A Real-Life Survey of Venous Thromboembolic Events Occurring in Myeloma Patients Treated in Third Line with Second-Generation Novel Agents

 , ,
, ,
Abstract
:1. Introduction
2. Patients’ Selection and Methods
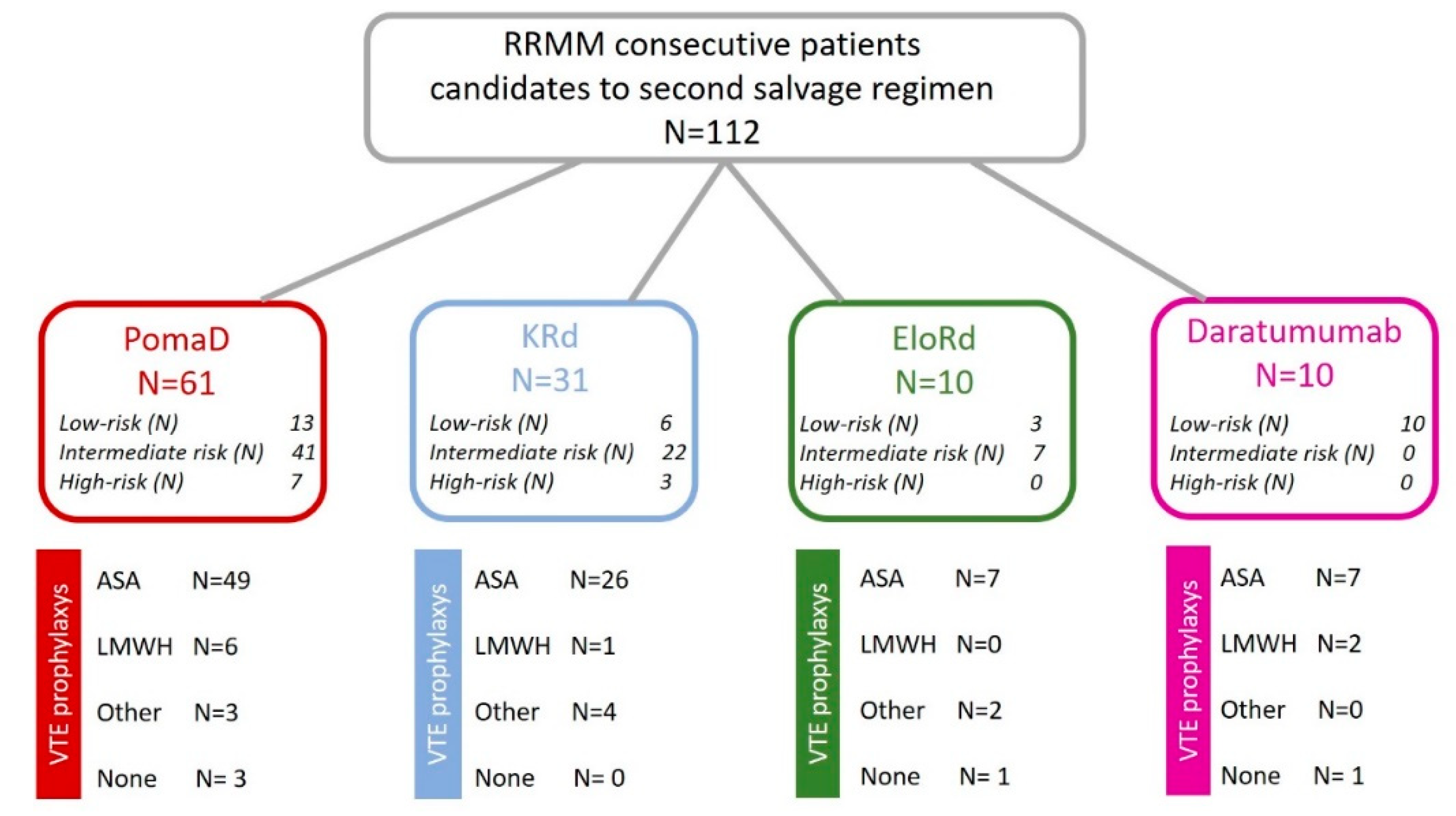
2.1. Patients’ Disposal
2.2. Patients’ Concomitant Treatments
2.3. VTE Thromboprophylaxis
2.4. Statistical Analysis
3. Results
3.1. Evaluation of VTE Risk Factors
3.2. VTE Thromboprophylaxis
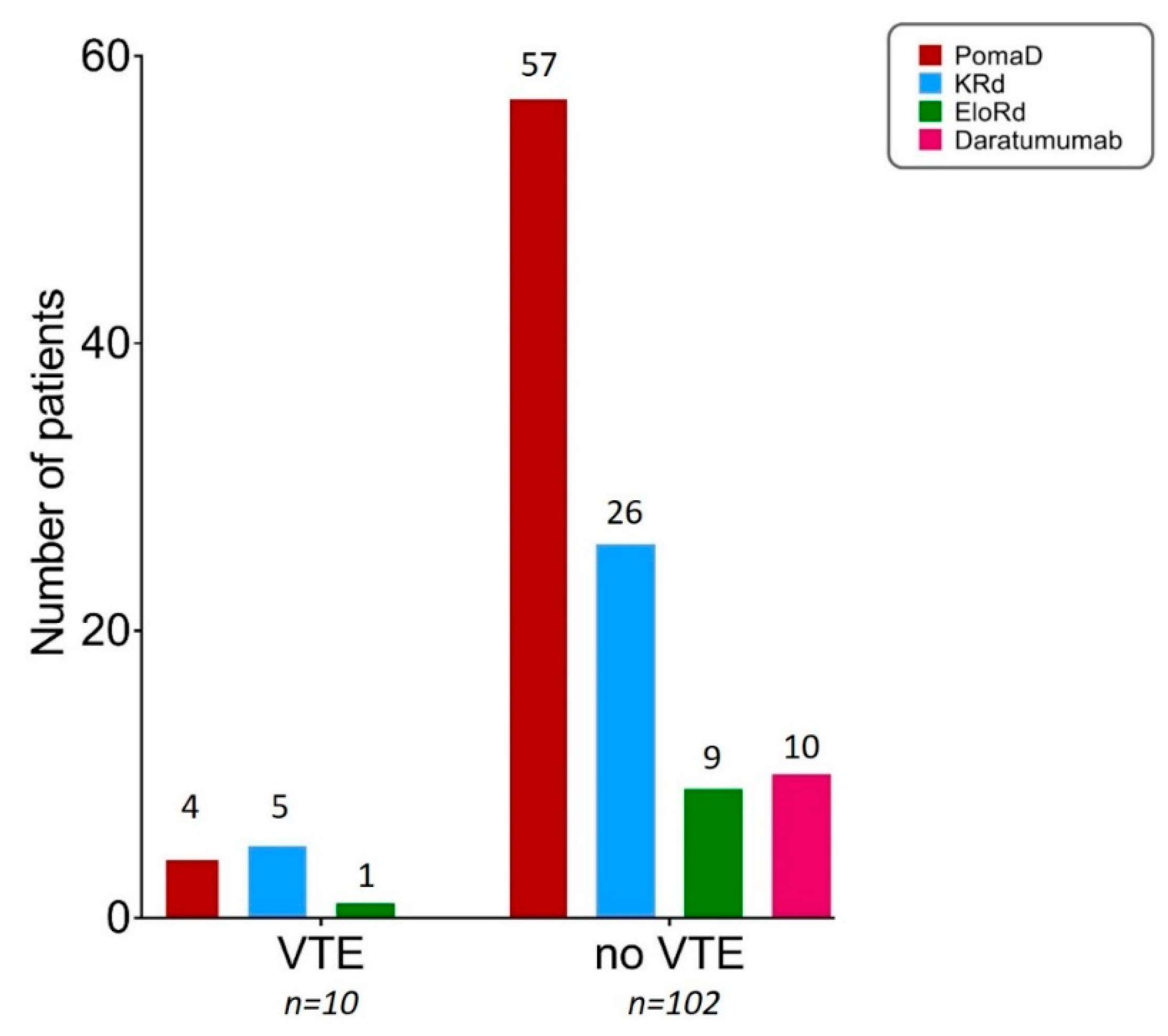
3.3. Description of Recorded VTEs
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Louzada, M.L.; Majeed, H.; Dao, V.; Wells, P.S. Risk of recurrent venous thromboembolism according to malignancy characteristics in patients with cancer-associated thrombosis: A systematic review of observational and intervention studies. Blood Coagul. Fibrinolysis 2011, 22, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Kyle, R.A.; Pfeiffer, R.M.; Katzmann, J.A.; Caporaso, N.E.; Hayes, R.B.; Dispenzieri, A.; Kumar, S.; Clark, R.J.; Baris, D.; et al. Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: A prospective study. Blood 2009, 113, 5412–5417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristinsson, S.Y.; Fears, T.R.; Gridley, G.; Turesson, I.; Mellqvist, U.H.; Bjorkholm, M.; Landgren, O. Deep vein thrombosis after monoclonal gammopathy of undetermined significance and multiple myeloma. Blood 2008, 112, 3582–3586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Za, T.; De Stefano, V.; Rossi, E.; Petrucci, M.T.; Andriani, A.; Annino, L.; Cimino, G.; Caravita, T.; Pisani, F.; Ciminello, A.; et al. Arterial and venous thrombosis in patients with monoclonal gammopathy of undetermined significance: Incidence and risk factors in a cohort of 1491 patients. Br. J. Haematol. 2013, 160, 673–679. [Google Scholar] [CrossRef]
- Fotiou, D.; Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Migkou, M.; Dimopoulos, M.A.; Terpos, E. Updates on thrombotic events associated with multiple myeloma. Expert Rev. Hematol. 2019, 12, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, F.; Parrinello, N.L.; Giallongo, C.; Cambria, D.; Camiolo, G.; Bellofiore, C.; Conticello, C.; Del Fabro, V.; Leotta, V.; Markovic, U.; et al. Plasticity of High-Density Neutrophils in Multiple Myeloma is Associated with Increased Autophagy via STAT3. Int. J. Mol. Sci. 2019, 20, 3548. [Google Scholar] [CrossRef] [Green Version]
- Fotiou, D.; Gerotziafas, G.; Kastritis, E.; Dimopoulos, M.A.; Terpos, E. A review of the venous thrombotic issues associated with multiple myeloma. Expert Rev. Hematol. 2016, 9, 695–706. [Google Scholar] [CrossRef]
