
Multiscale CT-Based Computational Modeling of Alveolar Gas Exchange during Artificial Lung Ventilation, Cluster (Biot) and Periodic (Cheyne-Stokes) Breathings and Bronchial Asthma Attack


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Mathematical Model of the Respiratory Gas Flow in the Lung
2.2. Boundary Conditions
2.3. Mathematical Model of the Oxygen and Carbon Dioxide Transport in the Lung
2.4. Numerical Implementation
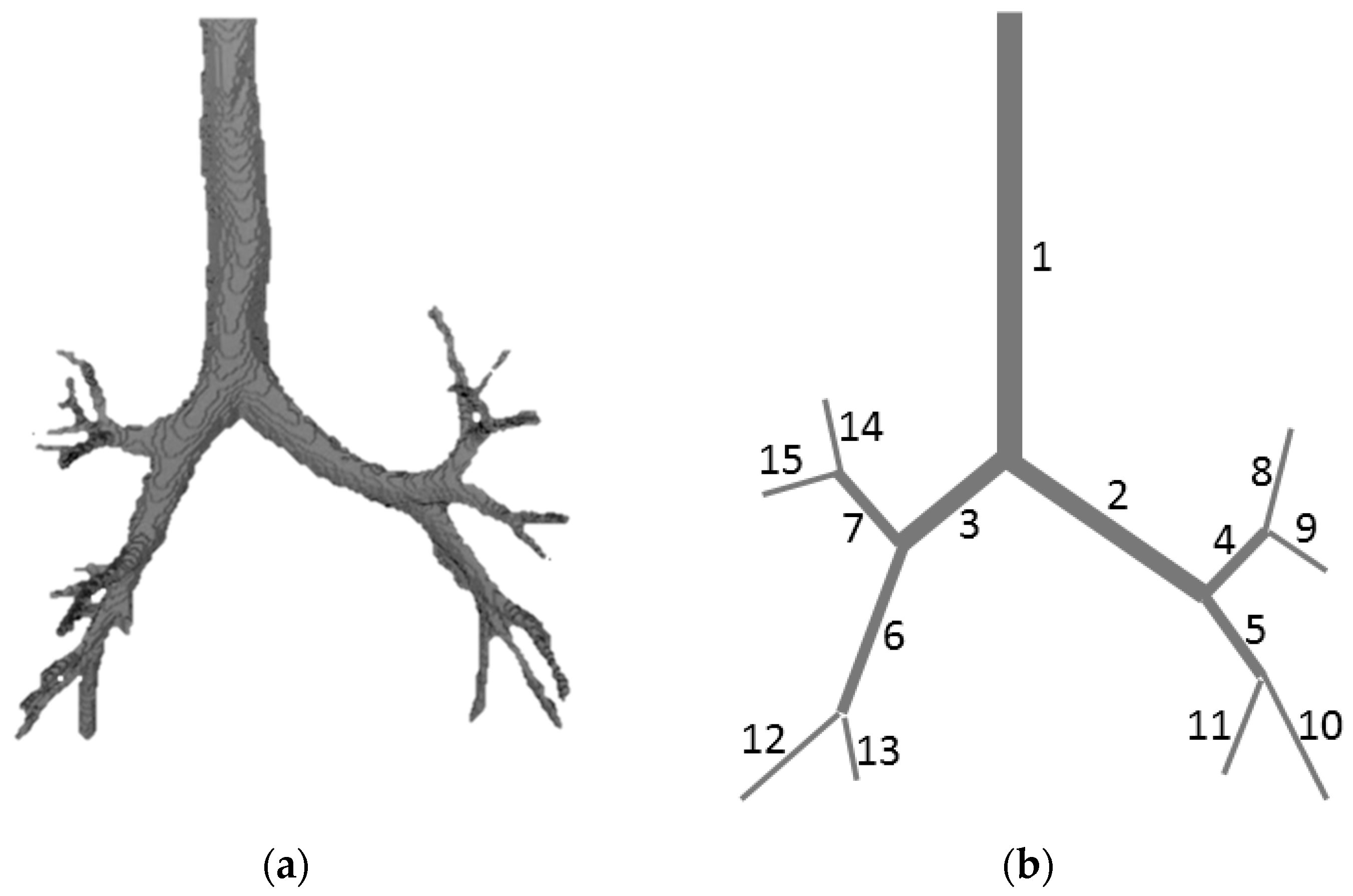
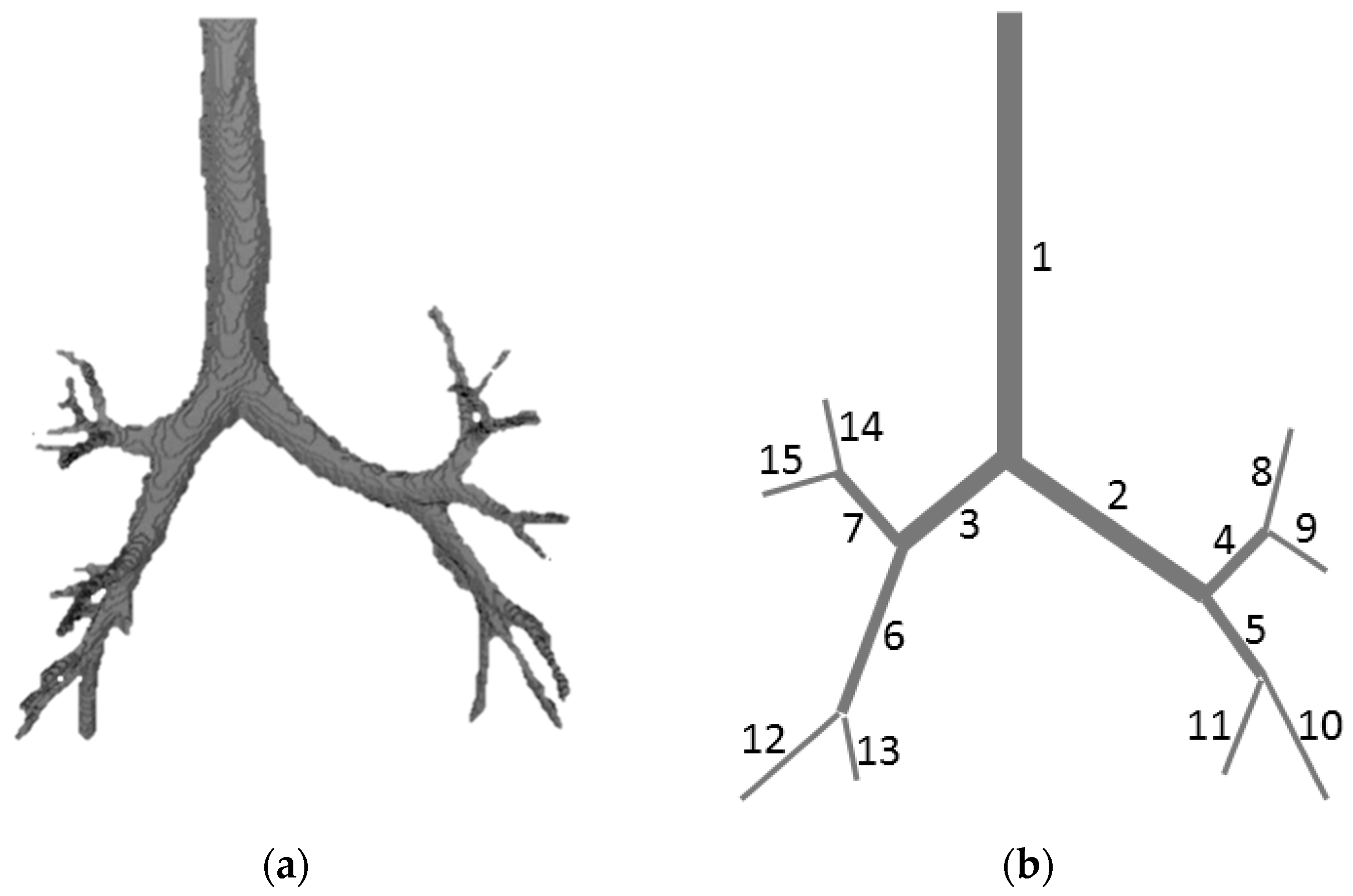
2.5. Computed Tomography (CT) Data Processing
3. Results
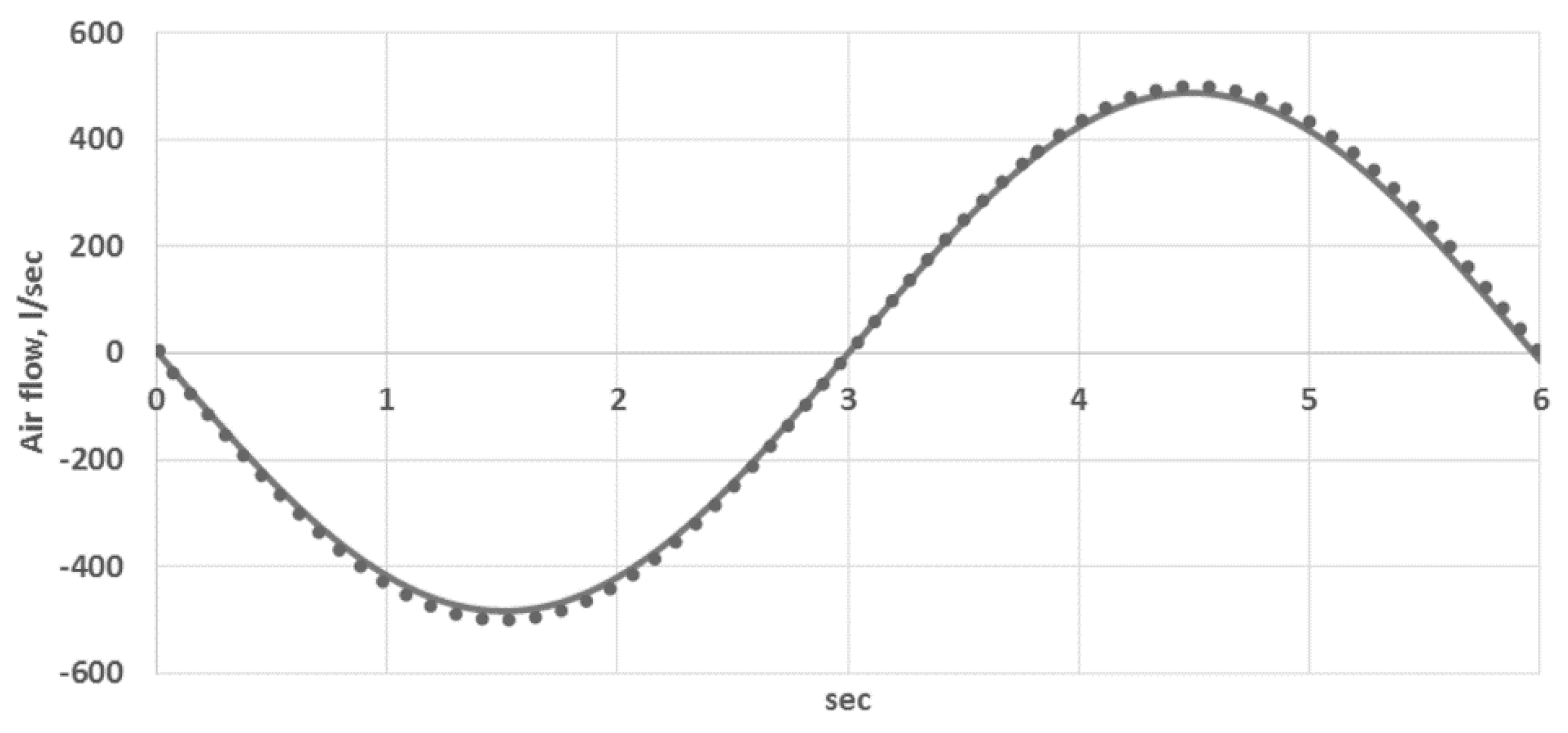
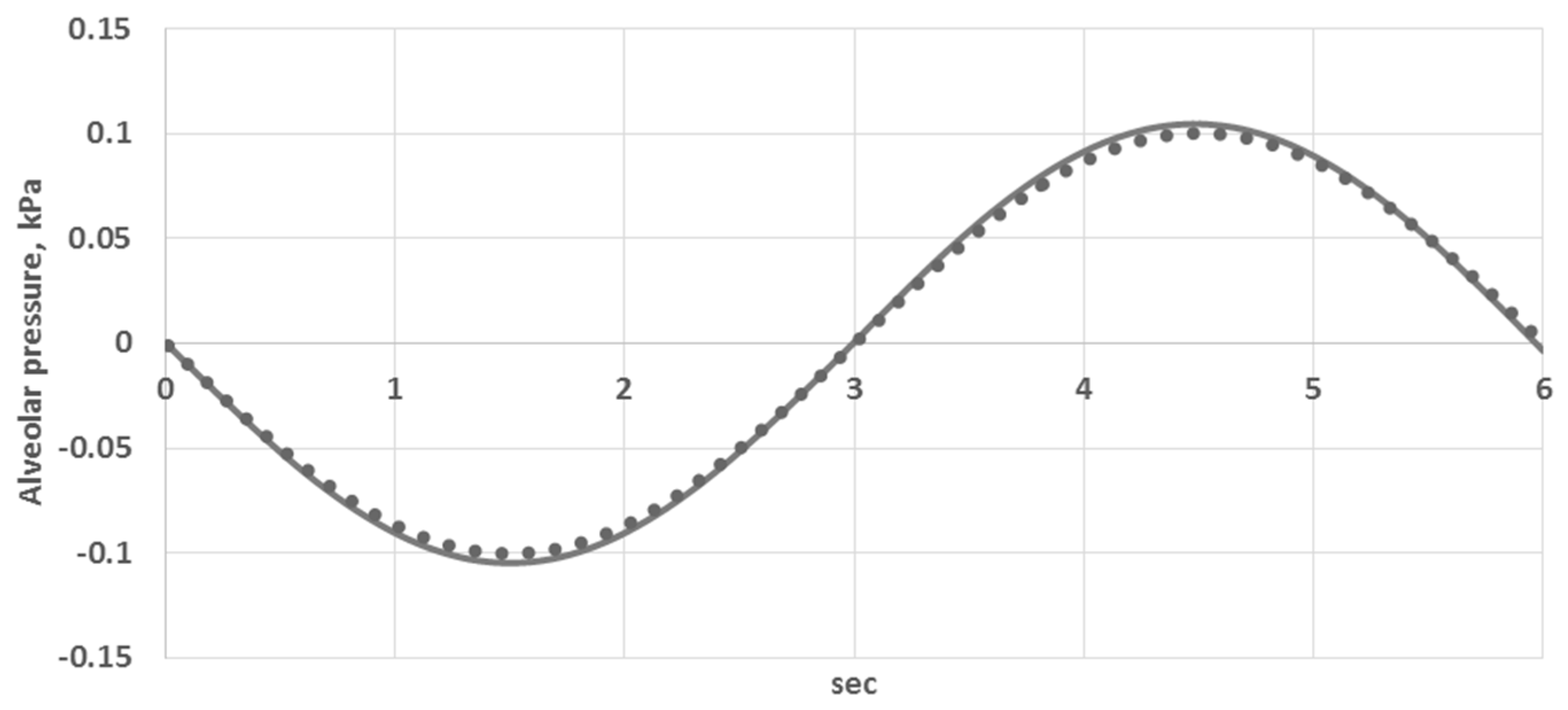
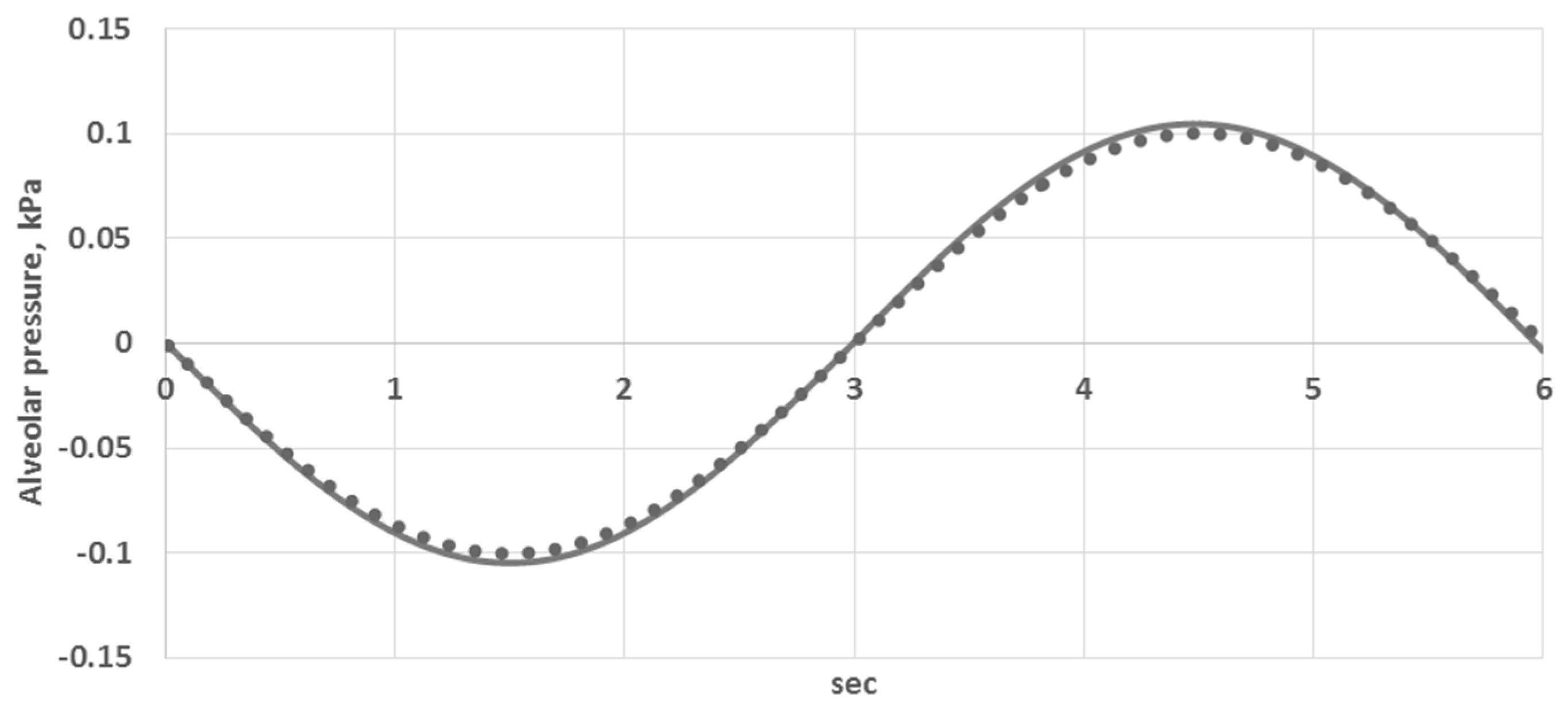
3.1. The Model Validation
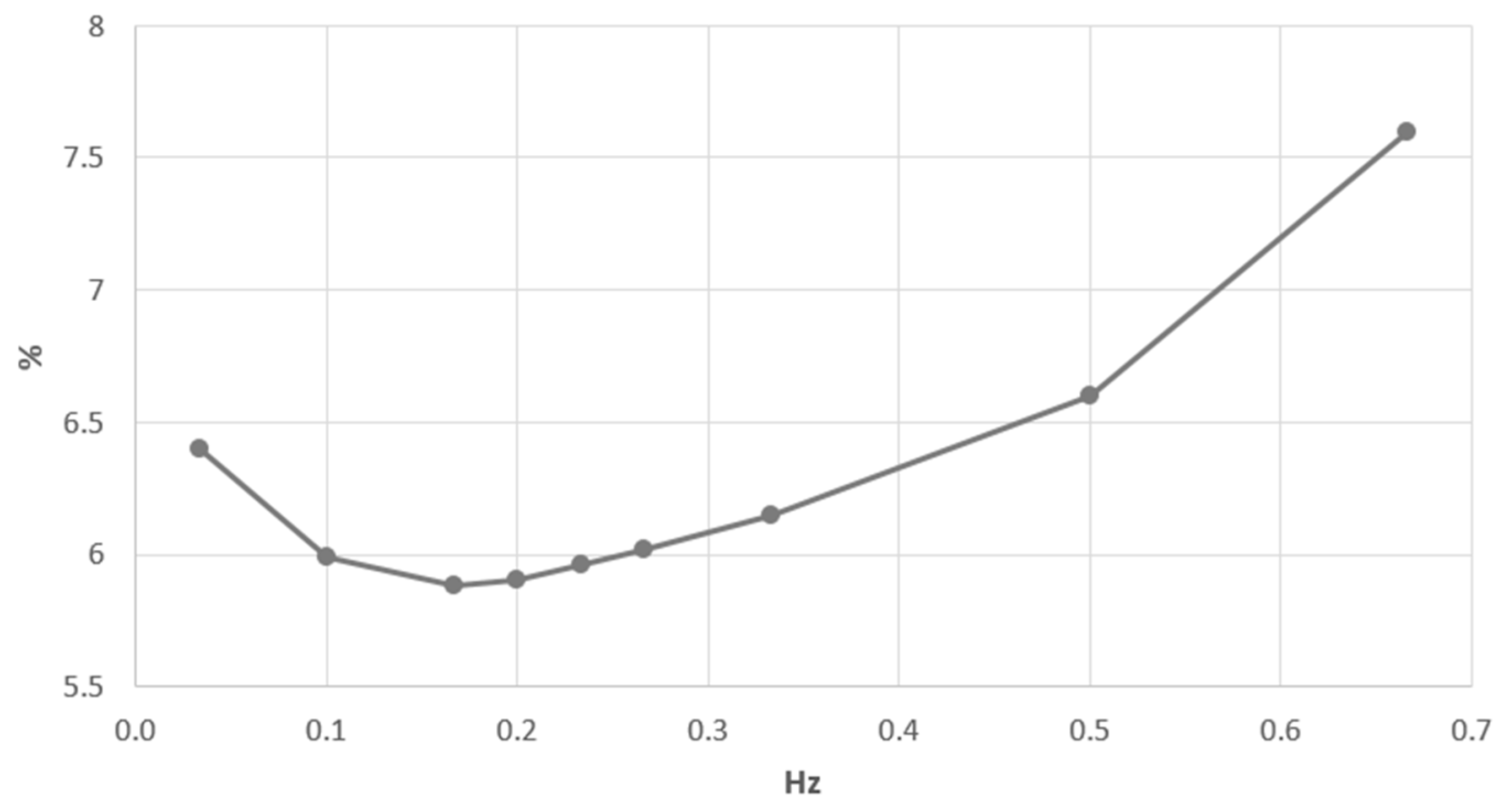
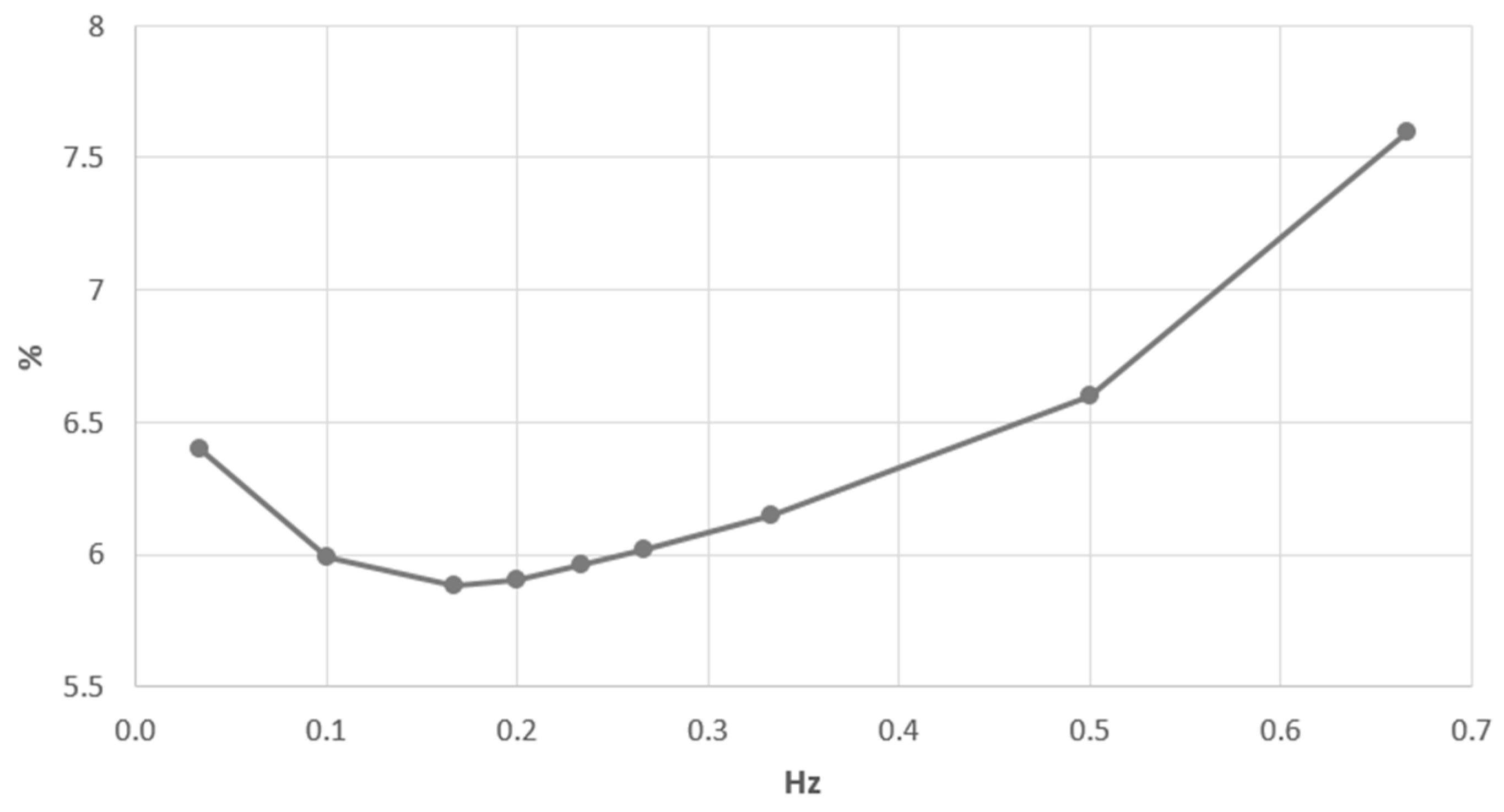
3.2. Carbon Dioxide Elimination Efficiency during Artificial Ventilation
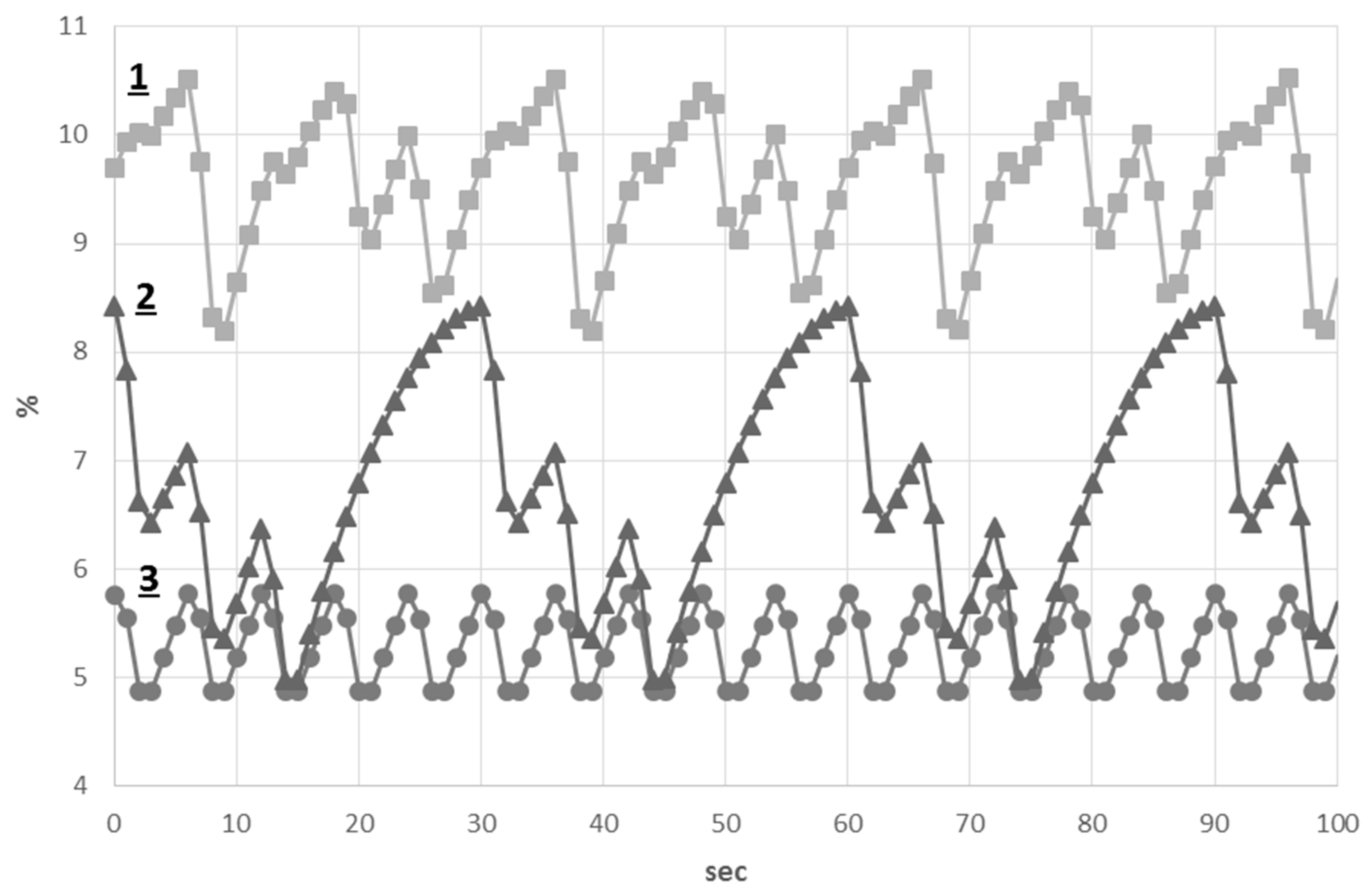
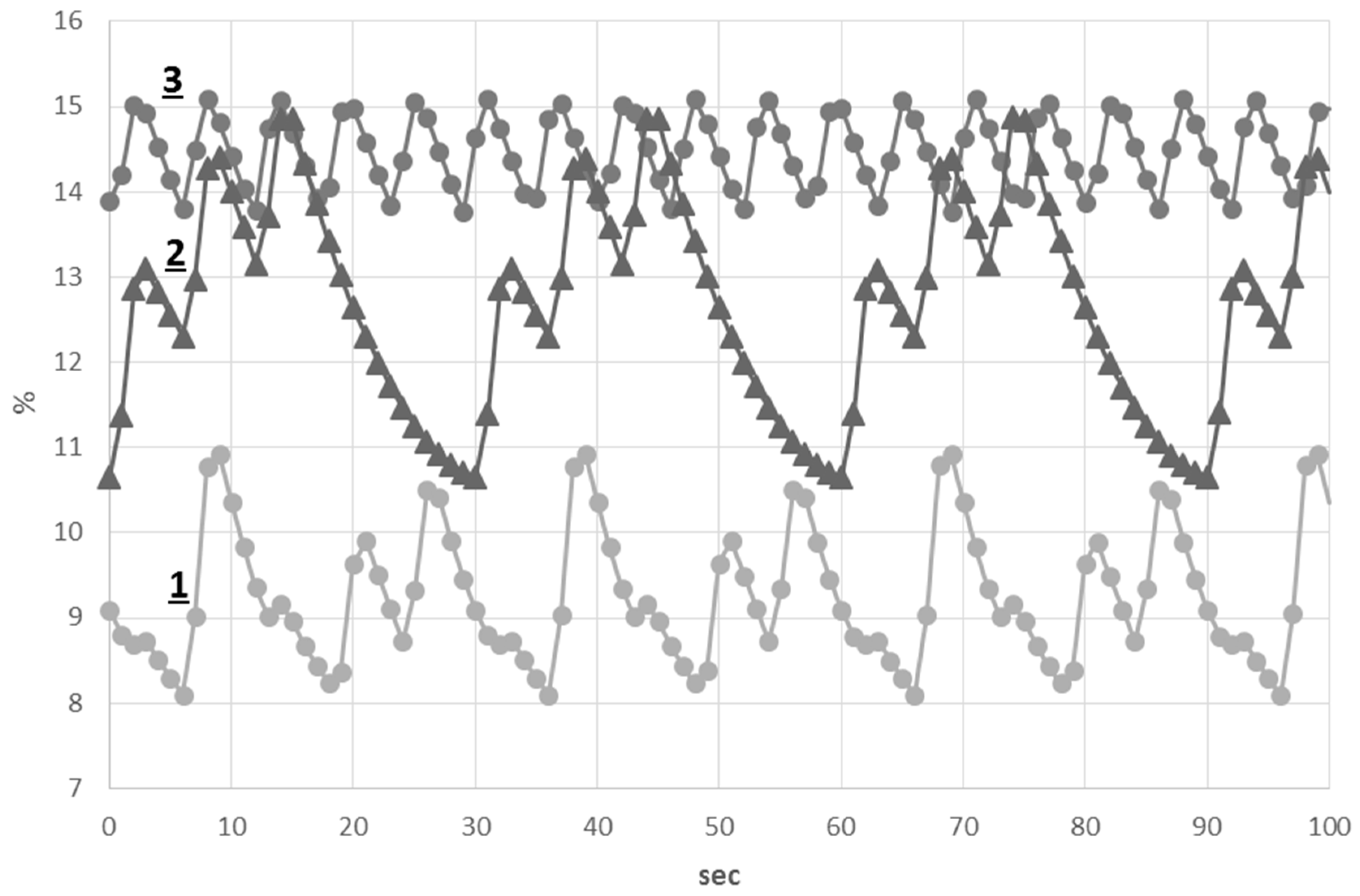
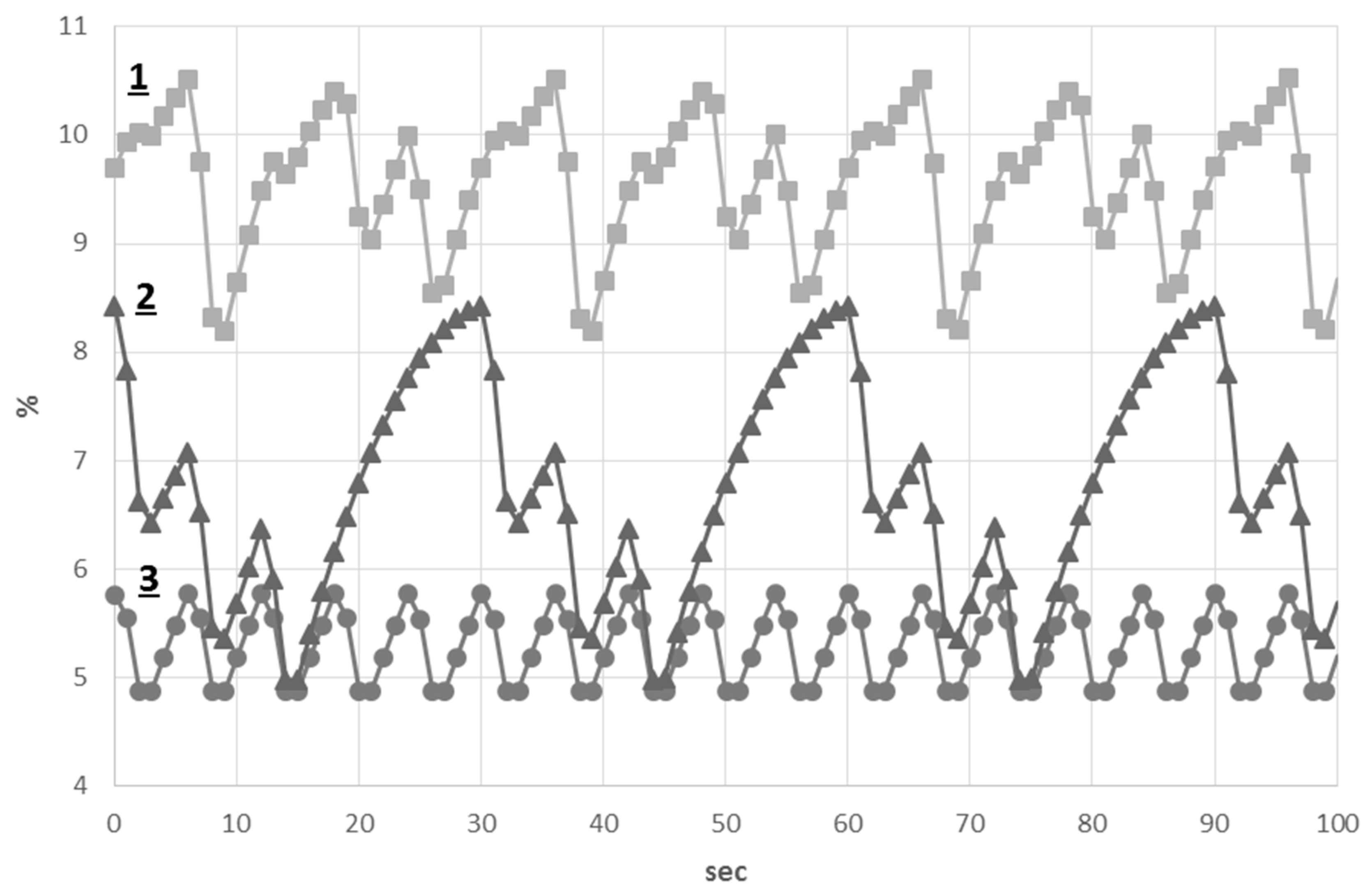
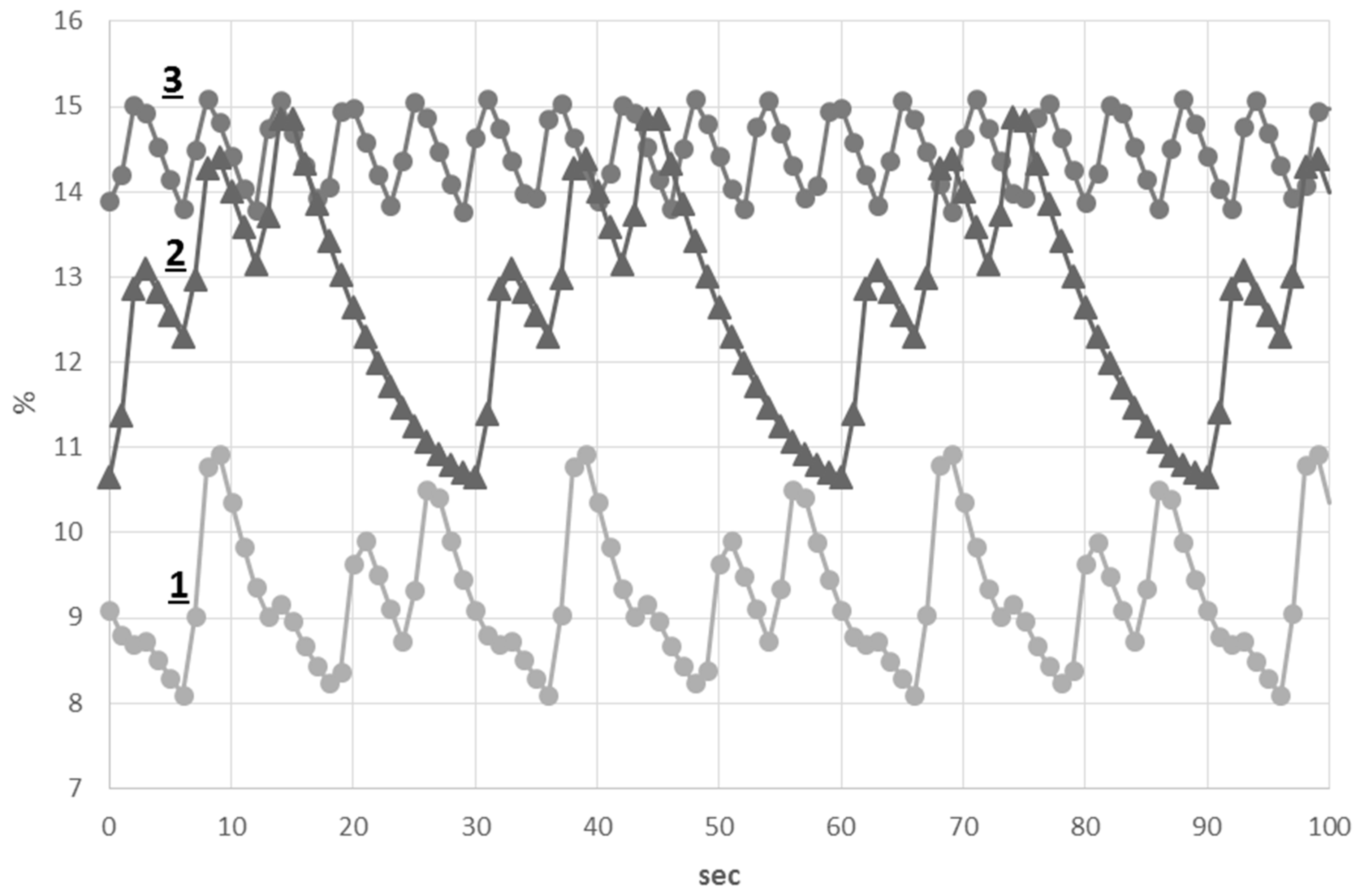
3.3. The Study of Pathological Breathing Patterns
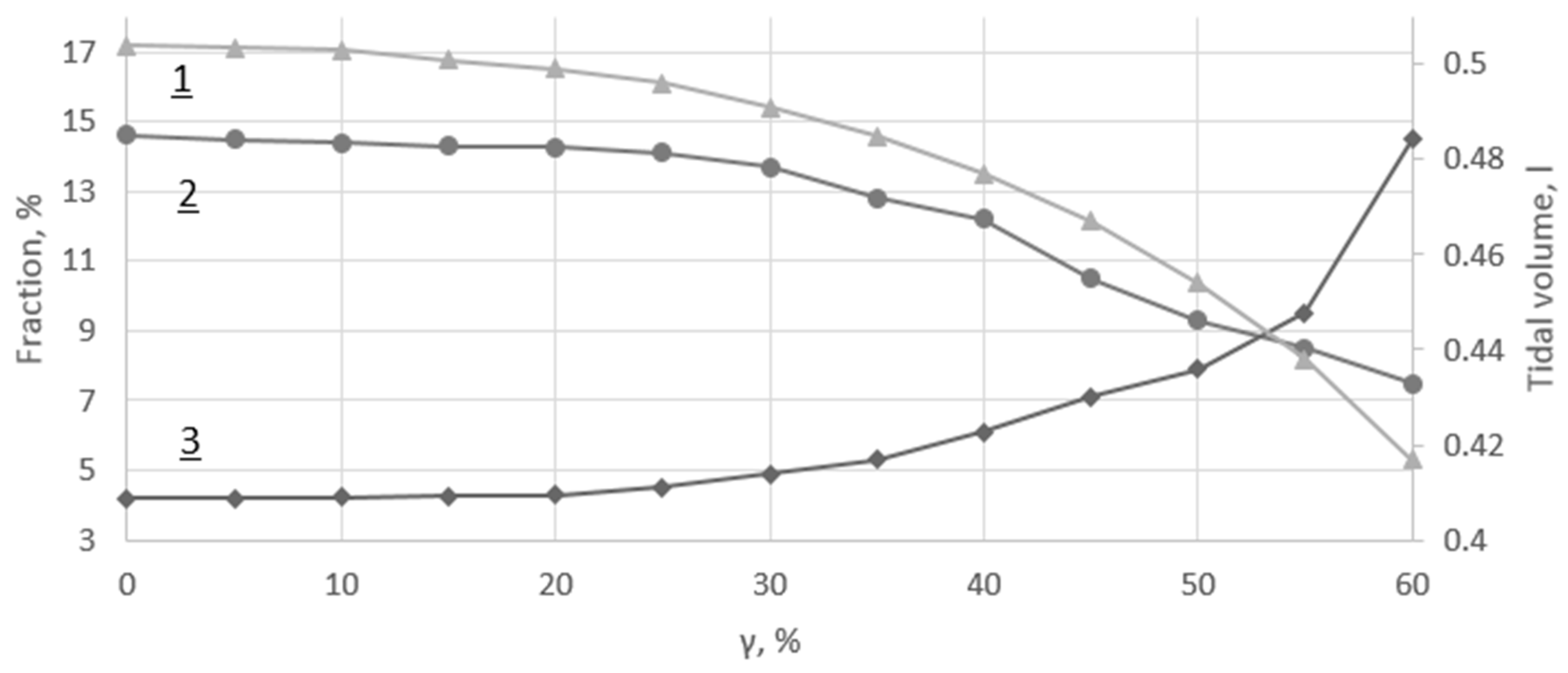
3.4. Asthma Model
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| FSI | Fluid-structure interaction |
| ARR | Artificial respiratory rate |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symbol | Value | Unit |
|---|---|---|
| 1.23 × 10−6 | ||
| 1.8 × 10−3 | ||
| 0.17 | ||
| 0.16 | ||
| 1.2 × 10−3 | ||
| 6.7 × 10−2 | ||
| 0.5 | ||
| 0.16 | ||
| 5 | ||
| 1.3 | ||
| 101.3 | ||
| 4 | ||
| 5 | ||
| 0.25 | ||
