

Performance of Commercial Deep Learning-Based Auto-Segmentation Software for Prostate Cancer Radiation Therapy Planning: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
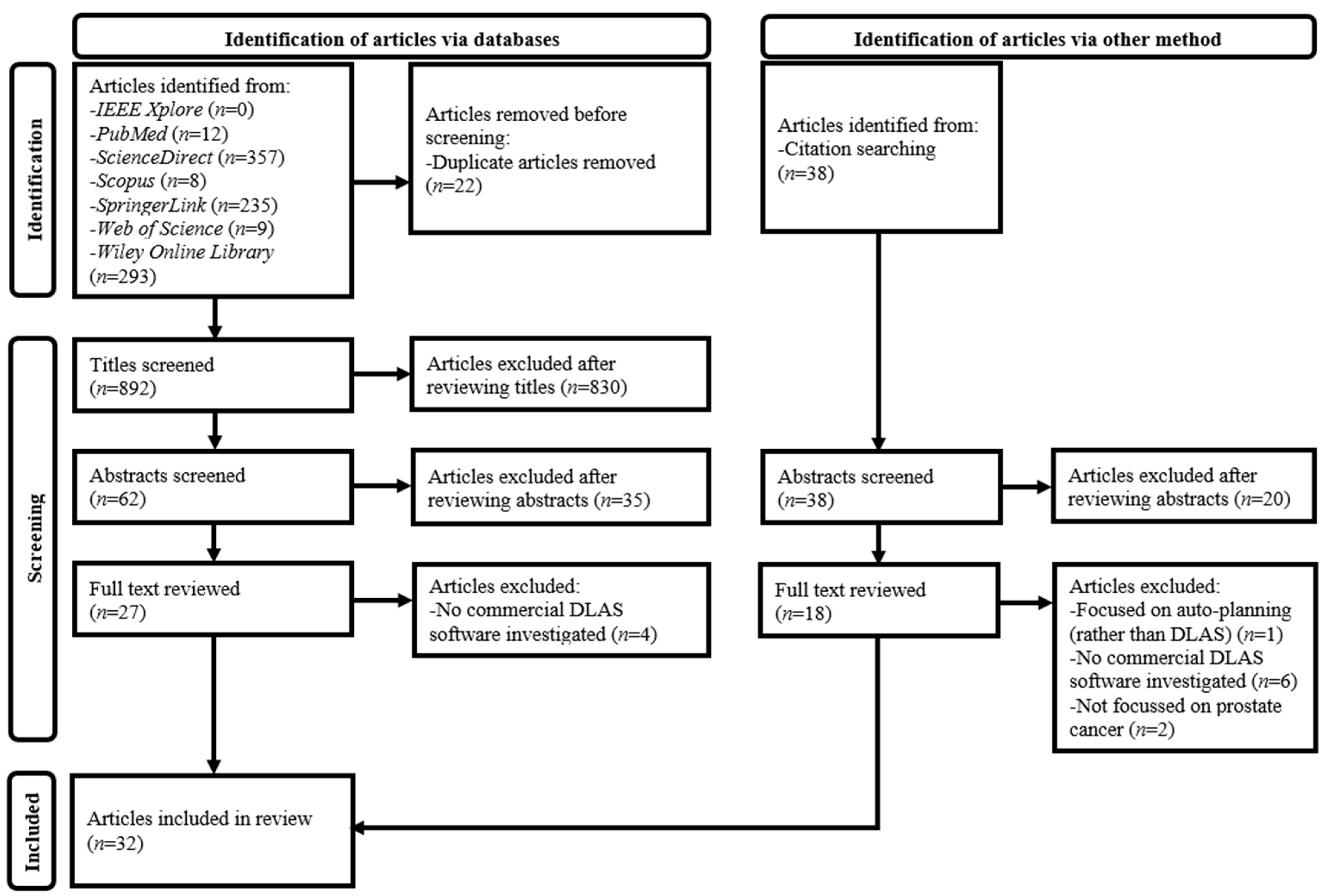
2.1. Literature Search
2.2. Article Selection
2.3. Data Extraction and Synthesis
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prostate Cancer Statistics. Available online: https://www.wcrf.org/preventing-cancer/cancer-statistics/prostate-cancer-statistics/ (accessed on 15 January 2025).
- Cancer in Men: Prostate Cancer is #1 for 118 Countries Globally. Available online: https://www.cancer.org/research/acs-research-news/prostate-cancer-is-number-1-for-118-countries-worldwide.html (accessed on 15 January 2025).
- Prostate Cancer: 3. Epidemiology and Aetiology. Available online: https://uroweb.org/guidelines/prostate-cancer/chapter/epidemiology-and-aetiology (accessed on 15 January 2025).
- Wasim, S.; Park, J.; Nam, S.; Kim, J. Review of current treatment intensification strategies for prostate cancer patients. Cancers 2023, 15, 5615. [Google Scholar] [CrossRef] [PubMed]
- Hekman, L.; Barrett, A.; Ross, D.; Palaganas, E.; Giridhar, P.; Elumalai, T.; Pragathee, V.; Block, A.M.; Welsh, J.S.; Harkenrider, M.M.; et al. A systematic review of clinical trials comparing radiation therapy versus radical prostatectomy in prostate cancer. Clin. Genitourin. Cancer 2024, 22, 102157. [Google Scholar] [CrossRef] [PubMed]
- Numakura, K.; Kobayashi, M.; Muto, Y.; Sato, H.; Sekine, Y.; Sobu, R.; Aoyama, Y.; Takahashi, Y.; Okada, S.; Sasagawa, H.; et al. The current trend of radiation therapy for patients with localized prostate cancer. Curr. Oncol. 2023, 30, 8092–8110. [Google Scholar] [CrossRef] [PubMed]
- Fassia, M.K.; Balasubramanian, A.; Woo, S.; Vargas, H.A.; Hricak, H.; Konukoglu, E.; Becker, A.S. Deep learning prostate MRI segmentation accuracy and robustness: A systematic review. Radiol. Artif. Intell. 2024, 6, e230138. [Google Scholar] [CrossRef]
- Nayagam, R.D.; Selvathi, D. A systematic review of deep learning methods for the classification and segmentation of prostate cancer on magnetic resonance images. Int. J. Imaging Syst. Technol. 2024, 34, e23064. [Google Scholar] [CrossRef]
- Khan, Z.; Yahya, N.; Alsaih, K.; Al-Hiyali, M.I.; Meriaudeau, F. Recent automatic segmentation algorithms of MRI prostate regions: A review. IEEE Access 2021, 9, 97878–97905. [Google Scholar] [CrossRef]
- Kalantar, R.; Lin, G.; Winfield, J.M.; Messiou, C.; Lalondrelle, S.; Blackledge, M.D.; Koh, D.M. Automatic segmentation of pelvic cancers using deep learning: State-of-the-art approaches and challenges. Diagnostics 2021, 11, 1964. [Google Scholar] [CrossRef]
- Wu, C.; Montagne, S.; Hamzaoui, D.; Ayache, N.; Delingette, H.; Renard-Penna, R. Automatic segmentation of prostate zonal anatomy on MRI: A systematic review of the literature. Insights Imaging 2022, 13, 202. [Google Scholar] [CrossRef]
- De Biase, A.; Sijtsema, N.M.; Janssen, T.; Hurkmans, C.; Brouwer, C.; van Ooijen, P. Clinical adoption of deep learning target auto-segmentation for radiation therapy: Challenges, clinical risks, and mitigation strategies. BJR Artif. Intell. 2024, 1, ubae015. [Google Scholar] [CrossRef]
- Isaksson, L.J.; Summers, P.; Mastroleo, F.; Marvaso, G.; Corrao, G.; Vincini, M.G.; Zaffaroni, M.; Ceci, F.; Petralia, G.; Orecchia, R.; et al. Automatic segmentation with deep learning in radiotherapy. Cancers 2023, 15, 4389. [Google Scholar] [CrossRef]
- Almeida, G.; Tavares, J.M.R.S. Deep learning in radiation oncology treatment planning for prostate cancer: A systematic review. J. Med. Syst. 2020, 44, 179. [Google Scholar] [CrossRef] [PubMed]
- Matoska, T.; Patel, M.; Liu, H.; Beriwal, S. Review of deep learning based autosegmentation for clinical target volume: Current status and future directions. Adv. Radiat. Oncol. 2024, 9, 101470. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.K.C.; Leung, V.W.S.; Hung, R.H.M. Clinical evaluation of deep learning and atlas-based auto-contouring for head and neck radiation therapy. Appl. Sci. 2022, 12, 11681. [Google Scholar] [CrossRef]
- Erdur, A.C.; Rusche, D.; Scholz, D.; Kiechle, J.; Fischer, S.; Llorián-Salvador, Ó.; Buchner, J.A.; Nguyen, M.Q.; Etzel, L.; Weidner, J.; et al. Deep learning for autosegmentation for radiotherapy treatment planning: State-of-the-art and novel perspectives. Strahlenther. Onkol. 2025, 201, 236–254. [Google Scholar] [CrossRef]
- Sun, Z.; Ng, C.K.C. Artificial intelligence (enhanced super-resolution generative adversarial network) for calcium deblooming in coronary computed tomography angiography: A feasibility study. Diagnostics 2022, 12, 991. [Google Scholar] [CrossRef]
- Sun, Z.; Ng, C.K.C. Finetuned super-resolution generative adversarial network (artificial intelligence) model for calcium deblooming in coronary computed tomography angiography. J. Pers. Med. 2022, 12, 1354. [Google Scholar] [CrossRef]
- Leung, V.W.S.; Ng, C.K.C.; Lam, S.K.; Wong, P.T.; Ng, K.Y.; Tam, C.H.; Lee, T.C.; Chow, K.C.; Chow, Y.K.; Tam, V.C.W.; et al. Computed tomography-based radiomics for long-term prognostication of high-risk localized prostate cancer patients received whole pelvic radiotherapy. J. Pers. Med. 2023, 13, 1643. [Google Scholar] [CrossRef]
- Rong, Y.; Chen, Q.; Fu, Y.; Yang, X.; Al-Hallaq, H.A.; Wu, Q.J.; Yuan, L.; Xiao, Y.; Cai, B.; Latifi, K.; et al. NRG Oncology assessment of artificial intelligence deep learning-based auto-segmentation for radiation therapy: Current developments, clinical considerations, and future directions. Int. J. Radiat. Oncol. Biol. Phys. 2024, 119, 261–280. [Google Scholar] [CrossRef]
- Ng, C.K.C. Performance of commercial deep learning-based auto-segmentation software for breast cancer radiation therapy planning: A systematic review. Multimodal Technol. Interact. 2024, 8, 114. [Google Scholar] [CrossRef]
- Ng, C.K.C. Artificial intelligence for radiation dose optimization in pediatric radiology: A systematic review. Children 2022, 9, 1044. [Google Scholar] [CrossRef]
- Ng, C.K.C. Diagnostic performance of artificial intelligence-based computer-aided detection and diagnosis in pediatric radiology: A systematic review. Children 2023, 10, 525. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.K.C. Generative adversarial network (generative artificial intelligence) in pediatric radiology: A systematic review. Children 2023, 10, 1372. [Google Scholar] [CrossRef] [PubMed]
- PRISMA Statement. Available online: https://www.prisma-statement.org/ (accessed on 17 January 2025).