- Fotiou, D.; Sergentanis, T.N.; Papageorgiou, L.; Stamatelopoulos, K.; Gavriatopoulou, M.; Kastritis, E.; Psaltopoulou, T.; Salta, S.; Van Dreden, P.; Sangare, R.; et al. Longer procoagulant phospholipid-dependent clotting time, lower endogenous thrombin potential and higher tissue factor pathway inhibitor concentrations are associated with increased VTE occurrence in patients with newly diagnosed multiple myeloma: Results of the prospective ROADMAP-MM-CAT study. Blood Cancer J. 2018, 8, 102. [Google Scholar] [CrossRef]
- Tiong, I.S.; Rodgers, S.E.; Lee, C.H.; McRae, S.J. Baseline and treatment-related changes in thrombin generation in patients with multiple myeloma. Leuk. Lymphoma 2017, 58, 941–949. [Google Scholar] [CrossRef]
- Crowley, M.P.; Kevane, B.; O’Shea, S.I.; Quinn, S.; Egan, K.; Gilligan, O.M.; Ni Ainle, F. Plasma Thrombin Generation and Sensitivity to Activated Protein C Among Patients With Myeloma and Monoclonal Gammopathy of Undetermined Significance. Clin. Appl. Thromb. Hemost. 2016, 22, 554–562. [Google Scholar] [CrossRef] [Green Version]
- Elice, F.; Fink, L.; Tricot, G.; Barlogie, B.; Zangari, M. Acquired resistance to activated protein C (aAPCR) in multiple myeloma is a transitory abnormality associated with an increased risk of venous thromboembolism. Br. J. Haematol. 2006, 134, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Li, H.; Li, D. Effect of serum monoclonal protein concentration on haemostasis in patients with multiple myeloma. Blood Coagul. Fibrinolysis 2015, 26, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.K.; Dispenzieri, A.; Lacy, M.Q.; Gertz, M.A.; Buadi, F.K.; Pandey, S.; Kapoor, P.; Dingli, D.; Hayman, S.R.; Leung, N.; et al. Continued improvement in survival in multiple myeloma: Changes in early mortality and outcomes in older patients. Leukemia 2014, 28, 1122–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romano, A.; Conticello, C.; Cavalli, M.; Vetro, C.; Di Raimondo, C.; Di Martina, V.; Schinocca, E.; La Fauci, A.; Parrinello, N.L.; Chiarenza, A.; et al. Salvage therapy of multiple myeloma: The new generation drugs. Biomed. Res. Int. 2014, 2014, 456037. [Google Scholar] [CrossRef]
- Romano, A.; Conticello, C.; Di Raimondo, F. Bortezomib for the treatment of previously untreated multiple myeloma. Immunotherapy 2013, 5, 327–352. [Google Scholar] [CrossRef]
- Conticello, C.; Giuffrida, R.; Adamo, L.; Anastasi, G.; Martinetti, D.; Salomone, E.; Colarossi, C.; Amato, G.; Gorgone, A.; Romano, A.; et al. NF-κB localization in multiple myeloma plasma cells and mesenchymal cells. Leuk. Res. 2011, 35, 52–60. [Google Scholar] [CrossRef]
- Srkalovic, G.; Cameron, M.G.; Rybicki, L.; Deitcher, S.R.; Kattke-Marchant, K.; Hussein, M.A. Monoclonal gammopathy of undetermined significance and multiple myeloma are associated with an increased incidence of venothromboembolic disease. Cancer 2004, 101, 558–566. [Google Scholar] [CrossRef]
