
Agent-Based Simulation Framework for Epidemic Forecasting during Hajj Seasons in Saudi Arabia

 , , and
, , and
Abstract
:1. Introduction
- A data-driven framework was proposed for assessing disease spread at the annual global religious gathering of Hajj using epidemic modeling and agent-based simulation.
- In the proposed framework, the pre-event and post-event stages of Hajj were included. To the best of our knowledge, existing works have not considered simulating the disease spread during the period before a pre-planned MG, the MG itself, and after the event (MG) is concluded.
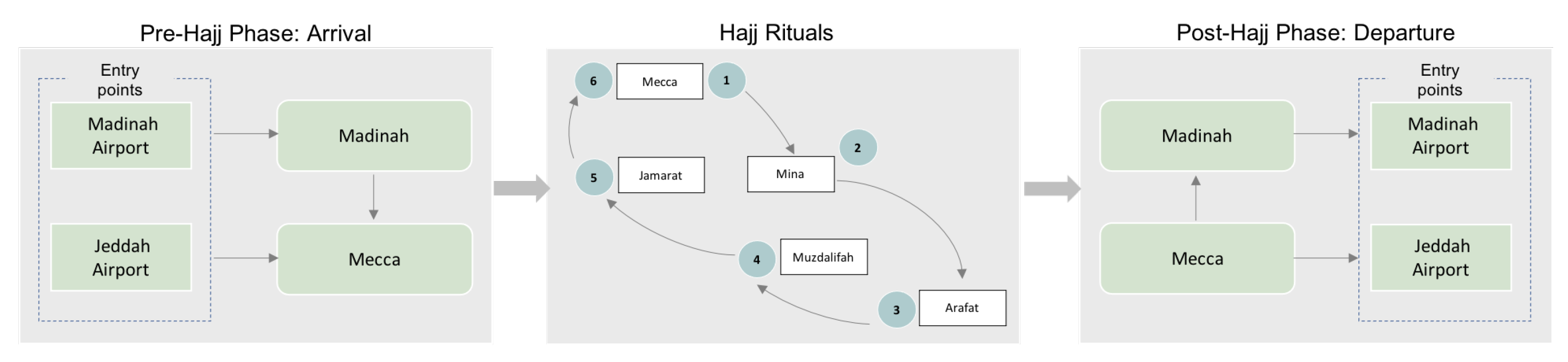
