Religion- and Spirituality-Based Effects on Health-Related Components with Special Reference to Physical Activity: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction
3. Results
3.1. Selected Articles
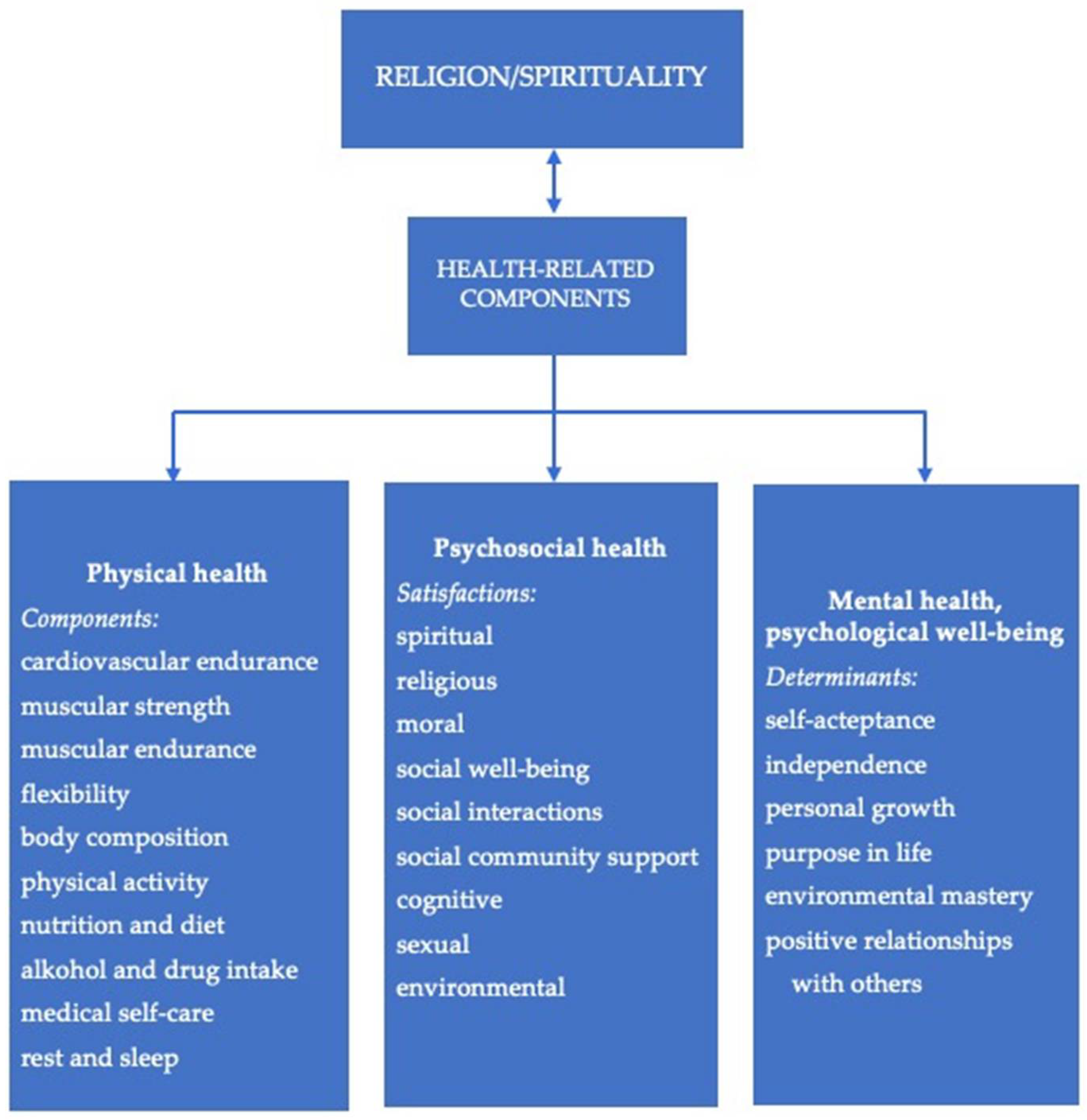
3.2. Role of Religion and Spirituality in Mental and Physical Health
3.3. Religion, Spirituality and, Physical Activity
3.3.1. Findings from Reviews
3.3.2. Findings from Experimental Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aggarwal, Shilpa, Judith Wright, Amy Morgan, George Patton, and Nicola Reavley. 2023. Religiosity and spirituality in the prevention and management of depression and anxiety in young people: A systematic review and meta-analysis. BMC Psychiatry 23: 729. [Google Scholar] [CrossRef]
- Ahrenfeldt, Linda J., Sören Möller, Niels C. Hvidt, and Rune Lindahl-Jacobsen. 2018. Religiousness and lifestyle among Europeans in SHARE. Public Health 165: 74–81. [Google Scholar] [CrossRef]
- Al Eid, Nawal A., Mohammed Mj Alqahtani, Khaldoun Marwa, Boshra A Arnout, Hajar S Alswailem, and Al Anoud Al Toaimi. 2020. Religiosity, psychological resilience, and mental health among breast cancer patients in Kingdom of Saudi Arabia. Breast Cancer: Basic and Clinical Research 14: 1178223420903054. [Google Scholar] [CrossRef]
- Almaraz, David, Jesús Saiz, Florentino Moreno Martín, Iván Sánchez-Iglesias, Antonio J. Molina, and Tamara L. Goldsby. 2022. What aspects of religion and spirituality affect the physical health of cancer patients? A systematic review. Healthcare 10: 1447. [Google Scholar] [CrossRef]
- Alves, Sabrina Alaíde Amorim, and Maryldes Lucena Bezerra de Oliveira. 2018. Sociocultural aspects of health and disease and their pragmatic impact. Journal of Human Growth and Development 28: 183–88. [Google Scholar] [CrossRef]
- Ansari, Serene, Erica G. Soltero, Elizabeth Lorenzo, and Rebecca E. Lee. 2017. The impact of religiosity on dietary habits and physical activity in minority women participating in the Health is Power (HIP) study. Preventive Medicine Reports 5: 210–13. [Google Scholar] [CrossRef]
- Arredondo, Elva M., John P. Elder, Jessica Haughton, Donald J. Slymen, James F. Sallis, Lilian G. Perez, Natalicio Serrano, Maíra T. Parra, Rodrigo Valdivia, and Guadalupe X. Ayala. 2017. Fe en Acción: Promoting physical activity among churchgoing Latinas. American Journal of Public Health 107: 1109–15. [Google Scholar] [CrossRef]
- Balish, Shea M., Dan Conacher, and Lori Dithurbide. 2016. Sport and Recreation Are Associated With Happiness Across Countries. Research Quarterly for Exercise and Sport 87: 382–88. [Google Scholar] [CrossRef]
- Basu-Zharku, Iulia O. 2011. The influence of religion on health. Inquiries Journal 3: 1–3. [Google Scholar]
- Bauman, Adrian E., Rodrigo S. Reis, James F. Sallis, Jonathan C. Wells, Ruth Jf Loos, and Brian W. Martin. 2012. Correlates of physical activity: Why are some people physically active and others not? The Lancet 380: 258–71. [Google Scholar] [CrossRef]
- Blankinship, Lisa A., William A. Rouse, Joshua Bernstein, Joanna Kruk, and Basil H. Aboul-Enein. 2021. A narrative review of ethnic minority studies for faith-based health promotion interventions with special reference to the contemporary Christian Nurse. Journal of Religion and Health 60: 1375–87. [Google Scholar] [CrossRef] [PubMed]
- Bopp, Melissa, Jane A. Peterson, and Benjamin L. Webb. 2012. A comprehensive review of faith-based physical activity interventions. American Journal of Lifestyle Medicine 6: 460–78. [Google Scholar] [CrossRef]
- Borges, Cezimar Correia, dos Patrícia Roberta Santos, Polissandro Mortoza Alves, Renata Custódio Maciel Borges, Giancarlo Lucchetti, Maria Alves Barbosa, Celmo Celeno Porto, and Marcos Rassi Fernandes. 2021. Association between spirituality/religiousness and quality of life among healthy adults: A systematic review. Health and Quality of Life Outcomes 19: 246. [Google Scholar] [CrossRef] [PubMed]