| 0.2 | ||
| 0.209 | ||
| 2.8 × 10−4 | ||
| 1 |
| Index | Length, | Diameter, | |
|---|---|---|---|
| 1 | 12.49 | 1.38 | 7700 |
| 2 | 5.41 | 0.87 | 7382 |
| 3 | 2.86 | 1.11 | 7382 |
| 4 | 1.25 | 0.68 | 7064 |
| 5 | 1.63 | 0.66 | 7064 |
| 6 | 2.45 | 0.84 | 7064 |
| 7 | 1.82 | 0.53 | 7064 |
| 8 | 2.32 | 0.25 | 6747 |
| 9 | 1.5 | 0.47 | 6747 |
| 10 | 3.86 | 0.26 | 6747 |
| 11 | 1.02 | 0.43 | 6747 |
| 12 | 2.1 | 0.44 | 6747 |
| 13 | 0.6 | 0.64 | 6747 |
| 14 | 0.54 | 0.4 | 6747 |
| 15 | 1,29 | 0.27 | 6747 |
References
- Agache, I.; Ciobanu, C.; Paul, G.; Rogozea, L. Dysfunctional breathing phenotype in adults with asthma—Incidence and risk factors. Clin. Transl. Allergy 2012, 2, 18. [Google Scholar] [CrossRef] [PubMed]
- Folgering, H. The pathophysiology of hyperventilation disorder. Monalsi. Arch. Chest. Dis. 1999, 54, 365–371. [Google Scholar]
- Howell, J.B. Behavioural breathlessness. Thorax 1990, 45, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Han, J.N.; Stegen, K.; Schepers, R.; Van den Bergh, O.; Woestinjne, K.P. Subjective symptoms and breathing pattern at rest and following hyperventilation in anxiety and somatiform disorders. J. Psychosom. Res. 1998, 45, 519–532. [Google Scholar] [CrossRef]
- Fekr, A.R.; Janidarmian, M.; Radecka, K.; Zilic, Z. A medical cloud-based platform for respiration rate measurement and hierarchical classification of breath disorders. Sensors 2014, 14, 11204–11224. [Google Scholar] [CrossRef] [PubMed]