- Simulation of disease spread at the different phases and rituals of Hajj integrating the spatial and temporal features of each phase.
2. Background
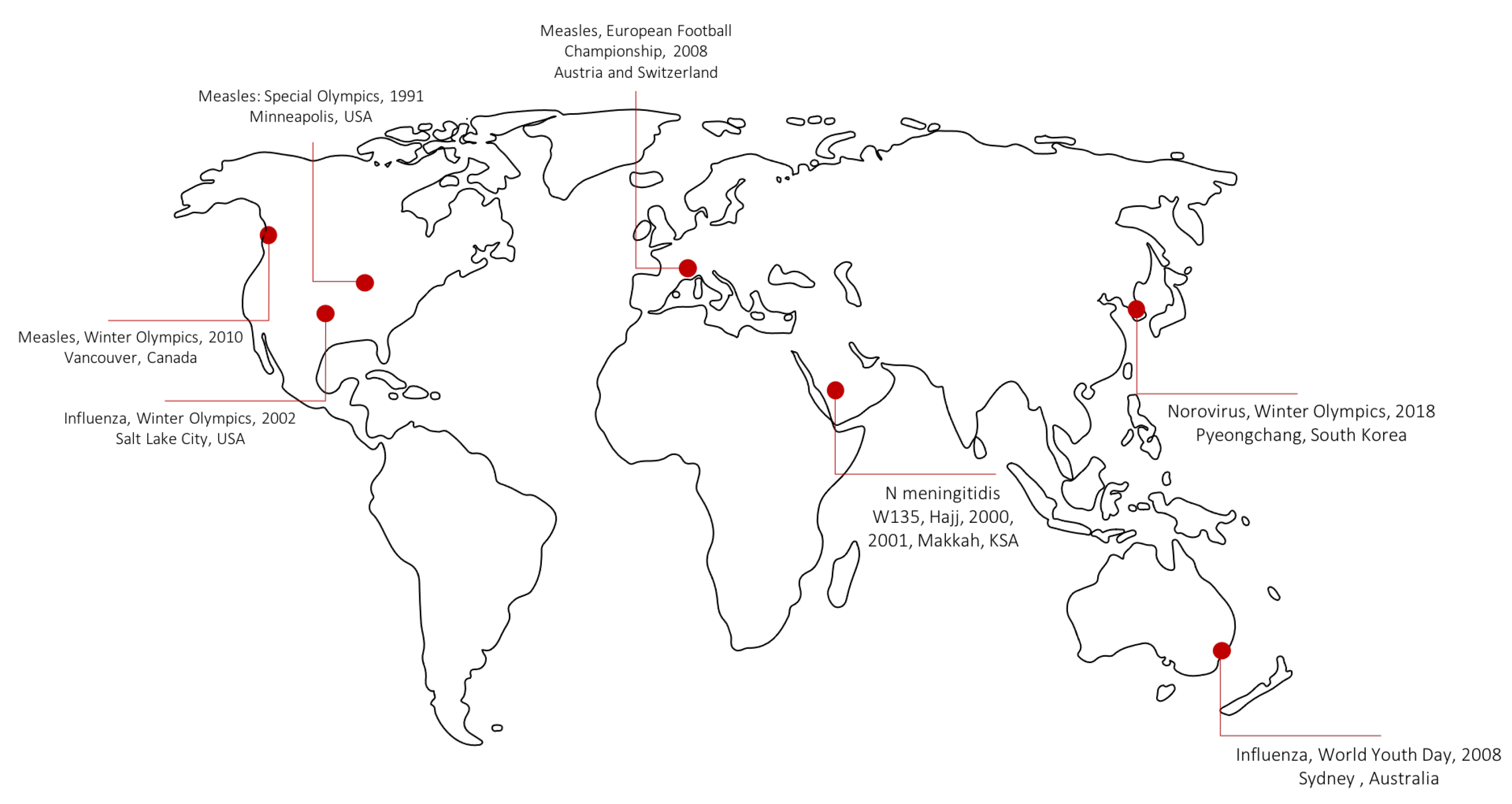
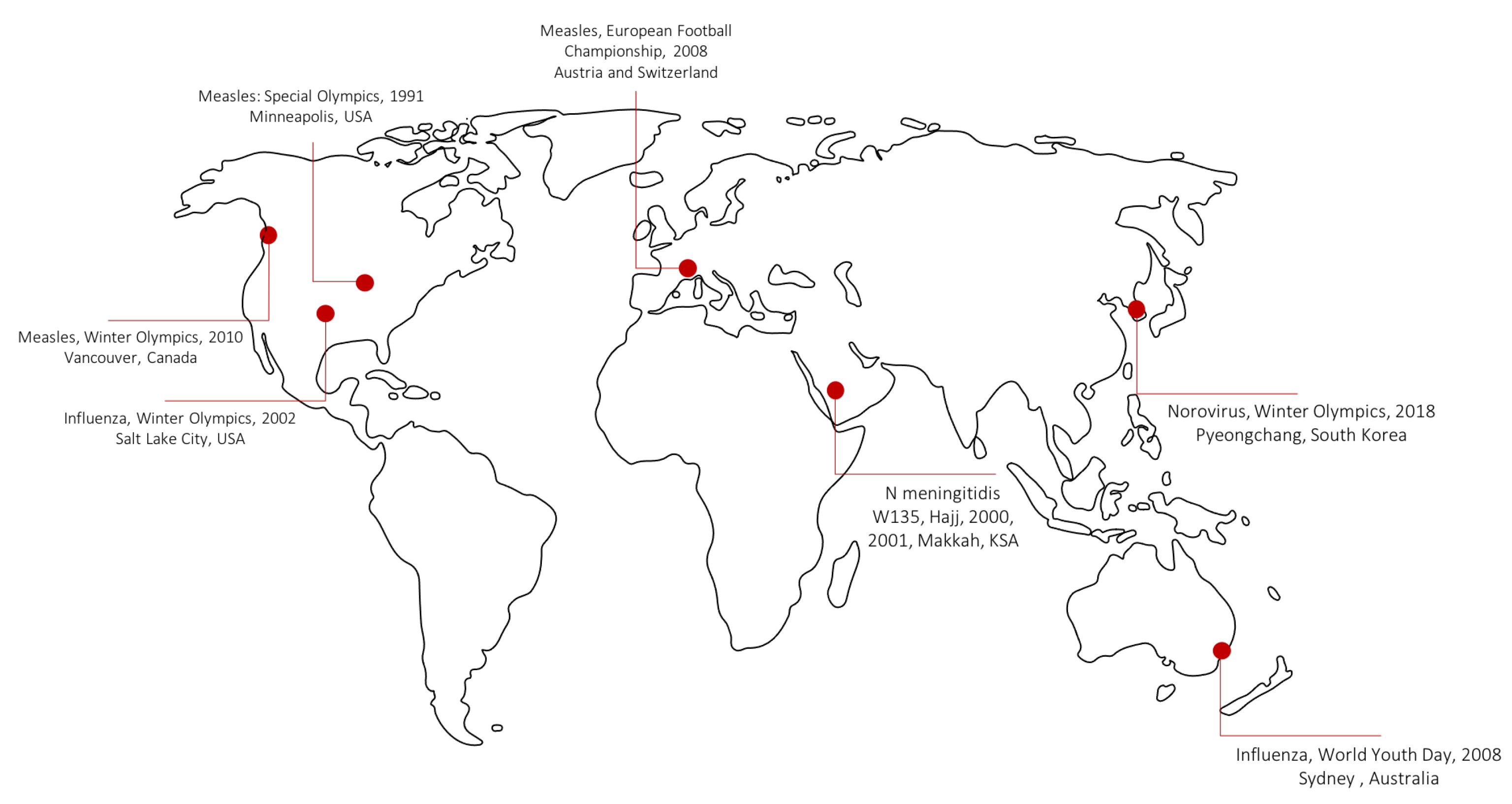
2.1. Global Mass Gatherings and Disease Epidemics
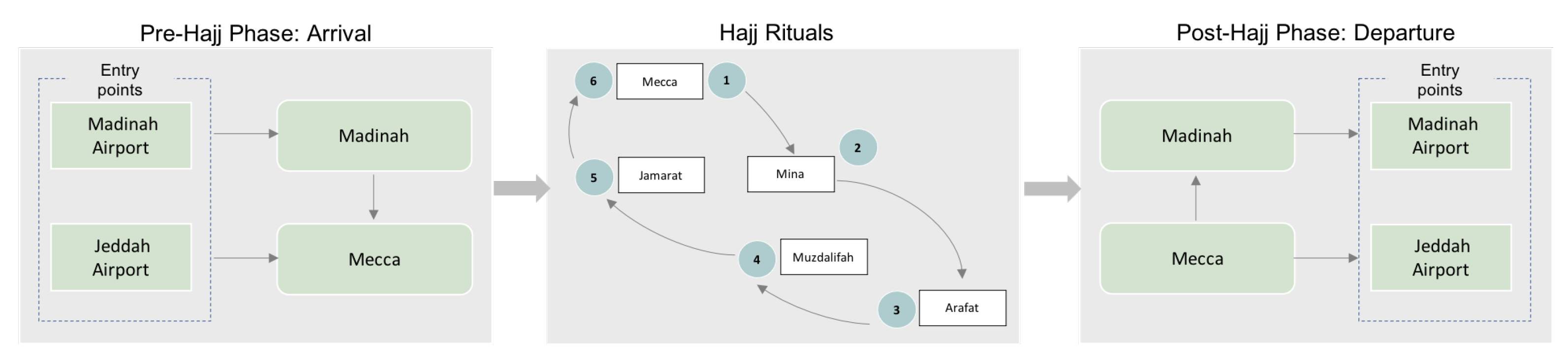
2.2. Religious Global Gathering of Hajj
2.3. Public Health Response during Hajj Seasons
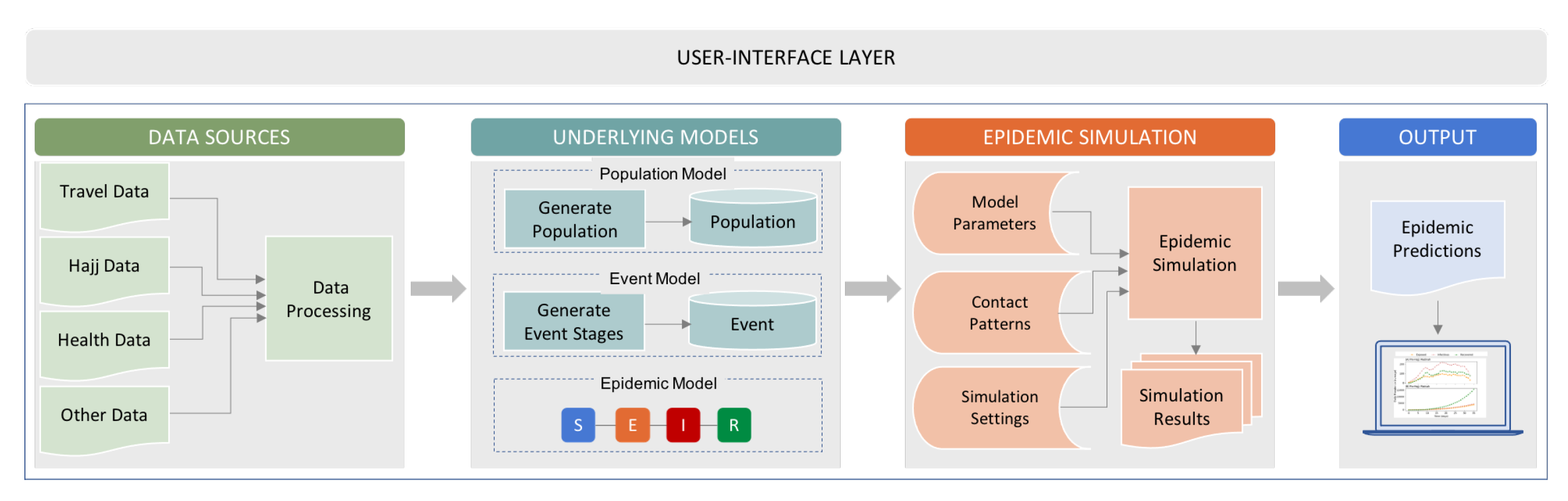
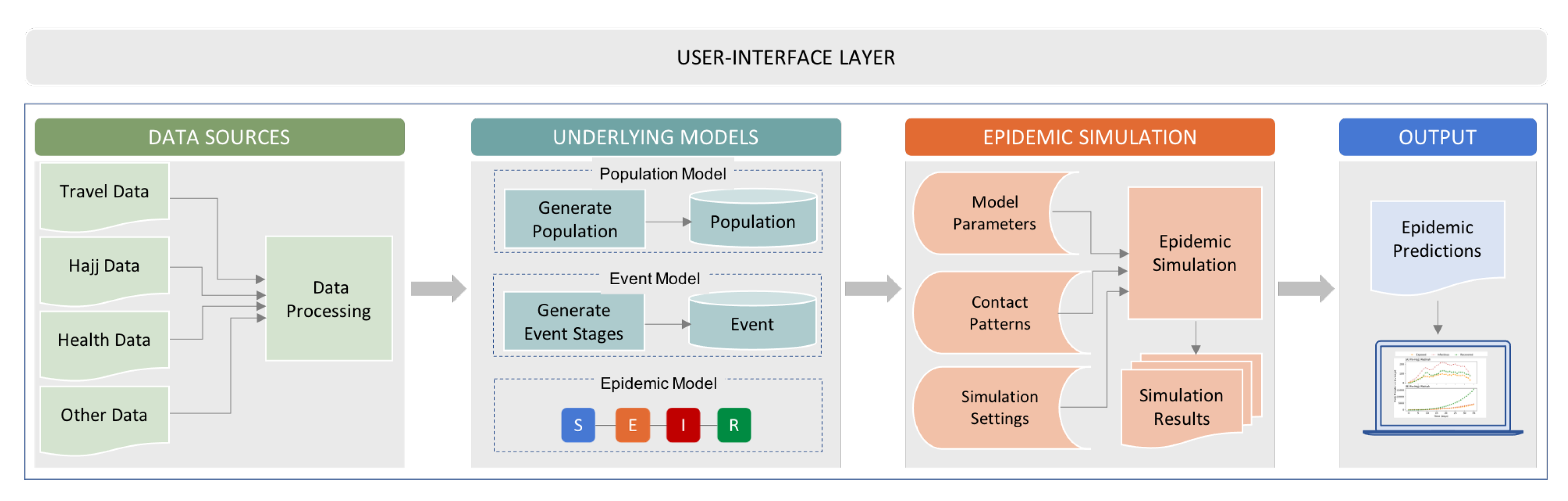
3. Epidemic Forecasting Framework
3.1. Underlying Models
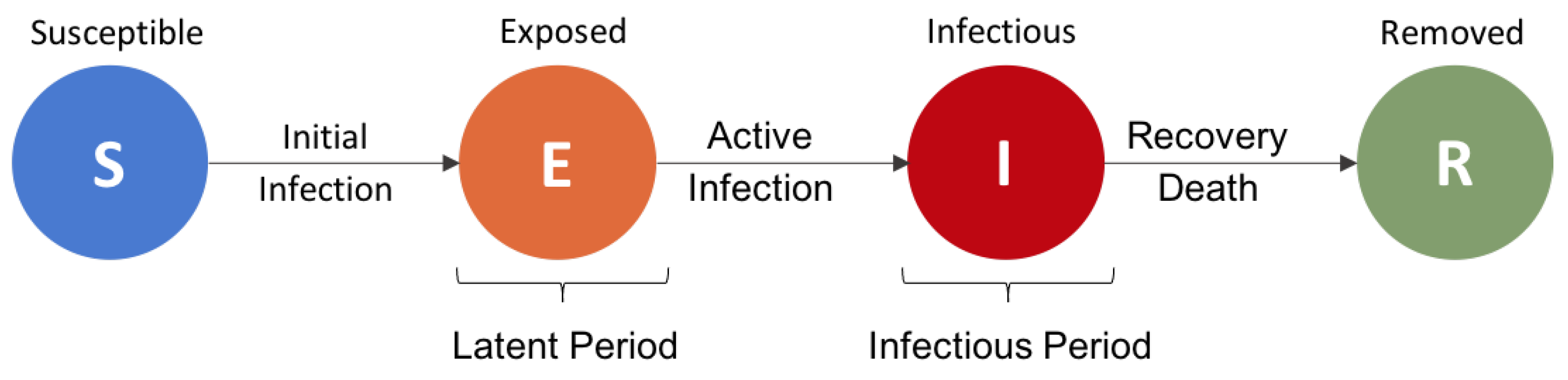
