
Cognitive Hybrid Intelligent Diagnostic System: Typical Architecture


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- To model the image of a diagnostic medical problem;
- To imitate mixed, integrated visual-figurative and verbal-sign representations of the problem by experts;
- To imitate collective restructuring of reduced representation of the problem image according to the principle of consultation using the methods of HISs as decision support diagnostic systems with cognitive visualization of problems arising in medicine.
- The visual metalanguage;
- Representations of the mental image “an integrated method for solving a diagnostic problem” and a heuristic mechanism for solving problems by dynamically restructuring the whole into a decomposition of related problems as well as a language for their description;
- A subject-figurative model of cognitive hybrid intelligent diagnostic systems (CHIDS), their typical architecture, and synthesis algorithm.
2. Literature Review
3. Materials and Methods
- The approach of M.A. Gaides to the system analysis of the human body [22];
- The principle of virtual consultation by S.B. Rumovskaya [17] according to which the virtual team model was developed as a stratified (multilevel) model of a council of highly specialized experts following the works of M. Mesarovich and I. Takahara on the theory of hierarchical multilevel systems [23].
4. The Core Results
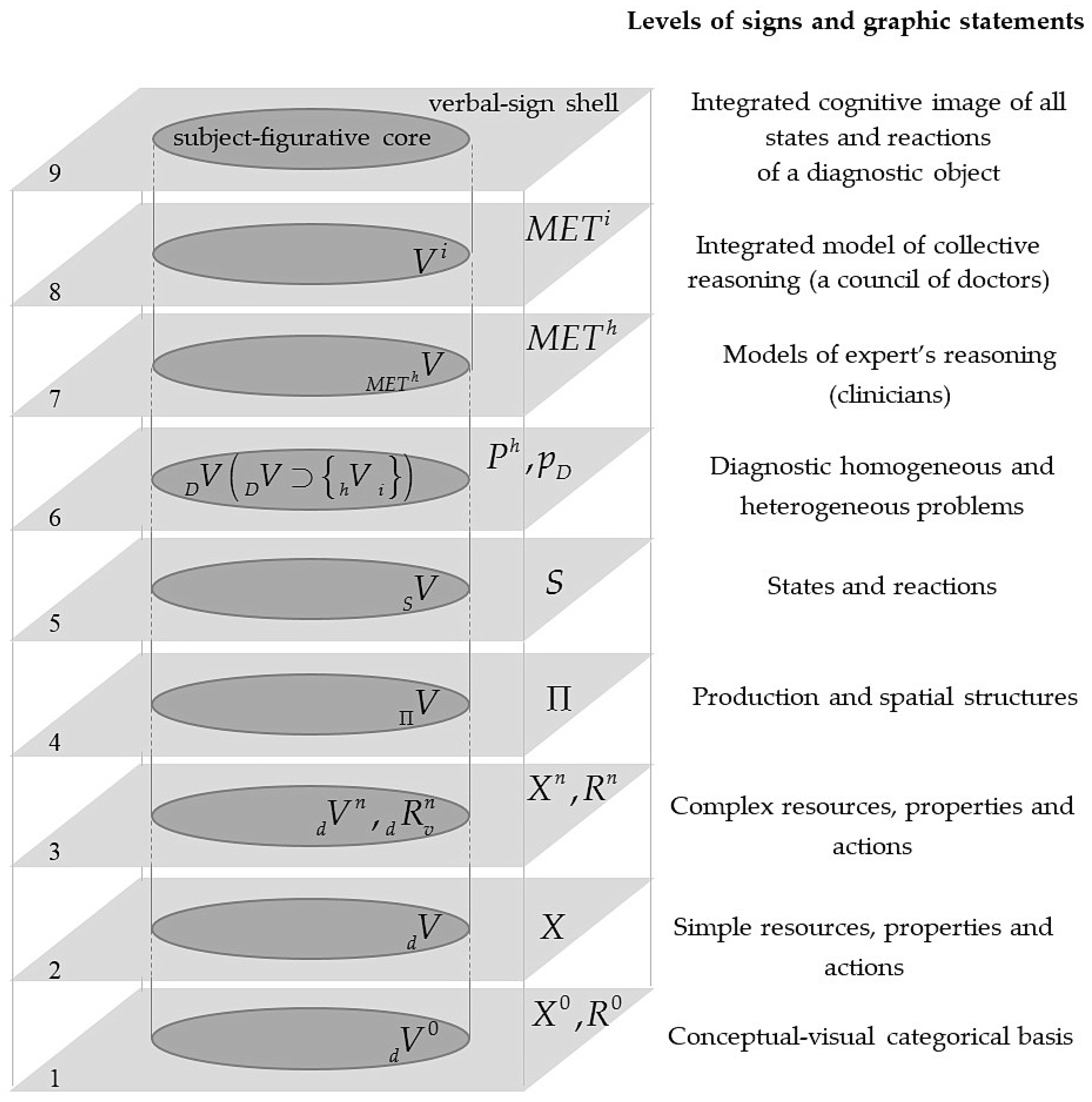
4.1. Metalanguage for Description and Representation of Patient’s States
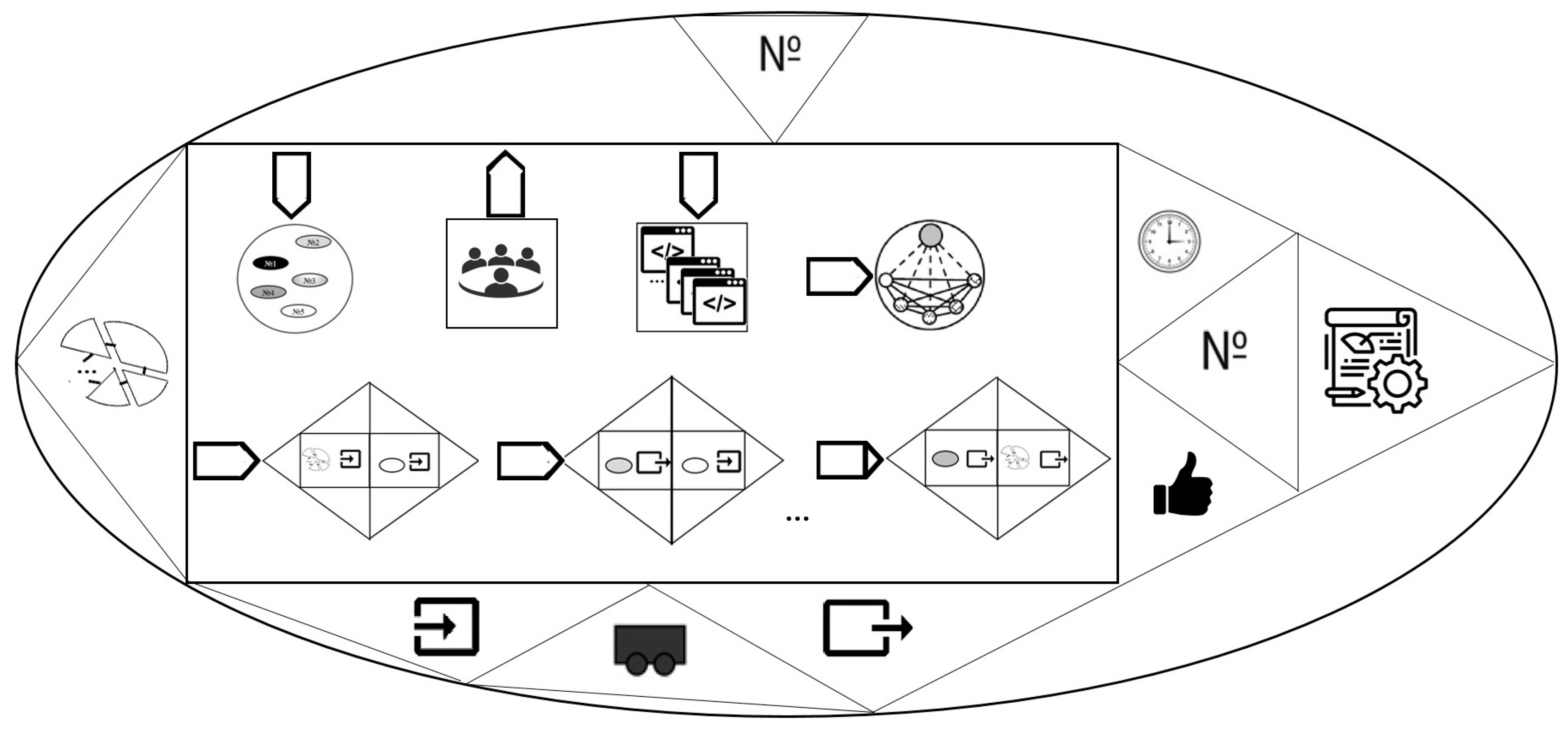
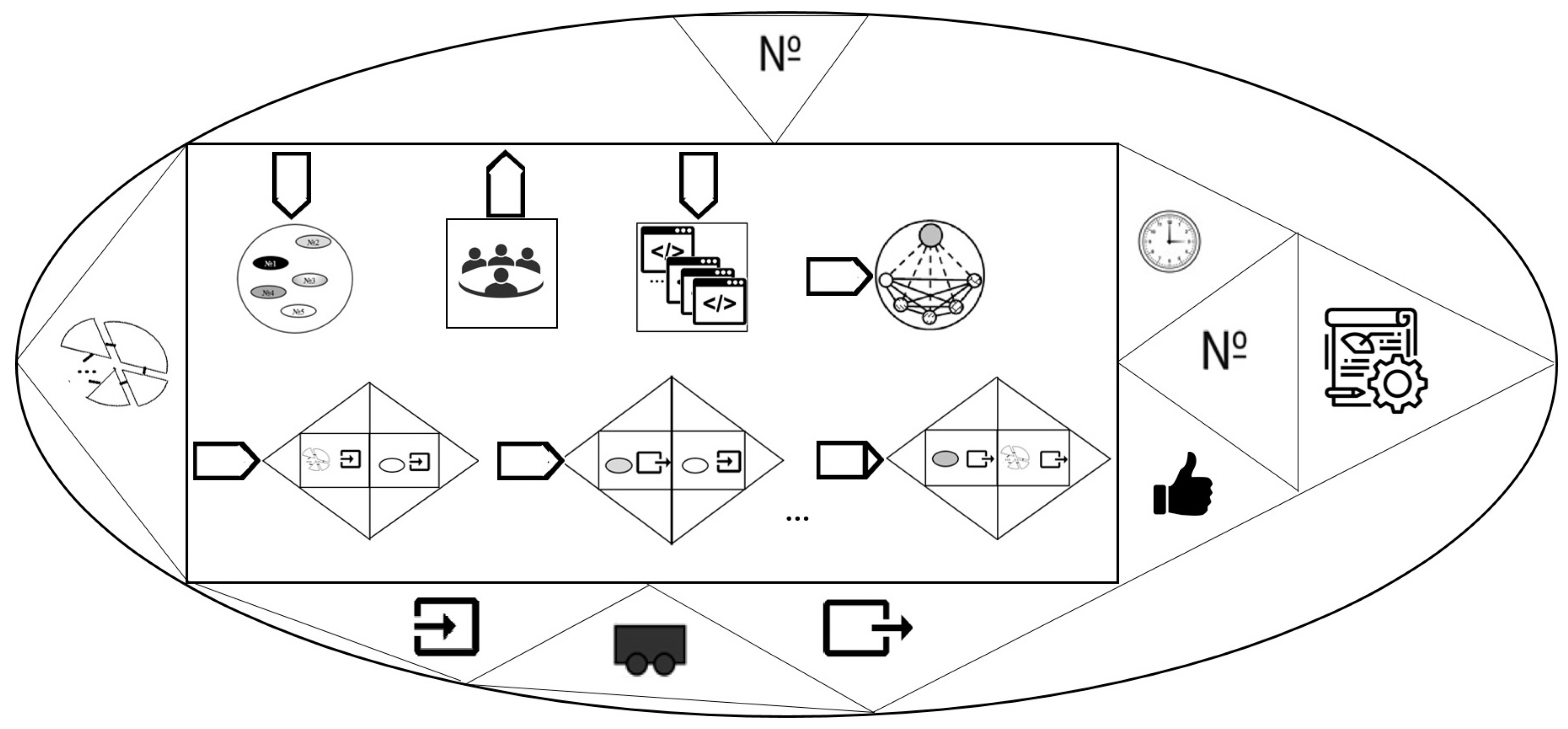
4.2. Subject-Figurative Model of the Functional Hybrid Intelligent Diagnostic System
- “action-object” where the object is HMF;
- “action-subject” where the right role is the resource “team of experts”; “action-object” where the right role of the resource is “a set of programs”;
- “action-result” where the right role is the architecture of the CHIDS that is relevant to the structure of the DP;
- “action-property” performed after a connection between the input of the CHIDS and the input of one of its elements is established. This connection is symbolized by the closed bases of triangles (properties). Each property consists of a role-visual relation “property-resource”: on the left, the “input” property and the resource is CHIDS (rectangle);
- “action-property” (shown at the Figure 2 by ellipsis which number is equal to the HMF dimension) which is performed after a connection between the output of one element of the CHIDS and the input of another is established. Each property is in a role-visual relation “property-resource”: on the left-the “output” property and the resource-element. The similar right one visualizes the statement “the input of the CHIDS element”;
- “action-property” which is performed after the connection between the output of the CHIDS element and its output is established. Each property consists of a role-based visual relation “property-resource”: on the left, the “output” property and the resource (an element). The similar right one visualizes the statement “CHIDS exit”.