- Longest, P.W.; Tian, G.; Delvadia, R.; Hindle, M. Development of a stochastic individual path (SIP) model for predicting the deposition of pharmaceutical aerosols: Effects of turbulence, polydisperse aerosol size, and evaluation of multiple lung lobes. Aerosol Sci. Technol. 2012, 46, 1271–1285. [Google Scholar] [CrossRef]
- Comerford, A.; Gravemeier, V.; Wall, W.A. An algebraic variational multiscale-multigrid method for large-eddy simulation of turbulent pulsatile flows in complex geometries with detailed insight into pulmonary airway flow. Int. J. Numer. Meth. Fluids 2013, 71, 1207–1225. [Google Scholar] [CrossRef]
- Tian, G.; Longest, P.W.; Su, G.; Walenga, R.L.; Hindle, M. Development of a Stochastic Individual Path (SIP) Model for Predicting the Tracheobronchial Deposition of Pharmaceutical Aerosols: Effects of Transient Inhalation and Sampling the Airways. J. Aerosol Sci. 2011, 42, 781–799. [Google Scholar] [CrossRef]
- Ismail, M.; Comerford, A.; Wall, W.A. Coupled and reduced dimensional modelling of respiratory mechanics during spontaneous breathing. Int. J. Numer. Meth. Biomed. Eng. 2013, 29, 1285–1305. [Google Scholar] [CrossRef] [PubMed]
- Roth, C.J.; Ismail, M.; Yoshihara, L.; Wall, W.A. A comprehensive computational human lung model incorporating inter-acinar dependencies: Application to spontaneous breathing and mechanical ventilation. Int. J. Numer. Meth. Biomed. Eng. 2017, 33, e02787. [Google Scholar] [CrossRef] [PubMed]
- Tian, G.; Longest, P.W.; Su, G.; Hindle, M. Characterization of Respiratory Drug Delivery with Enhanced Condensational Growth Using an Individual Path Model of the Entire Tracheobronchial Airways. Ann. Biomed. Eng. 2011, 39, 1136–1153. [Google Scholar] [CrossRef] [PubMed]