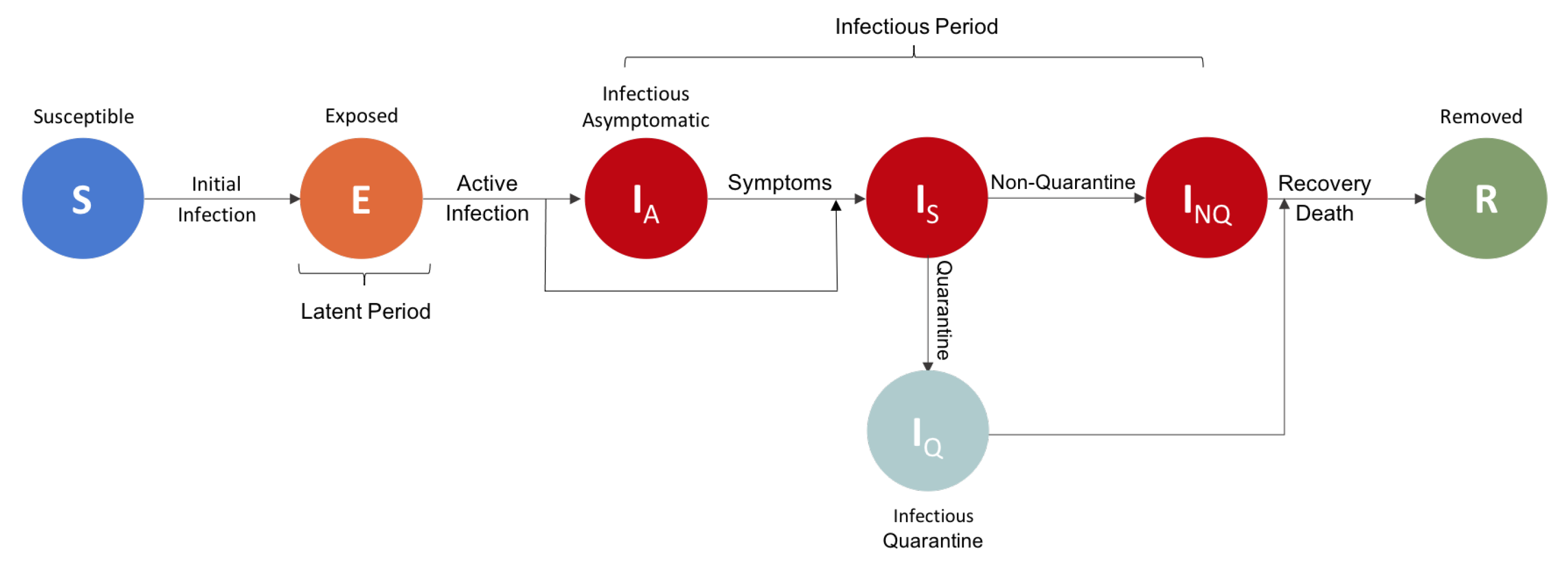
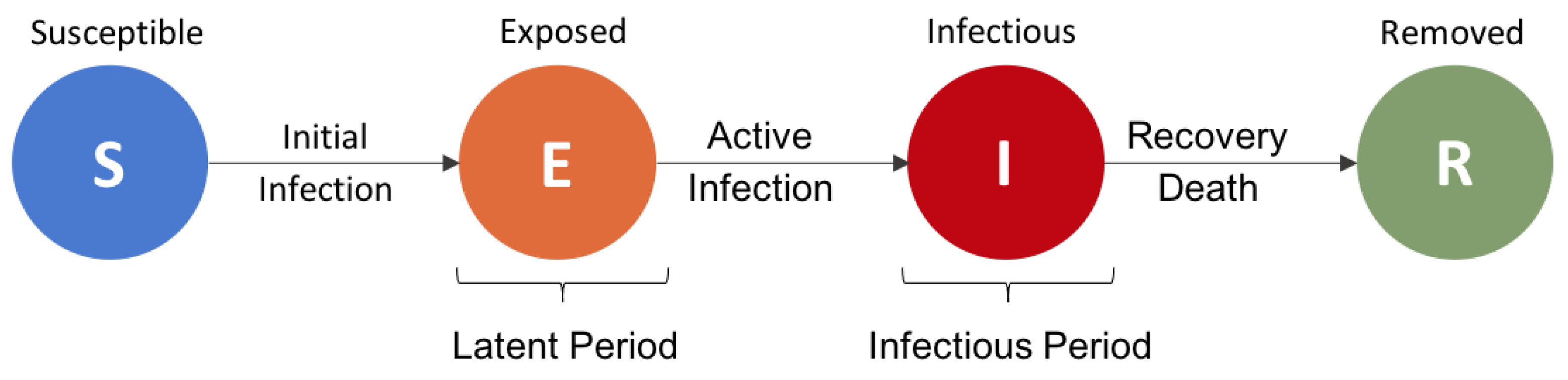
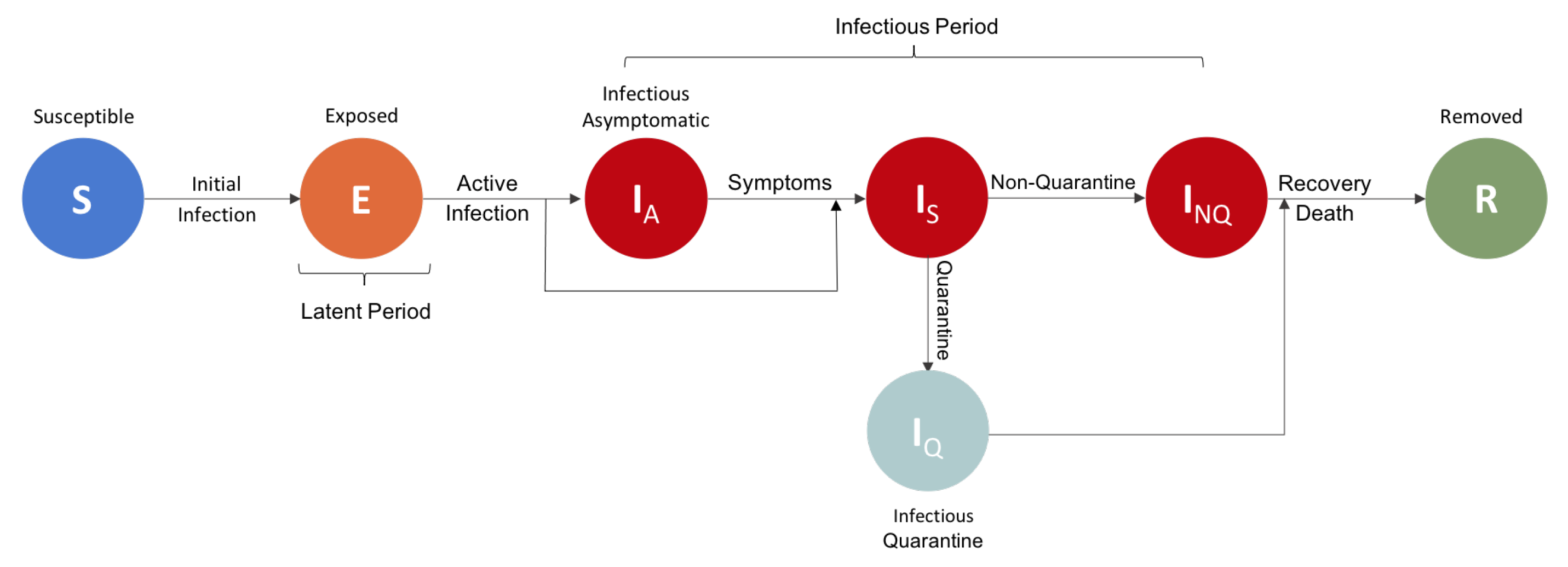
3.2. Disease Dynamics
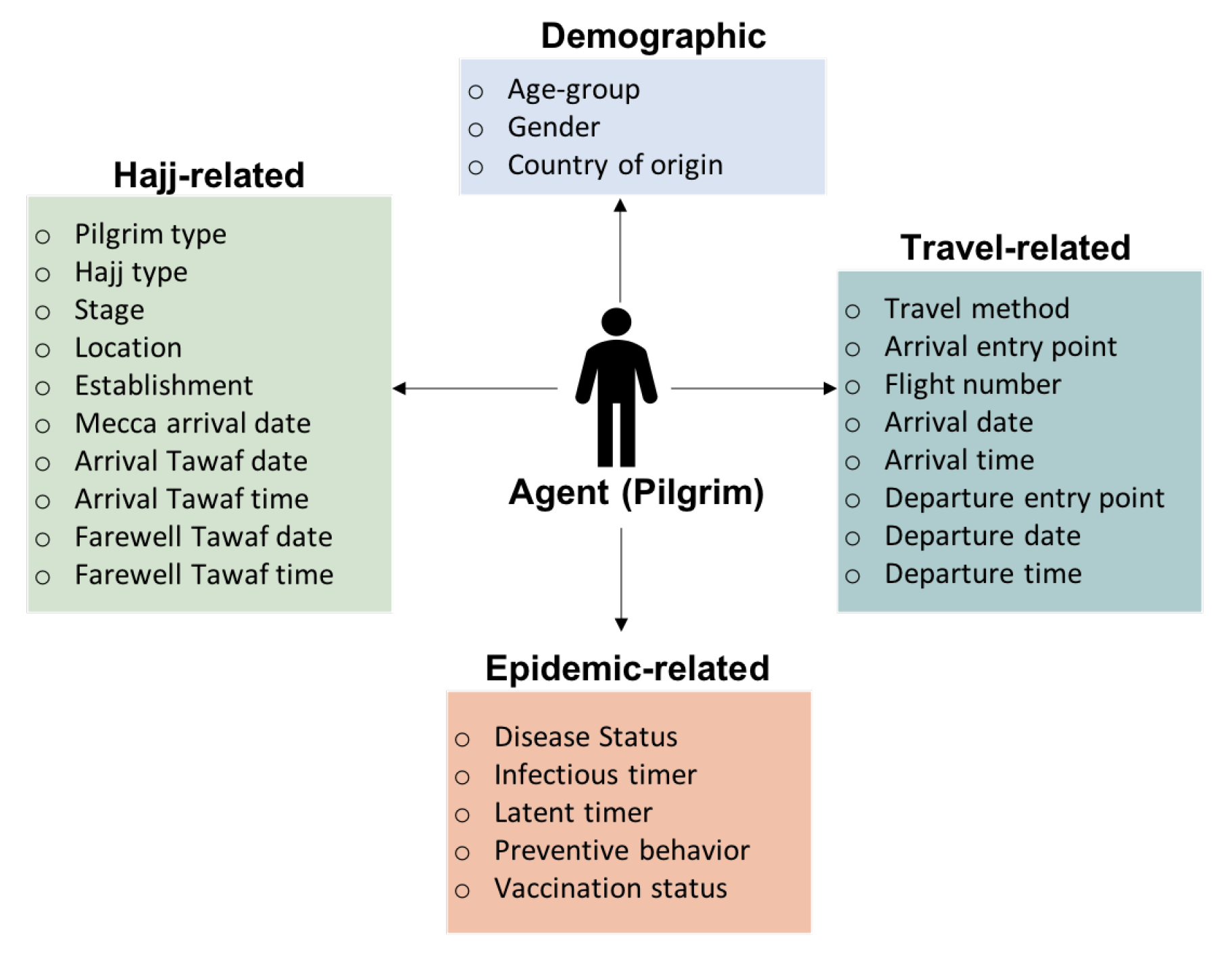
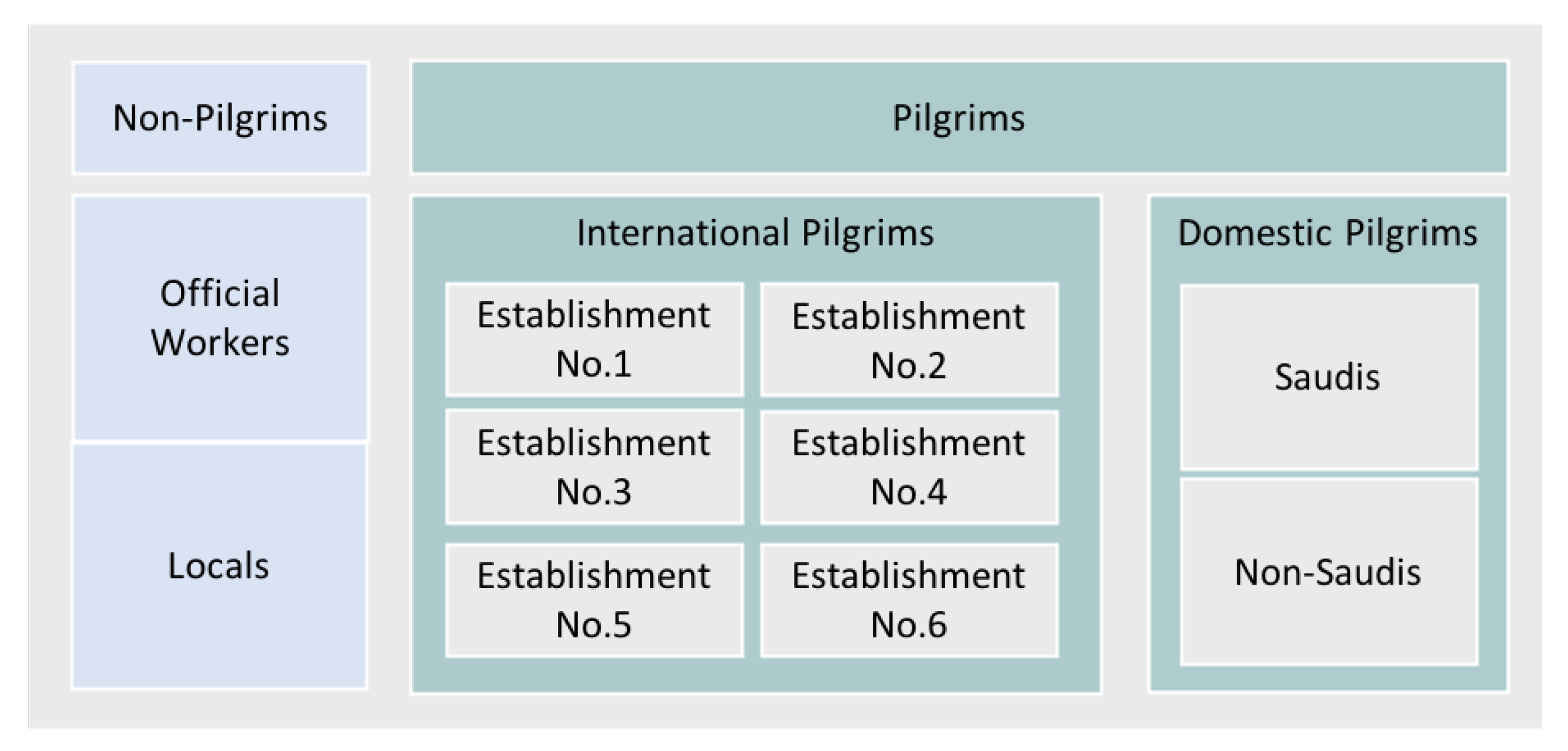
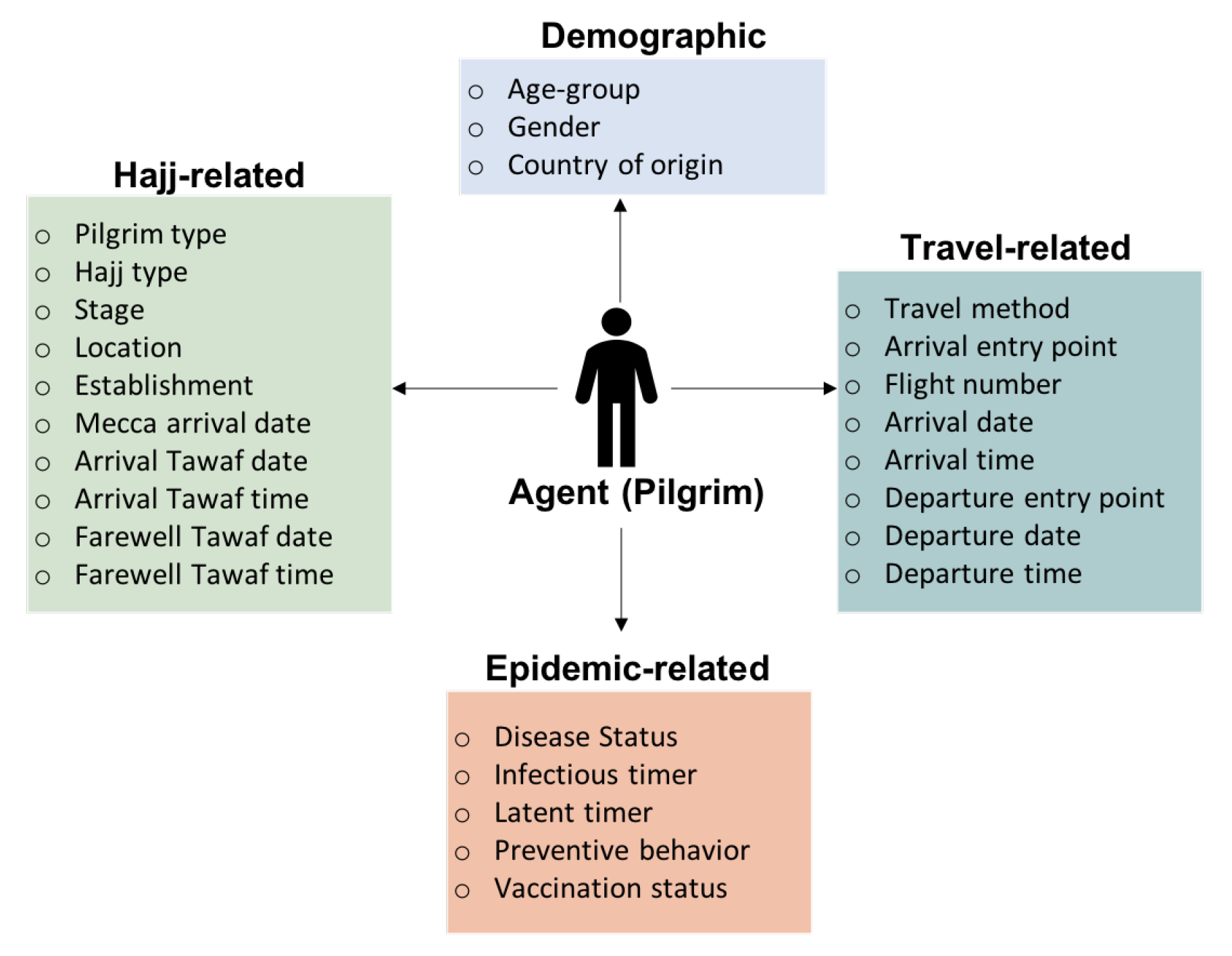
3.3. Agent-Based Simulation
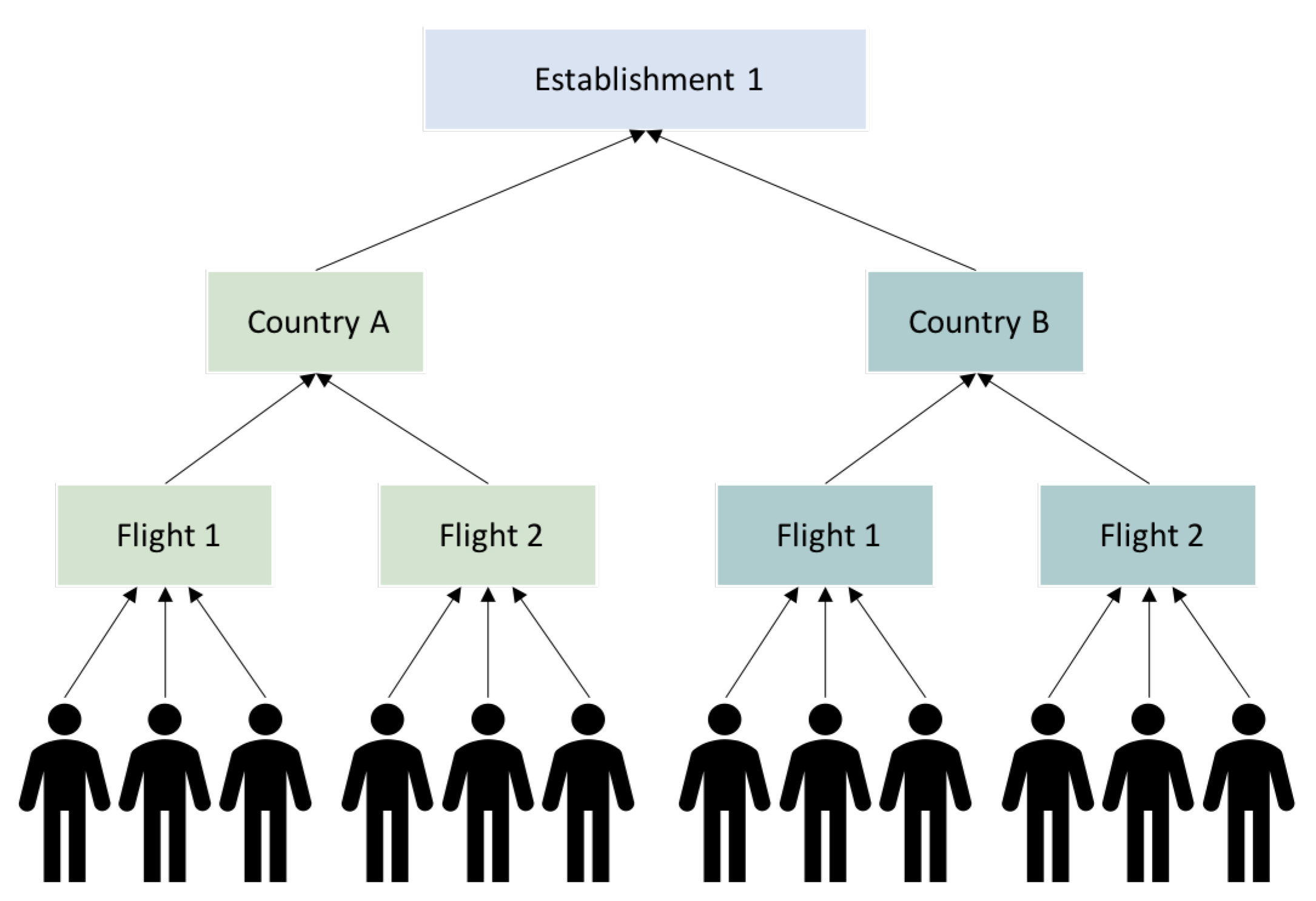
- Agents who arrive on the same flight will complete all rituals as a group.
- Agents will mix randomly with a higher rate towards agents belong to the same group and a lower rate across other groups.
- Agents interactions will be restricted to agents from the same gender at their tents at the campus in Mina.
