The Impact of Hypoxic Hepatitis on Clinical Outcomes after Extracorporeal Cardiopulmonary Resuscitation

 ,
,  and
and
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection, Definitions, and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
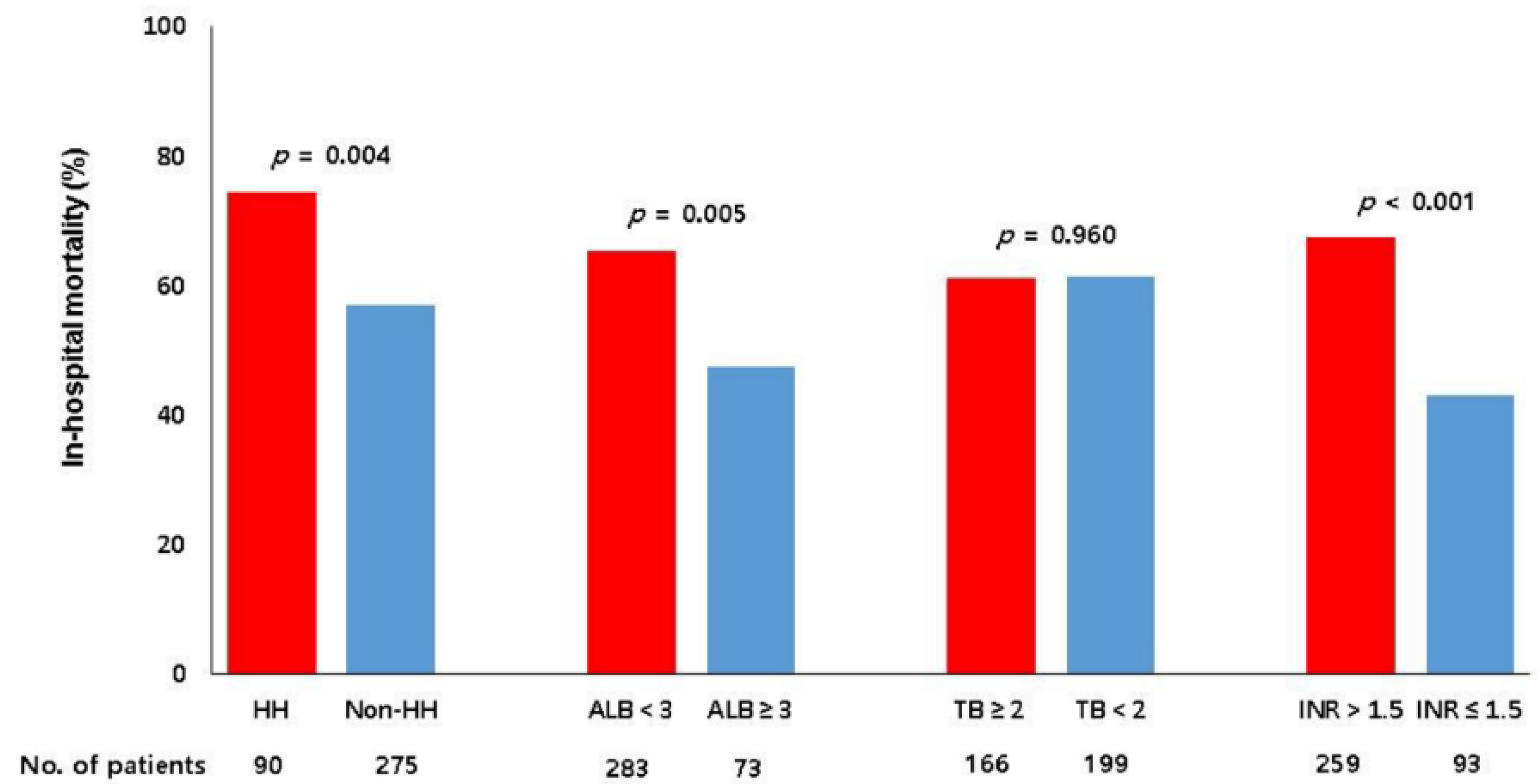
3.2. Hepatic Dysfunction and Mortality
3.3. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AST | aspartate aminotransferase; |
| ALT | alanine aminotransferase; |
| CPR | cardiopulmonary resuscitation; |
| CRRT | continuous renal replacement therapy; |
| ECMO | extracorporeal membrane oxygenation; |
| ECPR | extracorporeal cardiopulmonary resuscitation; |
| HH | hypoxic hepatitis; |
| INR | international normalized ratio. |
References
- Richardson, A.S.; Schmidt, M.; Bailey, M.; Pellegrino, V.A.; Rycus, P.T.; Pilcher, D.V. ECMO Cardio-Pulmonary Resuscitation (ECPR), trends in survival from an international multicentre cohort study over 12-years. Resuscitation 2017, 112, 34–40. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, F.H.; McDermott, K.M.; Kini, V.; Gutsche, J.T.; Wald, J.W.; Xie, D.; Szeto, W.Y.; Bermudez, C.A.; Atluri, P.; Acker, M.A.; et al. Trends in U.S. Extracorporeal Membrane Oxygenation Use and Outcomes: 2002–2012. Semin. Thorac. Cardiovasc. Surg. 2015, 27, 81–88. [Google Scholar] [CrossRef]
- Roedl, K.; Spiel, A.O.; Nurnberger, A.; Horvatits, T.; Drolz, A.; Hubner, P.; Warenits, A.M.; Sterz, F.; Herkner, H.; Fuhrmann, V. Hypoxic liver injury after in- and out-of-hospital cardiac arrest: Risk factors and neurological outcome. Resuscitation 2019, 137, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Champigneulle, B.; Geri, G.; Bougouin, W.; Dumas, F.; Arnaout, M.; Zafrani, L.; Pene, F.; Charpentier, J.; Mira, J.P.; Cariou, A. Hypoxic hepatitis after out-of-hospital cardiac arrest: Incidence, determinants and prognosis. Resuscitation 2016, 103, 60–65. [Google Scholar] [CrossRef]
- Oh, S.H.; Kim, H.J.; Park, K.N.; Kim, S.H.; Kim, Y.M.; Youn, C.S.; Lim, J.Y. Hypoxic hepatitis in survivors of out-of-hospital cardiac arrest. Am. J. Emerg. Med. 2015, 33, 1166–1170. [Google Scholar] [CrossRef]
- Pratt, D.S.; Kaplan, M.M. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N. Engl. J. Med. 2000, 342, 1266–1271. [Google Scholar] [CrossRef]
- Fuhrmann, V.; Jager, B.; Zubkova, A.; Drolz, A. Hypoxic hepatitis-epidemiology, pathophysiology and clinical management. Wien. Klin. Wochenschr. 2010, 122, 129–139. [Google Scholar] [CrossRef]