- Longest, P.W.; Holbrook, L.T. In Silico Models of Aerosol Delivery to the Respiratory tract—Development and Applications. Adv. Drug Deliv. Rev. 2012, 64, 296–311. [Google Scholar] [CrossRef] [PubMed]
- Kleinstreuer, C.; Feng, Y. Lung Deposition Analyses of Inhaled Toxic Aerosols in Conventional and Less Harmful Cigarette Smoke: A Review. Int. J. Environ. Res. Public Health 2013, 10, 4455–4458. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Hu, G.L.; Fan, J.R.; Pan, D. Study on Airflow and Inhaled Particle Deposition within Realistic Human Upper Respiratory Tract. J. Phys. Conf. Ser. 2009, 147, 1–10. [Google Scholar] [CrossRef]
- Tena, A.F.; Casan, P.; Fernandez, J.; Ferrera, C.; Marcos, A. Characterization of particle deposition in a lung model using an individual path. EPJ Web Conf. 2013, 45, 1–5. [Google Scholar] [CrossRef]
- Ilegbusi, O.J.; Li, Z.; Seyfi, B.; Min, Y.; Meeks, S.; Kupelian, P.; Santhanam, A.P. Modeling Airflow Using Subject-Specific 4DCT-Based Deformable Volumetric Lung Models. Int. J. Biomed. Imag. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Crooke, P.S.; Hotchkiss, J.R.; Marint, J.J. Linear and Nonlinear Mathematical Models for Noninvasive Ventilation. Math. Comput. Mod. 2002, 35, 1297–1313. [Google Scholar] [CrossRef]
- Ben-Tal, A. Simplified Models for Gas Exchange in the Human Lungs. J. Theor. Biol. 2006, 238, 474–495. [Google Scholar] [CrossRef] [PubMed]