- At Mina campus, agents will remain in their accommodations (tents) throughout the night time.
- Agents will follow an hourly schedule per establishment on the first day of the Jamarat ritual.
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nii-Trebi, N.I. Emerging and neglected infectious diseases: Insights, advances, and challenges. BioMed Res. Int. 2017, 2017, 5245021. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, S. Emerging infectious diseases: Epidemiological perspective. Indian J. Dermatol. 2017, 62, 459–467. [Google Scholar]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 51. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey={adgroupsurvey}&gclid=EAIaIQobChMIkuzvya6o8gIVB7qWCh2QHQk9EAAYASAAEgJddvD_BwE (accessed on 1 July 2021).
- World Health Organization. WHO Report on Global Surveillance of Epidemic-Prone Infectious Diseases; Technical Report; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Heymann, D.L.; Rodier, G.R. Hot spots in a wired world: WHO surveillance of emerging and re-emerging infectious diseases. Lancet Infect. Dis. 2001, 1, 345–353. [Google Scholar] [CrossRef]
- World Health Organization. Communicable Disease Surveillance and Response Systems: Guide to Monitoring and Evaluating; Technical Report; World Health Organization: Lyon, France, 2006. [Google Scholar]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.D.; Schuchat, A.; et al. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Hoang, V.T.; Gautret, P. Infectious diseases and mass gatherings. Curr. Infect. Dis. Rep. 2018, 20, 44. [Google Scholar] [CrossRef]
- World Health Organization. Public Health for Mass Gatherings: Key Considerations. Available online: https://www.who.int/publications/i/item/public-health-for-mass-gatherings-key-considerations (accessed on 1 July 2021).
