
A Scoping Review on Analysis of the Barriers and Support Factors of Open Data



Abstract
:1. Introduction
2. Open Data in Authorities, Companies, Research Institutions, and the Healthcare Sector
2.1. Authorities
2.2. Companies
2.3. Research Institutions
2.4. Healthcare Sector
3. Methodology
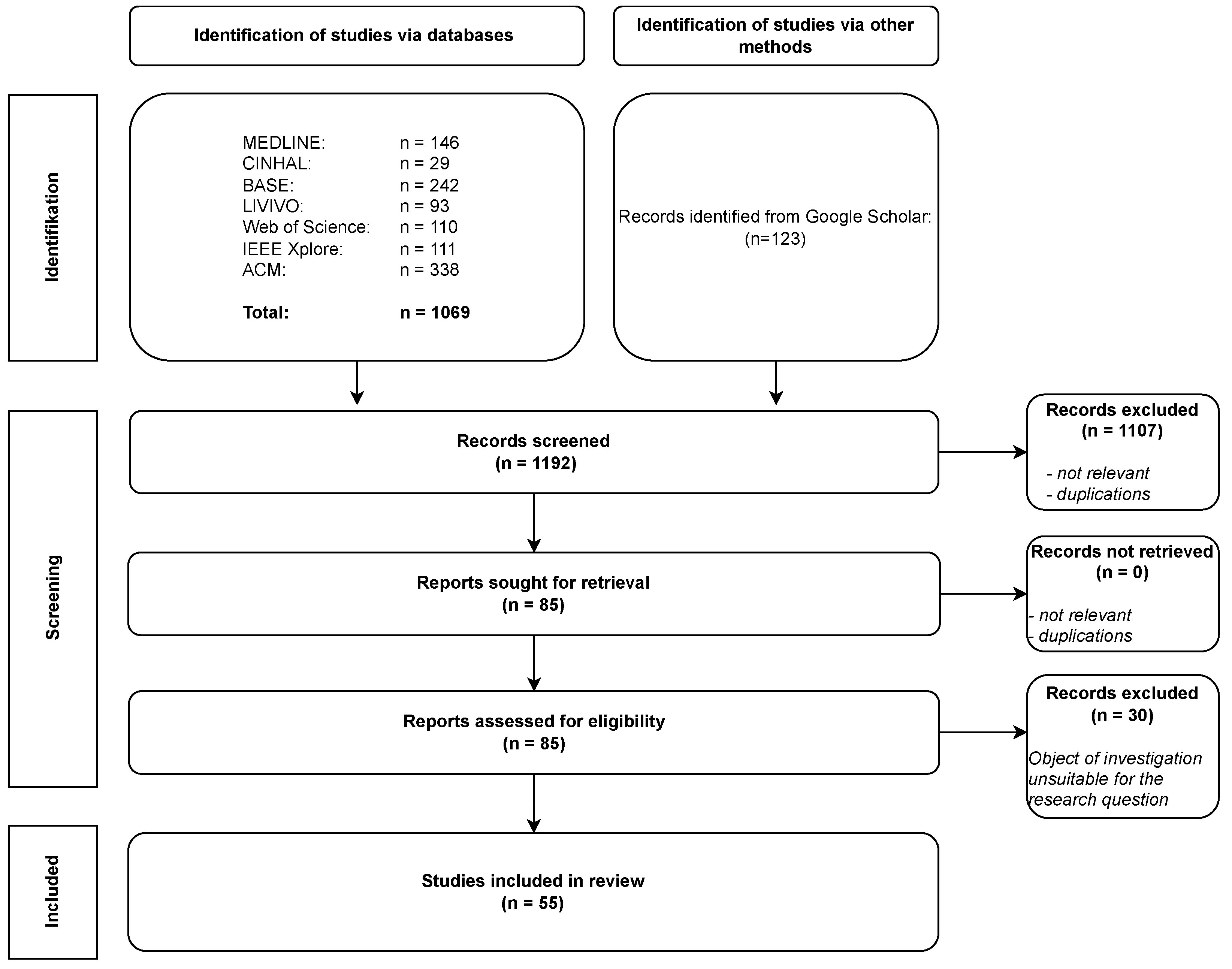
3.1. Systematic Research
- MEDLINE: One of the most extensive healthcare databases, providing a broad spectrum of content [37].
- CINAHL: Chosen to capture developments in healthcare, nursing, and therapy sciences.
- BASE: A meta-search engine encompassing disciplines such as computer science, information science, social sciences, health, medicine, and philosophy.
- Additionally, research encompassed cross-sectional databases, including LIVIVO, an interdisciplinary meta-search engine focused on life sciences, and the Web of Science Core Collection, a comprehensive database spanning various fields.
- The search was further augmented by investigating technical, information, and computer science databases: IEEE Xplore Digital Library, specializing in electrical engineering and information technology, and ACM Digital Library, primarily offering a full-text collection in computer science.
3.2. Search Strings
3.3. Evaluation of the Studies
4. Results
4.1. Barriers
4.1.1. ELSI
Ethical and Social Implications
Legal and Policy Implications
4.1.2. Personnel
4.1.3. Data Structure
4.1.4. Technical
4.1.5. Data Misuse
4.1.6. Clarification and Consent
4.1.7. Stigmatization
4.1.8. Institutional Barriers
4.1.9. Economic Barriers
4.1.10. Data Privacy
4.1.11. Commercial Interests
4.1.12. Trust
4.1.13. Communication
4.2. Support Factors
4.2.1. Positive Outcome
Public Sector/Public Authorities
Entrepreneurship
Research
Healthcare Sector
4.2.2. ELSI
Ethical Implications
Social Implications
Law and Policy
4.2.3. Technical Infrastructure
4.2.4. Data Access
4.2.5. Education and Training
4.2.6. Personnel Aspects
4.2.7. Data Structure
4.2.8. Trust
4.2.9. Consent Procedures
4.2.10. Collaborations
4.2.11. Communication
4.2.12. Economic Aspects
4.2.13. Institutional Aspects
4.2.14. Participation
5. Conclusions
6. Summary
- Data Privacy and Legal FrameworksIn the context of data privacy and legal frameworks, it is evident that the use of Open Data, especially personally identifiable information, relies on a robust legal foundation and a clear ethical framework. The European General Data Protection Regulation (GDPR) has undoubtedly contributed to harmonizing and enhancing data portability across Europe, yet challenges persist in its full implementation [25]. Data privacy, particularly in healthcare, continues to be perceived as one of the most significant barriers [64]. The GDPR, applicable throughout Europe, aims to safeguard personal data comprehensively and establish global standards for managing such data [65]. Furthermore, it has been complemented by the EU Data Governance Act (DGA), designed to promote the broader use of personal data and foster data altruism across Europe [65]. However, due to the ongoing developments in the field of Open Data, existing regulations for personal data protection are increasingly scrutinized [59].Addressing these challenges necessitates compliance with existing data protection regulations and the establishment of new legal frameworks capable of adapting to the evolving landscape of Open Data. Given the continuous advancements in the field of Open Data, the existing regulations for personal data protection are increasingly questioned [59]. So far, the EU GDPR and the EU proposals regarding regulations for using artificial intelligence represent some of the few mechanisms that encompass responsible regulation, which may not suffice in all cases [30]. Furthermore, developing specific data usage policies, particularly in health research data, is essential [6].