- Aggarwal, R.; Sounderajah, V.; Martin, G.; Ting, D.S.W.; Karthikesalingam, A.; King, D.; Ashrafian, H.; Darzi, A. Diagnostic accuracy of deep learning in medical imaging: A systematic review and meta-analysis. NPJ Digit. Med. 2021, 4, 65. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Liu, Y.; Zhang, X.; Ye, Y.; Yin, G.; Johnson, B.A. Deep learning in remote sensing applications: A meta-analysis and review. ISPRS J. Photogramm. Remote Sens. 2019, 152, 166–177. [Google Scholar] [CrossRef]
- Shah, K.A.; Ng, C.K.C. Workplace violence in medical radiation science: A systematic review. Radiography 2024, 30, 440–447. [Google Scholar] [CrossRef]
- Ng, C.K.C. A review of the impact of the COVID-19 pandemic on pre-registration medical radiation science education. Radiography 2022, 28, 222–231. [Google Scholar] [CrossRef]
- Vasey, B.; Ursprung, S.; Beddoe, B.; Taylor, E.H.; Marlow, N.; Bilbro, N.; Watkinson, P.; McCulloch, P. Association of clinician diagnostic performance with machine learning-based decision support systems: A systematic review. JAMA Netw. Open. 2021, 4, e211276. [Google Scholar] [CrossRef]
- Imrey, P.B. Limitations of meta-analyses of studies with high heterogeneity. JAMA Netw. Open. 2020, 3, e1919325. [Google Scholar] [CrossRef]
- Mongan, J.; Moy, L.; Kahn, C.E., Jr. Checklist for artificial intelligence in medical imaging (CLAIM): A guide for authors and reviewers. Radiol. Artif. Intell. 2020, 2, e200029. [Google Scholar] [CrossRef]
- Sivanesan, U.; Wu, K.; McInnes, M.D.F.; Dhindsa, K.; Salehi, F.; van der Pol, C.B. Checklist for artificial intelligence in medical imaging reporting adherence in peer-reviewed and preprint manuscripts with the highest Altmetric Attention Scores: A meta-research study. Can. Assoc. Radiol. J. 2023, 74, 334–342. [Google Scholar] [CrossRef]
- Bhandari, A.; Scott, L.; Weilbach, M.; Marwah, R.; Lasocki, A. Assessment of artificial intelligence (AI) reporting methodology in glioma MRI studies using the Checklist for AI in Medical Imaging (CLAIM). Neuroradiology 2023, 65, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Tejani, A.S.; Klontzas, M.E.; Gatti, A.A.; Mongan, J.T.; Moy, L.; Park, S.H.; Kahn, C.E. Jr; CLAIM 2024 Update Panel. Checklist for Artificial Intelligence in Medical Imaging (CLAIM): 2024 update. Radiol. Artif. Intell. 2024, 6, e240300. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Bernard, M.; Downes, L.; Willows, B.; Feng, X.; Mourad, W.F.; St Clair, W.; Chen, Q. Evaluating the clinical acceptability of deep learning contours of prostate and organs-at-risk in an automated prostate treatment planning process. Med. Phys. 2022, 49, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Hobbis, D.; Yu, N.Y.; Mund, K.W.; Duan, J.; Rwigema, J.M.; Wong, W.W.; Schild, S.E.; Keole, S.R.; Feng, X.; Chen, Q.; et al. First report on physician assessment and clinical acceptability of custom-retrained artificial intelligence models for clinical target volume and organs-at-risk auto-delineation for postprostatectomy patients. Pract. Radiat. Oncol. 2023, 13, 351–362. [Google Scholar] [CrossRef]
- Tegtmeier, R.C.; Kutyreff, C.J.; Smetanick, J.L.; Hobbis, D.; Laughlin, B.S.; Toesca, D.A.S.; Clouser, E.L.; Rong, Y. Custom-trained deep learning-based auto-segmentation for male pelvic iterative CBCT on c-arm linear accelerators. Pract. Radiat. Oncol. 2024, 14, e383–e394. [Google Scholar] [CrossRef]
- Jenkins, A.; Mullen, T.S.; Johnson-Hart, C.; Green, A.; McWilliam, A.; Aznar, M.; van Herk, M.; Vasquez Osorio, E. Novel methodology to assess the effect of contouring variation on treatment outcome. Med. Phys. 2021, 48, 3234–3242. [Google Scholar] [CrossRef]
- Wong, J.; Fong, A.; McVicar, N.; Smith, S.; Giambattista, J.; Wells, D.; Kolbeck, C.; Giambattista, J.; Gondara, L.; Alexander, A. Comparing deep learning-based auto-segmentation of organs at risk and clinical target volumes to expert inter-observer variability in radiotherapy planning. Radiother. Oncol. 2020, 144, 152–158. [Google Scholar] [CrossRef]
- Wong, J.; Huang, V.; Wells, D.; Giambattista, J.; Giambattista, J.; Kolbeck, C.; Otto, K.; Saibishkumar, E.P.; Alexander, A. Implementation of deep learning-based auto-segmentation for radiotherapy planning structures: A workflow study at two cancer centers. Radiat. Oncol. 2021, 16, 101. [Google Scholar] [CrossRef]
- Zabel, W.J.; Conway, J.L.; Gladwish, A.; Skliarenko, J.; Didiodato, G.; Goorts-Matthews, L.; Michalak, A.; Reistetter, S.; King, J.; Nakonechny, K.; et al. Clinical evaluation of deep learning and atlas-based auto-contouring of bladder and rectum for prostate radiation therapy. Pract. Radiat. Oncol. 2021, 11, e80–e89. [Google Scholar] [CrossRef]
- Radici, L.; Ferrario, S.; Borca, V.C.; Cante, D.; Paolini, M.; Piva, C.; Baratto, L.; Franco, P.; La Porta, M.R. Implementation of a commercial deep learning-based auto segmentation software in radiotherapy: Evaluation of effectiveness and impact on workflow. Life 2022, 12, 2088. [Google Scholar] [CrossRef]
- Hoque, S.M.H.; Pirrone, G.; Matrone, F.; Donofrio, A.; Fanetti, G.; Caroli, A.; Rista, R.S.; Bortolus, R.; Avanzo, M.; Drigo, A.; et al. Clinical use of a commercial artificial intelligence-based software for autocontouring in radiation therapy: Geometric performance and dosimetric impact. Cancers 2023, 15, 5735. [Google Scholar] [CrossRef] [PubMed]
- Radici, L.; Piva, C.; Casanova Borca, V.; Cante, D.; Ferrario, S.; Paolini, M.; Cabras, L.; Petrucci, E.; Franco, P.; La Porta, M.R.; et al. Clinical evaluation of a deep learning CBCT auto-segmentation software for prostate adaptive radiation therapy. Clin. Transl. Radiat. Oncol. 2024, 47, 100796. [Google Scholar] [CrossRef] [PubMed]
- Urago, Y.; Okamoto, H.; Kaneda, T.; Murakami, N.; Kashihara, T.; Takemori, M.; Nakayama, H.; Iijima, K.; Chiba, T.; Kuwahara, J.; et al. Evaluation of auto-segmentation accuracy of cloud-based artificial intelligence and atlas-based models. Radiat. Oncol. 2021, 16, 175. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, G.; Mangili, P.; Deantoni, C.; Fodor, A.; Broggi, S.; Castriconi, R.; Ubeira Gabellini, M.G.; Del Vecchio, A.; Di Muzio, N.G.; Fiorino, C. Real-world validation of artificial intelligence-based computed tomography auto-contouring for prostate cancer radiotherapy planning. Phys. Imaging Radiat. Oncol. 2023, 28, 100501. [Google Scholar] [CrossRef]
- Walker, Z.; Bartley, G.; Hague, C.; Kelly, D.; Navarro, C.; Rogers, J.; South, C.; Temple, S.; Whitehurst, P.; Chuter, R. Evaluating the effectiveness of deep learning contouring across multiple radiotherapy centres. Phys. Imaging Radiat. Oncol. 2022, 24, 121–128. [Google Scholar] [CrossRef]