- Comerford, A.; Förster, C.; Wall, W.A. Structured tree impedance outflow boundary conditions for 3D lung simulations. ASME J. Biomech. Eng. 2010, 132. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-L.; Tawhai, M.H.; McLennan, G.; Hoffman, E.A. Multiscale simulation of gas flow in subjectspecific models of the human lung. IEEE Eng. Med. Biol. 2009, 28, 25–33. [Google Scholar]
- Polak, A.G.; Lutchen, K.R. Computational Model for Forced Expiration from Asymmetric Normal Lungs. Ann. Biomed. Eng. 2003, 31, 891–907. [Google Scholar] [CrossRef] [PubMed]
- Malve, M.; del Palomar, A.P.; Chandra, S.; López-Villalobos, J.L.; Mena, A.; Finol, E.A.; Ginel, A.; Doblaré, M. FSI Analysis of a Healthy and a Stenotic Human Trachea Under Impedance-Based Boundary Conditions. J. Biomech. Eng. 2011, 133, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Brighenti, C.; Gnudi, G.; Avanzolini, G. A simulation model of the oxygen alveolo-capillary exchange in normal and pathological conditions. Physiol. Meas. 2003, 24, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Ermentrout, G.B.; Clermont, G. A mathematical model of pulmonary gas exchange under inflammatory stress. J. Theor. Biol. 2010, 264, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.G.; Riebesell, U.; Rost, B.; Thoms, S.; Zeebe, R.E. Determination of the rate constants for the carbon dioxide to bicarbonate inter-conversion in pH-buffered seawater systems. Mar. Chem. 2006, 100, 53–65. [Google Scholar] [CrossRef]
- Simakov, S.S.; Kholodov, A.S. Computational study of oxygen concentration in human blood under low frequency disturbances. Math. Models Comput. Simul. 2009, 1, 283–295. [Google Scholar] [CrossRef]