- Bull, Fiona C., Salih S. Al-Ansari, Stuart Biddle, Katja Borodulin, Matthew P Buman, Greet Cardon, Catherine Carty, Jean-Philippe Chaput, Sebastien Chastin, Roger Chou, and et al. 2020. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine 54: 1451–62. [Google Scholar] [CrossRef] [PubMed]
- Buro, Acadia W., Tiffany L. Carson, Brent J. Small, Wenyi Fan, Laura B. Oswald, Heather S. L. Jim, Endrina Salas, Kellie Zambrano, Crystal Bryant, Kosj Yamoah, and et al. 2023. Sociocultural factors associated with physical activity in Black prostate cancer survivors. Supportive Care in Cancer 31: 482. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, Érica, Daniel A. Marinho, Henrique P. Neiva, and Olga Lourenço. 2020. Inflammatory effects of high and moderate intensity exercise—A systematic review. Frontiers in Physiology 10: 1550. [Google Scholar] [CrossRef]
- Chen, Ying, Eric S. Kim, and Tyler J. VanderWeele. 2021. Religious-service attendance and subsequent health and well-being throughout adulthood: Evidence from three prospective cohorts. International Journal of Epidemiology 49: 2030–40. [Google Scholar] [CrossRef]
- de Diego-Cordero, Rocío, Paola Suárez-Reina, Bárbara Badanta, Giancarlo Lucchetti, and Juan Vega-Escaño. 2022. The efficacy of religious and spiritual interventions in nursing care to promote mental, physical and spiritual health: A systematic review and meta-analysis. Applied Nursing Research 67: 151618. [Google Scholar] [CrossRef] [PubMed]
- Doyle, David Matthew, and Bruce G. Link. 2024. On social health: History, conceptualization, and population patterning. Health Psychology Review 13: 1–30. [Google Scholar] [CrossRef]
- Duru, O. Kenrik, Catherine A. Sarkisian, Mei Leng, and Carol M. Mangione. 2010. Sisters in motion: A randomized controlled trial of a faith-based physical activity intervention. Journal of the American Geriatrics Society 58: 1863–69. [Google Scholar] [CrossRef]
- Ferreira, Laura Fernandes, Alyssa De Pinho Freire, Ana Luiza Cunha Silveira, Anthony Pereira Martins Silva, de Hermon Corrêa Sá, Igor Soares Souza, Lohane Stefany Araújo Garcia, Rafael Silva Peralta, and Laís Moreira Borges Araujo. 2020. The influence of spirituality and religiosity in acceptance of the disease and treatment of oncologic patients: An integrative literature review. Revista Brasileira de Cancerologia 66: e-07422. [Google Scholar] [CrossRef]
- Goerge, Ally, Maureen Sanderson, Cristen Flewellen, Katherine Busen, and Sarah Nechuta. 2023. The role of spirituality on physical activity and sleep among African American long-term breast cancer survivors. Journal of Racial and Ethnic Health Disparities, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, Juliane Piasseschi de Bernardin, Giancarlo Lucchetti, Paulo Rossi Menezes, and Homero Vallada. 2017. Complementary religious and spiritual interventions in physical health and quality of life: A systematic review of randomized controlled clinical trials. PLoS ONE 12: e0186539. [Google Scholar] [CrossRef] [PubMed]
- Gschwandtner, Christina M. 2021. Faith, religion, and spirituality: A phenomenological and hermeneutic contribution to parsing the distinctions. Religions 12: 476. [Google Scholar] [CrossRef]
- Hamdan, Abdullah Bany, Fawzi Al-Odeh, Sherwynn Javison, Abdullah AlSuheil, Sami Alshammary, and Musa AlHarbi. 2020. Religious belief and social support among cancer patients in Saudi Arabia. Cureus 12: e7012. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, Seyed-Mehdi, Mohammadreza Hormozi, Abolghasem Allahyari, Ali Arash Anoushirvani, Zahra Ameri, and Samaneh Ghasemipour. 2020. The prevalence of depression, anxiety, and stress in patients with breast cancer in Southeast Iran in 2019: A cross-sectional study. Oncology in Clinical Practice 16: 104–8. [Google Scholar] [CrossRef]
