1. Background
Twenty Americans die every day while waiting for an organ transplant [
1]. In 2021, approximately 107,294 men, women, and children in the U.S. await a lifesaving organ; 83% of them need a kidney [
2]. The number of people who need an organ is increasing faster than the number of donors. From 1991 to 2021, the number of donors nearly tripled, but the number of waiting increased by nearly five times (from 23,198 to 107,294) [
2].
The gap between demand and availability is a major public health problem. Almost all adults in the U.S. (95%) support organ donation, yet 42% have chosen not to register as donors [
3]. That percentage not being registered is even higher among young adults—a range of 47% to 69% depending on the study [
4,
5,
6,
7]. Globally, the demand for organs and organ donors continues to soar, but there are challenges such as lack of awareness, lower willingness, higher medical mistrust, dwindling altruism, societal divide, and conflicts.
Almost all past studies of young adults ages 18–24 in this topical area have involved college students, with a majority being Caucasian. Hence, little is known about non-students/noncollege graduates who are racial/ethnic minorities, their rate of organ donation registration, and their decision-making process regarding registering. The current study is the first theoretical approach to study a sample of such young adults living in the ten states in the U.S. with the lowest rates of organ donation registration.
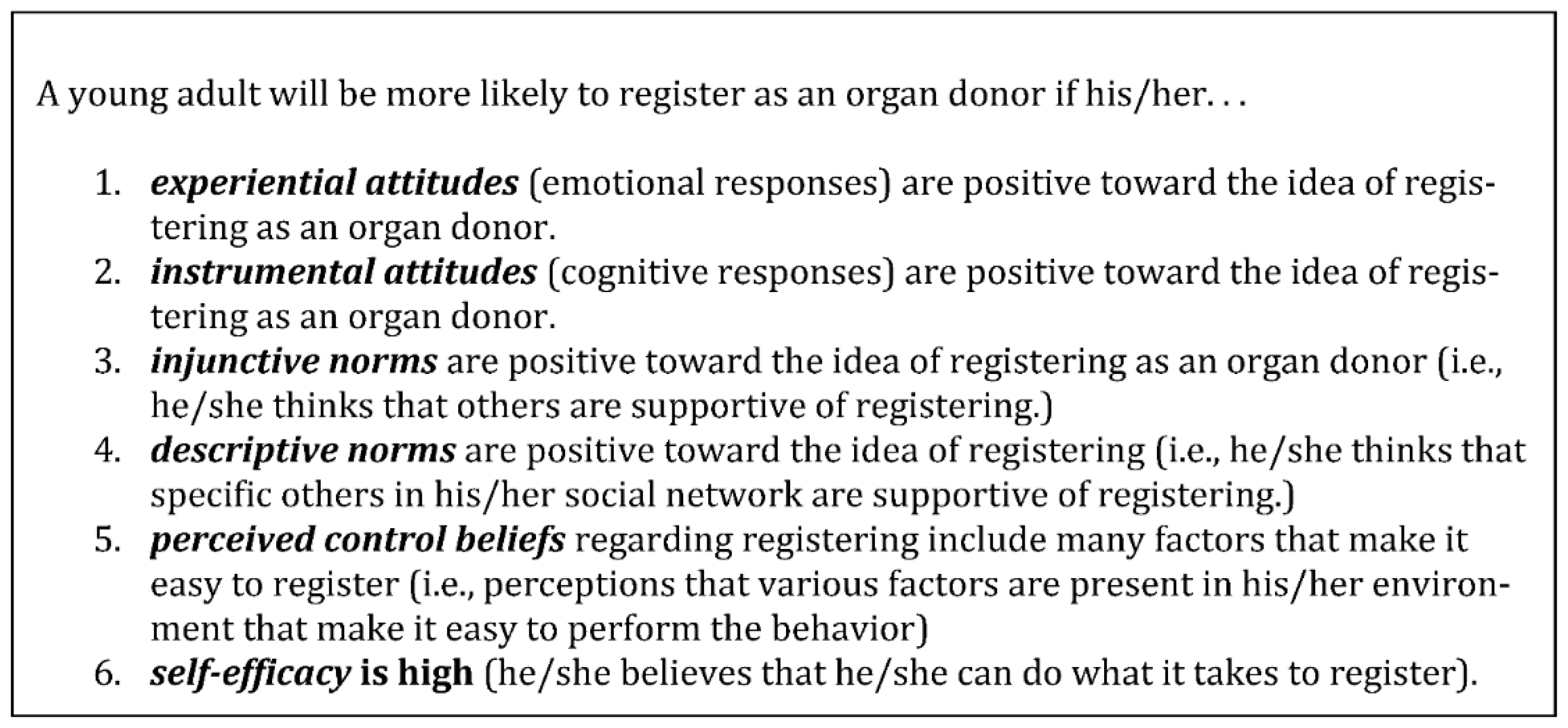
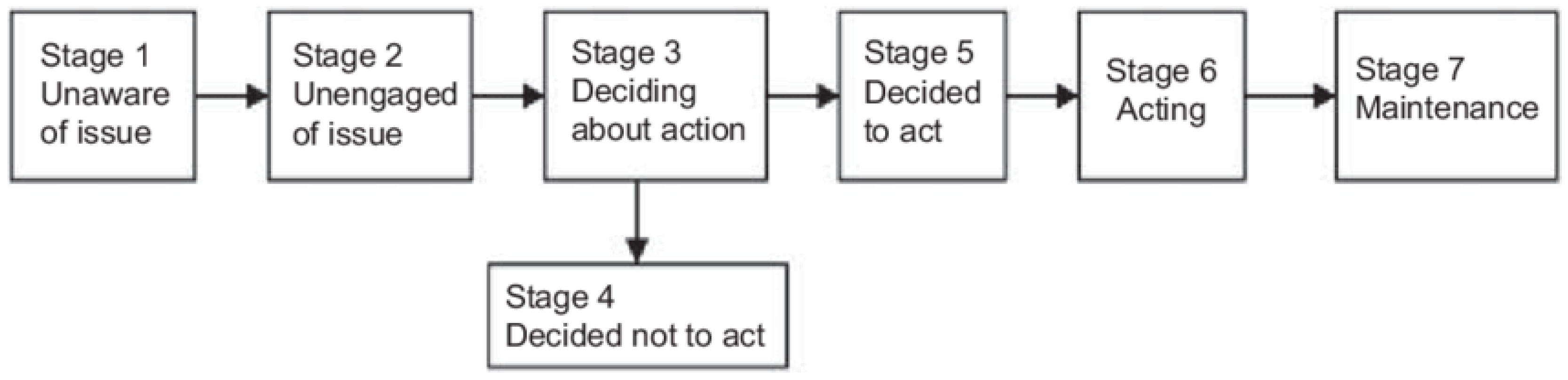
The aim of the study was to use the Integrated Behavioral Model (IBM) and the Precaution Adoption Process Model (PAPM) to identify factors that explained and/or predicted young adults’ decision-making process regarding registering as an organ donor.
3. Results
A total of 550 young adults met the inclusion/exclusion criteria and 407 of them completed the survey (74%). They were non-Hispanic (69.8%), female (51.4%), with a mean age of 20 years old (SD = 2.08). Less than one in four reported ever taking college classes. Respondents were White (34.6%), African American (29.5%), multi-racial (20.6%), Asian (10.8%), and American Indian or Alaska Native (3.7%). Just under a third were Hispanic. Most respondents (63%) did not have a close friend, relative, or loved one who currently needed or had needed an organ transplant in the past nor did they know anyone who had actually donated an organ (61%) (
Table 2).
3.1. Differences in Registration Status by Selected Socio-Demographic Variables
In terms of their current registration status, 28% were unaware of the issue; 19% were unengaged by the issue; 14% were thinking about it and deciding whether to take action; 12% had thought about it and decided not to register; 6% had decided to register in the near future, and 19% had recently registered. Thus, 62% of our respondents had either not heard about registering, never really thought about it, or were undecided.