- Kholodov, Y.A.; Kholodov, A.S.; Kovshov, N.V.; Simakov, S.S.; Severov, D.S.; Bordonos, A.K.; Bapayev, A. Computational models on graphs for nonlinear hyperbolic and parabolic system of equations. In III European Conference on Computational Mechanics; MotaSoares, C.A., Martins, J.A.C., Rodrigues, H.C., Ambrósio, J.A.C., Pina, C.A.B., Motasoares, C.M., Pereira, E.B.R., Folgado, J., Eds.; Springer: Dordrecht, The Netherlands, 2006; p. 43, CD-ROM ID 2279. [Google Scholar]
- Pedley, T.J.; Luo, X.Y. Modelling Flow and Oscillations in Collapsible Tubes. Theor. Comput. Fluid Dyn. 1998, 10, 277–294. [Google Scholar] [CrossRef]
- Schmidt, R.F.; Thews, G. Human Physiology, 2nd ed.; Springer: Berlin, Germany, 1989; pp. 600–605. [Google Scholar]
- Mead, J. Mechanical properties of lungs. Physiol. Rev. 1961, 41, 281–330. [Google Scholar] [PubMed]
- Hamid, Q.; Shannon, J.; Martin, J. Physiologic Basis of Respiratory Disease; BC Decker Inc.: Hamilton, ON, Canada, 2005. [Google Scholar]
- Magomedov, K.M.; Kholodov, A.S. Grid-Characteristic Numerical Methods; Nauka: Moscow, Russia, 1988. (In Russian) [Google Scholar]
- Kholodov, A.S. Some dynamic models of external breathing and blood circulation with consideration for their coherence and mass transfer. In Computer Models and Medicine Progress; Belotserkovskii, O.M., Kholodov, A.S., Eds.; Nauka: Moscow, Russia, 2001; pp. 127–163. (In Russian) [Google Scholar]
