Perceptions, Attitudes, and Barriers to Obesity Management in Spain: Results from the Spanish Cohort of the International ACTION-IO Observation Study


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Statistical Analysis
3. Results
3.1. Participants
3.2. Perception of Obesity as a Chronic Disease
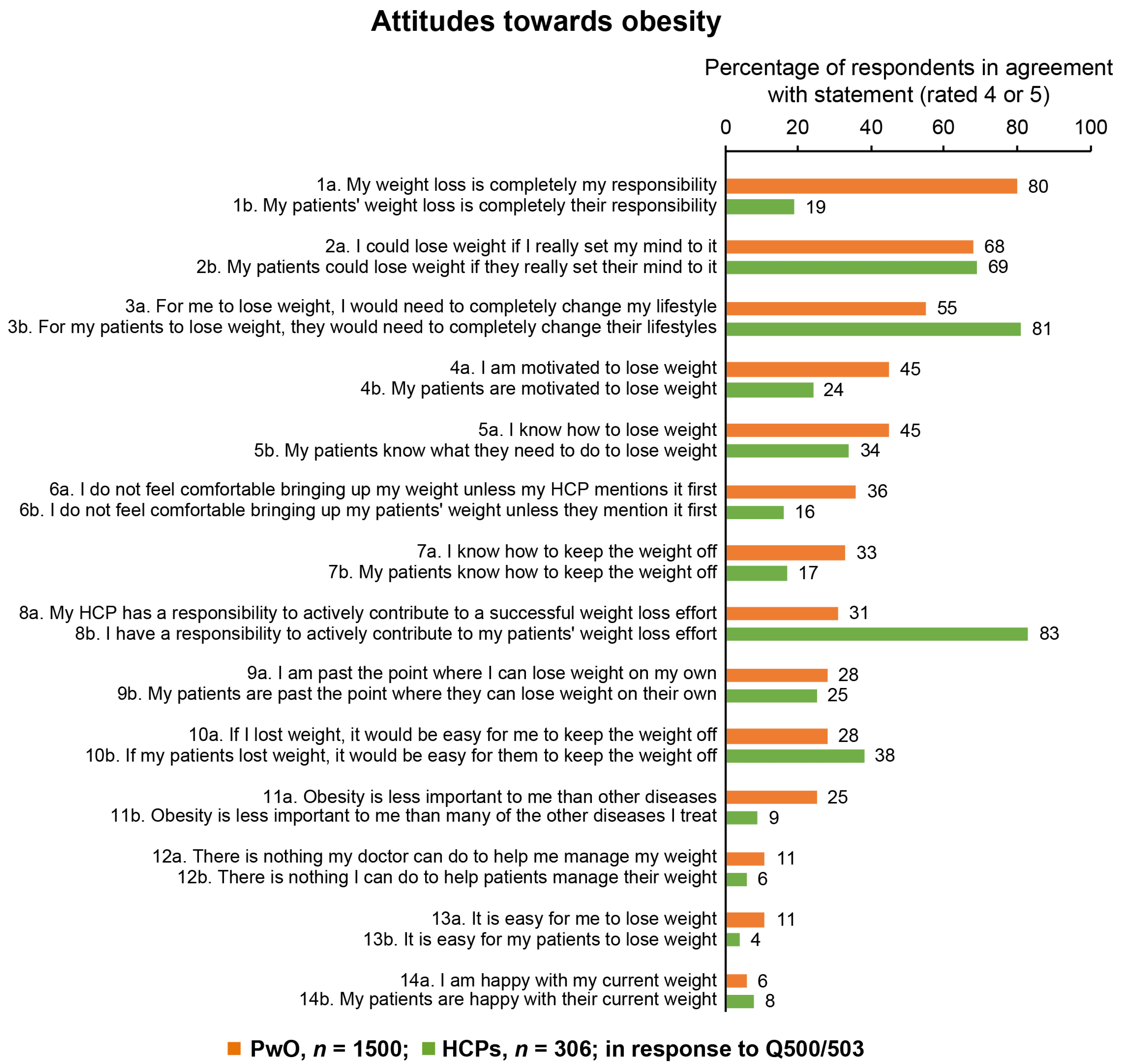
3.3. Responsibility and Motivation for Treating Obesity
3.4. Previous Weight Loss Attempts and Outcomes
3.5. Conversations Between PwO and HCPs
3.6. Treatment Objectives
3.7. Diagnosis of Obesity and Scheduling of Follow-Up Appointments
3.8. Perception of Efficacy and Indication of Treatments for Obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Ladeiras-Lopes, R.; Sampaio, F.; Bettencourt, N.; Fontes-Carvalho, R.; Ferreira, N.D.; Leite-Moreira, A.F.; Gama, V. The ratio between visceral and subcutaneous abdominal fat assessed by computed tomography is an independent predictor of mortality and cardiac events. Rev. Esp. Cardiol. 2017, 70, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Biener, A.I.; Decker, S.L. Agency for Healthcare Research and Quality. Medical care use and expenditures associated with adult obesity in the United States. JAMA 2018, 319, 218. [Google Scholar] [CrossRef] [Green Version]
- Kassir, R. Risk of COVID-19 for patients with obesity. Obes. Rev. 2020, 21, e13034. [Google Scholar] [CrossRef] [Green Version]
- Garg, S.; Kim, L.; Whitaker, M.; O’Halloran, A.; Cummings, C.; Holstein, R.; Prill, M.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019—COVID-NET, 14 states, March 1–30, 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 458–464. [Google Scholar] [CrossRef]
- Gutiérrez-Fisac, J.L.; Guallar-Castillón, P.; León-Muñoz, L.M.; Graciani, A.; Banegas, J.R.; Rodríguez-Artalejo, F. Prevalence of general and abdominal obesity in the adult population of Spain, 2008-2010: The ENRICA study. Obes. Rev. 2012, 13, 388–392. [Google Scholar] [CrossRef]
- Organization for Economic Co-Operation and Development (OECD) Obesity Update 2017. Available online: https://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf (accessed on 7 November 2019).