- Helmerhorst, Hendrik Hendrik JF, Søren Brage, Janet Warren, Herve Besson, and Ulf Ekelund. 2012. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. International Journal of Behavioral Nutrition and Physical Activity 9: 103–3. [Google Scholar] [CrossRef] [PubMed]
- Hussain, Umer, and George B. Cunningham. 2023. Physical activity among Muslim women: The roles of religious identity, health consciousness, and Muslim population density. Cogent Social Sciences 9: 2244839. [Google Scholar] [CrossRef]
- Irwin, Melinda L. 2009. Physical activity interventions for cancer survivors. British Journal of Sports Medicine 43: 32–38. [Google Scholar] [CrossRef]
- Jim, Heather S. L., James E. Pustejovsky, Crystal L. Park, Suzanne C. Danhauer, Allen C. Sherman, George Fitchett, Thomas V. Merluzzi, Alexis R. Munoz, Login George, Mallory A. Snyder, and et al. 2015. Religion, spirituality, and physical health in cancer patients: A meta-analysis. Cancer 121: 3760–68. [Google Scholar] [CrossRef]
- Jona, I. N., and F. T. Okou. 2013. Sports and religion. Asian Journal of Management Sciences & Education 2: 46–54. [Google Scholar]
- Kang, Mina, La Young Park, Seo Young Kang, Jisun Lim, and Young Sik Kim. 2020. Religion and health behaviors in primary care patients. Korean Journal of Family Medicine 41: 105–10. [Google Scholar] [CrossRef]
- Koenig, Harold G. 2012. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012: 278730. [Google Scholar] [CrossRef]
- Koenig, Harold G., Tyler VanderWeele, and John R. Peteet. 2023. Handbook of Religion and Health, 3rd ed. New York: Oxford Academic. [Google Scholar] [CrossRef]
- Kopeyko, Grigory, Olga Alexandrovna Borisova, E. V. Gedevani, and Vasilii Glebovich Kaleda. 2020. Vliianie faktora religioznosti na depressivnye sostoianiia i suitsidal’noe povedenie [The influence of religiosity on depressive disorders and suicidal behavior]. S.S. Korsakov Journal of Neurology and Psychiatry 120: 103–10. [Google Scholar] [CrossRef]
- Kowalczyk, Oliwia, Krzysztof Roszkowski, Wojciech Pawliszak, Agnieszka Rypel, Szymon Roszkowski, Jolanta Kowalska, Bartosz Tylkowski, and Anna Bajek. 2022. Religion and spirituality in oncology: An exploratory study of the communication experiences of clinicians in Poland. Journal of Religion and Health 61: 1366–75. [Google Scholar] [CrossRef]
- Kruk, Joanna, Basil Hassan Aboul-Enein, Joshua Bernstein, and Magdalena Gronostaj. 2019a. Psychological stress and cellular aging in cancer: A meta-analysis. Oxidative Medicine and Cellular Longevity 2019: 1270397. [Google Scholar] [CrossRef]
- Kruk, Joanna, Hassan Y. Aboul-Enein, Aleksandra Kładna, E. Jacquelyn, and Jacquelyn E. Bowser. 2019b. Oxidative stress in biological systems and its relation with pathophysiological functions: The effect of physical activity on cellular redox homeostasis. Free Radical Research 53: 497–521. [Google Scholar] [CrossRef]
- Kvesić, Antonija, Dragan Babic, Darjan Franjic, Inga Marijanovic, Romana Babic, and Marko Martinac. 2020. Correlation of religiousness with the quality of life and psychological symptoms in oncology patients. Psychiatria Danubina 32 Suppl. S2: 254–61. [Google Scholar]
- Lee, Paul H., Duncan J. Macfarlane, TH Lam, and Sunita M. Stewart. 2011. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. International Journal of Behavioral Nutrition and Physical Activity 8: 115–15. [Google Scholar] [CrossRef]
- Lucchetti, Giancarlo, Harold G. Koenig, and Alessandra Lamas Granero Lucchetti. 2021. Spirituality, religiousness, and mental health: A review of the current scientific evidence. World Journal of Clinical Cases 9: 7620–31. [Google Scholar] [CrossRef]