- Ethics and TrustEnsuring society’s trust in the handling of personal data and the strict adherence to ethical principles are fundamental requirements for Open Data. Transparency regarding data usage, especially when dealing with sensitive health data, is crucial in establishing this trust.The European Ethic Advisory Board underscores the need for a new digital ethics framework, given the challenges and disruptions caused by the increasing use of data streams, which are difficult to predict. The inseparable connection between individuals and their personal data is emphasized [43]. This emphasis necessitates a broad discourse on managing health data, considering expectations of security and privacy associated with a wide range of uses and applications [30].Another focal point of this discussion is the integrity and accountability in data handling, including data loss prevention and the accountability for adding data during processing and utilization [56]. Building trust in data exchange processes and shaping a societal data-sharing contract is pivotal. Both technological solutions and ethical principles must align to create the necessary trust and promote the societal acceptance of Open Data usage [29].
- ResourcesAdequate financial and human resources are essential for the collection, maintenance, and dissemination of Open Data [11,18]. Without sufficient funding and skilled personnel, data quality and accessibility can suffer, hindering the realization of Open Data’s full potential [46,61]. Moreover, long-term sustainability strategies are crucial to ensure that Open Data initiatives continue to evolve and meet the changing needs of their stakeholders. By allocating resources effectively, organizations can maximize the benefits of Open Data while addressing the challenges associated with data governance, privacy, and security. Developing a clear roadmap for resource allocation and sustainability is vital for Open Data efforts’ continued growth and success [52].
- Interoperability and StandardsIn the realm of Open Data processes, standards, guidelines, and professional associations also have a critical role to play. Examples of freely accessible databases developed using a multidisciplinary approach are presented [28]. Data aggregation into centralized databases, such as the Database of Genotypes and Phenotypes of the US National Institutes of Health and the European Genomic Phenome Archive, can offer solutions to interoperability challenges [27]. Promoting standards and guidelines for Open Data fosters a more unified and efficient data-sharing environment. This, in turn, enhances collaboration among diverse stakeholders and ensures the quality and utility of data for research, industries, and data-driven decision making.
- Evaluation and ReviewIt is imperative to identify and select appropriate data before release meticulously. Following this selection process, the decision to publish should be made with continuous evaluation of the impact and utility of the data. This process is a cyclical approach [13]. The entire approach to Open Data should be measured by its success, with data-driven applications aimed at enabling improved health outcomes, preventive measures, and forecasts [24].The comprehensive utilization of data necessitates a thorough evaluation [13] and ongoing audits and reviews of the associated processes [46]. Furthermore, there is an urgent requirement for tools and a step-by-step model to guide stakeholders, such as hospitals, in this process, ensuring that data are structured and organized following the FAIR principles (Findable, Accessible, Interoperable, Reusable) [6].
7. Limitations
- Lack of systematic risk assessment (risk of bias assessment): A systematic risk assessment was not carried out as part of this Scoping Review. Consequently, it is impossible to ascertain the risk of overestimating or underestimating the effects and results of the selected studies.
- Quality of selected studies: Despite carefully selecting and reviewing studies, some studies might have been erroneously considered relevant to Open Data. Including such studies could have implications for the results of Open Data.
- Limited search coverage: The search strategy primarily relied on seven databases supplemented with Google Scholar searches. Using only these sources may have led to the omission of some relevant studies, further emphasizing the limitations of the search. This study may not encompass all relevant synonyms and terms associated with Open Data.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ELSI | Ethical, Legal, and Social Implications |
| EOSC | European Open Science Cloud |
| FAIR | Findable, Accessible, Interoperable, Reusable |
| OGD | Open Governance Data |
| OUR | Open, Useful, Reusable |
Appendix A

{kind=link}
| Database | Search String |
|---|---|
| MEDLINEvia PubMed | (“personal data” OR “personal information” OR “person-related data” OR “personal identification information” OR “patient Data”) AND (barriers OR challenges OR obstacles OR impediments OR hindrances OR hurdle) AND (promotion OR support OR enabling OR opportunities OR incentives) AND (“data sharing” OR “data provision” OR “providing data” OR “data supply” OR “data publishing”) AND (y_5[Filter]) |