- Simakov, S.S.; Kholodov, A.S.; Kholodov, Y.A.; Nadolskiy, A.A. Computational study of the vibrating disturbances to the lung function. In III European Conference on Computational Mechanics; MotaSoares, C.A., Martins, J.A.C., Rodrigues, H.C., Ambrósio, J.A.C., Pina, C.A.B., Motasoares, C.M., Pereira, E.B.R., Folgado, J., Eds.; Springer: Dordrecht, The Netherlands, 2006; p. 205, CD-ROM, ID 1467. [Google Scholar]
- Vassilevski, Y.; Simakov, S.; Dobroserdova, T.; Salamatova, V. Numerical issues of modelling blood flow in networks of vessels with pathologies. Russ. J. Numer. Anal. Math. Mod. 2011, 26, 605–622. [Google Scholar] [CrossRef]
- Bessonov, N.; Sequeira, A.; Simakov, S.; Vassilevski, Y.; Volpert, V. Methods of Blood Flow Modelling. Math. Mod. Nat. Phenom. 2016, 11, 1–25. [Google Scholar] [CrossRef]
- Danilov, A.; Ivanov, Y.; Pryamonosov, R.; Vassilevski, Y. Methods of graph network reconstruction in personalized medicine. Int. J. Numer. Meth. Biomed. Eng. 2016, 32. [Google Scholar] [CrossRef] [PubMed]
- Pudney, C. Distance-ordered homotopic thinning: A skeletonization algorithm for 3D digital images. Comput. Vis. Image Underst. 1998, 72, 404–413. [Google Scholar] [CrossRef]
- Wijdicks, E.F. Biot’s breathing. J. Neurol. Neurosurg. Psychiatry 2007, 78, 512–513. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.M.S. Cheyne-Stokes respiration. J. Neurol. Neurosurg. Psychiatry 2002, 72, 595. [Google Scholar] [CrossRef]
- Colice, G.L. Categorizing Asthma Severity: An Overview of National Guidelines. Clin. Med. Res. 2004, 2, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.W. Clinical Application of Mechanical Ventilation, 4th ed.; CENGAGE Learning: Boston, MA, USA, 2014; p. 105. [Google Scholar]