- Li, A.; Wu, Q.; Warnick, G.; Li, S.; Libby, E.N.; Garcia, D.A.; Lyman, G.H. The incidence of thromboembolism for lenalidomide versus thalidomide in older patients with newly diagnosed multiple myeloma. Ann. Hematol. 2020, 99, 121–126. [Google Scholar] [CrossRef]
- Palmaro, A.; Rouge-Bugat, M.E.; Gauthier, M.; Despas, F.; Moulis, G.; Lapeyre-Mestre, M. Real-life practices for preventing venous thromboembolism in multiple myeloma patients: A cohort study from the French health insurance database. Pharmacoepidemiol. Drug Saf. 2017, 26, 578–586. [Google Scholar] [CrossRef]
- Palumbo, A.; Palladino, C. Venous and arterial thrombotic risks with thalidomide: Evidence and practical guidance. Ther. Adv. Drug Saf. 2012, 3, 255–266. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Gajra, A. Thromboembolism with immunomodulatory agents in the treatment of multiple myeloma. Cardiovasc. Hematol. Agents Med. Chem. 2011, 9, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Niesvizky, R.; Martinez-Banos, D.; Jalbrzikowski, J.; Christos, P.; Furst, J.; De Sancho, M.; Mark, T.; Pearse, R.; Mazumdar, M.; Zafar, F.; et al. Prophylactic low-dose aspirin is effective antithrombotic therapy for combination treatments of thalidomide or lenalidomide in myeloma. Leuk. Lymphoma 2007, 48, 2330–2337. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, R.; Bin Riaz, I.; Malik, S.U.; Marneni, N.; Mejia Garcia, A.; Anwer, F.; Khorana, A.A.; Rajkumar, S.V.; Kumar, S.; Murad, M.H.; et al. Venous thromboembolism risk with contemporary lenalidomide-based regimens despite thromboprophylaxis in multiple myeloma: A systematic review and meta-analysis. Cancer 2020, 126, 1640–1650. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Lee, J.J.; Kim, K.; Min, C.K.; Lee, J.O.; Suh, C.; Kim, J.S.; Lee, Y.J.; Yoon, S.S.; Jo, J.C.; et al. Venous thromboembolism in relapsed or refractory multiple myeloma patients treated with lenalidomide plus dexamethasone. Int. J. Hematol. 2019, 109, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.M.; Beck, B.; Sterud, S.; Lockhorst, R.; Ngorsuraches, S. Evaluating the use of appropriate anticoagulation with lenalidomide and pomalidomide in patients with multiple myeloma. J. Oncol. Pharm. Pract. 2019, 25, 806–812. [Google Scholar] [CrossRef]
- Maharaj, S.; Chang, S.; Seegobin, K.; Serrano-Santiago, I.; Zuberi, L. Increased risk of arterial thromboembolic events with combination lenalidomide/dexamethasone therapy for multiple myeloma. Expert Rev. Anticancer Ther. 2017, 17, 585–591. [Google Scholar] [CrossRef]