- Iesu, E.; Franchi, F.; Zama Cavicchi, F.; Pozzebon, S.; Fontana, V.; Mendoza, M.; Nobile, L.; Scolletta, S.; Vincent, J.L.; Creteur, J.; et al. Acute liver dysfunction after cardiac arrest. PLoS ONE 2018, 13, e0206655. [Google Scholar] [CrossRef]
- Park, S.B.; Yang, J.H.; Park, T.K.; Cho, Y.H.; Sung, K.; Chung, C.R.; Park, C.M.; Jeon, K.; Song, Y.B.; Hahn, J.Y.; et al. Developing a risk prediction model for survival to discharge in cardiac arrest patients who undergo extracorporeal membrane oxygenation. Int. J. Cardiol. 2014, 177, 1031–1035. [Google Scholar] [CrossRef]
- Ko, R.E.; Ryu, J.A.; Cho, Y.H.; Sung, K.; Jeon, K.; Suh, G.Y.; Park, T.K.; Lee, J.M.; Song, Y.B.; Hahn, J.Y.; et al. The differential neurologic prognosis of low-flow time according to the initial rhythm in patients who undergo extracorporeal cardiopulmonary resuscitation. Resuscitation 2020, 148, 121–127. [Google Scholar] [CrossRef]
- Moreno, R.P.; Metnitz, P.G.; Almeida, E.; Jordan, B.; Bauer, P.; Campos, R.A.; Iapichino, G.; Edbrooke, D.; Capuzzo, M.; Le Gall, J.R.; et al. SAPS 3--From evaluation of the patient to evaluation of the intensive care unit. Part 2: Development of a prognostic model for hospital mortality at ICU admission. Intensive Care Med. 2005, 31, 1345–1355. [Google Scholar] [PubMed]
- Child, C.G.; Turcotte, J.G. Surgery and portal hypertension. Major Probl. Clin. Surg. 1964, 1, 1–85. [Google Scholar]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure. J. Hepatol. 2017, 66, 1047–1081. [Google Scholar]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. Am. J. Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef]
- Cheung, A.; Flamm, S. Hepatobiliary Complications in Critically Ill Patients. Clin. Liver Dis. 2019, 23, 221–232. [Google Scholar]
- Dufour, D.R.; Lott, J.A.; Nolte, F.S.; Gretch, D.R.; Koff, R.S.; Seeff, L.B. Diagnosis and monitoring of hepatic injury. II. Recommendations for use of laboratory tests in screening, diagnosis, and monitoring. Clin. Chem. 2000, 46, 2050–2068. [Google Scholar]
- Giannini, E.G.; Testa, R.; Savarino, V. Liver enzyme alteration: A guide for clinicians. CMAJ 2005, 172, 367–379. [Google Scholar] [CrossRef]
- Dufour, D.R.; Lott, J.A.; Nolte, F.S.; Gretch, D.R.; Koff, R.S.; Seeff, L.B. Diagnosis and monitoring of hepatic injury. I. Performance characteristics of laboratory tests. Clin. Chem. 2000, 46, 2027–2049. [Google Scholar]