Caucasians were almost three times more likely to be registered donors (28%) than African Americans (10%) and almost two times more likely to have registered than other races (16%), χ² (3, N = 407) = 15.19, p = 0.002. Older young adults (ages 21–24) were more likely to be registered (25%) than younger adults (ages 18–20), (11%), χ² (2, N = 407) = 2.10, p ≤ 0.001. Those who were registered were more than twice as likely to know someone who donated an organ (34%), compared to non-registrants (14%) χ² (1, N = 407) = 18.23, p ≤ 0.001. No statistically significant differences in registration status were noted by ethnicity, gender, having a close friend, relative, or loved one who currently needs an organ transplant or who needed one in the past, χ² (1, N = 407) = 1.65, p = 0.199.
3.2. Knowledge
Overall, respondents lacked knowledge of organ donation and registration. The proportion of correct answers on the 6-item knowledge test ranged from 18.7% to 43.2%, depending on the item.
Table 3 indicates the proportion of participants who answered correctly (true) or incorrectly (false) for each question statement. Less than 1% of all respondents (
n = 3) answered all six questions correctly. To determine if young adults’ registration status differed in a statistically significant way by their knowledge level, we grouped them into four categories of knowledge based on their scores: (1) None: Zero items correct, (2) Low: 1–2 items correct, (3) Moderate: 3–4 items correct and, (4) High: 5–6 items correct. More registered donors than non-registered were in the “moderate” and “high” knowledge categories. Registered donors were statistically significantly more likely to be in the “high” knowledge category (21%) than non-registrants (3%), χ² (3, N = 407) = 44.69,
p ≤ 0.001. Further, the median knowledge score of those who had registered (3.0) was greater than non-registrants (1.5), U = 7716,
p ≤ 0.001 (See
Table 3).
3.3. Factors outside the IBM That Explained a Past Decision to Register
We wanted to know if factors outside the IBM (e.g., age, race, salience, knowledge) predicted a past decision to register. The regression model was statistically significant, χ2(9) = 99.21, p < 0.001, and explained 35% (Nagelkerke R2) of the variance in a past decision to register, and correctly classified 81% of cases. When controlling for race, Caucasians were 3.6 times more likely to be registered than African Americans (OR: 3.60, 95% CI [1.79, 7.24], p < 0.001). Past history of knowing someone who donated an organ (OR: 3.07, 95% CI [1.81, 5.23], p < 0.001), salience (OR: 2.67, 95% CI [2.04, 3.51], p < 0.001), increasing age (OR: 2.14, 95% CI [1.29, 3.55], p = 0.003), and knowledge (OR: 1.46, 95% CI [1.38, 1.93], p < 0.001) were also statistically significant predictors of a past decision to register.
3.4. IBM Constructs That Explained a Past Decision to Register
Our regression model using the IBM constructs was statistically significant, χ2(7) = 146.91, p < 0.001; explained 49% (Nagelkerke R2) of the variance in a past decision to register; and correctly classified 88% of cases. Direct attitude (OR: 2.13, 95% CI [1.75, 2.59], p < 0.001), indirect descriptive norms (OR: 1.87, 95% CI [1.54, 2.28], p < 0.001), direct subjective norm (OR: 1.82, 95% CI [1.54, 2.16], p < 0.001), direct descriptive norm (OR: 1.78, 95% CI [1.51, 2.08], p < 0.001), indirect subjective norm (OR: 1.08, 95% CI [1.06, 1.10], p < 0.001), and altruistic attitudes (1.07, 95% CI [1.05, 1.09], p < 0.001) were statistically significant predictors of registration status. We did not assess personal agency of registrants since that construct was not applicable to them.