- Lumpkins, Crystal Y., K Allen Greiner, Christine Daley, Jannette Berkley-Patton, Jinxiang Hu, and Shana Palla. 2019. An exploratory analysis of the role of religion in colorectal cancer screening among safety-net clinic patients. Journal of Geriatric Medicine and Gerontology 5: 058. [Google Scholar] [CrossRef]
- Malm, Christer, Johan Jakobsson, and Andreas Isaksson. 2019. Physical Activity and Sports—Real Health Benefits: A Review with Insight into the Public Health of Sweden. Sports 7: 127. [Google Scholar] [CrossRef]
- Maroney, Kieran, Jodie Laurent, Flor Alvarado, Alexandra Gabor, Caryn Bell, Keith Ferdinand, Jiang He, and Katherine T. Mills. 2023. Systematic review and meta-analysis of church-based interventions to improve cardiovascular disease risk factors. The American Journal of the Medical Sciences 366: 199–208. [Google Scholar] [CrossRef]
- McManus, Deborah Tessitore. 2024. The intersection of spirituality, religiosity, and lifestyle practices in religious communities to successful aging: A review article. Religions 15: 478. [Google Scholar] [CrossRef]
- Moreira, Wanderson Carneiro, Maria Do Perpétuo Socorro de Sousa Nóbrega, Fernanda Púpio Silva Lima, Eliana Campêlo Lago, and Mário Oliveira Lima. 2020. Effects of the association between spirituality, religiosity and physical activity on health/mental health: A systematic review. Revista da Escola de Enfermagem da USP 54: e03631. [Google Scholar] [CrossRef] [PubMed]
- Neufer, P. Darrell, Marcas M. Bamman, Deborah M. Muoio, Claude Bouchard, Dan M. Cooper, Bret H. Goodpaster, Frank W. Booth, Wendy M. Kohrt, Robert E. Gerszten, Mark P. Mattson, and et al. 2015. Understanding the cellular and molecular mechanisms of physical activity-induced health benefits. Cell Metabolism 22: 4–11. [Google Scholar] [CrossRef] [PubMed]
- Noh, Young-Eun, and Syazana Shahdan. 2020. A systematic review of religion/spirituality and sport: A psychological perspective. Psychology of Sport and Exercise 46: 101603. [Google Scholar] [CrossRef]
- Noh, Young-Eun, Boon Hooi Lim, and Mahmoud Danaee. 2023. Motives for physical activity participation: Does religious faith play a mediating role? International Journal of Sport and Exercise Psychology 21: 787–806. [Google Scholar] [CrossRef]
- Odynets, Tetiana, Yuriy Briskin, Valentina Todorova, and Olha Bondarenko. 2019. Impact of different exercise interventions on anxiety and depression in breast cancer patients. Physiotherapy Quarterly 27: 31–36. [Google Scholar] [CrossRef]
- Parra, Maíra Tristão, Gustavo J. M. Porfírio, Elva M. Arredondo, and Álvaro N. Atallah. 2018. Physical activity interventions in faith-based organizations: A systematic review. American Journal of Health Promotion 32: 677–90. [Google Scholar] [CrossRef]
- Paul Victor, Chitra G., and Judith V. Treschuk. 2020. Critical Literature Review on the Definition Clarity of the Concept of Faith, Religion, and Spirituality. Journal of Holistic Nursing 38: 107–13. [Google Scholar] [CrossRef]
- Powell, Lynda H., Leila Shahabi, and Carl E. Thoresen. 2003. Religion and spirituality: Linkages to physical health. American Psychologist 58: 36–52. [Google Scholar] [CrossRef] [PubMed]
- Rassouli, Maryam, Vahid Zamanzadeh, Akram Ghahramanian, Abbas Abbaszadeh, Hamid Alavi-Majd, and Alireza Nikanfar. 2015. Experiences of patients with cancer and their nurses on the conditions of spiritual care and spiritual interventions in oncology units. Iranian Journal of Nursing and Midwifery Research 20: 25–33. [Google Scholar] [PubMed]
- Rathod, Kalwyna. 2021. What Are the Health-Skill Related Components of Physical Fitness. Available online: https://www.femina.in/wellness/fitness/components-of-physical-fitness-183555.html (accessed on 30 March 2024).