- Gibbons, E.; Hoffmann, M.; Westhuyzen, J.; Hodgson, A.; Chick, B.; Last, A. Clinical evaluation of deep learning and atlas-based auto-segmentation for critical organs at risk in radiation therapy. J. Med. Radiat. Sci. 2023, 70, 15–25. [Google Scholar] [CrossRef]
- Wang, Y.; Boyd, G.; Zieminski, S.; Kamran, S.C.; Zietman, A.L.; Miyamoto, D.T.; Kirk, M.C.; Efstathiou, J.A. A pair of deep learning auto-contouring models for prostate cancer patients injected with a radio-transparent versus radiopaque hydrogel spacer. Med. Phys. 2023, 50, 3324–3337. [Google Scholar] [CrossRef]
- Kiljunen, T.; Akram, S.; Niemelä, J.; Löyttyniemi, E.; Seppälä, J.; Heikkilä, J.; Vuolukka, K.; Kääriäinen, O.S.; Heikkilä, V.P.; Lehtiö, K.; et al. A deep learning-based automated CT segmentation of prostate cancer anatomy for radiation therapy planning-A retrospective multicenter study. Diagnostics 2020, 10, 959. [Google Scholar] [CrossRef]
- Elisabeth Olsson, C.; Suresh, R.; Niemelä, J.; Akram, S.U.; Valdman, A. Autosegmentation based on different-sized training datasets of consistently-curated volumes and impact on rectal contours in prostate cancer radiation therapy. Phys. Imaging Radiat. Oncol. 2022, 22, 67–72. [Google Scholar] [CrossRef]
- Strolin, S.; Santoro, M.; Paolani, G.; Ammendolia, I.; Arcelli, A.; Benini, A.; Bisello, S.; Cardano, R.; Cavallini, L.; Deraco, E.; et al. How smart is artificial intelligence in organs delineation? Testing a CE and FDA-approved deep-learning tool using multiple expert contours delineated on planning CT images. Front. Oncol. 2023, 13, 1089807. [Google Scholar] [CrossRef]
- Miura, H.; Ishihara, S.; Kenjo, M.; Nakao, M.; Ozawa, S.; Kagemoto, M. Evaluation of the accuracy of automated segmentation based on deep learning for prostate cancer patients. Med. Dosim. 2025, 50, 91–95. [Google Scholar] [CrossRef] [PubMed]
- De Kerf, G.; Claessens, M.; Raouassi, F.; Mercier, C.; Stas, D.; Ost, P.; Dirix, P.; Verellen, D. A geometry and dose-volume based performance monitoring of artificial intelligence models in radiotherapy treatment planning for prostate cancer. Phys. Imaging Radiat. Oncol. 2023, 28, 100494. [Google Scholar] [CrossRef]
- Kanwar, A.; Merz, B.; Claunch, C.; Rana, S.; Hung, A.; Thompson, R.F. Stress-testing pelvic autosegmentation algorithms using anatomical edge cases. Phys. Imaging Radiat. Oncol. 2023, 25, 100413. [Google Scholar] [CrossRef] [PubMed]
- Marschner, S.; Datar, M.; Gaasch, A.; Xu, Z.; Grbic, S.; Chabin, G.; Geiger, B.; Rosenman, J.; Corradini, S.; Niyazi, M.; et al. A deep image-to-image network organ segmentation algorithm for radiation treatment planning: Principles and evaluation. Radiat. Oncol. 2022, 17, 129. [Google Scholar] [CrossRef] [PubMed]
- Pera, Ó.; Martínez, Á.; Möhler, C.; Hamans, B.; Vega, F.; Barral, F.; Becerra, N.; Jimenez, R.; Fernandez-Velilla, E.; Quera, J.; et al. Clinical validation of Siemens’ Syngo.via automatic contouring system. Adv. Radiat. Oncol. 2023, 8, 101177. [Google Scholar] [CrossRef]
- Yamauchi, R.; Itazawa, T.; Kobayashi, T.; Kashiyama, S.; Akimoto, H.; Mizuno, N.; Kawamori, J. Clinical evaluation of deep learning and atlas-based auto-segmentation for organs at risk delineation. Med. Dosim. 2024, 49, 167–176. [Google Scholar] [CrossRef]
- Berenato, S.; Williams, M.; Woodley, O.; Möhler, C.; Evans, E.; Millin, A.E.; Wheeler, P.A. Novel dosimetric validation of a commercial CT scanner based deep learning automated contour solution for prostate radiotherapy. Phys. Med. 2024, 122, 103339. [Google Scholar] [CrossRef]
- Künzel, L.A.; Nachbar, M.; Hagmüller, M.; Gani, C.; Boeke, S.; Wegener, D.; Paulsen, F.; Zips, D.; Thorwarth, D. Clinical evaluation of autonomous, unsupervised planning integrated in MR-guided radiotherapy for prostate cancer. Radiother. Oncol. 2022, 168, 229–233. [Google Scholar] [CrossRef]
- Nachbar, M.; Lo Russo, M.; Gani, C.; Boeke, S.; Wegener, D.; Paulsen, F.; Zips, D.; Roque, T.; Paragios, N.; Thorwarth, D. Automatic AI-based contouring of prostate MRI for online adaptive radiotherapy. Z. Med. Phys. 2024, 34, 197–207. [Google Scholar] [CrossRef]
- Moazzezi, M.; Rose, B.; Kisling, K.; Moore, K.L.; Ray, X. Prospects for daily online adaptive radiotherapy via ethos for prostate cancer patients without nodal involvement using unedited CBCT auto-segmentation. J. Appl. Clin. Med. Phys. 2021, 22, 82–93. [Google Scholar] [CrossRef]
- Duan, J.; Tegtmeier, R.C.; Vargas, C.E.; Yu, N.Y.; Laughlin, B.S.; Rwigema, J.M.; Anderson, J.D.; Zhu, L.; Chen, Q.; Rong, Y. Achieving accurate prostate auto-segmentation on CT in the absence of MR imaging. Radiother. Oncol. 2025, 202, 110588. [Google Scholar] [CrossRef] [PubMed]
- Bordigoni, B.; Trivellato, S.; Pellegrini, R.; Meregalli, S.; Bonetto, E.; Belmonte, M.; Castellano, M.; Panizza, D.; Arcangeli, S.; De Ponti, E. Automated segmentation in pelvic radiotherapy: A comprehensive evaluation of ATLAS-, machine learning-, and deep learning-based models. Phys. Med. 2024, 125, 104486. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Vargas, C.E.; Yu, N.Y.; Laughlin, B.S.; Toesca, D.S.; Keole, S.; Rwigema, J.C.M.; Wong, W.W.; Schild, S.E.; Feng, X.; et al. Incremental retraining, clinical implementation, and acceptance rate of deep learning auto-segmentation for male pelvis in a multiuser environment. Med. Phys. 2023, 50, 4079–4091. [Google Scholar] [CrossRef] [PubMed]
- Doolan, P.J.; Charalambous, S.; Roussakis, Y.; Leczynski, A.; Peratikou, M.; Benjamin, M.; Ferentinos, K.; Strouthos, I.; Zamboglou, C.; Karagiannis, E. A clinical evaluation of the performance of five commercial artificial intelligence contouring systems for radiotherapy. Front. Oncol. 2023, 13, 1213068. [Google Scholar] [CrossRef]
- Van Dijk, L.V.; Van den Bosch, L.; Aljabar, P.; Peressutti, D.; Both, S.; Steenbakkers, R.J.H.M.; Langendijk, J.A.; Gooding, M.J.; Brouwer, C.L. Improving automatic delineation for head and neck organs at risk by deep learning contouring. Radiother. Oncol. 2020, 142, 115–123. [Google Scholar] [CrossRef]
- Gay, H.A.; Jin, J.Y.; Chang, A.J.; Ten Haken, R.K. Utility of normal tissue-to-tumor a/b Ratio when evaluating isodoses of isoeffective radiation therapy treatment plans. Int. J. Radiat. Oncol. Biol. Phys. 2012, 85, e81–e87. [Google Scholar] [CrossRef]
- Lin, H.; Xiao, H.; Dong, L.; Teo, K.B.; Zou, W.; Cai, J.; Li, T. Deep learning for automatic target volume segmentation in radiation therapy: A review. Quant. Imaging Med. Surg. 2021, 11, 4847–4858. [Google Scholar] [CrossRef]
- Mackay, K.; Bernstein, D.; Glocker, B.; Kamnitsas, K.; Taylor, A. A review of the metrics used to assess auto-contouring systems in radiotherapy. Clin. Oncol. 2023, 35, 354–369. [Google Scholar] [CrossRef]