3.5. All Factors Combined That Predicted a Past Decision to Register
We then used multiple binomial logistic regression to assess which of the combined factors (both external to the IBM and within) were the strongest predictors of a past decision to register. Direct attitude (OR: 1.49, 95% CI [1.19, 1.86], p< 0.001), direct descriptive norm (OR: 1.40, 95% CI [1.16, 1.70], p< 0.001), indirect descriptive norm (OR: 1.38, 95% CI [1.06, 1.79], p = 0.018), knowledge (OR: 1.25, 95% CI [1.02, 1.53], p = 0.034), and altruism (OR: 1.03, 95% CI [1.01, 1.06], p = 0.017) were significant predictors of a past decision to register.
3.6. Predicting Behavioral Intentions to Register: Factors External to the IBM
We used binomial logistic regression to determine if factors external to the IBM (e.g., age, race, salience, knowledge) predicted respondents’ behavioral intentions to register in the next year. The logistic regression model was statistically significant, χ2(8) = 4.327, p < 0.001 and explained 29% (Nagelkerke R2) of the variance in behavioral intention. The model correctly classified 89% of cases. Having a history of knowing someone who donated an organ and knowing someone who currently needs an organ were strong predictors of intention. Young adults who knew someone who needed a transplant were almost six times more likely to intend to register compared to those who did not know such a person (OR: 5.67, 95% CI [2.86, 11.27], p < 0.001). Similarly, those who knew an organ donor were also six times more likely to report intention to register (OR: 6.18, 95% CI [3.09, 12.32], p < 0.001). Salience (OR: 2.06, 95% CI [1.47, 2.89], p < 0.001) and knowledge (OR: 1.43, 95% CI [1.14, 1.78], p < 0.001) were also statistically significant predictors of intention.
3.7. Predicting Behavioral Intentions to Register: IBM Constructs
In terms of the impact of the IBM constructs to predict behavioral intention to register, all of the IBM constructs, except altruism beliefs, were statistically significant predictors. The logistic regression model was statistically significant, χ2(8) = 5.273, p < 0.001 and explained 28% (Nagelkerke R2) of the variance in behavioral intention. It correctly classified 90% of cases. Indirect descriptive norm (OR: 1.91, 95% CI [1.48, 2.46], p < 0.001), indirect self-efficacy (OR: 1.77, 95% CI [1.21, 2.557], p = 0.003), direct attitude (OR: 1.62, 95% CI [1.31, 2.02], p < 0.001), direct subjective norm (OR: 1.44, 95% CI [1.20, 1.72], p < 0.001), direct descriptive norm (OR: 1.43, 95% CI [1.20, 1.71], p < 0.001), direct self-efficacy (OR: 1.39, 95% CI [1.18, 1.65], p < 0.001), perceived behavioral control (OR: 1.23, 95% CI [1.06, 1.42], p < 0.001), indirect general attitude (OR: 1.07, 95% CI [1.03, 1.10], p < 0.001), and indirect subjective norm (OR: 1.06, 95% CI [1.03, 1.09], p < 0.001) were statistically significant predictors of registration status.
3.8. Predicting Behavioral Intentions to Register: All Factors Combined
We then used binomial logistic regression to combine and analyze all statistically significant predictors (i.e., both those inside and external to the IBM) of behavioral intentions to register in the future. Young adults who knew someone who currently needed an organ transplant were almost 3 times more likely to intend to register in the next year, (OR: 2.90, 95% CI [1.31, 6.41], p = 0.009). Likewise, young adults who knew someone who was an organ donor were nearly 3 times more likely to intend to register in the next year, (OR: 2.75, 95% CI [1.23, 6.16], p = 0.014). Additionally, indirect descriptive norm, (OR: 1.67, 95% CI [1.22, 2.29], p = 0.001) and direct attitude, (OR: 1.54, 95% CI [1.22, 1.94], p < 0.001) significantly predicted whether someone had intention to register.