- Al-Ani, F.; Bermejo, J.M.; Mateos, M.V.; Louzada, M. Thromboprophylaxis in multiple myeloma patients treated with lenalidomide—A systematic review. Thromb. Res. 2016, 141, 84–90. [Google Scholar] [CrossRef]
- Isoda, A.; Sato, N.; Miyazawa, Y.; Matsumoto, Y.; Koumoto, M.; Ookawa, M.; Sawamura, M.; Matsumoto, M. Silent venous thromboembolism in multiple myeloma patients treated with lenalidomide. Int. J. Hematol. 2015, 102, 271–277. [Google Scholar] [CrossRef]
- Larocca, A.; Cavallo, F.; Bringhen, S.; Di Raimondo, F.; Falanga, A.; Evangelista, A.; Cavalli, M.; Stanevsky, A.; Corradini, P.; Pezzatti, S.; et al. Aspirin or enoxaparin thromboprophylaxis for patients with newly diagnosed multiple myeloma treated with lenalidomide. Blood 2012, 119, 933–939, quiz 1093. [Google Scholar] [CrossRef] [Green Version]
- Zangari, M.; Fink, L.; Zhan, F.; Tricot, G. Low venous thromboembolic risk with bortezomib in multiple myeloma and potential protective effect with thalidomide/lenalidomide-based therapy: Review of data from phase 3 trials and studies of novel combination regimens. Clin. Lymphoma Myeloma Leuk. 2011, 11, 228–236. [Google Scholar] [CrossRef]
- Zonder, J.A.; Crowley, J.; Hussein, M.A.; Bolejack, V.; Moore, D.F., Sr.; Whittenberger, B.F.; Abidi, M.H.; Durie, B.G.; Barlogie, B. Lenalidomide and high-dose dexamethasone compared with dexamethasone as initial therapy for multiple myeloma: A randomized Southwest Oncology Group trial (S0232). Blood 2010, 116, 5838–5841. [Google Scholar] [CrossRef] [PubMed]
- Klein, U.; Kosely, F.; Hillengass, J.; Hundemer, M.; Schmitt, S.; Neben, K.; Moehler, T.; Hegenbart, U.; Ho, A.D.; Goldschmidt, H. Effective prophylaxis of thromboembolic complications with low molecular weight heparin in relapsed multiple myeloma patients treated with lenalidomide and dexamethasone. Ann. Hematol. 2009, 88, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, S.P.; Rajkumar, S.V.; Lacy, M.; Falco, P.; Palumbo, A. Thromboembolic events with lenalidomide-based therapy for multiple myeloma. Cancer 2008, 112, 1522–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palumbo, A.; Rajkumar, S.V.; Dimopoulos, M.A.; Richardson, P.G.; San Miguel, J.; Barlogie, B.; Harousseau, J.; Zonder, J.A.; Cavo, M.; Zangari, M.; et al. Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia 2008, 22, 414–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Needleman, L.; Cronan, J.J.; Lilly, M.P.; Merli, G.J.; Adhikari, S.; Hertzberg, B.S.; DeJong, M.R.; Streiff, M.B.; Meissner, M.H. Ultrasound for Lower Extremity Deep Venous Thrombosis: Multidisciplinary Recommendations from the Society of Radiologists in Ultrasound Consensus Conference. Circulation 2018, 137, 1505–1515. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Cavo, M.; Bringhen, S.; Zamagni, E.; Romano, A.; Patriarca, F.; Rossi, D.; Gentilini, F.; Crippa, C.; Galli, M.; et al. Aspirin, warfarin, or enoxaparin thromboprophylaxis in patients with multiple myeloma treated with thalidomide: A phase III, open-label, randomized trial. J. Clin. Oncol. 2011, 29, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Lyman, G.H. Risk factors for chemotherapy-associated venous thromboembolism in a prospective observational study. Cancer 2005, 104, 2822–2829. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Kleber, M.; Engelhardt, M.; Zweegman, S.; Gay, F.; Kastritis, E.; van de Donk, N.W.; Bruno, B.; Sezer, O.; Broijl, A.; et al. European Myeloma Network guidelines for the management of multiple myeloma-related complications. Haematologica 2015, 100, 1254–1266. [Google Scholar] [CrossRef] [Green Version]
- Moreau, P.; San Miguel, J.; Sonneveld, P.; Mateos, M.V.; Zamagni, E.; Avet-Loiseau, H.; Hajek, R.; Dimopoulos, M.A.; Ludwig, H.; Einsele, H.; et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv52–iv61. [Google Scholar] [CrossRef]
- Cornell, R.F.; Goldhaber, S.Z.; Engelhardt, B.G.; Moslehi, J.; Jagasia, M.; Patton, D.; Harrell, S.; Hall, R.; Wyatt, H.; Piazza, G. Apixaban for Primary Prevention of Venous Thromboembolism in Patients With Multiple Myeloma Receiving Immunomodulatory Therapy. Front. Oncol. 2019, 9, 45. [Google Scholar] [CrossRef]
- Parisi, M.S.; Leotta, S.; Romano, A.; Del Fabro, V.; Martino, E.A.; Calafiore, V.; Giubbolini, R.; Markovic, U.; Leotta, V.; Di Giorgio, M.A.; et al. Clinical Benefit of Long-Term Disease Control with Pomalidomide and Dexamethasone in Relapsed/Refractory Multiple Myeloma Patients. J. Clin. Med. 2019, 8, 1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumura-Kimoto, Y.; Kuroda, J.; Kaneko, H.; Kamitsuji, Y.; Fuchida, S.I.; Nakaya, A.; Shibayama, H.; Uoshima, N.; Yokota, I.; Uchiyama, H.; et al. Pomalidomide with or without dexamethasone for relapsed/refractory multiple myeloma in Japan: A retrospective analysis by the Kansai Myeloma Forum. Int. J. Hematol. 2018, 107, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Gueneau, P.; Chretien, M.L.; Cransac-Miet, A.; Aho, L.S.; Lafon, I.; Favennec, C.; Guy, J.; Caillot, D.; Boulin, M. Efficacy, safety, and cost of pomalidomide in relapsed and refractory multiple myeloma. Eur. J. Haematol. 2018, 100, 518–525. [Google Scholar] [CrossRef]
- Man, L.; Morris, A.; Brown, J.; Palkimas, S.; Davidson, K. Use of direct oral anticoagulants in patients on immunomodulatory agents. J. Thromb. Thrombolysis 2017, 44, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.K.; Rajkumar, S.V.; Dimopoulos, M.A.; Masszi, T.; Spicka, I.; Oriol, A.; Hajek, R.; Rosinol, L.; Siegel, D.S.; Mihaylov, G.G.; et al. Carfilzomib, lenalidomide, and dexamethasone for relapsed multiple myeloma. N. Engl. J. Med. 2015, 372, 142–152. [Google Scholar] [CrossRef]