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golov, A.; Simakov, S.; Soe, Y.N.; Pryamonosov, R.; Mynbaev, O.; Kholodov, A. Multiscale CT-Based Computational Modeling of Alveolar Gas Exchange during Artificial Lung Ventilation, Cluster (Biot) and Periodic (Cheyne-Stokes) Breathings and Bronchial Asthma Attack. Computation 2017, 5, 11. https://doi.org/10.3390/computation5010011
Golov A, Simakov S, Soe YN, Pryamonosov R, Mynbaev O, Kholodov A. Multiscale CT-Based Computational Modeling of Alveolar Gas Exchange during Artificial Lung Ventilation, Cluster (Biot) and Periodic (Cheyne-Stokes) Breathings and Bronchial Asthma Attack. Computation. 2017; 5(1):11. https://doi.org/10.3390/computation5010011
Chicago/Turabian StyleGolov, Andrey, Sergey Simakov, Yan Naing Soe, Roman Pryamonosov, Ospan Mynbaev, and Alexander Kholodov. 2017. "Multiscale CT-Based Computational Modeling of Alveolar Gas Exchange during Artificial Lung Ventilation, Cluster (Biot) and Periodic (Cheyne-Stokes) Breathings and Bronchial Asthma Attack" Computation 5, no. 1: 11. https://doi.org/10.3390/computation5010011
APA StyleGolov, A., Simakov, S., Soe, Y. N., Pryamonosov, R., Mynbaev, O., & Kholodov, A. (2017). Multiscale CT-Based Computational Modeling of Alveolar Gas Exchange during Artificial Lung Ventilation, Cluster (Biot) and Periodic (Cheyne-Stokes) Breathings and Bronchial Asthma Attack. Computation, 5(1), 11. https://doi.org/10.3390/computation5010011