- Almberg, S.S.; Lervåg, C.; Frengen, J.; Eidem, M.; Abramova, T.M.; Nordstrand, C.S.; Alsaker, M.D.; Tøndel, H.; Raj, S.X.; Wanderås, A.D. Training, validation, and clinical implementation of a deep-learning segmentation model for radiotherapy of loco-regional breast cancer. Radiother. Oncol. 2022, 173, 62–68. [Google Scholar] [CrossRef]
- Chai, Y. Letter to the editor regarding the article “comparison of transfer learning models in pelvic tilt and rotation measurement in pediatric anteroposterior pelvic radiographs”. J. Imaging Inform. Med. 2024, 37, 1259–1260. [Google Scholar] [CrossRef]
- Waffenschmidt, S.; Knelangen, M.; Sieben, W.; Bühn, S.; Pieper, D. Single screening versus conventional double screening for study selection in systematic reviews: A methodological systematic review. BMC Med. Res. Methodol. 2019, 19, 132. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Ng, C.K.C.; Dos Reis, C.S. Synchrotron radiation computed tomography versus conventional computed tomography for assessment of four types of stent grafts used for endovascular treatment of thoracic and abdominal aortic aneurysms. Quant. Imaging Med. Surg. 2018, 8, 609–620. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Software Name and Version | Author, Year and Country | Geometric Accuracy | ||
|---|---|---|---|---|
| DLAS | IOV | DLAS VS IOV | ||
| Carina Medical LLC | ||||
| INTContour | Duan et al. (2022), USA [37] | Mean DSC, HD95 (mm), MSD (mm), sDSC, HD90 (mm), HD98 (mm), recall, precision, and VR: prostate (0.83, 5.3, 2.1, 0.75, 4.5, 6.1, 0.84, 0.82, and 1.05); SVs (0.72, 5.7, 2.0, 0.81, 4.8, 6.9, 0.76, 0.70, and 1.09); bladder (0.93, 4.6, 1.3, 0.91, 3.6, 5.7, 0.94, 0.92, and 1.02); L (0.96, 2.4, 0.6, 0.97, 1.8, 2.9, 0.95, 0.98, and 0.97) and R femoral heads (0.97, 2.2, 0.6, 0.97, 1.8, 2.8, 0.96, 0.97, and 0.99); penile bulb (0.53, 6.2, 2.6, 0.28, 5.4, 7.1, 0.55, 0.56, and 1.01); rectum (0.85, 7.6, 2.0, 0.82, 5.4, 10.0, 0.83, 0.88, and 0.94); all structures (0.83, 5.3, 2.1, 0.75, 4.5, 6.1, 0.84, 0.82, and 1.05) | Mean DSC, HD95 (mm), MSD (mm), sDSC, HD90 (mm), HD98 (mm), recall, precision, and VR: all structures (0.80, 6.1, 2.2, 0.78, 5.0, 6.9, 0.93, 0.72, and 1.32) | DLAS outperforming ROs with statistically significantly different precision, and VR (p < 0.001) and ns for DSC, HD95, MSD, sDSC, HD90, and HD98 |
| Hobbis et al. (2023), USA [38] | Median DSC, HD95 (mm), and MSD (mm) for model finetuned by 60 cases (90 for CTVs): prostate and SV beds (0.73, 11.3, and 7.3); bladder (0.98, 2.0, and 0.7); L (0.98, 1.8, and 0.5) and R femoral heads (0.97, 1.1, and 0.6); penile bulb (0.54, 5.7, and 2.7); rectum (0.92, 5.7, and 1.6) | NA | NA | |
| Tegtmeier et al. (2024), USA [39] | Mean DSC, HD95 (mm), MSD (mm), and PVD: prostate (0.91, 2.3, 1.0, and 2.2%); prostate bed (0.75, 9.5, 3.2, and −14.9%); bladder (0.96, 3.4, 1.0, and 0.3%); L and R femoral heads (0.96, 1.1, 0.3, and 4.9%); rectum (0.90, 3.4, 0.8, and 12.0%) | NA | NA | |
| Elekta AB | ||||
| ADMIRE v3.4 | Jenkins et al. (2021), UK [40] | Mean DSC: prostate (0.81) | NA | NA |
| Limbus AI Inc. | ||||
| Contour v1.0.22 | Wong et al. (2020), Canada [41] | Mean DSC and HD95 (mm): prostate (0.79 and 6.7); SVs (0.64 and 6.0); bladder (0.97 and 3.2); L and R femoral heads (0.91 and 7.1); rectum (0.78 and 12.1) | Mean DSC and HD95 (mm): prostate (0.83 and 5.3); SVs (0.63 and 5.9); bladder (0.96 and 3.0); L and R femoral heads (0.91 and 7.0); rectum (0.79 and 11.3) | DLAS outperforming ROs for bladder and L and R femoral heads with statistically significantly different DSC (p < 0.005–0.018) and ns for DSC and HD95 of SVs and rectum and HD95 of L and R femoral heads |
| Wong et al. (2021), Canada [42] | Median DSC and HD95 (mm): prostate (0.90 and 4.3); bladder (0.99 and 0.6), L (0.99 and 1.3) and R femoral heads (0.99 and 1.3); rectum (0.95 and 3.0) | NA | NA | |
| Contour v1.0.18 | Zabel et al. (2021), Canada [43] | Mean DSC: bladder (0.99); rectum (0.95) | Mean DSC: bladder (0.99); rectum (0.97) | ns |
| Contour v1.5.0 | Radici et al. (2022), Italy [44] | Mean DSC, DCOM (mm), and PVD: bladder (0.89, 2.7, and 9.1%); L (0.95, 1.7, and −6.4%) and Rand femoral heads (0.92, 0.8, and −4.7%); penile bulb (0.39, 3.3, and 0.7 cm3); rectum (0.77, 5.0, and 11.3%) | NA | NA |
| Contour v1.0.18 | Hoque et al. (2023), Italy [45] | Mean DSC, HD (mm), and PVD: prostate (0.80, 15.4, and 12.0%); anal canal (0.70, 5.4, and 33.0%); bladder (0.94, 4.1, and 3.0%); L (0.78, 18.1, and 50.0%) and R femurs (0.78, 18.0, and 49.0%); rectum (0.83, 14.2, and 15.0%) | Mean DSC, HD (mm), and PVD: prostate (0.91, 5.9, and 9.0%); anal canal (0.91, 3.1, and 12.0%); bladder (0.98, 3.1, and 2.0%); L (0.98, 2.0, and 3.0%) and R femurs (0.98, 2.5, and 3.0%); rectum (0.97, 4.8, and 6.0%) | NA |
| Contour v1.5.0-D2 | Radici et al. (2024), Italy [46] | Mean DSC, DCOM (mm), and PVD for CT/CBCT: prostate (0.74, 6.1, and −11.5%/0.83, 2.5, and −11.8%); SVs (0.59, 6.8, and −40.0%/0.70, 3.9, and −21.0%); bladder (0.89, 3.0, and −9.0%/0.90, 2.2, and −2.0%); L and R femoral heads (0.96, <2.0, and −2.0%/0.96, <2.0, and −5.0%); rectum (0.81, 5.7, and −13.0%/0.86, 3.8, and −15.0%) | Median DSC, DCOM (mm), and PVD: prostate (0.83, 2.5, and −18.5%); SVs (0.71, 2.0, and −26.0%); bladder (0.90, 1.9, and −12.4%); L and R femoral heads (0.93, 2.0, and −4.0%); rectum (0.81, 6.5, −22.0%) 1 | DLAS based on CBCT outperforming ROs for L and R femoral heads with statistically significantly different median DSC and DCOM (p < 0.01–0.02) and ns for other structures |
| MIM Software Inc. | ||||
| ProtégéAI v0.9 | Urago et al. (2021), Japan [47] | Median DSC, HD (mm), MDA (mm), and PVD: bladder (0.95, 6.1, 0.9, and 6.2%); rectum (0.87, 7.9, 1.2, and 17.6%) | NA | NA |
| Contour ProtégéAI v1.1.2 | Palazzo et al. (2023), Italy [48] | Median DSC and HD (mm): prostate (0.82 and 12.0); SVs (0.66 and 12.8); bladder (0.94 and 6.6), L and R femoral heads (0.82 and 112.8); rectum (0.82 and 22.1) | Median DSC and HD (mm): prostate (0.83 and 10.9); SVs (0.73 and 8.5); bladder (0.93 and 5.9); L and R femoral heads (0.65 and 216.1); rectum (0.81 and 18.3) | NA |
| Mirada Medical Ltd. | ||||
| DLCExpert | Walker et al. (2022), UK [49] | Median DSC and MDA (mm): bladder (0.88 and 1.9); L (0.92 and 1.6) and R femoral heads (0.91 and 1.7); rectum (0.67 and 4.7) | NA | NA |
| Gibbons et al. (2023), Australia [50] | Median DSC and HD (mm): bladder (0.96 and 12.8); L and R femoral heads (0.98 and 6.8); rectum (0.87 and 9.6) | NA | NA | |
| Wang et al. (2023), USA [51] | Mean DSC and MDA (mm) for model 1/2: prostate (0.84 and 1.8/0.85 and 1.7); SVs (0.60 and 2.4/0.62 and 2.3); bladder (0.91 and 1.4/0.95 and 0.8); L (0.94 and 0.8/0.96 and 0.5) and R femoral heads (0.95 and 0.7/0.96 and 0.5); penile bulb (0.66 and 2.2/0.65 and 2.2); rectum (0.81 and 2.3/0.84 and 1.9); spacer (0.52 and 2.9/0.84 and 0.9) | Mean DSC and MDA (mm) for model 2: prostate (0.83 and 2.0); SVs (0.62 and 2.3); bladder (0.95 and 0.9); L (0.96 and 0.5) and R femoral heads (0.96 and 0.5); penile bulb (0.63 and 2.3); rectum (0.84 and 1.9); spacer (0.83 and 1.0) | NA | |