4. Discussion
Our finding that only 19% of our sample participants were registered as organ donors was on the low end of past research with this age group. Surprisingly, 62% of our respondents had either not heard about registering, never really thought about it, or were undecided. This lack of awareness is likely reflective of our sample. Our sample of non-college students likely received less education regarding organ donation registration than college students. For example, in our sample, the average knowledge score was very low. In contrast, although the knowledge test was different, college students in the northeast had an average score of 80%, and 44% of them were already registered organ donors [
11]. Increased education has been shown to increase awareness and organ donation registration [
12,
13].
Our sample of non-students included 65% racial/ethnic minorities—much higher than most other studies of college students. Caucasians in our sample were much more likely than racial/ethnic minorities to be registered donors. Our findings are corroborated by past research that has reported lower registration rates among racial/ethnic minorities [
14,
15]. The reticence of Black Americans to register and their negative opinions of organ donation may be due to their experiences with institutional racism and their distrust of the health care system [
16,
17,
18,
19].
Young adults who are racial/ethnic minorities may also be reticent to register as organ donors because of common perceptions that the system for allocating organs to patients is unfair; beliefs that physicians will not provide the best care if one is an organ donor; and beliefs that minorities have a lower chance of being selected to receive a donated organ [
14,
17,
20]. Some of their perceptions may be accurate. For example, Black Americans have a greater need for organs than White Americans. Yet, in a study of almost 1400 patients in need of organs, 1/3 of Black patients were on official transplant lists compared to more than 1/2 of the White patients [
21]. Furthermore, health care providers are less likely to approach people of color about organ donation registration compared to Whites [
16,
22]. For example, white families were more than twice as likely as black families to be approached for organ donation [
22]. Such institutional racism obviously lowers rates of registration and organ donation among racial/ethnic minorities [
16].
In terms of explaining the past decision to register, IBM was useful. By way of review, the constructs of attitudes and perceived norms were statistically significant predictors of past registration. Two factors outside the IBM (i.e., salience and knowledge) were also statistically significant predictors of a past decision to register. When we combined and analyzed all statistically significant predictors, young adults with more positive direct attitudes were 1.5 times more likely to be registered than those with negative direct attitudes. In future health communication campaigns, public health specialists and transplant advocates should emphasize both the cognitive and affective components of attitudes while emphasizing the benefits of registering as a donor.
The IBM was also useful in predicting future behavioral intentions to register. By way of review, the constructs of attitudes (except altruism), perceived norms, and personal agency were statistically significant predictors of intention. Once again, factors outside the IBM, including salience, knowledge, and past history of knowing someone who needed a transplant or knowing a donor, were also predictive of behavioral intentions. When we combined and analyzed all statistically significant predictors, we found that indirect descriptive norm, direct attitude, and a history of knowing a donor and knowing someone who needed a transplant remained statistically significant. Those who knew someone who donated an organ and knew someone who needed a transplant was almost three times more likely to intend to register in the next year than those who did not know such individuals. Such results point to the need to connect young adults who are not yet registered as donors with those who need an organ and those who have served as living donors. Although past research is limited regarding the impact of knowing someone who donated or knowing someone who needs an organ, we would expect that such social influence would be positively influential. Therefore, we strongly recommend that those responsible for organ donation programs find creative ways to connect non-college students and young adults with those who need organs and those who have donated organs in the past. This could be done in person, through virtual means, or via creative health messaging campaigns.
Future studies should use IBM as a needs-assessment tool for planning interventions. Our survey could be used with a similar population of non-college students and young adults. The factors that predict and explain the greatest amount of variance in behavioral intention to register can be identified. Subsequently, interventions can be designed based on the most predictive factors. Young adults can then be randomly assigned to control and intervention groups and the theory-based intervention can be administered. Following the intervention, both the control and intervention groups can be assessed again using the same survey to determine if the intervention improved the construct(s) upon which it was based. Then program participants can be followed into the future and measured again in 6 or 12 months to determine if they actually registered. Such a study would prove beyond a doubt whether IBM was a useful framework for actually changing registration behavior. Another potential research avenue relates to social marketing campaigns targeting young adults, especially those who are minorities or who are not enrolled in post-secondary education. The impact of such campaigns could be assessed using intervention groups and matched control groups. These social marketing campaigns could be done through powerful advertisements that increase positive perceived norms and attitudes towards organ donation. Social media channels could be used to expose young adults to pro organ donation registration messages. These messages could be designed to provide cognitive and affective comfort about organ donation, show the benefits of organ donation, and provide positive normative beliefs about organ donation.