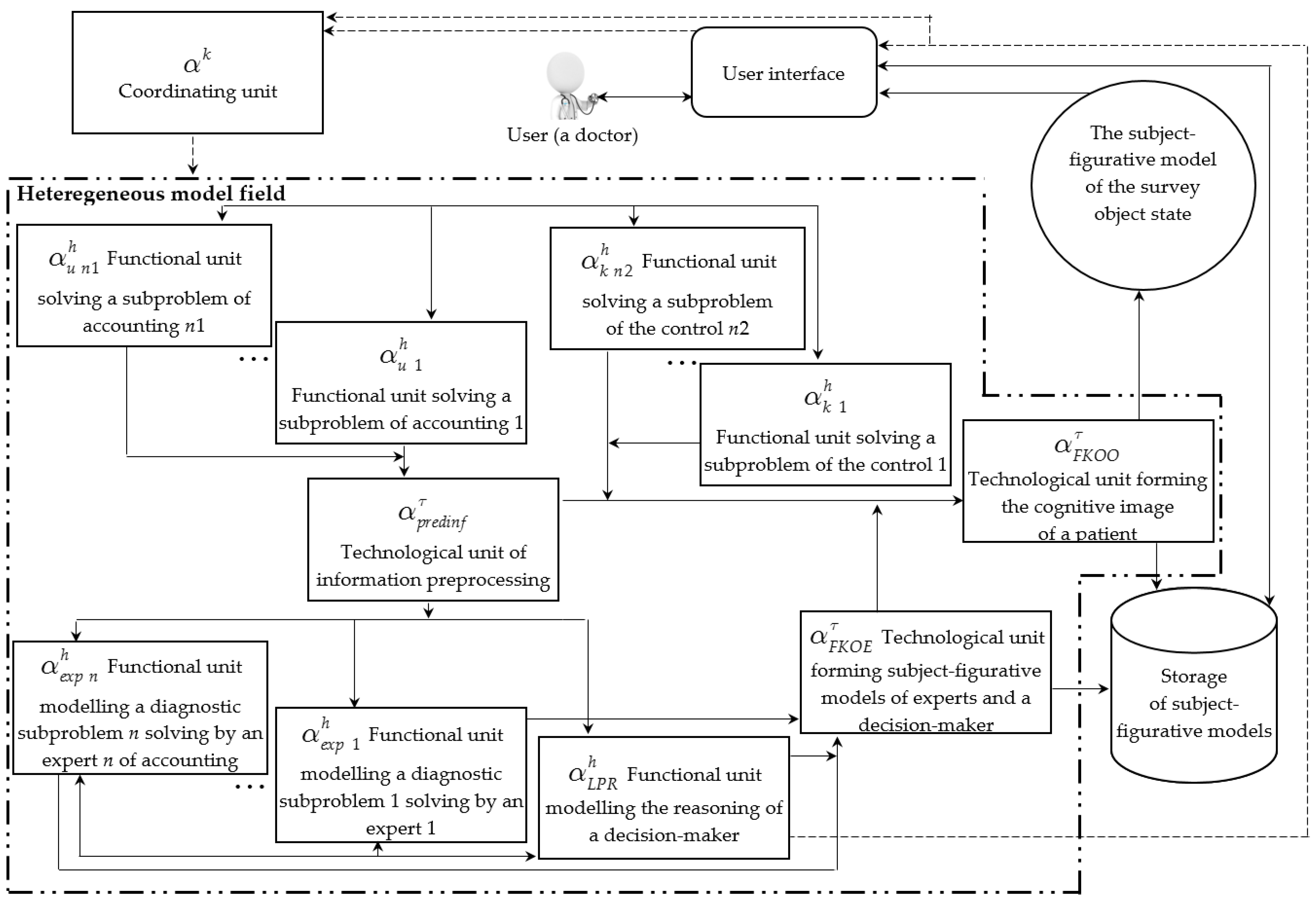
4.3. Typical Architecture of the Cognitive Hybrid Intelligent Diagnostic System
- user interface;
- functional elements (FE) that solve a set of subproblems of accounting and control as well as diagnostic subproblems solved by experts and the decision-maker;
- technological elements that solve the subproblem of information preprocessing and the problem of forming cognitive images of experts, decision-maker and the diagnostic object;
- the storage of subject-figurative models.