| MVision.ai | ||||
| Contour+ | Kiljunen et al. (2020), Estonia, Finland, and Singapore [52] | Mean DSC, HD95 (mm), sDSC, and PVD: prostate (0.82, 6.1, 0.38, and −31.6%); lymph nodes (0.80, 14.7, 0.39, and 5.2%); SVs (0.72, 7.1, 0.52, and −11.1%); bladder (0.93, 3.3, 0.68, and −1.7%); L (0.68, 25.0, 0.22, and −37.9%) and R femoral heads (0.69, 24.7, 0.22, and −30.5%); penile bulb (0.51, 7.7, 0.33, and −6.8%); rectum (0.84, 11.4, 0.58, and −9.6%) | Mean DSC: prostate (0.83); lymph nodes (0.76); SVs (0.77); bladder (0.91); penile bulb (0.64); rectum (0.75) | NA |
| Contour+ v1.2.1 | Olsson et al. (2022), Finland and Sweden [53] | Mean DSC, HD (mm), and PVD: rectum (0.89, 4.7, and 3.7%) | NA | NA |
| Contour+ v1.2.5 | Miura et al. (2024), Japan [55] | Mean DSC, HD95, and PVD: prostate (0.86, 2.6, and −12.8%); SVs (0.80, 2.6, and −2.1%); bladder (0.96, 1.2, and −2.1%); L (0.98, 1.2, and −4.1%) and R femoral heads (0.97, 1.5, and −4.7%); penile bulb (0.64, 2.6, and −1.2%); rectum (0.92, 2.4, and 5.9%) | NA | NA |
| RaySearch Laboratories AB | ||||
| RayStation v11B | De Kerf et al. (2023), Belgium [56] | Mean sDSC and local sDSC: bladder (0.98 and 0.97); anorectum (0.98 and 0.93) | NA | NA |
| RayStation v9B | Kanwar et al. (2023), USA [57] | Mean DSC, HD95, and MSD (mm) for normal/variants: prostate (0.81, 6.3, and 4.4/0.75, 10.4, and 5.0); bladder (0.95, 3.3, and 2.2/0.87, 8.3, and 3.5); L and R femoral heads (0.87, 14.6, and 2.5/0.83, 13.7, and 3.0); rectum (0.63, 29.5, and 6.9/0.51, 33.4, and 9.4) | NA | NA |
| Siemens Healthineers AG | ||||
| AI-Rad Companion Organs RT VA20/syngo.via RT Image Suite VB50 | Marschner et al. (2022), Germany and USA [58] | Mean DSC, HD95 (mm), DCOM (mm), MSD (mm), PVD, RMSD (mm), sensitivity, specificity, JCI, DI, GMI, and left, right, anterior, posterior, superior, and inferior boundaries (mm): bladder (0.88, 6.7, 4.1, 1.8, 9.4%, 3.1, 0.93, 0.99, 0.81, 0.13, 0.07, 0.1, 2.9, 2.0, −1.9, −1.8, and −0.3); rectum (0.79, 10.8, 8.9, 2.5, 9.0%, 4.6, 0.84, 0.99, 0.67, 0.22, 0.16, 2.5, −0.9, 5.2, 1.7, −8.7, and 7.0) | NA | NA |
| syngo.via RT Image Suite VB40 | Pera et al. (2023), Germany and Spain [59] | Mean DSC: prostate (0.87); abdominopelvic cavity (0.94); bladder (0.95); body (0.99); L (0.99), and R femoral heads (0.98); rectum (0.90) | NA | NA |
| AI-Rad Companion Organs RT VA30 | Yamauchi et al. (2024), Japan [60] | Median DSC, HD (mm), and MDA (mm): prostate (0.78, 8.2, and 2.4); SVs (0.68, 7.3, and 1.3); bladder (0.94, 7.6, and 1.2); rectum (0.76, 27.1, and 4.6) | NA | NA |
| DirectORGANS VA30 | Berenato et al. (2024), Germany and UK [61] | Median DSC and MSD (mm): bladder (0.95 and 0.8); L (0.95 and 1.0) and R proximal femurs (0.96 and 0.8); rectum (0.89 and 1.2) | Median DSC and MSD (mm): bladder (0.97 and 0.5); L (0.97 and 0.5) and R proximal femurs (0.97 and 0.5); rectum (0.92 and 0.9) | Observer outperforming DLAS for all structures with statistically significant difference (p = 0.00) |
| Therapanacea | ||||
| Annotate ART-Plan v1.8.3 | Nachbar et al. (2024), France and Germany [63] | Median DSC, HD95 (mm), sDSC, and APL (mm): prostate (0.86, 5.0, 0.90, and 402); SVs (0.77, 4.4, 0.88, and 321); anal canal (0.74, 5.6, 0.75, and 0.0); bladder (0.97, 2.7, 0.97, and 101); L (0.92, 4.6, 0.99, and 123) and R femurs (0.92, 4.7, 0.98, and 157); L (0.91, 2.5, 0.96, and 539) and R pelvis (0.90, 3.3, 0.95, and 1010); penile bulb (0.73, 5.6, 0.93, and 119); rectum (0.91, 6.9, 0.98, and 225); sacrum (0.89, 4.8, 0.95, and 191) | NA | NA |
| Varian Medical Systems, Inc. | ||||
| Ethos | Moazzezi et al. (2021), USA [64] | Mean PVD: CTVs (4.5%) | NA | NA |
| Carina Medical LLC and RaySearch Laboratories AB | ||||
| INTContour and RayStation | Duan et al. (2025), USA [65] | Median DSC, HD (mm), HD95 (mm), MSD (mm), sDSC, and HD98 (mm) for INTContour original/RayStation original/INTContour finetuned model: prostate (0.77, 13.4, 8.0, 2.7, 0.64, and 9.5/0.78, 15.2, 8.3, 2.6, 0.64, and 10.3/0.82, 10.7, 6.3, 2.1, 0.78, and 7.4) | Median DSC, HD (mm), HD95 (mm), MSD (mm), sDSC, and HD98 (mm): prostate (0.93, 11.0, 8.0, 1.0, 0.89, and 9.3) | Finetuned DLAS model outperforming ROs with statistically significantly different HD95 and HD98 (p < 0.05) and ns for DSC, HD, MSD, and sDSC |
| Limbus AI Inc. and MVision.ai | ||||
| Contour v1.7.0-B3 and Contour+ v1.2.2 | Bordigoni et al. (2024), Italy and Sweden [66] | Median DSC, HD (mm), and DAP for Limbus/MVision.ai: bladder (0.93, 12.4, and 93.4%/0.94, 11.4, and 94.0%); L (0.97, 7.9, and 98.6%/0.97, 10.6, and 97.4%) and R femoral heads (0.97, 10.6, and 96.8%/0.97, 8.2, and 97.9%); rectum (0.87, 18.6, and 66.3%/0.87, 19.6, and 62.5%) | NA | NA |
| Carina Medical LLC, Manteia Medical Technologies Co., and MIM Software Inc. | ||||
| INTContour, AccuContour, and Contour ProtégéAI | Duan et al. (2023), USA [67] | Mean (finetuned model)/median (original models) DSC, HD95 (mm), MSD (mm), sDSC, HD90 (mm), and HD98 (mm) for deidentified original model 1/2/3/INTContour finetuned model: prostate (0.73, 8.8, 3.5, 0.56, 7.7, and 10.1/0.80, 6.5, 2.6, 0.69, 5.3, and 7.9/0.76, 9.4, 3.4, 0.57, 8.0, and 10.1/0.82, 6.6, 2.4, 0.73, 5.5, and 7.7); SVs (0.30, 13.0, 4.8, 0.39, 11.1, and 14.6/0.38, 11.3, 4.5, 0.46, 9.6, and 13.0/0.32, 11.6, 4.5, 0.46, 9.9, and 13.6/0.48, 10.0, 3.8, 0.5, 8.5, and 11.3); balloon (NA/NA/NA/0.89, 5.9, 1.9, 0.87, 3.8, and 8.6); bladder (0.96, 1.9, 0.7, 0.97, 2.1, and 3.5/0.96, 2.3, 0.8, 0.97, 1.9, and 4.4/0.96, 3.2, 1.0, 0.95, 2.4, and 4.8/0.96, 5.0, 1.5, 0.96, 4.1, and 6.0); L (0.95, 3.6, 0.8, 0.93, 2.1, and 6.0/0.78, 64.3, 13.6, 0.75, 49.5, and 70.9/0.95, 3.8, 1.0, 0.90, 3.2, and 4.1/0.92, 9.6, 2.0, 0.90, 6.4, and 12.2) and R femoral heads (0.94, 4.8, 0.9, 0.91, 3.2, and 6.6/0.71, 79.4, 20.4, 0.70, 67.1, and 87.7/0.87, 8.4, 2.4, 0.77, 6.1, and 11.1/0.92, 9.1, 1.9, 0.90, 6.0, and 11.7); large (NA/NA/NA/0.49, 36.9, 12.5, 0.41, 30.7, and 41.4) and small bowels (NA/NA/NA/0.30, 40.7, 19.9, 0.30, 36.7, and 44.1); penile bulb (NA/NA/NA/0.47, 6.9, 3.1, 0.17, 6.1, and 7.5); rectum (0.84, 10.1, 3.0, 0.65, 7.7, and 12.3/0.86, 7.6, 2.6, 0.66, 6.1, and 10.4/0.79, 9.0, 3.3, 0.55, 8.5, and 9.8/0.92, 5.4, 1.5, 0.89, 3.8, and 7.4); spacer (NA/NA/NA/0.84, 4.5, 1.7, 0.79, 3.9, and 5.3) | NA | NA |
| Mirada Medical Ltd., MVision.ai, Radformation Inc., RaySearch Laboratories AB, and Therapanacea | ||||