- Aboelsoud, M.M.; Javaid, A.I.; Al-Qadi, M.O.; Lewis, J.H. Hypoxic hepatitis-its biochemical profile, causes and risk factors of mortality in critically-ill patients: A cohort study of 565 patients. J. Crit. Care 2017, 41, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Fuhrmann, V.; Kneidinger, N.; Herkner, H.; Heinz, G.; Nikfardjam, M.; Bojic, A.; Schellongowski, P.; Angermayr, B.; Kitzberger, R.; Warszawska, J.; et al. Hypoxic hepatitis: Underlying conditions and risk factors for mortality in critically ill patients. Intensive Care Med. 2009, 35, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Ebert, E.C. Hypoxic liver injury. Mayo Clin. Proc. 2006, 81, 1232–1236. [Google Scholar] [CrossRef]
- Henrion, J. Hypoxic hepatitis. Liver Int. 2012, 32, 1039–1052. [Google Scholar] [CrossRef]
- Elinav, E.; Ben-Dov, I.Z.; Ackerman, E.; Kiderman, A.; Glikberg, F.; Shapira, Y.; Ackerman, Z. Correlation between serum alanine aminotransferase activity and age: An inverted U curve pattern. Am. J. Gastroenterol. 2005, 100, 2201–2204. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.H.; Bettencourt, R.; Barrett-Connor, E.; Loomba, R. Alanine aminotransferase decreases with age: The Rancho Bernardo Study. PLoS ONE 2010, 5, e14254. [Google Scholar] [CrossRef]
- Aaboud, M.; Aad, G.; Abbott, B.; Abdallah, J.; Abdinov, O.; Abeloos, B.; Abhayasinghe, D.K.; Abidi, S.H.; AbouZeid, O.S.; Abraham, N.L.; et al. Operation and performance of the ATLAS Tile Calorimeter in Run 1. Eur. Phys. J. C 2018, 78, 987. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| HH (n = 90) | Non-HH (n = 275) | p Value | |
|---|---|---|---|
| Patient demographics | |||
| Age (year) | 59.5 (47–71) | 62 (52–72) | 0.203 |
| Gender, male | 67 (74.4%) | 185 (67.3%) | 0.201 |
| Weight (kg) | 66 (57.2–75.8) | 65 (57.3–72.2) | 0.360 |
| Smoking | 31 (34.8%) | 95 (34.8%) | 0.995 |
| Comorbidities | |||
| Diabetes mellitus | 28 (31.1%) | 94 (34.2%) | 0.592 |
| Hypertension | 36 (40.0%) | 141 (51.3%) | 0.063 |
| Malignancy | 18 (20.0%) | 40 (14.5%) | 0.219 |
| Dyslipidemia | 11 (12.2%) | 35 (12.7%) | 0.900 |
| Chronic kidney disease a | 6 (6.7%) | 41 (14.9%) | 0.043 |
| Chronic liver disease | 6 (6.7%) | 20 (7.3%) | 0.846 |
| Previous coronary artery disease | 16 (17.8%) | 51 (18.5%) | 0.870 |
| Arrest due to ischemic heart disease | 38 (42.2%) | 142 (51.6%) | 0.121 |
| Initial shockable rhythm | 22 (24.4%) | 95 (34.5%) | 0.075 |
| Out-of-hospital cardiac arrest | 6 (6.7%) | 42 (15.3%) | 0.036 |
| ECPR details | |||