4.4. Cognitive Hybrid Intelligent Diagnostic System Synthesis: The Algorithm
- A decomposition of the DP in the view of oriented graph. Nodes are , —homogeneous subproblems (functional and technological) and edges are for —relations over HMF;
- HMF Ma and a set of one-to-one correspondence where is a set of correspondence relations between goals and input data of subproblems from the decomposition of the DP and goals and input data of the DP;
- A set of interpreters Ia of autonomous models and inter-model interfaces ;
- Correspondences of and interpreters where a—analytical methods, s—statistical, e—expert systems, f—fuzzy systems, n—neural networks, g—genetic algorithms, p—CBR-systems;
- A set of valid states for each model and the order over the – where and —inferior indexes of subproblems from .
- The beginning, l = 1;
- Choose from the decomposition of in which each has the priority from Inl;
- j = 1, El =;
- Choose the next j-th pare from ;
- Initialize the matrix for j-th pair: the columns are models solving subproblem , and rows are models in the state solving subproblem .
- Supplement the by the matrix ;
- ? If NO then j = j + 1 and go to the item 4;
- j = 1;
- Choose from El. Only those elements are activated for which integration relations are specified between models. Using an expert system, the models are evaluated. Estimations of are entered in the denominators, and estimations of —in the numerators of the elements. For the initial states of the models, select a pair of models with the maximum value of the integrated estimation and add it to the LsD;
- ? If NO then j = j + 1 and go to the item 9;
- l = NT? If NO then l = l + 1 and go to the item 2, otherwise supplement LsD with interpreters and interfaces and form a knowledge base of a functional element that models the decision of the decision-maker subproblem from matrices E, so that it can rebuild the integrated model of the CHIDS depending on the situation and combine both symbolic reasoning and visual.
5. Discussion
- Immanuel Kant Baltic Federal University, Kaliningrad (hybrid computational intelligence methods [45]);
- Rostov State Transport University, Rostov-on-Don (hybrid intelligent systems [46]);
- Lipetsk State Technical University, Lipetsk (hybrid intelligent information systems for natural language text processing [47]);
- Belarusian State University of Informatics and Radioelectronics, Minsk, Belarus (hybrid semantically compatible intelligent systems [48]);
- University of Electronic Science and Technology of China, Chengdu, China (hybrid intelligent systems for diagnosing cardiovascular diseases [49]), et al.
6. Conclusions
- Reduction of a problem according to the method and general scheme of the representation of the diagnostic problem decomposition proposed in the [29];
- Developing of the heterogeneous model field on the basis of the obtained decomposition. Every model of the field will be built by means of a certain method of artificial intelligence depending on the type of used calculations. The limit of the study regarding types of calculations: neuro-, fuzzy, reasoning based on experience, analytical, evolutionary, statistical, and logical reasoning;
- Synthesizing of the integrated model by the proposed in the manuscript algorithm. It would have to be rebuilt over the heterogeneous model field depending on the input information about the object every time the object is being diagnosed;
- Initialization of the Cognitive Hybrid Intelligent Diagnostic System for the pancreas;
- Laboratory research of the system and interpretation of the results according to which we could have to return back at the step of “Development of the heterogeneous model field” for revision of models.
Funding
Data Availability Statement
Conflicts of Interest
References
- Fominykh, I.B. Image engineering, creative tasks, emotional assessments. Ontol. Des. 2018, 8, 175–189. [Google Scholar] [CrossRef]
- Hachumov, V.M.; Vinogradov, A.N. The development of new methods for identification and predicting of the state of dynamical objects on bases of intellectual data. Matematicheskie metody raspoznavaniya obrazov. In Proceedings of the 13th National Conference Related to 15th Anniversary of RFBR “the Mathematical Methods of Recognition”, Zelenogorsk, Russia, 30 Septempber–6 October 2007; pp. 548–550. [Google Scholar]
- Kobrinskiy, B.A. The significance of visual-image presentations for medical intelligent systems. Sci. Tech. Inf. Process. 2013, 40, 337–341. [Google Scholar] [CrossRef]
- Kobrinsky, B.A. Subjectivity and objectivity in the world of medicine: A view from the position of knowledge representation for a hybrid intelligent system. In Proceedings of the Collection of Scientific Papers of the X-th International Scientific and Technical Conference “Integrated Models and Soft Computing in Artificial Intelligence” (IMMV-2021) in 2 Volumes, Kolomna, Russia, 17–20 May 2021; Volume 1, pp. 56–67. [Google Scholar]
- Vardell, E.; Bou-Crick, C. VisualDx: A Visual Diagnostic Decision Support Tool. Med. Ref. Serv. Q. 2012, 31, 414–424. [Google Scholar] [CrossRef] [PubMed]
- The Trend of Software in the Area of Visualization of Data for Business-Users. Available online: http://iso.ru/ru/press-center/journal/1831.phtml (accessed on 1 February 2022).