| CINAHLvia EBSCOhost | ((“personal data” OR “personal information” OR “person-related data” OR “personal identification information” OR “patient Data”)) AND (barriers OR challenges OR obstacles OR impediments OR hindrances OR hurdle)) AND ((promotion OR support OR enabling OR opportunities OR incentives)) AND ((“data sharing” OR “data provision” OR “providing data” OR “data supply” OR “data publishing”)) |
| BASE | (“personal data” OR “personal information” OR “person-related data” OR “personal identification information” OR “patient Data”) AND (open data” OR “open information” OR “open science”) AND (“data sharing” OR “data provision” OR “providing data” OR “data supply” OR “data publishing”) AND (barriers OR challenges OR obstacles OR impediments OR hindrances OR hurdle) AND (promotion OR support OR enabling OR opportunities OR incentives) year: [2018 TO *] |
| LIVIVO | ((((“personal data” OR “personal information” OR “person-related data” OR “personal identification information” OR “patient Data”)) AND TI = ((barriers OR challenges OR obstacles OR impediments OR hindrances OR hurdle) AND (promotion OR support OR enabling OR opportunities OR incentives))) AND TI = ((“data sharing” OR “data provision” OR “providing data” OR “data supply” OR “data publishing”) AND (“open data” OR “open information” OR “open science”))) AND PY = 2018: |
| Web of Science Core Collection | ((((#1) AND ALL = ((“personal data” OR “personal information” OR “person-related data” OR “personal identification information” OR “patient Data”))) AND ALL = ((barriers OR challenges OR obstacles OR impediments OR hindrances OR hurdle))) AND ALL = ((promotion OR support OR enabling OR opportunities OR incentives))) AND ALL = ((“data sharing” OR “data provision” OR “providing data” OR “data supply” OR “data publishing”)) and 2023 or 2022 or 2021 or 2018 or 2019 or 2020 (Publication Years) |
| IEEE Xplore Digital Library | (((“All Metadata”:“personal data” OR “All Metadata”:“personal information” OR “All Metadata”:“person-related data” OR “All Metadata”:“personal identification information” OR “All Metadata”:“patient data”) AND (“All Metadata”:barriers OR “All Metadata”:challenges OR “All Metadata”:obstacles OR “All Metadata”:impediments OR “All Metadata”:hindrances OR “All Metadata”:hurdle)) AND(“All Metadata”:promotion OR “All Metadata”:support OR “All Metadata”:enabling OR “All Metadata”:opportunities OR “All Metadata”:incentives) AND (“All Metadata”:“data sharing” OR “All Metadata”:“data provision” OR “All Metadata”:“providing data” OR “All Metadata”:“data supply” OR “All Metadata”:“data publishing”) AND (“All Metadata”:“open data” OR “All Metadata”:“open information” OR “All Metadata”:“open science”)) |
| ACM Digital Library | 333 Results for: [[All: “personal data”] OR [All: “personal information”] OR [All: “person-related data”] OR [All: “personal identification information”] OR [All: “patient data”]] AND [[All: barriers] OR [All: challenges] OR [All: obstacles] OR [All: impediments] OR [All: hindrances] OR [All: hurdle]] AND [[All: promotion] OR [All: support] OR [All: enabling] OR [All: opportunities] OR [All: incentives]] AND [[All: “data sharing”] OR [All: “data provision”] OR [All: “providing data”] OR [All: “data supply”] OR [All: “data publishing”]] AND [[All: “open data”] OR [All: “open information”] OR [All: “open science”]] AND [E-Publication Date: (01/01/2018 TO 12/31/2023)] |
Appendix B
| Nr. | Search String | MEDLINE | CINAHL | BASE | LIVIVO | Web of Science | IEEE Xplore | ACM | |
|---|---|---|---|---|---|---|---|---|---|
| Date | 1 June 2023 | 5 June 2023 | 5 June 2023 | 7 June 2023 | 7 June 2023 | 9 June 2023 | 12 June 2023 | ||
| 1 | Personal Data | (“personal data” OR “personal information” OR “person-related data” OR “personal identification information” OR “patient Data”) | 12,741 | 4,301 | 182,713 | 14,463 | 19,338 | 8405 | 21,662 |
| 2 | Barriers | (barriers OR challenges OR obstacles OR impediments OR hindrances OR hurdle) | 658,970 | 133,618 | 1,783,959 | 1,056,699 | 1,411,084 | 217,496 | 340,022 |
| 3 | Support factors | (promotion OR support OR enabling OR opportunities OR incentives) | 2,752,603 | 261,118 | 3,441,003 | 1,664,052 | 3,982,684 | 290,271 | 488,208 |
| 4 | Providing Data | (“data sharing” OR “data provision” OR “providing data” OR “data supply” OR “data publishing”) | 5198 | 10,961 | 58,194 | 6813 | 15,972 | 433,303 | 13,625 |
| 5 | Open Data | (“open data” OR “open information” OR “open science”) | 4428 | 696 | 475,197 | 16,229 | 15,464 | 177,906 | 7187 |
| 6 | 1+2 | Personal Data + Barriers | 1505 | 361 | 15,540 | - | - | 766 | 16,433 |
| 7 | 1 + 2 + 3 | Personal Data + Barriers + support factors | 942 | 146 | - | - | - | 250 | 15,950 |
| 8 | 1 + 2 + 3 + 4 | Personal Data + Barriers + support factors + providing Data | 66 | 11 | - | 47 | 81 | 74 | 2614 |
| 9 | 1 + 2 + 3 + 4 + 5 | Personal Data + Barriers + support factors + providing Data + Open Data | 5 | 1 | 242 | 8 | 8 | 37 | 338 |
| 10 | 1 + 3 | Personal Data + support factors | - | - | - | - | - | - | - |
| 11 | 1 + 4 | Personal Data + providing Data | 264 | - | - | - | - | - | - |
| 12 | 1 + 4 + 2 | Personal Data + providing Data + Barriers | - | - | - | - | - | - | - |
| 13 | 1 + 4 + 3 | Personal Data + providing Data + support factors | - | - | - | - | - | - | - |
| 14 | 1 + 4 + 5 | Personal Data + providing Data + Open Data | 22 | - | 1.937 | 27 | 21 | - | - |
| 15 | 1 + 4 + 5 + 2 | Personal Data + providing Data + Open Data + Barriers | - | - | 440 | 11 | - | - | - |
| 16 | 1 + 4 + 5 + 3 | Personal Data + providing Data + Open Data + support factors | - | - | - | - | - | - | - |