- Ahmed, Q.A.; Memish, Z.A. The cancellation of mass gatherings (MGs)? Decision making in the time of COVID-19. Travel Med. Infect. Dis. 2020, 34, 101631. [Google Scholar] [CrossRef]
- World Health Organization. How to Use WHO Risk Assessment and Mitigation Checklist for Mass Gatherings in the Context of COVID-19: Interim Guidance, 20 March 2020; Technical Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Chao, D.L.; Halloran, M.E.; Obenchain, V.J.; Longini, I.M., Jr. FluTE, a publicly available stochastic influenza epidemic simulation model. PLoS Comput. Biol. 2010, 6, e1000656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; Enanoria, W.T.; Zipprich, J.; Blumberg, S.; Harriman, K.; Ackley, S.F.; Wheaton, W.D.; Allpress, J.L.; Porco, T.C. The role of vaccination coverage, individual behaviors, and the public health response in the control of measles epidemics: An agent-based simulation for California. BMC Public Health 2015, 15, 447. [Google Scholar] [CrossRef] [Green Version]
- Gwalani, H.; Hawamdeh, F.; Mikler, A.R.; Xiong, K. Modeling the 2013 zika outbreak in French Polynesia: Intervention strategies. Appl. Syst. Innov. 2018, 1, 31. [Google Scholar] [CrossRef] [Green Version]
- Wiratsudakul, A.; Suparit, P.; Modchang, C. Dynamics of Zika virus outbreaks: An overview of mathematical modeling approaches. PeerJ 2018, 6, e4526. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Ma, Z.; Brauer, F. A discrete epidemic model for SARS transmission and control in China. Math. Comput. Model. 2004, 40, 1491–1506. [Google Scholar] [CrossRef]
- Rocklöv, J.; Sjödin, H.; Wilder-Smith, A. COVID-19 outbreak on the Diamond Princess cruise ship: Estimating the epidemic potential and effectiveness of public health countermeasures. J. Travel Med. 2020, 27, taaa030. [Google Scholar] [CrossRef] [Green Version]
- Hamzah, F.B.; Lau, C.; Nazri, H.; Ligot, D.; Lee, G.; Tan, C.; Shaib, M.; Zaidon, U.; Abdullah, A.; Chung, M.; et al. CoronaTracker: Worldwide COVID-19 outbreak data analysis and prediction. Bull. World Health Organ. 2020, 1, 32. [Google Scholar] [CrossRef]
- Goscé, L.; Phillips, A.; Spinola, P.; Gupta, R.K.; Abubakar, I. Modelling SARS-COV2 Spread in London: Approaches to Lift the Lockdown. J. Infect. 2020, 81, 260–265. [Google Scholar] [CrossRef]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Flasche, S.; Clifford, S.; Pearson, C.A.; Munday, J.D.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Alkahtani, B.S.T.; Alzaid, S.S. A novel mathematics model of covid-19 with fractional derivative. Stability and numerical analysis. Chaos Solitons Fractals 2020, 138, 110006. [Google Scholar] [CrossRef]
- Hedayati, M.; Ezzati, R.; Noeiaghdam, S. New Procedures of a Fractional Order Model of Novel Coronavirus (COVID-19) Outbreak via Wavelets Method. Axioms 2021, 10, 122. [Google Scholar] [CrossRef]
- Noeiaghdam, S.; Micula, S.; Nieto, J.J. A Novel Technique to Control the Accuracy of a Nonlinear Fractional Order Model of COVID-19: Application of the CESTAC Method and the CADNA Library. Mathematics 2021, 9, 1321. [Google Scholar] [CrossRef]
- Alshammari, S.M.; Mikler, A.R. Modeling Disease Spread at Global Mass Gatherings: Data Requirements and Challenges. In Recent Advances in Information and Communication Technology 2016; Springer: Berlin/Heidelberg, Germany, 2016; pp. 17–26. [Google Scholar]
- Chowell, G.; Nishiura, H.; Viboud, C. Modeling Rapidly Disseminating Infectious Disease during Mass Gatherings. BMC Med. 2012, 10, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stehlé, J.; Voirin, N.; Barrat, A.; Cattuto, C.; Colizza, V.; Isella, L.; Régis, C.; Pinton, J.F.; Khanafer, N.; Van den Broeck, W.; et al. Simulation of an SEIR Infectious Disease mMdel on the Dynamic Contact Network of Conference Attendees. BMC Med. 2011, 9, 87. [Google Scholar] [CrossRef]
- Buldú, J.M.; Antequera, D.R.; Aguirre, J. The resumption of sports competitions after COVID-19 lockdown: The case of the Spanish football league. Chaos Solitons Fractals 2020, 138, 109964. [Google Scholar] [CrossRef]
- Shi, P.; Keskinocak, P.; Swann, J.L.; Lee, B.Y. The Impact of Mass Gatherings and Holiday Traveling on the Course of an Influenza Pandemic: A Computational Model. BMC Public Health 2010, 10, 778. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.; Arino, J.; Hu, W.; Raposo, P.; Sears, J.; Calderon, F.; Heidebrecht, C.; Macdonald, M.; Liauw, J.; Chan, A.; et al. Spread of a novel influenza A (H1N1) virus via global airline transportation. N. Engl. J. Med. 2009, 361, 212–214. [Google Scholar] [CrossRef]
- Al Tawfiq, J.; Smallwood, C.; Arbuthnott, K.; Malik, M.; Barbeschi, M.; Memish, Z. Emerging respiratory and novel coronavirus 2012 infections and mass gatherings. EMHJ-East. Mediterr. Health J. 2013, 19 (Suppl. 1), S48–S54. [Google Scholar] [CrossRef]
- Memish, Z.A.; Al-Tawfiq, J.A.; Al-Rabeeah, A.A. Hajj: Preparations underway. Lancet Glob. Health 2013, 1, e331. [Google Scholar] [CrossRef] [Green Version]
- Bieh, K.L.; Khan, A.; El-Ganainy, A.; Alotaibi, B.; Ghallab, S.; Abdulmalek, N.; Mukhtar, N.; Jokhdar, H. Guidance for health risk assessment at recurrent mass gatherings: The Jeddah tool framework. Prehospital Disaster Med. 2021, 36, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Jokhdar, H.; Khan, A.; Asiri, S.; Motair, W.; Assiri, A.; Alabdulaali, M. COVID-19 mitigation plans during Hajj 2020: A success story of zero cases. Health Secur. 2021, 19, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Coburn, B.J.; Wagner, B.G.; Blower, S. Modeling influenza epidemics and pandemics: Insights into the future of swine flu (H1N1). BMC Med. 2009, 7, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Xie, W.; Wang, Y.; Xiong, Y.; Chen, S.; Han, J.; Wu, Q. A comparative overview of COVID-19, MERS and SARS. Int. J. Surg. 2020, 81, 1–8. [Google Scholar] [CrossRef]
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef]
- Jhung, M.A.; Swerdlow, D.; Olsen, S.J.; Jernigan, D.; Biggerstaff, M.; Kamimoto, L.; Kniss, K.; Reed, C.; Fry, A.; Brammer, L.; et al. Epidemiology of 2009 Pandemic Influenza A (H1N1) in the United States. Clin. Infect. Dis. 2011, 52, S13–S26. [Google Scholar] [CrossRef]