- Conticello, C.; Romano, A.; Del Fabro, V.; Martino, E.A.; Calafiore, V.; Sapienza, G.; Leotta, V.; Parisi, M.S.; Markovic, U.; Garibaldi, B.; et al. Feasibility, Tolerability and Efficacy of Carfilzomib in Combination with Lenalidomide and Dexamethasone in Relapsed Refractory Myeloma Patients: A Retrospective Real-Life Survey of the Sicilian Myeloma Network. J. Clin. Med. 2019, 8, 877. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Garcia, D.; Cornell, R.F.; Gailani, D.; Laubach, J.; Maglio, M.E.; Richardson, P.G.; Moslehi, J. Cardiovascular and Thrombotic Complications of Novel Multiple Myeloma Therapies: A Review. JAMA Oncol. 2017, 3, 980–988. [Google Scholar] [CrossRef]
- Fotiou, D.; Gavriatopoulou, M.; Terpos, E. Multiple Myeloma and Thrombosis: Prophylaxis and Risk Prediction Tools. Cancers 2020, 12, 191. [Google Scholar] [CrossRef] [Green Version]
- Sayar, Z.; Czuprynska, J.; Patel, J.P.; Benjamin, R.; Roberts, L.N.; Patel, R.K.; Cornelius, V.; Arya, R. What are the difficulties in conducting randomised controlled trials of thromboprophylaxis in myeloma patients and how can we address these? Lessons from apixaban versus LMWH or aspirin as thromboprophylaxis in newly diagnosed multiple myeloma (TiMM) feasibility clinical trial. J. Thromb. Thrombolysis 2019, 48, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Bradbury, C.A.; Craig, Z.; Cook, G.; Pawlyn, C.; Cairns, D.A.; Hockaday, A.; Paterson, A.; Jenner, M.W.; Jones, J.R.; Drayson, M.T.; et al. Thrombosis in Patients with Myeloma Treated in the Myeloma IX and Myeloma XI Phase III Randomized Controlled Trials. Blood 2020, 136, 1091–1104. [Google Scholar] [CrossRef]
- Sanfilippo, K.M.; Luo, S.; Wang, T.F.; Fiala, M.; Schoen, M.; Wildes, T.M.; Mikhael, J.; Kuderer, N.M.; Calverley, D.C.; Keller, J.; et al. Predicting venous thromboembolism in multiple myeloma: Development and validation of the IMPEDE VTE score. Am. J. Hematol. 2019, 94, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Wu, Q.; Luo, S.; Warnick, G.S.; Zakai, N.A.; Libby, E.N.; Gage, B.F.; Garcia, D.A.; Lyman, G.H.; Sanfilippo, K.M. Derivation and Validation of a Risk Assessment Model for Immunomodulatory Drug-Associated Thrombosis Among Patients with Multiple Myeloma. J. Natl. Compr. Cancer Netw. 2019, 17, 840–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pegourie, B.; Karlin, L.; Benboubker, L.; Orsini-Piocelle, F.; Tiab, M.; Auger-Quittet, S.; Rodon, P.; Royer, B.; Leleu, X.; Bareau, B.; et al. Apixaban for the prevention of thromboembolism in immunomodulatory-treated myeloma patients: Myelaxat, a phase 2 pilot study. Am. J. Hematol. 2019, 94, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.M.; Moneta, G.L. Reporting standards in venous disease: An update. International Consensus Committee on Chronic Venous Disease. J. Vasc. Surg. 1995, 21, 635–645. [Google Scholar] [CrossRef]