| 17 | 1 + 5 | Personal Data + Open Data | 56 | 17 | 61.833 | - | - | - | - |
| 18 | 1 + 5 + 2 | Personal Data + Open Data + Barriers | 15 | - | - | - | - | - | - |
| 19 | 1 + 5 + 3 | Personal Data + Open Data + support factors | 38 | - | - | - | - | - | - |
| 20 | 1 + 5 + 2 + 3 | Personal Data + Open Data + support factors + Barriers | - | - | - | - | - | - | - |
| total | studies (n)/Database | 146 | 29 | 242 | 93 | 110 | 111 | 338 |
References
- Kamikubo, R.; Lee, K.; Kacorri, H. Contributing to Accessibility Datasets: Reflections on Sharing Study Data by Blind People. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems, Hamburg, Germany, 23–28 April 2023. [Google Scholar] [CrossRef]
- Rehman, A.; Naz, S.; Razzak, I. Leveraging big data analytics in healthcare enhancement: Trends, challenges and opportunities. Multimed. Syst. 2022, 28, 1339–1371. [Google Scholar] [CrossRef]
- Ethikrat, D. Big Data und Gesundheit: Datensouveränität als Informationelle Freiheitsgestaltung: Stellungnahme: Kurzfassung; Bundesministerium für Gesundheit: Bonn, Germany, 2017. [Google Scholar]
- Sleigh, J. Experiences of Donating Personal Data to Mental Health Research: An Explorative Anthropological Study. Biomed. Inform. Insights 2018, 10, 1178222618785131. [Google Scholar] [CrossRef] [PubMed]
- Dove, G.; Shanley, J.; Matuk, C.; Nov, O. Open Data Intermediaries: Motivations, Barriers and Facilitators to Engagement. Proc. ACM Hum.-Comput. Interact. 2023, 7, 1–22. [Google Scholar] [CrossRef]
- Queralt-Rosinach, N.; Kaliyaperumal, R.; Bernabé, C.H.; Long, Q.; Joosten, S.A.; van der Wijk, H.J.; Flikkenschild, E.L.A.; Burger, K.; Jacobsen, A.; Mons, B.; et al. Applying the FAIR principles to data in a hospital: Challenges and opportunities in a pandemic. J. Biomed. Semant. 2022, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Roguljić, M.; Šimunović, D.; Poklepović Peričić, T.; Viđak, M.; Utrobičić, A.; Marušić, M.; Marušić, A. Publishing Identifiable Patient Photographs in Scientific Journals: Scoping Review of Policies and Practices. J. Med. Internet Res. 2022, 24, e37594. [Google Scholar] [CrossRef] [PubMed]
- Rempel, E.; Barnett, J.; Durrant, H. Contrasting views of public engagement on local government data use in the UK. In Proceedings of the 12th International Conference on Theory and Practice of Electronic Governance, Melbourne, Australia, 3–5 April 2019; Ben Dhaou, S., Ed.; ACM Digital Library: New York, NY, USA, 2019; pp. 118–128. [Google Scholar] [CrossRef]
- Seo, J.; Kim, B.; Kwon, H.Y. Open Data Policies Analysis Disputes Mediation Cases in Korea: Based on OUR Data Index and ODB. In Proceedings of the DG.O2021: The 22nd Annual International Conference on Digital Government Research, Omaha, NE, USA, 9–11 June 2021; ACM Digital Library: New York, NY, USA, 2021; pp. 153–167. [Google Scholar] [CrossRef]
- Mutambik, I.; Nikiforova, A.; Almuqrin, A.; Liu, Y.D.; Floos, A.Y.M.; Omar, T. Benefits of Open Government Data Initiatives in Saudi Arabia and Barriers to Their Implementation. J. Glob. Inf. Manag. 2022, 29, 1–22. [Google Scholar] [CrossRef]
- Kawashita, I.; Baptista, A.A.; Soares, D. Open Government Data Use by the Public Sector—An Overview of its Benefits, Barriers, Drivers, and Enablers. In Proceedings of the 55th Hawaii International Conference on System Sciences, Maui, HI, USA, 4–7 January 2022. [Google Scholar]
- Smith, G.; Sandberg, J. Barriers to innovating with open government data: Exploring experiences across service phases and user types. Inf. Polity 2018, 23, 249–265. [Google Scholar] [CrossRef]
- Crusoe, J.; Melin, U. Investigating Open Government Data Barriers; Springer: Cham, Switerland, 2018; pp. 169–183. [Google Scholar] [CrossRef]
- Csányi, G.M.; Nagy, D.; Vági, R.; Vadász, J.P.; Orosz, T. Challenges and Open Problems of Legal Document Anonymization. Symmetry 2021, 13, 1490. [Google Scholar] [CrossRef]
- van Donge, W.; Bharosa, N.; Janssen, M.F.W.H.A. Future government data strategies: Data-driven enterprise or data steward? In Proceedings of the 21st Annual International Conference on Digital Government Research, Seoul, Republic of Korea, 15–19 June 2020; Eom, S.J., Ed.; ACM Digital Library: New York, NY, USA, 2020; pp. 196–204. [Google Scholar] [CrossRef]
- Pesqueira, A.; Sousa, M.J.; Rocha, Á. Big Data Skills Sustainable Development in Healthcare and Pharmaceuticals. J. Med. Syst. 2020, 44, 197. [Google Scholar] [CrossRef]
- Dos Santos Rocha, A.; Albrecht, E.; El-Boghdadly, K. Open science should be a pleonasm. Anaesthesia 2023, 78, 551–556. [Google Scholar] [CrossRef]
- Eva, G.; Liese, G.; Stephanie, B.; Petr, H.; Leslie, M.; Roel, V.; Martine, V.; Sergi, B.; Mette, H.; Sarah, J.; et al. Position paper on management of personal data in environment and health research in Europe. Environ. Int. 2022, 165, 107334. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, A.G.; Alhomoud, A.; Wills, G. A Framework of the Critical Factors for Healthcare Providers to Share Data Securely Using Blockchain. IEEE Access 2022, 10, 41064–41077. [Google Scholar] [CrossRef]
- Phillips, M.; Knoppers, B.M. Whose Commons? Data Protection as a Legal Limit of Open Science. J. Law Med. Ethics 2019, 47, 106–111. [Google Scholar] [CrossRef]
- Medley, N.; Cuthbert, A.; Crew, R.; Stewart, L.; Smith, C.T.; Alfirevic, Z. Developing a topic-based repository of clinical trial individual patient data: Experiences and lessons learned from a pilot project. Syst. Rev. 2021, 10, 162. [Google Scholar] [CrossRef]
