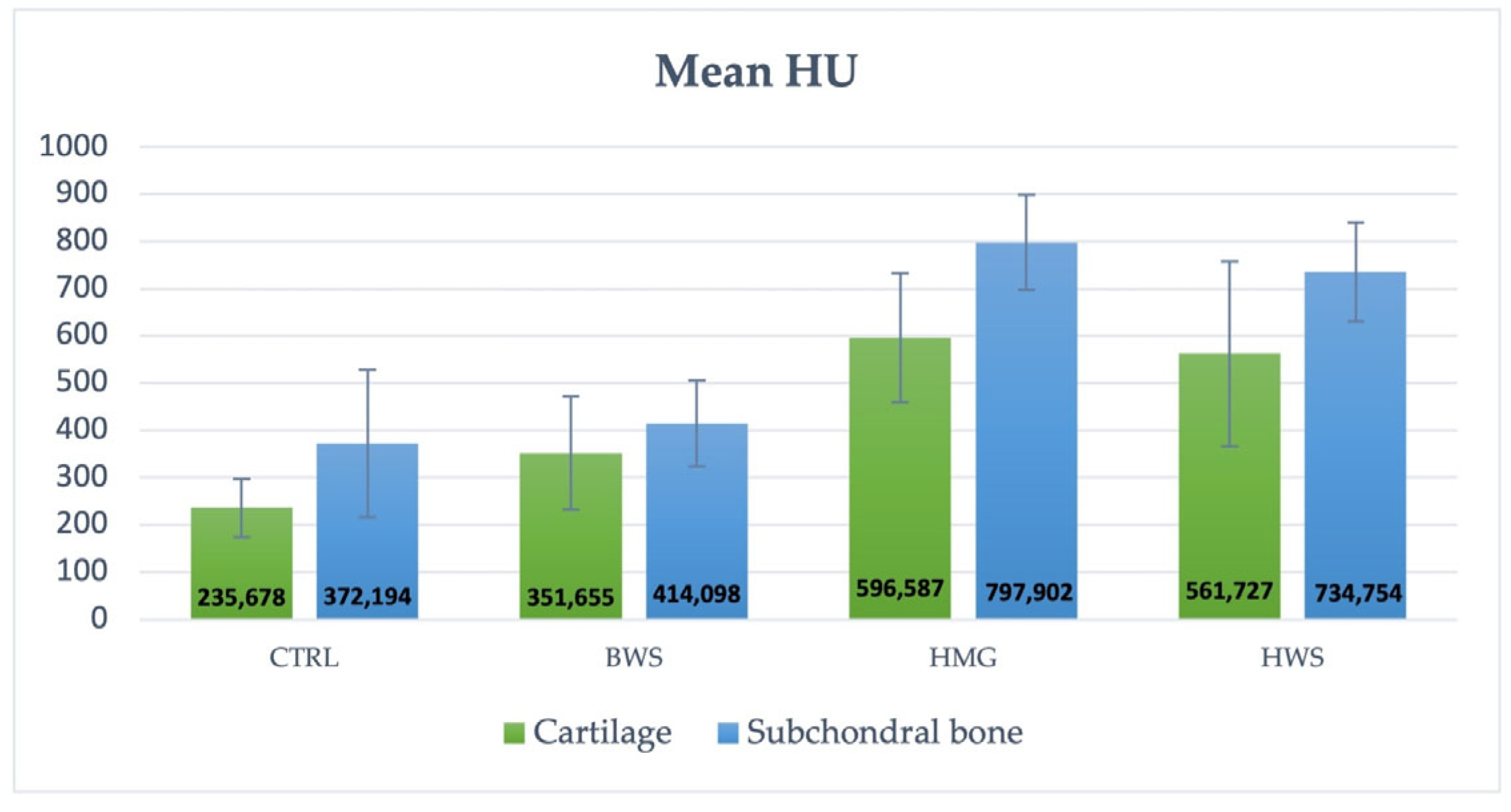
| Group | Cartilage Part | Subchondral Part |
|---|---|---|
| CTRL | 235.678 ± 61.66 HU | 372.194 ± 156.27 HU |
| BWS | 351.655 ± 120.38 HU | 414.098 ± 90.37 HU |
| HMG | 596.587 ± 136.97 HU | 797.902 ± 99.63 HU |
| HWS | 561.727 ± 196.11 HU | 734.754 ± 104.65 HU |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goga, T.; Goxha, B.; Crovace, A.M.; Cinone, M.; Lacitignola, L.; Guadalupi, M.; Lika, E. Tomographic Assessment of Bone Regeneration in Osteochondral Lesion Treated with Various Biomaterials in a Sheep Model Study. J. Funct. Biomater. 2025, 16, 120. https://doi.org/10.3390/jfb16040120
Goga T, Goxha B, Crovace AM, Cinone M, Lacitignola L, Guadalupi M, Lika E. Tomographic Assessment of Bone Regeneration in Osteochondral Lesion Treated with Various Biomaterials in a Sheep Model Study. Journal of Functional Biomaterials. 2025; 16(4):120. https://doi.org/10.3390/jfb16040120
Chicago/Turabian StyleGoga, Taulant, Bledar Goxha, Alberto Maria Crovace, Mario Cinone, Luca Lacitignola, Marta Guadalupi, and Erinda Lika. 2025. "Tomographic Assessment of Bone Regeneration in Osteochondral Lesion Treated with Various Biomaterials in a Sheep Model Study" Journal of Functional Biomaterials 16, no. 4: 120. https://doi.org/10.3390/jfb16040120
APA StyleGoga, T., Goxha, B., Crovace, A. M., Cinone, M., Lacitignola, L., Guadalupi, M., & Lika, E. (2025). Tomographic Assessment of Bone Regeneration in Osteochondral Lesion Treated with Various Biomaterials in a Sheep Model Study. Journal of Functional Biomaterials, 16(4), 120. https://doi.org/10.3390/jfb16040120