- Anaissie, E.J.; Coleman, E.A.; Goodwin, J.A.; Kennedy, R.L.; Lockhart, K.D.; Stewart, C.B.; Coon, S.K.; Bailey, C.; Barlogie, B. Prophylactic recombinant erythropoietin therapy and thalidomide are predictors of venous thromboembolism in patients with multiple myeloma: Limited effectiveness of thromboprophylaxis. Cancer 2012, 118, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.A.; Jakubowiak, A.J.; McCarthy, P.L.; Orlowski, R.Z.; Attal, M.; Bladé, J.; Goldschmidt, H.; Weisel, K.C.; Ramasamy, K.; Zweegman, S.; et al. Developments in continuous therapy and maintenance treatment approaches for patients with newly diagnosed multiple myeloma. Blood Cancer J. 2020, 10, 17. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Poma D | KRd | Daratumumab | EloRd | |
|---|---|---|---|---|
| N = 61 (100%) | N = 31 (100%) | N = 10 (100%) | N = 10 (100%) | |
| Median age (range) | 71 (45–87) | 66 (50–78) | 66 (52–74) | 61 (48–72) |
| Males, n (%) | 39 (64) | 22(71) | 6(60) | 5 (50) |
| ECOG performance status, n (%) | ||||
| 0–2 | 30 (49) | 26 (84) | 9 (90) | 10 (100) |
| >2 | 31 (51) | 5 (16) | 1 (10) | 0 (0) |
| International Staging System stage, n (%) | ||||
| I | 5 (9) | 10 (32) | 8 (80) | 8 (80) |
| II | 22 (36) | 5 (16) | 2 (20) | 1 (10) |
| III | 34 (55) | 16 (52) | 0 (0) | 1 (10) |
| Cytogenetics risk (FISH) available at baseline | 39 (64) | 23 (74) | 9 (90) | 8 (80) |
| High-risk | 13 (21) | 11 (35) | 3 (30) | 3 (30) |
| Standard-risk | 26 (43) | 12 (39) | 6 (60) | 5 (50) |
| Glomerular filtration rate (GFR, mL/hour) | ||||
| >60 mL/hour | 54 (89) | 13 (43) | 2 (20) | 6 (60) |
| 30–60 mL/hour | 5 (10) | 5 (17) | 6 (60) | 4 (40) |
| <30 mL/hour | 2 (1) | 3 (10) | 2 (20) | 0 (0) |
| Median haemoglobin (range), g/dL | 9.3 (7.1–12.2) | 9.5 (7.8–14.6) | 10.1 (8.1–14.6) | 10.2 (7.2–11.6) |
| Median platelet count (range), *103/mmc | 145 (30–316) | 130 (20–560) | 136 (25–198) | 156 (70–215) |
| Median monoclonal component (range), g/dL | 2.3 (0.3–3.2) | 1.6 (0.2–2.1) | 0.9 (0.1–3.1) | 0.5 (0.1–2.0) |
| Previous treatments | ||||
| Autologous transplantation | 12 (20) | 15 (48) | 5 (50) | 3 (30) |
| Allogeneic transplantation | 4 (6) | 0 (0) | 2 (20) | 0 (0) |
| Continuous lenalidomide | 61 (100) | 7 (23) | 2 (20) | 0 (0) |
| Disease status | ||||
| Refractory disease | 36 (59) | 17 (55) | 5 (50) | 8 (80) |
| Aggressive relapse | 8 (13) | 5 (16) | 0 (0) | 2 (20) |