- Zuiderwijk, A.; Spiers, H. Sharing and re-using open data: A case study of motivations in astrophysics. Int. J. Inf. Manag. 2019, 49, 228–241. [Google Scholar] [CrossRef]
- Schwalbe, N.; Wahl, B.; Song, J.; Lehtimaki, S. Data Sharing and Global Public Health: Defining What We Mean by Data. Front. Digit. Health 2020, 2, 612339. [Google Scholar] [CrossRef] [PubMed]
- Horn, R.; Kerasidou, A. Sharing whilst caring: Solidarity and public trust in a data-driven healthcare system. BMC Med. Ethics 2020, 21, 110. [Google Scholar] [CrossRef]
- Feeney, O.; Werner-Felmayer, G.; Siipi, H.; Frischhut, M.; Zullo, S.; Barteczko, U.; ∅ystein Ursin, L.; Linn, S.; Felzmann, H.; Krajnović, D.; et al. European Electronic Personal Health Records initiatives and vulnerable migrants: A need for greater ethical, legal and social safeguards. Dev. World Bioeth. 2020, 20, 27–37. [Google Scholar] [CrossRef]
- Bentzen, H.B.; Castro, R.; Fears, R.; Griffin, G.; ter Meulen, V.; Ursin, G. Remove obstacles to sharing health data with researchers outside of the European Union. Nat. Med. 2021, 27, 1329–1333. [Google Scholar] [CrossRef]
- Hallock, H.; Marshall, S.E.; ’t Hoen, P.A.C.; Nygård, J.F.; Hoorne, B.; Fox, C.; Alagaratnam, S. Federated Networks for Distributed Analysis of Health Data. Front. Public Health 2021, 9, 712569. [Google Scholar] [CrossRef]
- Thoral, P.J.; Peppink, J.M.; Driessen, R.H.; Sijbrands, E.J.G.; Kompanje, E.J.O.; Kaplan, L.; Bailey, H.; Kesecioglu, J.; Cecconi, M.; Churpek, M.; et al. Sharing ICU Patient Data Responsibly Under the Society of Critical Care Medicine/European Society of Intensive Care Medicine Joint Data Science Collaboration: The Amsterdam University Medical Centers Database (AmsterdamUMCdb) Example. Crit. Care Med. 2021, 49, e563–e577. [Google Scholar] [CrossRef]
- Fylan, F.; Fylan, B. Co-creating social licence for sharing health and care data. Int. J. Med. Inform. 2021, 149, 104439. [Google Scholar] [CrossRef] [PubMed]
- Johansson, J.V.; Bentzen, H.B.; Mascalzoni, D. What ethical approaches are used by scientists when sharing health data? An interview study. BMC Med. Ethics 2022, 23, 41. [Google Scholar] [CrossRef]
- Deist, T.M.; Dankers, F.J.W.M.; Ojha, P.; Scott Marshall, M.; Janssen, T.; Faivre-Finn, C.; Masciocchi, C.; Valentini, V.; Wang, J.; Chen, J.; et al. Distributed learning on 20,000+ lung cancer patients—The Personal Health Train. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2020, 144, 189–200. [Google Scholar] [CrossRef] [PubMed]
- McWhirter, R.; Eckstein, L.; Chalmers, D.; Critchley, C.; Nielsen, J.; Otlowski, M.; Nicol, D. A Scenario-Based Methodology for Analyzing the Ethical, Legal, and Social Issues in Genomic Data Sharing. J. Empir. Res. Hum. Res. Ethics JERHRE 2020, 15, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Kuo, T.T.; Jiang, X.; Tang, H.; Wang, X.; Harmanci, A.; Kim, M.; Post, K.; Bu, D.; Bath, T.; Kim, J.; et al. The evolving privacy and security concerns for genomic data analysis and sharing as observed from the iDASH competition. J. Am. Med. Inform. Assoc. JAMIA 2022, 29, 2182–2190. [Google Scholar] [CrossRef]
- Nellåker, C.; Alkuraya, F.S.; Baynam, G.; Bernier, R.A.; Bernier, F.P.J.; Boulanger, V.; Brudno, M.; Brunner, H.G.; Clayton-Smith, J.; Cogné, B.; et al. Enabling Global Clinical Collaborations on Identifiable Patient Data: The Minerva Initiative. Front. Genet. 2019, 10, 611. [Google Scholar] [CrossRef]
- Scheibner, J.; Raisaro, J.L.; Troncoso-Pastoriza, J.R.; Ienca, M.; Fellay, J.; Vayena, E.; Hubaux, J.P. Revolutionizing Medical Data Sharing Using Advanced Privacy-Enhancing Technologies: Technical, Legal, and Ethical Synthesis. J. Med. Internet Res. 2021, 23, e25120. [Google Scholar] [CrossRef]
- Househ, M.; Grainger, R.; Petersen, C.; Bamidis, P.; Merolli, M. Balancing between Privacy and Patient Needs for Health Information in the Age of Participatory Health and Social Media: A Scoping Review. Yearb. Med. Inform. 2018, 27, 29–36. [Google Scholar] [CrossRef]
- Nordhausen und Hirt. 10 Schritte zur systematischen Literaturrecherche. RefHunter—Systematische Literaturrecherche. 2022. Available online: https://refhunter.org/research_support/rechercheschritte/ (accessed on 22 November 2023).
- Davies, K.S. Formulating the Evidence Based Practice Question: A Review of the Frameworks. Evid. Based Libr. Inf. Pract. 2011, 6, 75–80. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Aleixandre-Benavent, R.; Vidal-Infer, A.; Alonso-Arroyo, A.; Peset, F.; Ferrer Sapena, A. Research Data Sharing in Spain: Exploring Determinants, Practices, and Perceptions. Data 2020, 5, 29. [Google Scholar] [CrossRef]
- Alorwu, A.; Kheirinejad, S.; van Berkel, N.; Kinnula, M.; Ferreira, D.; Visuri, A.; Hosio, S. Assessing MyData Scenarios: Ethics, Concerns, and the Promise. In Proceedings of the CHI’21, 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; Kitamura, Y., Quigley, A., Isbister, K., Igarashi, T., Bjørn, P., Drucker, S., Eds.; Association for Computing Machinery: New York, NY, USA, 2021; pp. 1–11. [Google Scholar] [CrossRef]
- Broes, S.; Lacombe, D.; Verlinden, M.; Huys, I. Toward a Tiered Model to Share Clinical Trial Data and Samples in Precision Oncology. Front. Med. 2018, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.P.; Floridi, L.; Pols, A.; van den Hoven, J. Towards a Digital Ethics: EDPS Ethics Advisory Group. 2018. Available online: https://philpapers.org/rec/BURTAD-3 (accessed on 22 November 2023).