- Plaisant, C.; Mushlin, R.; Snyder, A.; Li, J.; Heller, D.; Shneiderman, B. LifeLines: Using Visualization to Enhance Navigation and Analysis of Patient Records. In Proceedings of the American Medical Informatic Association Annual Fall Symposium AMIA, Lake Buena Vista, FL, USA, 7–11 November 1998; pp. 76–80. [Google Scholar]
- Wang, T. Interactive Visualization Techniques for Searching Temporal Categorical Data. Ph.D. Dissertation, University of Maryland, University Park, MD, USA, 2010; p. 260. [Google Scholar]
- Zhang, Z.; Ahmed, F.; Mittal, A.; Ramakrishnan, A.; Zhao, R.; Viccellio, A.; Mueller, K. AnamneVis: A Framework for the Visualization of Patient History and Medical Diagnostics Chains. In Proceedings of the 23rd IEEE VAHC Workshop, Providence, RI, USA, 24 October 2011; pp. 71–72. Available online: https://visualanalyticshealthcare.org/docs/VAHC2011-Proceedings-LowRes.pdf (accessed on 8 February 2022).
- Comby, C.; Keravnou-Papailiou, E.; Shahar, Y. Temporal Information Systems in Medicine; Springer: New York, NY, USA, 2010; p. 378. [Google Scholar]
- Navarrete-Welton, A.; Hashimoto, D. Current applications of artificial intelligence for intraoperative decision support in surgery. Front. Med. 2020, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ban, Y.; Rosman, G.; Ward, T.; Hashimoto, D.; Kondo, T.; Meireles, O.; Rus, D. Aggregating Long-Term Context Learning Surgical Workflows. arXiv 2020, arXiv:2009.00681. Available online: https://arxiv.org/pdf/2009.00681v4.pdf (accessed on 23 March 2022).
- Shinozuka, K.I.; Turuda, S.; Fujinaga, A.; Nakanuma, H.; Kawamura, M.; Matsunobu, Y.; Tanaka, Y.; Kamiyama, T.; Ebe, K.; Tokuyasu, T.; et al. Artificial intelligence software available for medical devices: Surgical phase recognition in laparoscopic cholecystectomy. Surg. Endosc. 2022. Available online: https://link.springer.com/content/pdf/10.1007/s00464-022-09160-7.pdf (accessed on 23 February 2022). [CrossRef] [PubMed]
- Hashimoto, D.; Rosman, G.; Rus, D.; Meireles, O. Artificial Intelligence in Surgery: Promises and Perils. Ann. Surg. 2018, 268, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Samsonova, M.V.; Efimov, V.V. Technology and Methods of Collective Problem Solving: Textbook; UlGTU: Ulyanovsk, Russia, 2003; p. 152. [Google Scholar]
- Spiridonov, V.F. Psychology of Thinking: Solving Tasks and Problems, 2nd ed.; corrected and add; Urait Ed.: Moscow, Russia, 2019; p. 324. [Google Scholar]
- Rumovskaya, S.B. The Research of Methods of Collective Diagnostic Decision Support and Development of Instruments of the “Virtual Council” (Illustrated with the Diagnostic of Arterial Hypertension). Ph.D. Thesis, Institute for Systems Analysis of the Federal Research Center “Computer Science and Control” of Russian Academy of Sciences, Moscow, Russia, 2017; p. 138. [Google Scholar]
- Kolesnikov, A.V. Hybrid Intelligent Systems. Theory and Technology of Development; Yashin, A.M., Ed.; Publishing House of St. Petersburg State Technical University: St. Petersburg, Russia, 2001; p. 711. [Google Scholar]
- Uyomov, A.I. Things, Properties, Relations; Book on Demand: Moscow, Russia, 2013; p. 184. [Google Scholar]
- Nazarenko, G.I.; Osipov, G.S. Fundamentals of Medical Technological Processes. Part 1; PHYSMATHLIT: Moscow, Russia, 2005; p. 144. [Google Scholar]
- Grigoriev, O.G.; Kobrinskii, B.A.; Osipov, G.S.; Molodchenkov, A.I.; Smirnov, I.V. Health management system knowledge base for formation and support of a preventive measures plan. Procedia Computer Science. In Proceedings of the 9th Annual International Conference on Biologically Inspired Cognitive Architectures BICA-2018, Prague, Czech Republic, 22–24 August 2018; pp. 238–241. [Google Scholar]
- Gaydes, M.A. General Systems Theory. Anthropological cosmoconception. In System Analysis of the Origin and Evolution of the Universe. Book 1; SUPER Publishing House: St. Petersburg, Russia, 2020; p. 435. [Google Scholar]
- Mesarovic, M.; Mako, D.; Takahara, I. Theory of Hierarchical Multilevel Systems; Publishing House “Mir”: Moscow, Russia, 1973; p. 344. [Google Scholar]
- Pospelov, D.A.; Pushkin, V.N. Thinking and Automata; Publishing House “Soviet Radio”: Moscow, Russia, 1972; p. 224. [Google Scholar]