| DLCExpert v2.6.4.47181, Contour+ v1.2.1, AutoContour v1.0.25.0, RayStation v12.0.0.932, and Annotate v1.10.0 | Doolan et al. (2023), Cyprus and Germany [68] | Median DSC, HD (mm), sDSC, and APL (mm) for DLCExpert/MVision Contour+/Radformation AutoContour/RayStation/Therapanacea Annotate: prostate (0.86, 7.8, 0.36, and 3226/0.89, 6.9, 0.45, and 2957/0.87, 7.0, 0.34, and 3591/0.85, 7.8, 0.33, and 3415/0.91, 6.9, 0.48, and 3063); SVs (0.76, 9.0, 0.43, and 1862/0.83, 8.0, 0.57, and 1489/0.75, 8.8, 0.48, and 1817/NA/0.82, 7.9, 0.59, and 1404); bladder (0.95, 16.2, 0.62, and 7044/0.97, 6.3, 0.74, and 5342/0.97, 6.9, 0.70, and 6886/0.95, 7.7, 0.60, and 8203/0.97, 5.7, 0.77, and 4753); bowels (0.59, 75.5, 0.06, and 118000/0.75, 76.5, 0.13, and 103000/0.73, 69.2, 0.10, and 113000/NA/0.76, 55.6, 0.17, and 105000); cauda equina (NA/NA/0.75, 30, 0.39, and 3416/NA/NA); L (0.91, 16.1, 0.61, and 5586/0.91, 16.9, 0.66, and 4724/0.90, 17.2, 0.64, and 5242/0.89, 25.3, 0.59, and 5887/0.90, 18.8, 0.70, and 4067) and R femoral heads (0.89, 18.4, 0.59, and 5624/0.91, 16.0, 0.65, and 4957/0.91, 15.9, 0.62, and 5511/0.88, 27.8, 0.51, and 6887/0.90, 18.6, 0.68, and 4068); penile root (0.54, 11.9, 0.23, and 794/0.68, 11.0, 0.36, and 800/0.66, 11.4, 0.35, and 758/NA/0.71, 8.9, 0.39, and 698); rectum (0.87, 15.0, 0.53, and 3802/0.91, 11.6, 0.59, and 3322/0.88, 15.6, 0.57, and 3425/0.87, 19.0, 0.53, and 3565/0.83, 26.0, 0.57, and 3630); sigmoid (NA/0.77, 26.3, 0.55, and 2798/NA/NA/0.52, 47.1, 0.37, and 2950) | NA | NA |
| Software Name and Version | Author, Year, and Country | Evaluation Results | ||
|---|---|---|---|---|
| Subjective | Efficiency | Dosimetric | ||
| Carina Medical LLC | ||||
| INTContour | Duan et al. (2022), USA [37] | No/minor corrections required for 95.7%/4.3% of structures; no unusable contours | NA | No statistically significant difference in doses to OARs except bladder between DLAS and manual contouring, and DLAS bladder dose being lower |
| Hobbis et al. (2023), USA [38] | No/minor corrections required for 36.0%/51.0% of OARs and 17.0%/37.0% of CTVs; unusable OARs (1.0%) and CTVs contours (2.0%) delineated by original model | NA | NA | |
| Tegtmeier et al. (2024), USA [39] | Mean contour score: prostate (4.4), prostate bed (3.0), bladder (4.6), L and R femoral heads (4.0), and rectum (3.9) out of 5.0 (1 and 5 indicating unusable and no corrections required), respectively | NA | NA | |
| Limbus AI Inc. | ||||
| Contour v1.0.22 | Wong et al. (2020), Canada [41] | NA | Mean time reduction/patient: 98.1% (manual: 21.3 min vs. DLAS: 0.4 min) 1 | NA |
| Wong et al. (2021), Canada [42] | Mean contour score: prostate (2.8), SVs (2.1), bladder (1.4), L and R femoral heads (1.6), and rectum (1.7) out of 5.0 (1 and 5 indicating minimal and significant corrections required); mean user satisfaction score: CTV (4.1) and OARs (4.6) out of 5.0 (1 and 5 representing poor and high satisfactions), respectively | NA | NA | |
| Contour v1.0.18 | Zabel et al. (2021), Canada [43] | No corrections required for 89.0% and 76.0% of bladder and rectum contours, respectively | Mean time reduction/patient: 55.6% (manual: 15.3 min vs. DLAS: 6.8 min) | NA |
| Contour v1.5.0 | Radici et al. (2022), Italy [44] | NA | Mean time reduction/patient: 18.0% (4.0 min) | No clinically relevant difference in doses to L and R femoral heads between DLAS and manual contouring; other OARs with relevant dosimetric differences |
| Contour v1.0.18 | Hoque et al. (2023), Italy [45] | No/minor contour corrections required: prostate (0.0%/65.0%), anal canal (25.0%/75.0%), bladder (5.0%/75.0%), L (65.0%/35.0%) and R femurs (65.0%/30.0%), and rectum (90.0%/10.0%); unusable contours: prostate (5.0%) and R femur (5.0%) | Mean time reduction/patient: 72.1% (manual: 23.0 min vs. DLAS: 6.4 min) 2 | No statistically significant difference in doses to all structures except anal canal between DLAS with contour corrections and manual contouring |
| Contour v1.5.0-D2 | Radici et al. (2024), Italy [46] | No corrections required for all OARs except rectum | NA | NA |
| MIM Software Inc. | ||||
| Contour ProtégéAI v0.9 | Urago et al. (2021), Japan [47] | NA | NA | NA |
| Contour ProtégéAI v1.1.2 | Palazzo et al. (2023), Italy [48] | No/minor corrections required for 10.0%/77.5% of structures; no unusable contours | Mean time reduction/patient: 75.6% (manual: 20.5 min vs. DLAS: 5.0 min) | NA |
| Mirada Medical Ltd. | ||||
| DLCExpert | Walker et al. (2022), UK [49] | Mean contour scores for centre 1/2: bladder (4.5/3.6), L (1.8/1.3) and R femoral heads (1.5/1.2) and rectum (5.3/3.6) out of 7.0 (1–3 and 7 indicating no corrections required and gross error)/5.0 (1–2 and 5 representing no corrections required and unusable), respectively | Mean time reduction/patient: 30.0% (manual: 19.5 min vs. DLAS: 13.7 min) 2 | NA |
| Gibbons et al. (2023), Australia [50] | Median contour score: bladder (2.0), L (1.5) and R femoral heads (1.0) and rectum (2.0) out of 4.0 (1 and 4 indicating no and major corrections required) | Mean time reduction/patient: 65.4% (manual: 10.7 min vs. DLAS: 3.7 min) 2 | NA | |
| Wang et al. (2023), USA [51] | Mean contour score for model 1/2: prostate (2.7/2.2), SVs (3.3/2.4), bladder (2.3/1.3), L (1.1/1.0) and R femoral heads (1.1/1.0), penile bulb (3.4/2.4), rectum (3.0/2.1), and spacer (3.6/1.3) out of 4.0 (1 and 4 indicating no/minor corrections required and unusable), respectively | Mean efficiency gain score for model 1/2: 2.79/2.20 out of 4.00 (1.00–1.75: nearly complete; 1.76–2.50: substantial; 2.51–3.25: meaningful; 3.26–4.00: no efficiency gain) | NA | |
| MVision.ai | ||||
| Contour+ | Kiljunen et al. (2020), Estonia, Finland, and Singapore [52] | NA | Mean time reduction/patient: 44.4% (manual: 27.0 min vs. DLAS: 15.0 min) | NA |
| Contour+ v1.2.1 | Olsson et al. (2022), Finland and Sweden [53] | NA | NA | No clinically relevant difference in dose to OAR between DLAS and manual contouring |
| Strolin et al. (2023), Italy [54] | Mean contour score: 4.8 out of 5.0 (1 and 5 indicating unusable and no corrections required), respectively | Median time reduction/patient: 53.0% (manual: 25.8 min vs. DLAS: 12.1 min) 2 | NA | |
| Contour+ v1.2.5 | Miura et al. (2024), Japan [55] | NA | Estimation of time reduction/patient: 90.0% (manual: 30.0 min vs. DLAS: 3.0 min) 1 | NA |
| RaySearch Laboratories AB | ||||
| RayStation v11B | De Kerf et al. (2023), Belgium [56] | NA | NA | No clinically relevant difference in doses to OARs between DLAS and manual contouring |
| Siemens Healthineers AG | ||||
| syngo.via RT Image Suite VB40 | Pera et al. (2023) [59], Germany and Spain | No/minor contour corrections required for 53.4%/42.0% of structures; no unusable contours | Mean time reduction/patient: 76.4% (manual: 34.7 min vs. DLAS: 8.2 min) | NA |