- Fischer, C.; Hirsbrunner, S.D.; Teckentrup, V. Producing Open Data; Pensoft Publishers: Sofia, Bulgaria, 2022; Volume 8, p. e86384. [Google Scholar] [CrossRef]
- Fischer-Hübner, S.; Alcaraz, C.; Ferreira, A.; Fernandez-Gago, C.; Lopez, J.; Markatos, E.; Islami, L.; Akil, M. Stakeholder perspectives and requirements on cybersecurity in Europe. J. Inf. Secur. Appl. 2021, 61, 102916. [Google Scholar] [CrossRef]
- Floridi, L.; Luetge, C.; Pagallo, U.; Schafer, B.; Valcke, P.; Vayena, E.; Addison, J.; Hughes, N.; Lea, N.; Sage, C.; et al. Key Ethical Challenges in the European Medical Information Framework. Minds Mach. 2019, 29, 355–371. [Google Scholar] [CrossRef]
- Galdon Clavell, G. Exploring the ethical, organisational and technological challenges of crime mapping: A critical approach to urban safety technologies. Ethics Inf. Technol. 2018, 20, 265–277. [Google Scholar] [CrossRef]
- Kwon, S.; Motohashi, K. Incentive or disincentive for research data disclosure? A large-scale empirical analysis and implications for open science policy. Int. J. Inf. Manag. 2021, 60, 102371. [Google Scholar] [CrossRef]
- Mahomed, S.; Labuschaigne, M.L. The evolving role of research ethics committees in the era of open data. S. Afr. J. Bioeth. Law 2023, 15, 80–83. [Google Scholar] [CrossRef]
- Nunes Vilaza, G.; Coyle, D.; Bardram, J.E. Public Attitudes to Digital Health Research Repositories: Cross-sectional International Survey. J. Med. Internet Res. 2021, 23, e31294. [Google Scholar] [CrossRef]
- Papageorgiou, V.; Wharton-Smith, A.; Campos-Matos, I.; Ward, H. Patient data-sharing for immigration enforcement: A qualitative study of healthcare providers in England. BMJ Open 2020, 10, e033202. [Google Scholar] [CrossRef]
- Rockhold, F.; Bromley, C.; Wagner, E.K.; Buyse, M. Open science: The open clinical trials data journey. Clin. Trials (Lond. Engl.) 2019, 16, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Sandoval-Almazan, R.; Valle Gonzalez, L.; Millan Vargas, A. Barriers for Open Government Implementation at Municipal Level: The Case of the State of Mexico. In Proceedings of the DG.O2021: The 22nd Annual International Conference on Digital Government Research, Omaha, NE, USA, 9–11 June 2021; ACM Digital Library: New York, NY, USA, 2021; pp. 113–122. [Google Scholar] [CrossRef]
- Smart, D.; Jackson, K.; Alderson, H.; Foley, T.; Foreman, S.; Kaner, B.; Kaner, E.; Lancaster, H.; Lingam, R.; Rankin, J.; et al. What Influences Parents and Practitioners’ Decisions to Share Personal Information within an Early Help (Social Care) Context? Implications for Practice in Sharing Digital Data across Sectors. Br. J. Soc. Work 2022, 52, 2146–2165. [Google Scholar] [CrossRef]
- Tan, A.C.; Askie, L.M.; Hunter, K.E.; Barba, A.; Simes, R.J.; Seidler, A.L. Data sharing-trialists’ plans at registration, attitudes, barriers and facilitators: A cohort study and cross-sectional survey. Res. Synth. Methods 2021, 12, 641–657. [Google Scholar] [CrossRef] [PubMed]
- Tuler de Oliveira, M.; Amorim Reis, L.H.; Marquering, H.; Zwinderman, A.H.; Delgado Olabarriaga, S. Perceptions of a Secure Cloud-Based Solution for Data Sharing During Acute Stroke Care: Qualitative Interview Study. JMIR Form. Res. 2022, 6, e40061. [Google Scholar] [CrossRef] [PubMed]
- van der Burg, S.; Wiseman, L.; Krkeljas, J. Trust in farm data sharing: Reflections on the EU code of conduct for agricultural data sharing. Ethics Inf. Technol. 2021, 23, 185–198. [Google Scholar] [CrossRef]
- Vianen, N.J.; Maissan, I.M.; den Hartog, D.; Stolker, R.J.; Houmes, R.J.; Gommers, D.A.M.P.J.; van Meeteren, N.L.U.; Hoeks, S.E.; van Lieshout, E.M.M.; Verhofstad, M.H.J.; et al. Opportunities and barriers for prehospital emergency medical services research in the Netherlands; results of a mixed-methods consensus study. Eur. J. Trauma Emerg. Surg. 2023. [Google Scholar] [CrossRef]
- Wang, C.; Guo, F.; Ji, M. Analysis of Legal Issues of Personal Information Protection in the Field of Big Data. J. Environ. Public Health 2022, 2022, 1678360. [Google Scholar] [CrossRef]
- Wieczorkowski, J. Barriers to Using Open Government Data. In Proceedings of the 2019 3rd International Conference on E-commerce, E-Business and E-Government, Lyon, France, 18–21 June 2019; ACM Digital Library: New York, NY, USA, 2019; pp. 15–20. [Google Scholar] [CrossRef]
- Wolff, A.; Tylosky, N.; Hasan, T. Open Data Inclusion through Narrative Approaches. In Proceedings of the 2022 IEEE/ACM 44th International Conference on Software Engineering: Software Engineering in Society (ICSE-SEIS), Pittsburgh, PA, USA, 21–29 May 2022; pp. 125–129. [Google Scholar] [CrossRef]
- Yerden, X.; Luna-Reyes, L.F. Promoting Government Impacts through Open Data: Key Influential Factors. In Proceedings of the DG.O2021: The 22nd Annual International Conference on Digital Government Research, Omaha, NE, USA, 9–11 June 2021; ACM Digital Library: New York, NY, USA, 2021; pp. 180–188. [Google Scholar] [CrossRef]
- Smart, M.A.; Sood, D.; Vaccaro, K. Understanding Risks of Privacy Theater with Differential Privacy. Proc. ACM Hum.-Comput. Interact. 2022, 6, 1–24. [Google Scholar] [CrossRef]
- Avraam, D.; Jones, E.; Burton, P. A deterministic approach for protecting privacy in sensitive personal data. BMC Med. Inform. Decis. Mak. 2022, 22, 24. [Google Scholar] [CrossRef]
- Kamocki, P.; Linden, K. EU Data Governance Act: New Opportunities and New Challenges for CLARIN. In Proceedings of the CLARIN Annual Conference Proceedings, Prague, Czech Republic, 10–12 October 2022; pp. 44–47. [Google Scholar]
| P | Personal data |
| I | Barriers and support factors |
| C | - |
| O | Provision of persona data as Open Data |
| Search Components | Personal Data | Barriers | Support Factors | Providing Data | Open Data |
|---|---|---|---|---|---|
| (Population) | (Intervention) | (Intervention) | (Outcome) | (Outcome) | |
| Synonyms | Personal Data, Personal Information, Person-related Data, Personal Identification Information, Patient Data | Barriers, Challenges, Obstacles, Impediments, Hindrances, Hurdle | Promotion, Support, Enabling, Opportunities, Incentives | Data Sharing, Data Provision, Providing Data, Data Supply, Data Publishing | Open Data, Open Information, Open Science |