| CPR to ECMO pump-on time (min) | 35 (20–53) | 30 (20–47) | 0.373 |
| ECMO duration (day) | 3 (1–6) | 1 (0–3) | <0.001 |
| In-hospital management | |||
| Mechanical ventilator | 82 (91.1%) | 232 (84.4%) | 0.109 |
| CRRT | 54 (60.0%) | 83 (30.2%) | <0.001 |
| Vasopressor | 88 (97.8%) | 255 (92.7%) | 0.081 |
| * Adjusted OR (95% CI) | p Value | |
|---|---|---|
| Age (year) | 0.983 (0.966–0.999) | 0.046 |
| Gender, male | 1.503 (0.839–2.691) | 0.171 |
| Chronic liver disease | 0.868 (0.310–2.429) | 0.788 |
| Arrest due to ischemic heart disease | 0.955 (0.544–1.675) | 0.873 |
| Initial shockable rhythm | 0.605 (0.333–1.098) | 0.098 |
| Out-of-hospital cardiac arrest | 2.449 (0.950–6.313) | 0.064 |
| CPR to ECMO pump-on time ≥ 30 min | 1.608 (0.944–2.736) | 0.080 |
| CRRT | 3.518 (2.103–5.885) | <0.001 |
| * Adjusted OR (95% CI) | p Value | |
|---|---|---|
| Age (year) | 1.033 (1.015–1.051) | <0.001 |
| Arrest due to ischemic heart disease | 0.517 (0.301–0.889) | 0.017 |
| Initial shockable rhythm | 0.452 (0.261–0.782) | 0.005 |
| Out-of-hospital cardiac arrest | 3.114 (1.401–6.923) | 0.005 |
| CPR to ECMO pump-on time (min) | 1.036 (1.023–1.050) | <0.001 |
| CRRT | 1.880 (1.073–3.293) | 0.027 |
| HH | 1.955 (1.048–3.647) | 0.035 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.I.; Kang, M.G.; Ko, R.-E.; Park, T.K.; Chung, C.R.; Cho, Y.H.; Jeon, K.; Suh, G.Y.; Yang, J.H. The Impact of Hypoxic Hepatitis on Clinical Outcomes after Extracorporeal Cardiopulmonary Resuscitation. J. Clin. Med. 2020, 9, 2994. https://doi.org/10.3390/jcm9092994
Lee YI, Kang MG, Ko R-E, Park TK, Chung CR, Cho YH, Jeon K, Suh GY, Yang JH. The Impact of Hypoxic Hepatitis on Clinical Outcomes after Extracorporeal Cardiopulmonary Resuscitation. Journal of Clinical Medicine. 2020; 9(9):2994. https://doi.org/10.3390/jcm9092994
Chicago/Turabian StyleLee, Yun Im, Min Goo Kang, Ryoung-Eun Ko, Taek Kyu Park, Chi Ryang Chung, Yang Hyun Cho, Kyeongman Jeon, Gee Young Suh, and Jeong Hoon Yang. 2020. "The Impact of Hypoxic Hepatitis on Clinical Outcomes after Extracorporeal Cardiopulmonary Resuscitation" Journal of Clinical Medicine 9, no. 9: 2994. https://doi.org/10.3390/jcm9092994
APA StyleLee, Y. I., Kang, M. G., Ko, R.-E., Park, T. K., Chung, C. R., Cho, Y. H., Jeon, K., Suh, G. Y., & Yang, J. H. (2020). The Impact of Hypoxic Hepatitis on Clinical Outcomes after Extracorporeal Cardiopulmonary Resuscitation. Journal of Clinical Medicine, 9(9), 2994. https://doi.org/10.3390/jcm9092994