- Oshanin, D.A. Subject Action and Operational Image: Selected Psychological Works; Moscow Psychological and Social Institute, MODEK: Moscow, Russia, 1999; p. 512. [Google Scholar]
- Lindenbraten, L.D. Methodology for the Study of X-rays: 2nd Revised. and Ext. Ed.; Publishing House “Medicine”: Moscow, Russia, 1971; p. 338. [Google Scholar]
- Kolesnikov, A.V.; Kirikov, I.A. Methodology and Technology for Solving of Complex Problems Using the Methodology of Functional Hybrid Artificial Systems; IPI RAS: Moscow, Russia, 2007; p. 387. [Google Scholar]
- Kolesnikov, A.; Jasinski, E.; Rumovskaya, S. Predicative representations of relations and links of the intellectual operational—technological control in complex dynamic systems. In Proceedings of the Research Papers Collection of the Open Semantic Technologies for Intelligent Systems, Minsk, Belarus, 18–22 February 2020; Volume 4, pp. 43–50. [Google Scholar]
- Rumovskaya, S. Representation of the Mechanism for Constructing an Integrated Method of Solving a Diagnostic Problem and Results of Its Work. In Proceedings of the 3rd International Conference on Control Systems, Mathematical Modeling, Automation and Energy Efficiency SUMMA-2021, Lipetsk, Russia, 10–12 November 2021; pp. 798–804. [Google Scholar] [CrossRef]
- Rumovskaya, S.B.; Kolesnikov, A.V.; Litvin, A.A. Representation of methods for solving subtasks of different types from the decomposition of a diagnostic problem. IKBFU’s Vestn. Phys. Math. Technol. 2020, 2, 62–73. [Google Scholar]
- Gelfandbein, Y.A.; Kolesnikov, A.V.; Rudinsky, I.D. Hybrid Modeling of a Transport Node and Its Application in Decision-Making Procedures; Riga Polytechnic Institute: Riga, Latvia, 1984; pp. 93–100. [Google Scholar]
- Borisov, A.N. Principles of construction and implementation of hybrid expert systems. In Proceedings of the A Short-Term Scientific and Technical Seminar “Hybrid Expert Systems in the Tasks of Designing Complex Technical Objects”, Saint Petersburg, Russia, 24–25 June 1992; pp. 6–9. [Google Scholar]
- Rybina, G.V. Integrated expert systems: State of the art, problems and trends. Izv. RAS. Theory Control Syst. 2002, 5, 111–126. [Google Scholar]
- Medsker, L.R. Hybrid Intelligent Systems; Kluwer Academic Publishers: Boston, MA, USA, 1995; p. 298. [Google Scholar]
- Goonatilake, S.; Khebbal, S. Intelligent Hybrid Systems. In Proceedings of the First Singapore Int. Conference on Intelligent Systems, 28 September–1 October 1992; pp. 356–364. [Google Scholar]
- Kasabov, N.; Kozma, R. Hybrid Intelligent Adaptive Systems: A Framework and a Case Study on Speech Recognition. Intell. Syst. 1998, 13, 455–466. [Google Scholar] [CrossRef] [Green Version]
- Osipov, G.S. Dynamics in systems based on knowledge. Izv. RAN. Theory Control Syst. 1998, 5, 24–28. [Google Scholar]
- Vagin, V.N.; Eremeev, A.P. Implementation of the concept of distributed AI and multi-agent in decision support systems based on the G2 + GDA complex. In Proceedings of the International Seminar “Distributed Artificial Intelligence and Multi-Agent Systems” DIAMAS’ 97, St. Petersburg, Russia, 15–18 June 1997; pp. 262–264. [Google Scholar]
- Kolesnikov, A.V.; Soldatov, S.A. Coordination algorithm for a hybrid intelligent system for solving a complex problem of operational and production planning. Sci. J. Inform. Appl. 2010, 4, 58–64. [Google Scholar]
- Kolesnikov, A.V.; Kirikov, I.A.; Listopad, S.V.; Rumovskaya, S.B.; Domanitsky, A.A. Solving Complex Traveling Salesman Problems Using Functional Hybrid Intelligent Systems; Kolesnikov, A.V., Ed.; IPI RAS: Moscow, Russia, 2011; p. 295. [Google Scholar]
- Rumovskaya, S.B.; Kolesnikov, A.V.; Kirikov, I.A. Modeling of collective decisions by the virtual council. Sci. Tech. Inf. Process. 2019, 46, 356–365. [Google Scholar] [CrossRef]
- Kolesnikov, A.V.; Listopad, S.V.; Maitakov, F.G. Conceptual-Visual Metalanguage of Hybrid Intelligent Systems. In Proceedings of the II International Scientific and Practical Conference “Fuzzy Technologies in the Industry—FTI 2018”, Ulianovsk, Russia, 23–25 October 2018; pp. 305–313. Available online: http://ceur-ws.org/Vol-2258/paper36.pdf (accessed on 8 February 2022).