| Search Component | Search String |
|---|---|
| 1—Personal Data (P) | (“personal data” OR “personal information” OR “person-related data” OR “personal identification information” OR “patient data”) |
| 2—Barriers (I) | (barriers OR challenges OR obstacles OR impediments OR hindrances OR hurdle) |
| 3—Support factors (I) | (promotion OR support OR enabling OR opportunities OR incentives) |
| 4—Providing Data (O) | (“data sharing” OR “data provision” OR “providing data” OR “data supply” OR “data publishing”) |
| 5—Open Data (O) | (“open data” OR “open information” OR “open science”) |
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Language | English, German | Other Languages |
| Date of Publication | Published as of 2018, as 2018 GDPR was used as a benchmark at the European Level | Published before 2018 |
| Type of Publication | Original Papers, Reviews, Systematic Reviews | Case Studies, Opinion Articles |
| Author | Focus | Barriers | Supporting Factors | |
|---|---|---|---|---|
| Aleixandre-Benavent et al. | [40] | Research Data Sharing | ELSI; Personnel barriers; data misuse; institutional barriers; | education and training; participation |
| Alorwu et al. | [41] | Ethics and concerns | ELSI; Personnel barriers; data misuse | ELSI; technical infrastructure; education and training; personnel aspects; trust; consent procedures; |
| Alzahrani et al. | [19] | Healthcare/Blockchain | ELSI; data structure; technical barriers | technical infrastructure; data access; education and training; data structure; consent procedures; |
| Broes et al. | [42] | Healthcare/Oncology | data structure | positive outcome; participation |
| Burgess et al. | [43] | EU—Ethics Advisory Group | Stigmatization; commercial interests; | - |
| Crusoe and Melin | [13] | Open Government Data Barriers | ELSI; Personnel barriers; data structure; technical barriers; institutional barriers; economic barriers; | technical infrastructure; communication; |
| Csányi et al. | [14] | Open Data in Judicial Systems | technical barriers; data privacy; | - |
| Deist et al. | [31] | Healthcare | ELSI; Personnel barriers; data structure; technical barriers; institutional barriers; | technical infrastructure; data structure; collaborations; |
| Dos Santos Rocha et al. | [17] | Research/Open Science | ELSI; Personnel barriers; technical barriers; data misuse; economic barriers; | positive outcome; |
| Dove et al. | [5] | Open Government | Personnel barriers; data structure; communication; | positive outcome; technical infrastructure; data access; education and training; personnel aspects; collaborations; |
| Feeney et al. | [25] | Healthcare | ELSI; Personnel barriers; data structure; technical barriers; trust; | ELSI; data access; data structure; trust; |
| Fischer et al. | [44] | Research/Open Science | data structure; clarification and consent; economic barriers; | positive outcome; ELSI; economic aspects |
| Fischer-Hübner et al. | [45] | Cybersecurity/Open Data | ELSI; Personnel barriers; technical barriers; data privacy; trust; | ELSI; technical infrastructure; data access; education and training; institutional aspects |
| Floridi et al. | [46] | Ethics/Healthcare | ELSI | positive outcome; data access; education and training; personnel aspects; economic aspects |
| Fylan and Fylan | [29] | Healthcare | Personnel barriers; technical barriers; data misuse; clarification and consent; stigmatization; commercial interests; trust; | technical infrastructure; data access; data structure; trust; consent procedures; collaborations; |
| Galdon Clavell | [47] | Open Data for Urban Safety | - | ELSI; |
| Govarts et al. | [18] | Healthcare/Research | ELSI; Personnel barriers; data structure; technical barriers; clarification and consent; institutional barriers; economic barriers; data privacy; | ELSI; technical infrastructure; data access; personnel aspects; data structure; consent procedures; collaborations; |
| Hallock et al. | [27] | Healthcare | ELSI; Personnel barriers; data structure; technical barriers; clarification and consent; institutional barriers; data privacy; | positive outcome; education and training; personnel aspects; trust; institutional aspects |
| Horn and Kerasidou | [24] | Healthcare | economic barriers; data privacy; commercial interests; trust; communication; | positive outcome; ELSI; data access; trust; collaborations; economic aspects; participation |
| Househ et al. | [36] | Healthcare | ELSI; Personnel barriers; data structure; technical barriers; stigmatization; trust; | ELSI; education and training; personnel aspects; communication; economic aspects; participation |
| Kamikubo et al. | [1] | Healthcare/Research | data misuse; clarification and consent; stigmatization; commercial interests; | positive outcome; technical infrastructure; data access; education and training; education and training; data structure; trust; consent procedures; participation |
| Kawashita et al. | [11] | Open Government | ELSI; Personnel barriers; data structure; technical barriers; clarification and consent; institutional barriers; communication; | positive outcome; ELSI; technical infrastructure; education and training; personnel aspects; data structure; collaborations; communication; economic aspects; institutional aspects |
| Kuo et al. | [33] | Healthcare/genomic data | ELSI; data misuse; stigmatization | positive outcome; |
| Kwon and Motohashi | [48] | Research/Open Science | Personnel barriers | positive outcome; |
| Mahomed and Labuschaigne | [49] | Ethics/Research | ELSI; data structure; technical barriers; data misuse; stigmatization; economic barriers; communication; | ELSI; |
| McWhirter et al. | [32] | Healthcare | ELSI; economic barriers; | - |
| Medley et al. | [21] | Healthcare | ELSI; clarification and consent; economic barriers; | technical infrastructure; data access; trust; collaborations; |
| Mutambik et al. | [10] | Open Government | ELSI; Personnel barriers; data structure; technical barriers; clarification and consent; stigmatization; institutional barriers; economic barriers; data privacy; trust; | positive outcome; ELSI; |