- Reisi, Sajjad, Seyed Mojtaba Ahmadi, and Kheirollah Sadeghi. 2021. The effect of religion and spirituality on anxiety and depression in cancer patients: A review article. Journal of Quran and Medicine 6: 75–86. [Google Scholar]
- Rizvi, Mohd Ahsan Kabir, and Mohammad Zakir Hossain. 2017. Relationship between religious belief and happiness: A systematic literature review. Journal of Religion and Health 56: 1561–82. [Google Scholar] [CrossRef]
- Salsman, John M., James E. Pustejovsky, Heather S. L. Jim, Alexis R. Munoz, Thomas V. Merluzzi, Login George, Crystal L. Park, Suzanne C. Danhauer, Allen C. Sherman, Mallory A. Snyder, and et al. 2015. A meta-analytic approach to examining the correlation between religion/spirituality and mental health in cancer. Cancer 121: 3769–78. [Google Scholar] [CrossRef]
- Saxena, S., M. Van Ommeren, K. C. Tang, and T. P. Armstrong. 2005. Mental health benefits of physical activity. Journal of Mental Health 14: 445–51. [Google Scholar] [CrossRef]
- Schlundt, David G., Monica D. Franklin, Kushal Patel, Linda McClellan, Celia Larson, Sarah Niebler, and Margaret Hargreaves. 2008. Religious affiliation, health behaviors and outcomes: Nashville REACH 2010. American Journal of Health Behavior 32: 714–24. [Google Scholar] [CrossRef] [PubMed]
- Seeman, Teresa E., Linda Fagan Dubin, and Melvin Seeman. 2003. Religiosity/spirituality and health: A critical review of the evidence for biological pathways. American Psychologist 58: 53–63. [Google Scholar] [CrossRef]
- Shattuck, Eric C., and Michael P. Muehlenbein. 2020. Religiosity/spirituality and physiological markers of health. Journal of Religion and Health 59: 1035–54. [Google Scholar] [CrossRef]
- Sherman, Allen C., Thomas V. Merluzzi, James E. Pustejovsky, Crystal L. Park, Login George, George Fitchett, Heather S. L. Jim, Alexis R. Munoz, Suzanne C. Danhauer, Mallory A. Snyder, and et al. 2015. A meta-analytic review of religious or spiritual involvement and social health among cancer patients. Cancer 121: 3779–88. [Google Scholar] [CrossRef]
- Shojaee, Mahnaz, and Carmel French. 2014. The relationship between mental health components and locus of control in youth. Psychology 5: 966–78. [Google Scholar] [CrossRef]
- Silfee, Valerie J., Christina F. Haughton, Stephenie C. Lemon, Vilma Lora, and Milagros C. Rosal. 2017. Spirituality and physical activity and sedentary behavior among Latino men and women in Massachusetts. Ethnicity & Disease 27: 3–10. [Google Scholar] [CrossRef]
- Silverman, Marni N., and Patricia A. Deuster. 2014. Biological mechanisms underlying the role of physical fitness in health and resilience. Interface Focus 4: 20140040. [Google Scholar] [CrossRef] [PubMed]
- Stehr, Paula, Hanna Luetke Lanfer, and Constanze Rossmann. 2021. Beliefs and motivation regarding physical activity among older adults in Germany: Results of a qualitative study. International Journal of Qualitative Studies on Health and Well-Being 16: 1932025. [Google Scholar] [CrossRef] [PubMed]
- Stelmach, Marian. 2018. Physical activity assessment tools in monitoring physical activity: The Global Physical Activity Questionnaire (GPAQ), the International Physical Activity Questionnaire (IPAQ) or accelerometers—Choosing the best tools. Health Problems of Civilization 12: 57–63. [Google Scholar] [CrossRef]
- Sun, Hengwen, Yuan Yang, Jingying Zhang, Ting Liu, Hongmei Wang, Samradhvi Garg, and Bin Zhang. 2019. Fear of cancer recurrence, anxiety and depressive symptoms in adolescent and young adult cancer patients. Neuropsychiatric Disease and Treatment 15: 857–65. [Google Scholar] [CrossRef] [PubMed]
- Svensson, Nanna Herning, Niels Christian Hvidt, Susanne Pagh Nissen, Maria Munch Storsveen, Elisabeth Assing Hvidt, Jens Søndergaard, and Trine Thilsing. 2020. Religiosity and health-related risk behaviours in a secular culture—Is there a correlation? Journal of Religion and Health 59: 2381–96. [Google Scholar] [CrossRef] [PubMed]
- Tejero-González, Carlos M. 2020. Participating in sports and practicing a religion are related to levels of happiness. Physical Culture and Sport. Studies and Research 88: 11–17. [Google Scholar] [CrossRef]
- VanderWeele, Tyler J. 2017. Physical activity and physical and mental well-being in church settings. American Journal of Public Health 107: 1023–24. [Google Scholar] [CrossRef] [PubMed]
- Vitorino, Luciano Magalhães, Giancarlo Lucchetti, Frederico Camelo Leão, Homero Vallada, and Mario Fernando Prieto Peres. 2018. The association between spirituality and religiousness and mental health. Scientific Reports 8: 17233. [Google Scholar] [CrossRef]