- Haq, A.U.; Li, J.P.; Memon, M.H.; Nazir, S.; Sun, R. A Hybrid Intelligent System Framework for the Prediction of Heart Disease Using Machine Learning Algorithms. Mob. Inf. Syst. 2018, 8, 1–21. [Google Scholar] [CrossRef]
- Taran, M.O.; Gapanyuk, Y.E. Architecture of a hybrid intelligent information system for the analysis of judicial arbitration practice. Leg. Inform. 2020, 1, 15–25. [Google Scholar]
- Berezkin, D.V.; Terekhov, V.I.; Chernenkiy, I.M. Methods of hybrid artificial intelligence in the problems of processing, analysis and visualization of big data flows. In Proceedings of the IV All-Russian Pospelov Conference with International Participation “Hybrid and Synergistic Intelligent Systems”, Svetlogorsk, Russia, 14–19 May 2018; pp. 155–160. [Google Scholar]
- Klachek, P.M.; Polupan, K.L.; Koryagin, S.I.; Liberman, I.V. Hybrid Computational Intelligence. Fundamentals of Theory and Technology for Creating Applied Systems; IKBFU Publishing House: Kaliningrad, Russia, 2018; p. 118. [Google Scholar]
- Dolgiy, A.I.; Kolodenkova, A.E.; Kovalev, S.M. Problems and methods of merging heterogeneous data in hybrid intelligent systems. In Proceedings of the IV All-Russian Pospelov Conference with International Participation “Hybrid and Synergistic Intelligent Systems”, Svetlogorsk, Russia, 14–19 May 2018; pp. 181–187. [Google Scholar]
- Blyumin, S.L.; Pogodaev, A.K.; Prinkov, A.S.; Khabibullina, E.L. Processing and classification of text in natural language using hybrid intelligent information systems. In Proceedings of the IV All-Russian Pospelov Conference with International Participation “Hybrid and Synergistic Intelligent Systems”, Svetlogorsk, Russia, 14–19 May 2018; pp. 167–176. [Google Scholar]
- Golenkov, V.V.; Gulyakina, N.A.; Davydenko, I.T.; Shunkevich, D.V.; Eremeev, A.P. Ontological design of hybrid semantically compatible intelligent systems based on the semantic representation of knowledge. Ontol. Des. 2019, 9, 132–151. [Google Scholar] [CrossRef]
- Guidelines for Comparing the Final Clinical and Pathoanatomical Forensic Diagnoses; Russian Society of Pathologists, Association of Forensic Experts, 2019. Available online: http://www.patolog.ru/sites/default/files/metod.rekom._mz_rf_sopostavl.ds__0.pdf (accessed on 23 March 2022).
- Sowa, J.F. Conceptual Structures—Information Processing in Mind and Machine; The Systems Programming Series; Addison-Wesley Longman Publishing Co. Inc.: Boston, MA, USA, 1984; p. 481. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rumovskaya, S. Cognitive Hybrid Intelligent Diagnostic System: Typical Architecture. Computation 2022, 10, 66. https://doi.org/10.3390/computation10050066
Rumovskaya S. Cognitive Hybrid Intelligent Diagnostic System: Typical Architecture. Computation. 2022; 10(5):66. https://doi.org/10.3390/computation10050066
Chicago/Turabian StyleRumovskaya, Sophiya. 2022. "Cognitive Hybrid Intelligent Diagnostic System: Typical Architecture" Computation 10, no. 5: 66. https://doi.org/10.3390/computation10050066
APA StyleRumovskaya, S. (2022). Cognitive Hybrid Intelligent Diagnostic System: Typical Architecture. Computation, 10(5), 66. https://doi.org/10.3390/computation10050066