| AI-Rad Companion Organs RT VA30 | Yamauchi et al. (2024), Japan [60] | Mean contour score: prostate (3.3), SVs (3.5), bladder (3.7), and rectum (3.8) out of 4.0 (1 and 4 indicating major and no/minor corrections required) | Mean time reduction/patient: 5.7% (manual: 14.6 min vs. DLAS: 13.8 min) | NA |
| DirectORGANS VA30 | Berenato et al. (2024), Germany and UK [61] | NA | Median time reduction/patient: 41.3% (manual: 25.9 min vs. DLAS: 15.2 min) | No statistically significant difference in dose to bladder between DLAS and manual contouring; other OARs with statistically significant differences |
| Therapanacea | ||||
| Annotate ART-Plan v1.7.1 | Künzel et al. (2022), Germany [62] | No/minor corrections required for 54.0%/24.0% of OARs and 30.0%/36.0% of CTVs; no unusable OARs but 4.0% of unusable CTVs contours | NA | NA |
| Annotate ART-Plan v1.8.3 | Nachbar et al. (2024), France and Germany [63] | Mean contour score: prostate (2.0), SVs (1.5), anal canal (1.0), bladder (1.3), L (1.0) and R femurs (1.0), L (1.0) and R pelvis (1.2), penile bulb (1.1), rectum (1.2), and sacrum (1.0) out of 4.0 (1 and 4 indicating no corrections required and unusable), respectively | NA | NA |
| Varian Medical Systems, Inc. | ||||
| Ethos | Moazzezi et al. (2021), USA [64] | No/minor corrections required for 4.0% of structures/70.0%, 88.0%, and 90.0% of CTVs, bladder, and rectum, respectively. | NA | CTV coverage (D98 > 95%): 100%; no clinically relevant difference in doses to bladder and rectum between DLAS and manual contouring |
| Carina Medical LLC and RaySearch Laboratories AB | ||||
| INTContour and RayStation | Duan et al. (2025), USA [65] | No corrections required for 69.0% of prostate contours | NA | NA |
| Limbus AI Inc. and MVision.ai | ||||
| Contour v1.7.0-B3 and Contour+ v1.2.2 | Bordigoni et al. (2024), Italy and Sweden [66] | No/minor contour corrections required for 80.0%/20.0% (Limbus) and 60.0%/0.0% (MVision.ai) of structures; no unusable contours | Median time reduction/patient for Limbus/MVision.ai: 81.1%/80.2% (manual: 90.0 min vs. DLAS: 17.0/17.8 min) | NA |
| Carina Medical LLC, Manteia Medical Technologies Co., and MIM Software Inc. | ||||
| INTContour, AccuContour, and Contour ProtégéAI | Duan et al. (2023), USA [67] | No and minor corrections required for 80.0% of structures; unacceptable contours (unusable and major corrections required) delineated by finetuned model: 20.0% | NA | NA |
| Mirada Medical Ltd., MVision.ai, Radformation Inc., RaySearch Laboratories AB, and Therapanacea | ||||
| DLCExpert v2.6.4.47181, Contour+ v1.2.1, AutoContour v1.0.25.0, RayStation v12.0.0.932, and Annotate v1.10.0 | Doolan et al. (2023), Cyprus and Germany [68] | NA | Mean time reduction/patient for DLCExpert/Mvision Contour+/Radformation AutoContour/RayStation/Therapanacea Annotate: 82.4%/99.3%/89.8%/87.6%/99.8% (manual: 42.0 min vs. DLAS: 7.4/0.3/4.3/5.2/0.1 min) 2 | NA |
| Author, Year, and Country | DLAS Architecture | Study Design | Multi-Centre | Patient/Population | Model Finetuning | Training Dataset | Testing Dataset | Sample Size Calculation | External Testing | Modality | Reference Contour Source | Contouring Guidelines | Article Quality (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Source | Size (Number of Patient) | Source | Size (Number of Patient) | ||||||||||||
| Carina Medical LLC INTContour | |||||||||||||||
| Duan et al. (2022), USA [37] | 3D CNN U-Net | Retrospective | No | PCa patients | Yes | Private: 1 USA centre | 84 | Private: 1 USA centre | 23 | No | No | CT | 1 RO with final review by 2 ROs with >10-year experience | RTOG-0815 | 72 |
| Hobbis et al. (2023), USA [38] | 3D U-Net | Retrospective | No | Postprostatectomy PCa patients | Yes | Private: 1 USA centre for finetuned models | 120 for original model; 30, 60, and 90 for 3 finetuned models | Private: 1 USA centre | 49 | No | Only for original model | CT | 6 expert ROs | FROGG | 58 |
| Tegtmeier et al. (2024), USA [39] | 3D CNN U-Net | Retrospective | No | Intact and postprostatectomy PCa patients | Yes | Private: 2 USA centres | 84 for original model; 116 for finetuned model (72 intact and 44 postprostatectomy) | Private: 1 USA centre | 50 (25 intact and 25 postprostatectomy) | No | Only for original model | CBCT | 2 physicists and 2 physicians | ESTRO and FROGG | 60 |
| Elekta AB ADMIRE v3.4 | |||||||||||||||
| Jenkins et al. (2021), UK [40] | NA | Retrospective | No | Intermediate- and high-risk PCa patients | No | NA | NA | Private: 1 UK centre | 232 | No | Yes | CT | 1 RO | NA | 44 |
| Limbus AI Inc. Contour | |||||||||||||||
| Wong et al. (2020), Canada [41] | CNN U-Net | Retrospective | No | PCa patients without bilateral hip implants/rectal spacer | No | Public: USA TCIA | 328 | Private: 1 Canadian centre | 20 | No | Yes | CT | At least 2 expert ROs | RTOG | 56 |
| Wong et al. (2021), Canada [42] | CNN U-Net | Prospective | Yes | PCa patients | No | Public: USA TCIA | 328 | Private: 2 Canadian centres | 71 | No | Yes | CT | 1 RO | NA | 60 |
| Zabel et al. (2021), Canada [43] | CNN U-Net | Retrospective | No | PCa patients with 1 unilateral hip implant case | No | Public: USA TCIA | NA | Private: 1 Canadian centre | 15 | No | Yes | CT | 3 ROs | RTOG | 49 |
| Radici et al. (2022), Italy [44] | CNN U-Net | Prospective | No | PCa patients | No | Public: USA TCIA | At least hundreds | Private: 1 Italian centre | 3 | No | Yes | CT | 4 expert ROs | RTOG | 56 |
| Hoque et al. (2023), Italy [45] | CNN U-Net | Retrospective | No | PCa patients without bilateral hip implants/rectal spacer | No | Public: USA TCIA | 328 | Private: 1 Italian centre | 20 | No | Yes | CT | 1 RO with >10-year experience | ESTRO | 58 |
| Radici et al. (2024), Italy [46] | CNN U-Net | Retrospective | No | PCa patients | No | Public and private | NA | NA | 10 | No | NA | CT and CBCT | 4 expert ROs | NA | 42 |
| MIM Software Inc. Contour ProtégéAI | |||||||||||||||
| Urago et al. (2021), Japan [47] | U-Net | NA | No | PCa patients | No | Private: multi-centres over the world | 500–1000 | Private: 1 Japanese centre | 21 | No | Yes | CT | 3 ROs | NA | 40 |
| Palazzo et al. (2023), Italy [48] | U-Net | Retrospective | No | Intermediate- and high-risk PCa patients | No | Private: multi-centres | NA | Private: 1 Italian centre | 20 | No | Yes | CT | 2 ROs with >10-year experience | NA | 44 |
| Mirada Medical Ltd. DLCExpert | |||||||||||||||
| Walker et al. (2022), UK [49] | CNN | Retrospective | Yes | PCa patients | No | Private: 1 Dutch centre | 437 | Private: 3 UK centres | 61 | No | Yes | CT | 1 RT/RO | CHHiP and RTOG | 49 |
| Gibbons et al. (2023), Australia [50] | CNN | Retrospective | No | PCa patients without hip implant/rectal spacer | No | Private: 1 Dutch centre | 437 | Private: 1 Australian centre | 30 | No | Yes | CT | 1 expert RO | NA | 47 |