- Wankel, Leonard M., and Bonnie G. Berger. 1990. The psychological and social benefits of sport and physical activity. Journal of Leisure Research 22: 167–82. [Google Scholar] [CrossRef]
- Warburton, Darren E.R., Crystal Whitney Nicol, and Shannon S.D. Bredin. 2006. Health benefits of physical activity: The evidence. CMAJ: Canadian Medical Association Journal 174: 801–9. [Google Scholar] [CrossRef] [PubMed]
- Waters, Edward K., Zelda Doyle, and Ellen Finlay. 2018. Spirituality/Religiosity (SpR), leisure-time physical activity, and sedentary behaviour in students at a Catholic University. Journal of Religion and Health 57: 869–82. [Google Scholar] [CrossRef] [PubMed]
- Whitt-Glover, Melicia C., Moses V. Goldmon, Ziya Gizlice, Marie Sillice, Lyndsey Hornbuckle, and Daniel P. Heil. 2017. Increasing physical activity in black women: Results from a randomized trial conducted in faith-based settings. Ethnicity & Disease 27: 411–20. [Google Scholar] [CrossRef]
- Wilcox, Sara, Ruth P. Saunders, Andrew T. Kaczynski, Melinda Forthofer, Patricia A. Sharpe, Cheryl Goodwin, Margaret Condrasky, Vernon L. Kennedy, Danielle E. Jake-Schoffman, Deborah Kinnard, and et al. 2018. Faith, activity, and nutrition randomized dissemination and implementation study: Countywide adoption, reach, and effectiveness. American Journal of Preventive Medicine 54: 776–85. [Google Scholar] [CrossRef] [PubMed]
- Yan, Bo, Xinyi Xu, Denise Shuk Ting Cheung, and Chia-Chin Lin. 2020. Spiritual and religious interventions for adults with cancer and their carers: An overview of systematic reviews. Cochrane Database of Systematic Reviews 2020: CD013675. [Google Scholar] [CrossRef]
- You, Tongjian, Nicole C. Arsenis, Beth L. Disanzo, and Michael J. LaMonte. 2013. Effects of exercise training on chronic inflammation in obesity. Sports Medicine 43: 243–56. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author/Year/Location/Reference | Design, Sample/Period/Objectives | Religion/Spirituality Assessment/Instruments | PA/PE Detection | Main Results | Author’s Conclusions |
|---|---|---|---|---|---|
| Ahrenfeldt et al. 2018, Europe | Longitudinal study (11 years); cohort n = 23,864, aged 50+ years. Religion: Protestants, Catholic, Orthodox, Muslims, others (13.4%), none. To examine association between religiousness and lifestyle determinants | Self-reported participation in a religious organization, frequency of praying during the past month, religious education, and affiliation | Answers on three questions informing about frequency of engaging in PA of moderate and vigorous intensity | Praying or participation in religious organization lowered risk of physical inactivity: OR = 0.88 (0.79–0.98), OR = 0.54 (0.48–0.61); or performing no vigorous PA: OR = 0.92 (0.85–0.98), OR = 0.63 (0.58–0.68), respectively | Strong positive association between R and PA and lifestyle for the more religious people |
| Ansari et al. 2017, USA | RCT; n = 132 women (aged 25–60 years), African American, Hispanic/Latina; religion: Protestant, Catholic, Jewish, other, nonreligious; 6-month intervention. To determine the impact of R and S on PA and diet | The National Institute of Aging/Fetzer Short-Form Questionnaire for Measurement of Religiousness and Spirituality (testing traditional religion/ non-institutional spirituality) | The International Physical Activity Questionnaire Long Form (IPAQ). Self-reported walking, leisure-time, and total PA over the last 7 days were measured | Insignificantly increased total, leisure time PA and walking by 413, 432, and 64 MET-min/wk, respectively, vs. baseline | There was no association between R/S and changes in PA and diet |
| Arredondo et al. 2017, USA | RCT; 436 Latina adults aged 18–65 years from 16 Catholic churches; 12-month PA intervention. To evaluate the impact of faith-based intervention to promote PA | Participants declared attending church for the next 24 months | Accelerometer; assessed moderate to vigorous leisure PA; self-reported activity measure using the World Health Organization’s Global Physical Activity Questionnaire (GPAQ) | Significant increase in PA duration by 22 min/wk (accelerometer usage) and by 40 min/wk (self-reported leisure-time PA) relative to baseline | A faith-based intervention significantly increases PA of moderate to vigorous intensity |