| Biochemical relapse | 17 (28) | 9 (29) | 5 (50) | 0 (0) |
| Risk Factors | PomaD N = 61 (100%) | KRd N = 31 (100%) | EloRd N = 10 (100%) | Daratumumab N = 10 (100%) | Total N = 112 (100%) |
|---|---|---|---|---|---|
| Individual | 55 (90) | 31 (100) | 6 (60) | 10 (100) | 102 (91) |
| Obesity (BMI > 30 kg/m2) | 22 (35) | 13 (42) | 1 (10) | 1(10) | 37(33) |
| Previous VTE | 1 (2) | 2 (6) | 0 (0) | 0 (0) | 3 (3) |
| CVC or PM | 1 (2) | 4 (13) | 0 (0) | 1 (10) | 6 (7) |
| Associated comorbidities | 43 (70) | 30 (97) | 4 (40) | 7 (70) | 84 (75) |
| Surgical procedures | 7 (11) | 7 (23) | 1 (10) | 3 (30) | 18 (16) |
| Erythropoietin | 50 (82) | 19 (61) | 6 (60) | 6(60) | 75 (67) |
| MM-related | 47 (78) | 17 (55) | 6 (60) | 6 (60) | 78 (70) |
| Hyperviscosity | 2 (3) | 3(10) | 0 (0) | 0 (0) | 5 (4) |
| Active uncontrolled disease | 45 (74) | 17 (55) | 6 (60) | 6 (60) | 74 (66) |
| Treatment Group | Number of Subjects | Number of Individual and MM-Related Risk Factors | ||
|---|---|---|---|---|
| ≤1 | 2 | 3 or More | ||
| PomaD | 61 (100) | 14 (23) | 19 (31) | 28 (46) |
| No VTE | 57 (93) | 14 (23) | 18 (29) | 25 (41) |
| VTE | 4 * (7) | 0 (0) | 1 (2) | 3 (5) |
| KRd | 31 (100) | 5 (16) | 8 (26) | 18 (58) |
| No VTE | 26 (84) | 4 (13) | 8 (26) | 14 (45) |
| VTE | 5 ** (16) | 1 (3) | 0 (0) | 4 (13) |
| EloRd | 10 (100) | 4 (40) | 4 (40) | 2 (20) |
| No VTE | 9 (90) | 4 (40) | 3 (30) | 2 (20) |
| VTE | 1 *** (10) | 0 (0) | 1 (10) | 0 (0) |
| Daratumumab | ||||
| No VTE | 10 (100) | 4 (40) | 5 (50) | 1 (10) |
| VTE | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calafiore, V.; Giamporcaro, S.; Conticello, C.; Romano, A.; Parisi, M.; Giuffrida, G.; Tibullo, D.; Di Raimondo, F.; Signorelli, S.S. A Real-Life Survey of Venous Thromboembolic Events Occurring in Myeloma Patients Treated in Third Line with Second-Generation Novel Agents. J. Clin. Med. 2020, 9, 2876. https://doi.org/10.3390/jcm9092876
Calafiore V, Giamporcaro S, Conticello C, Romano A, Parisi M, Giuffrida G, Tibullo D, Di Raimondo F, Signorelli SS. A Real-Life Survey of Venous Thromboembolic Events Occurring in Myeloma Patients Treated in Third Line with Second-Generation Novel Agents. Journal of Clinical Medicine. 2020; 9(9):2876. https://doi.org/10.3390/jcm9092876
Chicago/Turabian StyleCalafiore, Valeria, Silvia Giamporcaro, Concetta Conticello, Alessandra Romano, Marina Parisi, Gaetano Giuffrida, Daniele Tibullo, Francesco Di Raimondo, and Salvatore Santo Signorelli. 2020. "A Real-Life Survey of Venous Thromboembolic Events Occurring in Myeloma Patients Treated in Third Line with Second-Generation Novel Agents" Journal of Clinical Medicine 9, no. 9: 2876. https://doi.org/10.3390/jcm9092876