| Wang et al. (2023), USA [51] | 2D CNN U-Net | Retrospective | No | Intermediate- and high-risk PCa patients | Yes | Private: 1 USA centre | 135 | Private: 1 USA centre | Model 1 (24) and Model 2 (64) | No | No | CT | 3 expert ROs | RTOG-0815 | 47 |
| MVision.ai Contour+ | |||||||||||||||
| Kiljunen et al. (2020), Estonia, Finland, and Singapore [52] | Encoder-decoder-based CNN | Retrospective | Yes | PCa patients without any prostatectomy and femoral implant | No | Private: 3 centres | 900 | Private: 1 Estonian, 4 Finnish, and 1 Singaporean centres | 30 (5 from each centre) | No | Yes | CT | 3–4 dosimetrists, physicists, ROs and RTTs | NA | 42 |
| Olsson et al. (2022), Finland and Sweden [53] | Encoder-decoder-based CNN | Retrospective | No | PCa patients | Yes | Private: <40 centres for original model and 1 Swedish centre for finetuned model | 891 for original model; 325 for finetuned model | Private: 1 Swedish centre | 299 | No | Only for original model | CT | 1 researcher supervised by 1 senior RO | ESTRO and RTOG | 60 |
| Strolin et al. (2023), Italy [54] | Encoder-decoder-based CNN | Retrospective | No | PCa patients | No | Private: <40 centres | 891 | Private: 1 Italian centre | 20 | No | Yes | CT | 1 senior and 2 junior ROs with >10-year and 3-month experiences, respectively | ESTRO and RTOG | 56 |
| Miura et al. (2024), Japan [55] | Encoder-decoder-based CNN | NA | No | PCa patients without any iodine spacer, rectal balloon, and hip implant | No | Private: <40 centres | 891 | Private: 1 Japanese centre | 10 | No | Yes | CT | 1 5-year-experienced RO with final review by 2 ROs with >20-year experience | NA | 53 |
| RaySearch Laboratories AB RayStation | |||||||||||||||
| De Kerf et al. (2023), Belgium [56] | NA | Retrospective | NA | PCa patients | No | Private: Belgian Iridium Network centre(s) | NA | Private: Belgian Iridium Network centre(s) | 50 | No | No | CT | 1 experienced RO | NA | 40 |
| Kanwar et al. (2023), USA [57] | U-Net | Retrospective | No | PCa patients with normal anatomy and variations | No | NA | NA | Private: 1 USA centre | 131 (19 normal and 112 variants) | No | Yes | CT | 1 RO | In-house protocol | 58 |
| Siemens Healthineers AG AI-Rad Companion Organs RT/syngo. via RT Image Suite/DirectORGANS | |||||||||||||||
| Marschner et al. (2022), Germany and USA [58] | U-Net variant | NA | Yes | Prostate and cervical cancer patients | No | Private: multi-centres | 784 | 1 German centre | 102 | No | Yes | CT | 1 experienced RO | RTOG | 56 |
| Pera et al. (2023), Germany and Spain [59] | U-Net variant | NA | No | PCa patients | No | Private: multi-centres in Asia, Europe, and North and South America | At least hundreds | Private: 1 Spanish centre | 35 | No | Yes | CT | 1 expert RTT with final review by 1 RO | NA | 44 |
| Yamauchi et al. (2024), Japan [60] | U-Net variant | Retrospective | No | PCa patients with and without rectal spacer | No | Private: multi-centres in Europe and America | NA | Private: 1 Japanese centre | 30 (15 with spacer) | No | Yes | CT | 6 expert ROs | RTOG | 49 |
| Berenato et al. (2024), Germany and UK [61] | U-Net variant | Retrospective | No | Intermediate-risk PCa patients without any bilateral hip implants | No | NA | NA | Private: 1 UK centre | 20 (3 with single hip implant) | No | Yes | CT | 1 fully trained observer | RTOG | 58 |
| Therapanacea Annotate ART-Plan | |||||||||||||||
| Künzel et al. (2022), Germany [62] | NA | Retrospective | No | Intermediate-risk PCa patients | No | NA | NA | Private: 1 German centre | 10 | No | Yes | CT | NA | NA | 40 |
| Nachbar et al. (2024), France and Germany [63] | 3D CNN U-Net | Retrospective | No | PCa patients | Yes | Private: 1 German centre | 47 | Private: 1 German centre | 20 | No | No | MRI | 1 RO | NA | 58 |
| Varian Medical Systems, Inc. Ethos | |||||||||||||||
| Moazzezi et al. (2021), USA [64] | CNN U-Net | Retrospective | No | Intermediate-risk PCa patients without nodal involvement | No | Private: multi-centres in Americas, Asia, Australia, and Europe | Hundreds | Private: 1 USA centre | 25 | No | Yes | CBCT | 1 medical physicist with final review by 1 RO | NA | 53 |
| Carina Medical LLC INTContour and RaySearch Laboratories AB RayStation | |||||||||||||||
| Duan et al. (2025), USA [65] | 3D U-Net | Retrospective | No | Intact PCa patients | Yes | Private: 1 USA centre for INTContour | 84 for original model; 57 for finetuned model | Private: 1 USA centre | 37 for INTContour and RayStation original models; 54 for finetuned model | No | Only for original models | CT | Experienced ROs | ESTRO | 67 |
| Limbus AI Inc. Contour and MVision.ai Contour+ | |||||||||||||||
| Bordigoni et al. (2024), Italy and Sweden [66] | CNN U-Net | Retrospective | No | PCa patients | No | NA | NA | Private: 1 Italian centre | 20 | No | Yes | CT | 1 expert RO | NA | 51 |
| Carina Medical LLC INTContour, Manteia Medical Technologies Co. AccuContour, and MIM Software Inc. Contour ProtégéAI | |||||||||||||||
| Duan et al. (2023), USA [67] | 3D U-Net | NA | No | Intact PCa patients with and without iodine spacer/rectal balloon | Yes | Private: 1 USA centre for INTContour model finetuning | 100 | Private: 1 USA centre | 20 for INTContour, AccuContour, and ProtégéAI original models; 115 for INTContour finetuned model | No | Only for original models | CT | 1 dosimetrist and 6 expert ROs | NA | 53 |
| Mirada Medical Ltd. DLCExpert, MVision.ai Contour+, Radformation Inc. AutoContour, RaySearch Laboratories AB RayStation, and Therapanacea Annotate | |||||||||||||||
| Doolan et al. (2023), Cyprus and Germany [68] | NA | Retrospective | No | PCa patients | No | NA | NA | Private: 1 Cypriot centre | 20 | No | Yes | CT | 3 ROs with >10-year experience | Gay et al.’s [70] guidelines | 47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, C.K.C. Performance of Commercial Deep Learning-Based Auto-Segmentation Software for Prostate Cancer Radiation Therapy Planning: A Systematic Review. Information 2025, 16, 215. https://doi.org/10.3390/info16030215
Ng CKC. Performance of Commercial Deep Learning-Based Auto-Segmentation Software for Prostate Cancer Radiation Therapy Planning: A Systematic Review. Information. 2025; 16(3):215. https://doi.org/10.3390/info16030215
Chicago/Turabian StyleNg, Curtise K. C. 2025. "Performance of Commercial Deep Learning-Based Auto-Segmentation Software for Prostate Cancer Radiation Therapy Planning: A Systematic Review" Information 16, no. 3: 215. https://doi.org/10.3390/info16030215
APA StyleNg, C. K. C. (2025). Performance of Commercial Deep Learning-Based Auto-Segmentation Software for Prostate Cancer Radiation Therapy Planning: A Systematic Review. Information, 16(3), 215. https://doi.org/10.3390/info16030215