| Buro et al. 2023, USA | Cross-sectional; 257 Black prostate cancer survivors aged ≥20 years, mean age 68.7 years. To examine relation between religiosity and cancer fatalism in relation to PA levels | Religiosity assessed by the Lukwago Religiosity scale: low religious belief, religious belief, religious behavior, high religiosity (high belief and behavior) | Valid in cancer survivors: Godin–Shephard Leisure-Time Physical Activity Questionnaire; PA duration (min/wk) and intensity (METs) assessment; activity dichotomized as meeting the ACS guidelines | Weekly duration PA was positively correlated with religiosity (β = 0.54); no significant interaction between religiosity and PA of moderate intensity; negative association between fatalism and meeting ACS guidelines (OR = 0.87 (0.77–0.99) | Religiosity may be positively associated with some forms of PA |
| Goerge et al. 2023, USA | Cros-sectional; 323 breast cancer survivors, 59.1 years. To examine the effect of spirituality on PA and sleep duration | Validated measures for spirituality using questionnaire (the range of spirituality scores 7–48) | The Arizona Activity Frequency Questionnaire (a modified version); engaging in all domains of PA (min/wk) was determined | Positive association between spirituality score and higher levels of PA; activity duration ≥681 min/wk, OR = 1.90 (1.03–3.50); meeting PA guidelines (≥150 min/wk), OR = 1.78 (1.0–2.98) | Higher spirituality scores increased the likelihood of practicing PA |
| Hussain and Cunningham 2023, USA | Cross-sectional; 177 Muslim women living in USA and 322 living in 34 countries aged 18–65 years. To examine association between religious identity and PA | Questionnaire measuring religious identity and reporting that Islam is essential part of women’s personality | Questionnaire assessed PA using a single question about the likelihood of engaging in moderate intensity activity during the next free weeks | Religious identity was significantly associated with PA intentions (β = 4.746), as well as with self-reported PA (β = 7.344) | Positive correlations between religious identity and predicted PA intention in Muslim women |
| Kang et al. 2020, South Korea | Cohort study; 973 participants (47.8% men): 345 Christian, 153 Roman Catholic, 308 Buddhist, 163 non-religious aged ≥ 18 years; April 2009–June 2011. To examine the association between religion and health behavior | Religious affiliation and status were determined | Duration and intensity of PA in the last 7 days tested using IPAQ—Short Form | Significant increase in vigorous PA; OR = 2.20 (1.31–3.67) only in Catholics; decreased alcohol drinking in Christians vs. control | Positive significant association between religiosity and vigorous PA in Catholics |
| Noh et al. 2023, Malaysia | Cross-sectional; 689 volunteers (390 males, 299 females) aged 18–65 years; Religion: Islam (77.4%), Christianity (12.2%) Buddhism (6.8%) Hinduism (3.5%) Catholicism (0.1%). To examine impact of religious faith on PA | Strength of religious faith measured using the Santa Clara Strength of Religious Faith Questionnaire (41 items) | Self-administered Physical Activity Questionnaire (type, intensity, and duration of moderate and vigorous PA evaluated); the Physical Activity and Leisure Motivation Scale for motivation of recreational activity used | Positive correlations between extrinsic motivation to engage in PA and intrinsic motivation to exercise; there was no association between these motives and engaging in activity | Religious faith did not mediate changes in PA |
| Silfee et al. 2017, USA | Cross-sectional; 602 Latino and Hispanic adults aged 21–85 years. To examine the association between spirituality, PA, and sedentary lifestyle | Spirituality assessed by the Daily Spirituality Experience Scale; religion determined by frequency of going to church or to a religious service in the past month | The Women’s Health Initiative Brief Physical Activity Questionnaire and the Sedentary Behavior Questionnaire; walking and leisure-time PA weekly duration and frequency measured | Significantly decreased sedentary behavior (β = −0.12, p = 0.004) in men and non-significant increase in engaging in >150 min/week PA caused by higher spirituality; OR = 1.12 (0.91–1.38) | Spirituality reduces a sedentary lifestyle, especially in men. A lack of association between spirituality and PA dose exceeding ACS guidelines |