Organ donation tendencies have been explored from a variety of societal and individual-level perspectives. Concepts such as incentive-based versus voluntary donations, demand versus supply, altruism versus narcissism, positive versus negative attitudes, selflessness versus selfishness, and other motivations versus aversions have been employed to explore organ donation preferences [
7,
11,
12,
14,
23,
24,
25]. With the global COVID-19 pandemic, rising medical mistrust, declining altruism, lower social cohesion, and increasing self-interests, organ donation and procurement may become even more challenging. While we did not measure many of these concepts, future studies should consider the inclusion of such measures in organ donation preference research. Also, policy and advocacy initiatives may help alleviate some of the aforementioned barriers. For example, a recently discussed legislation bill in the U.S. (i.e., The Living Donor Protection Act) had certain provisions that could address the aforementioned issues. Some of the key components of the legislation bill were coverage for living donors under the Family and Medical Leave Act (FMLA), prohibition of denial of life, disability, long-term care insurance coverage for donors, and increasing awareness about the benefits of organ donation [
26,
27].
Limitations and Strengths
Our results should be interpreted with its potential limitations and strengths in mind. First, we tested the stability–reliability of the survey with college students. This may have biased our reliability results. Second, the recruitment and sampling method used by Qualtrics did not allow us to calculate a true response rate. Thus, we do not know how many young adults were contacted, looked at the survey, and decided not to start it. Although we were able to calculate a completion rate, it is possible that our study had limitations with external validity. Third, we did not conduct an elicitation phase with the priority population prior to designing our survey items. Thus, although we established face and content validity of the items and included several text boxes in the survey to capture qualitative data, it is possible that the indirect survey items were not as valid as they could have been. Fourth, due to the cross-sectional nature of data collection, we cannot infer any causality and we lack the ability to determine whether respondents who expressed intention to register in the next year actually do so. Fifth, our study may have been hindered by recall bias. Asking respondents about their past decisions is always a potential limitation due to faulty memories. Sixth, while our sample is highly representative of the total population the extent to which the respondents differed from non-respondents could be a threat to the validity of the findings. Also, there could be other sociodemographic characteristics of respondents that could have influenced their responses and we may not have assessed these influential characteristics (e.g., the religion of the respondents, geographical location, etc.). Lastly, social desirability bias may have influenced some of the participants’ answers. If that is the case, the percentage of those registered as organ donors and those stating a positive intention to register in the future may have been overstated.
Our study also features numerous strengths. We used well-accepted theoretical models as the framework of our research. Using proven theories and models in research increases the validity of such research (8). Second, ours was the first study to ever use the IBM and the PAPM to elucidate the decision-making process of a racially diverse sample of non-college students regarding organ donation registration—a population that has been grossly understudied. The majority of our respondents (65%) were racial/ethnic minorities—which is very rare in this line of investigation. Third, we designed a valid and reliable survey that can be used by researchers in the future. Our findings provide many new insights into this important yet under-researched population. Lastly, our study was also the first to assess non-college student young adults from the ten states in the U.S. with the lowest organ donation registration rates. Hence, our results will be of great importance to those who are responsible for organ donation registration and for procuring organs from both living and deceased donors.
The low rate of organ donation registration among our sample indicates that there is much work to be done, especially among racial/ethnic minorities. There is a significant need for culturally appropriate messaging and educational programs tailored to this unique population. Those who are promoting organ donation in the U.S., especially in the ten states with the lowest rates of registration, can use our results to design future health communication and education campaigns for this important population.







{kind=link}
{kind=link}