| Nellåker et al. | [34] | Healthcare/Research | ELSI; data privacy; | positive outcome; data access; consent procedures; |
| Nunes Vilaza et al. | [50] | Healthcare | ELSI; data misuse; clarification and consent; stigmatization; commercial interests; | positive outcome; data access; education and training; personnel aspects; consent procedures; communication; |
| Papageorgiou et al. | [51] | Healthcare/Migration | Personnel barriers; stigmatization; trust; communication; | participation |
| Queralt-Rosinach et al. | [6] | Healthcare/Hospital | data structure; clarification and consent; communication; | technical infrastructure; education and training; data structure; consent procedures; collaborations; communication; institutional aspects |
| Rehman et al. | [2] | Healthcare | ELSI; data structure; technical barriers | positive outcome; |
| Rempel et al. | [8] | Open Government | Personnel barriers; data misuse; institutional barriers; | positive outcome; ELSI; communication; |
| Rockhold et al. | [52] | Open Sciences | - | data access; consent procedures; |
| Roguljić et al. | [7] | Healthcare/Patient images | Personnel barriers; technical barriers; clarification and consent | - |
| Sandoval-Almazan et al. | [53] | Open Government | ELSI; data misuse; institutional barriers; | ELSI; data access; trust; institutional aspects |
| Scheibner et al. | [35] | Healthcare | technical barriers; institutional barriers; | technical infrastructure; |
| Schwalbe et al. | [23] | Healthcare | ELSI; Personnel barriers; data structure; technical barriers; stigmatization; economic barriers; | - |
| Seo et al. | [9] | Open Government Data | - | data structure; |
| Sleigh | [4] | Healthcare/Data donation | data misuse; commercial interests; | positive outcome; personnel aspects; |
| Smart et al. | [54] | Healthcare | stigmatization | education and training; personnel aspects; trust; institutional aspects |
| Smith and Sandberg | [12] | Open Government | Personnel barriers | positive outcome; personnel aspects; communication; |
| Tan et al. | [55] | Open Science | Personnel barriers; clarification and consent; data privacy; | - |
| Thoral et al. | [28] | Healthcare | ELSI; stigmatization; institutional barriers; | ELSI; collaborations; |
| Tuler de Oliveira et al. | [56] | Healthcare | data structure | technical infrastructure; data access; education and training; personnel aspects; trust; |
| van der Burg et al. | [57] | Agriculture | commercial interests; trust; | ELSI; data access; |
| van Donge et al. | [15] | Open Government | Personnel barriers; data structure; technical barriers; institutional barriers; communication; | positive outcome; data access; economic aspects |
| Vianen et al. | [58] | Healthcare/Pre-Hospital | ELSI; economic barriers; data privacy; | - |
| Viberg et al. | [30] | Healthcare/Research | ELSI; data misuse; commercial interests; | positive outcome; ELSI; trust; |
| Wang et al. | [59] | ELSI data misuse; | data privacy; | - |
| Wieczorkowski | [60] | Open Government | ELSI; data structure | positive outcome; |
| Wolff et al. | [61] | Open Government/Research | Personnel barriers; data structure | technical infrastructure; education and training; data structure; |
| Yerden and F. Luna-Reyes | [62] | Open Government | - | ELSI; technical infrastructure; data structure; |
| Zuiderwijk and Spiers | [22] | Research/astrophysics | - | positive outcome; ELSI; technical infrastructure; personnel aspects; data structure; collaborations; |
| Barriers | # | Authors |
|---|---|---|
| ELSI | 27 | [2,10,11,13,17,18,19,21,23,25,27,28,30,31,32,33,34,36,40,41,45,46,49,50,53,58,60] |
| personnel barriers | 23 | [5,7,8,10,11,12,13,15,17,18,23,25,27,29,31,36,40,41,45,48,51,55,61] |
| data structure | 20 | [2,5,6,10,11,13,15,18,19,23,25,27,31,36,42,44,49,56,60,61] |
| technical barriers | 19 | [2,7,10,11,13,14,15,17,18,19,23,25,27,29,31,35,36,45,49] |
| data misuse | 13 | [1,4,8,17,29,30,33,40,41,49,50,53,59] |
| clarification and consent | 13 | [1,6,7,10,11,18,21,27,29,44,50,55] |
| stigmatization | 12 | [1,10,23,28,29,33,36,43,49,50,51,54] |
| institutional barriers | 12 | [8,10,11,13,15,18,27,28,31,35,40,53] |
| economic barriers | 12 | [10,11,13,17,18,21,23,24,32,44,49,58] |
| data privacy | 10 | [10,14,18,24,27,34,45,55,58,59] |
| commercial interests | 8 | [1,4,24,29,30,43,50,57] |
| trust | 8 | [10,24,25,29,36,45,51,57] |
| communication | 7 | [5,6,11,15,24,49,51] |
| Support Factors | # | Authors |
|---|---|---|
| positive outcome | 22 | [1,2,4,5,8,10,11,12,15,17,22,24,27,30,33,34,42,44,46,48,50,60] |
| ELSI | 18 | [8,10,11,18,22,24,25,28,30,36,41,44,45,47,49,53,57,62] |
| technical infrastructure | 17 | [1,5,6,11,13,18,19,21,22,29,31,35,41,45,56,61,62] |
| data access | 17 | [1,5,15,18,19,21,24,25,29,34,45,46,50,52,53,56,57] |
| education and training | 15 | [1,5,6,11,19,27,36,40,41,45,46,50,54,56,61] |
| personnel aspects | 13 | [4,5,11,12,18,22,27,36,41,46,50,54,56] |
| data structure | 12 | [1,6,9,11,18,19,22,25,29,31,61,62] |
| trust | 11 | [1,21,24,25,27,29,30,41,53,54,56] |
| consent procedures | 10 | [1,6,18,19,29,34,41,50,52] |
| collaborations | 10 | [5,6,11,18,21,22,24,28,29,31] |
| communication | 7 | [6,8,11,12,13,36,50] |
| economic aspects | 6 | [11,15,24,36,44,46] |
| institutional aspects | 6 | [6,11,27,44,53,54] |
| participation | 6 | [1,24,36,40,42,51] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lichtenauer, N.; Schmidbauer, L.; Wilhelm, S.; Wahl, F. A Scoping Review on Analysis of the Barriers and Support Factors of Open Data. Information 2024, 15, 5. https://doi.org/10.3390/info15010005
Lichtenauer N, Schmidbauer L, Wilhelm S, Wahl F. A Scoping Review on Analysis of the Barriers and Support Factors of Open Data. Information. 2024; 15(1):5. https://doi.org/10.3390/info15010005
Chicago/Turabian StyleLichtenauer, Norbert, Lukas Schmidbauer, Sebastian Wilhelm, and Florian Wahl. 2024. "A Scoping Review on Analysis of the Barriers and Support Factors of Open Data" Information 15, no. 1: 5. https://doi.org/10.3390/info15010005
APA StyleLichtenauer, N., Schmidbauer, L., Wilhelm, S., & Wahl, F. (2024). A Scoping Review on Analysis of the Barriers and Support Factors of Open Data. Information, 15(1), 5. https://doi.org/10.3390/info15010005