| Svensson et al. 2020, Denmark | Cross-sectional; 1024 individuals aged 29–60 years. To examine association between religiosity and health related risk factors | Questionnaire assessed religious attendance in churches/mosques and prayer/meditation practice; last year | Questionnaire assessed PA: Categorization: inactive (primarily sedentary behavior); active (participation in sport competition or recreational sports ≥4 h/wk, or walking/cycling or heavy gardening) | Physically inactive individuals reporting opening towards church/mosque attendance had lower risk of disease vs. individuals not practicing religion, OR = 0.60 (0.40–0.90) | Religious practice may be positively correlated with health lifestyle determinants, including PA |
| Waters et al. 2018, Australia | Cross-sectional; 185 students at a Catholic University (76% females), aged 18–34 years; 13 options for religious affiliation, a 7-day recall. To examine association between religion and spirituality, recreational PA, and sedentary lifestyle | 17 questions from the Spiritual and Religious Attitudes in Dealing with Illness Questionnaire relating to beliefs and levels of engagement | Four questions from IPAQ used for leisure time PA and five question for sedentary behavior | Respondents with high scores in spiritual practice components undertook moderate PA; frequency and duration were age dependent: the highest frequency in group 20–24 years (OR = 2.21) and longest duration in 20–24 years (0.69 h) vs. other age groups | Spirituality may increase PA, causing undertaking more frequently exercise of moderate intensity |
| Whitt-Glover et al. 2017, USA | RCT; African American women aged >18 years from 31 churches (each church 12–15 women); women divided into: faith-integrated (Group 1), secular intervention (Group 2), controls (Group 3). To compare a faith-integrated and a secular intervention group regarding PA with controls | Faith curriculum included biblical scripture and faith tenets. Secular curriculum was similar but did not include references to scripture or faith tenets | Physical activity measured using pedometer and accelerometer; women participated in 24 sessions weekly for four months (16 sessions) and monthly for four months (4 sessions) | Significantly increased daily walking over baseline by 1451, 1107 steps/day after 10 months of intervention in Groups 1 and 2, respectively, vs. Group 3; increases kept up after 22 months in Group 1. | The faith-integrated intervention allows short- and long-term increasing of PA |
| Wilcox et al. 2018, USA | RCT; 54 churches; 1308 participants; religions: Presbyterian, African, Methodist, Baptist; interventions: churches 36, control churches 18; mean age 53 years (12-month study). To study countrywide adoption, reach, and effectiveness from faith and increases in recreational PA | Implementation of religion and faith program in church attendance; ccommittees focused on creating opportunity for exercise, sharing messages about PA, distributing bulletins, and engaging pastors in PA | Overview of PA using six questions from the 2010 Behavioral Risk Factor Surveillance System PA module; pedometer measurements; classification into two PA levels: inactive (<10 min/wk) and regularly active (≥150 min/wk of moderate PA or ≥75 min/wk of vigorous PA or an equivalent combination) | Intervention church attendees reported more frequent PA opportunities, messages, and pastor support vs. control church attendees; lower proportion of physically inactive attendees in intervention churches vs. control churches (24 month maintenance); Cohen’s d for continuous out-come (0.96) | The intervention program, despite the minimal training and intervention duration, may be suited for wider dissemination, particularly in predominantly African American churches |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kruk, J.; Aboul-Enein, B.H. Religion- and Spirituality-Based Effects on Health-Related Components with Special Reference to Physical Activity: A Systematic Review. Religions 2024, 15, 835. https://doi.org/10.3390/rel15070835
Kruk J, Aboul-Enein BH. Religion- and Spirituality-Based Effects on Health-Related Components with Special Reference to Physical Activity: A Systematic Review. Religions. 2024; 15(7):835. https://doi.org/10.3390/rel15070835
Chicago/Turabian StyleKruk, Joanna, and Basil Hassan Aboul-Enein. 2024. "Religion- and Spirituality-Based Effects on Health-Related Components with Special Reference to Physical Activity: A Systematic Review" Religions 15, no. 7: 835. https://doi.org/10.3390/rel15070835
APA StyleKruk, J., & Aboul-Enein, B. H. (2024). Religion- and Spirituality-Based Effects on Health-Related Components with Special Reference to Physical Activity: A Systematic Review. Religions, 15(7), 835. https://doi.org/10.3390/rel15070835