- Tuite, A.R.; Greer, A.L.; Whelan, M.; Winter, A.L.; Lee, B.; Yan, P.; Wu, J.; Moghadas, S.; Buckeridge, D.; Pourbohloul, B.; et al. Estimated Epidemiologic Parameters and Morbidity Associated with Pandemic H1N1 Influenza. Can. Med. Assoc. J. 2010, 182, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Assiri, A.; Al-Tawfiq, J.A.; Al-Rabeeah, A.A.; Al-Rabiah, F.A.; Al-Hajjar, S.; Al-Barrak, A.; Flemban, H.; Al-Nassir, W.N.; Balkhy, H.H.; Al-Hakeem, R.F.; et al. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: A descriptive study. Lancet Infect. Dis. 2013, 13, 752–761. [Google Scholar] [CrossRef] [Green Version]
- Song, R.; Han, B.; Song, M.; Wang, L.; Conlon, C.P.; Dong, T.; Tian, D.; Zhang, W.; Chen, Z.; Zhang, F.; et al. Clinical and epidemiological features of COVID-19 family clusters in Beijing, China. J. Infect. 2020, 81, e26–e30. [Google Scholar] [CrossRef] [PubMed]
- Bulut, C.; Kato, Y. Epidemiology of COVID-19. Turk. J. Med. Sci. 2020, 50, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Macal, C.M.; North, M.J. Tutorial on agent-based modeling and simulation. In Proceedings of the Winter Simulation Conference, Orlando, FL, USA, 4 December 2005. [Google Scholar]
- Ren, C.; Yang, C.; Jin, S. Agent-based modeling and simulation on emergency evacuation. In International Conference on Complex Sciences; Springer: Berlin/Heidelberg, Germany, 2009; pp. 1451–1461. [Google Scholar]
- Luo, L.; Zhou, S.; Cai, W.; Low, M.Y.H.; Tian, F.; Wang, Y.; Xiao, X.; Chen, D. Agent-based human behavior modeling for crowd simulation. Comput. Animat. Virtual Worlds 2008, 19, 271–281. [Google Scholar] [CrossRef]
- Carley, K.M.; Fridsma, D.B.; Casman, E.; Yahja, A.; Altman, N.; Chen, L.C.; Kaminsky, B.; Nave, D. BioWar: Scalable agent-based model of bioattacks. IEEE Trans. Syst. Man Cybern. Part A Syst. Hum. 2006, 36, 252–265. [Google Scholar] [CrossRef]
- Perez, L.; Dragicevic, S. An agent-based approach for modeling dynamics of contagious disease spread. Int. J. Health Geogr. 2009, 8, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Cuevas, E. An agent-based model to evaluate the COVID-19 transmission risks in facilities. Comput. Biol. Med. 2020, 121, 103827. [Google Scholar] [CrossRef] [PubMed]
- Marini, M.; Brunner, C.; Chokani, N.; Abhari, R.S. Enhancing response preparedness to influenza epidemics: Agent-based study of 2050 influenza season in Switzerland. Simul. Model. Pract. Theory 2020, 103, 102091. [Google Scholar] [CrossRef]
- Hu, H.; Nigmatulina, K.; Eckhoff, P. The Scaling of Contact Rates with Population Density for the Infectious Disease Models. Math. Biosci. 2013, 244, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, S.M.; Gwalani, H.; Helsing, J.E.; Mikler, A.R. Disease spread simulation to assess the risk of epidemics during the global mass gathering of Hajj pilgrimage. In Proceedings of the 2019 Winter Simulation Conference (WSC), National Harbor, MD, USA, 8–11 December 2019; pp. 215–226. [Google Scholar]
- Fedosejev, A. React. js essentials; Packt Publishing Ltd.: Birmingham, UK, 2015. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Event | Type | Location | Frequency | Duration | Size (in Millions) |
|---|---|---|---|---|---|
| World Expo | Fair | Multiple locations | Every 5 Years | 6 months | up to 73 |
| Summer/Winter Olympics | Sports | Multiple locations | Every 2 Years | 16 days | up to 10 |
| FIFA World Cup | Sports | Multiple locations | Every 4 Years | 32 days | 1.5–3.5 |
| World Youth Day | Religious | Multiple locations | Every 3 Years | 6 days | 0.5–2 |
| Hajj | Religious | Mecca, Saudi Arabia | Annual | 5–8 days | 2–3 |
| Pandemic | H1N1 | MERS-CoV | COVID-19 |
| Identification | April 2009 | September 2012 | December 2019 |
| Hajj Season | 2009 | 2012 | 2020 |
| Hajj Dates | 25–30 November | 23–28 October | 28 July–2 August |
| Vaccine Approval | September 2009 | No vaccine | December 2020 |
| Estimated Value of | 1.4–1.6 [35] | 0.8–1.3 [36] | 2.4–3.58 [37,38] |
| Incubation Period | 2.7 days [39,40] | 5.2–6.0 [41] | 2–14 days [38,42] |
| Infectious Period | 3.8 days [40] | 7.6 days [41] | 3–6 days [42,43] |
| Confirmed Cases | 482,000 | 132 | 24,854,140 |
| By November 2009 | By September 2013 | By August 2020 | |
| Deaths | 6000 | 58 | 838,924 |
| By November 2009 | By September 2013 | By August 2020 |
| Stage | Duration | Susceptible | Exposed | Infectious | Recovered |
|---|---|---|---|---|---|
| Arrival | 35 days | ||||
| Jeddah airport | 500,476 () | 373 () | 851 () | 0 | |
| Madinah airport | 409,675 () | 310 () | 705 () | 0 | |
| Pre-Hajj | 35 days | ||||
| Madinah | 407,539 () | 418 () | 1107 () | 1625 () | |
| Mecca | 888,633() | 3805 () | 4470 () | 15,482 () | |
| Hajj rituals | 6 days | 831,485 () | 18,579 () | 25,475 () | 36,851 () |
| Post-Hajj | 30 days | ||||
| Mecca | 395,435 () | 7540 () | 19,097 () | 79,628 () | |
| Madinah | 313,203 () | 6316 () | 15,947 () | 75,224 () | |
| Departure | 30 days | ||||
| Jeddah airport | 392,535 () | 10,440 () | 19,097 () | 79,628 () | |
| Madinah airport | 310,781 () | 8738 () | 15,947 () | 75,224 () |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshammari, S.M.; Ba-Aoum, M.H.; Alganmi, N.A.; Allinjawi, A.A. Agent-Based Simulation Framework for Epidemic Forecasting during Hajj Seasons in Saudi Arabia. Information 2021, 12, 325. https://doi.org/10.3390/info12080325
Alshammari SM, Ba-Aoum MH, Alganmi NA, Allinjawi AA. Agent-Based Simulation Framework for Epidemic Forecasting during Hajj Seasons in Saudi Arabia. Information. 2021; 12(8):325. https://doi.org/10.3390/info12080325
Chicago/Turabian StyleAlshammari, Sultanah Mohammed, Mohammed Hassan Ba-Aoum, Nofe Ateq Alganmi, and Arwa AbdulAziz Allinjawi. 2021. "Agent-Based Simulation Framework for Epidemic Forecasting during Hajj Seasons in Saudi Arabia" Information 12, no. 8: 325. https://doi.org/10.3390/info12080325
APA StyleAlshammari, S. M., Ba-Aoum, M. H., Alganmi, N. A., & Allinjawi, A. A. (2021). Agent-Based Simulation Framework for Epidemic Forecasting during Hajj Seasons in Saudi Arabia. Information, 12(8), 325. https://doi.org/10.3390/info12080325