- Hernáez, Á.; Zomeño, M.D.; Dégano, I.R.; Fernández, S.P.; Goday, A.; Vila, J.; Civeira, F.; Moure, R.; Marrugat, J. Excess weight in Spain: Current situation, projections for 2030, and estimated direct extra cost for the Spanish health system. Rev. Esp. Cardiol. 2019, 72, 916–924. [Google Scholar] [CrossRef]
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H. World Obesity Federation. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Ralston, J.; Brinsden, H.; Buse, K.; Candeias, V.; Caterson, I.; Hassell, T.; Kumanyika, S.; Nece, P.; Nishtar, S.; Patton, I.; et al. Time for a new obesity narrative. Lancet 2018, 392, 1384–1386. [Google Scholar] [CrossRef]
- Ghanemi, A.; Yoshioka, M.; St-Amand, J. Broken energy homeostasis and obesity pathogenesis: The surrounding concepts. J. Clin. Med. 2018, 7, 453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129 (Suppl. S2), S102–S138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity. Endocr. Pract. 2016, 22 (Suppl. S3), 1–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schutz, D.D.; Busetto, L.; Dicker, D.; Farpour-Lambert, N.; Pryke, R.; Toplak, H.; Widmer, D.; Yumuk, V.; Schutz, Y. European practical and patient-centred guidelines for adult obesity management in primary care. Obes. Facts 2019, 12, 40–66. [Google Scholar] [CrossRef]
- Glauser, T.A.; Roepke, N.; Stevenin, B.; Dubois, A.M.; Ahn, S.M. Physician knowledge about and perceptions of obesity management. Obes. Res. Clin. Pract. 2015, 9, 573–583. [Google Scholar] [CrossRef]
- Turner, M.; Jannah, N.; Kahan, S.; Gallagher, C.; Dietz, W. Current knowledge of obesity treatment guidelines by health care professionals. Obesity 2018, 26, 665–671. [Google Scholar] [CrossRef]
- Puhl, R.M.; Heuer, C.A. Obesity stigma: Important considerations for public health. Am. J. Public Health 2010, 100, 1019–1028. [Google Scholar] [CrossRef]
- Rubino, F.; Puhl, R.M.; Cummings, D.E.; Eckel, R.H.; Ryan, D.H.; Mechanick, J.I.; Nadglowski, J.; Salas, X.R.; Schauer, P.R.; Twenefour, D.; et al. Joint international consensus statement for ending stigma of obesity. Nat. Med. 2020, 26, 485–497. [Google Scholar] [CrossRef] [Green Version]
- Apovian, C.M.; Aronne, L.; Rubino, D.; Still, C.; Wyatt, H.; Burns, C.; Kim, D.; Dunayevich, E.; Cor-II Study Group. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity 2013, 21, 935–943. [Google Scholar] [CrossRef] [Green Version]
- Magallares, A.; Bolaños-Rios, P.; Ruiz-Prieto, I.; de Benito Valle, P.; Irles, J.A.; Jáuregui-Lobera, I. The mediational effect of weight self-stigma in the relationship between blatant and subtle discrimination and depression and anxiety. Span. J. Psychol. 2017, 20, E4. [Google Scholar] [CrossRef]
- Kaplan, L.M.; Golden, A.; Jinnett, K.; Kolotkin, R.L.; Kyle, T.K.; Look, M.; Nadglowski, J.; O’Neil, P.M.; Parry, T.; Tomaszewski, K.J.; et al. Perceptions of barriers to effective obesity care: Results from the national ACTION study. Obesity 2018, 26, 61–69. [Google Scholar] [CrossRef]
- Sharma, A.M.; Bélanger, A.; Carson, V.; Krah, J.; Langlois, M.; Lawlor, D.; Lepage, S.; Liu, A.; Macklin, D.A.; Mackay, N.; et al. Perceptions of barriers to effective obesity management in Canada: Results from the ACTION study. Clin. Obes. 2019, 9, e12329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caterson, I.D.; Alfadda, A.; Auerbach, P.; Coutinho, W.; Cuevas, A.; Dicker, D.; Hughes, C.; Iwabu, M.; Kang, J.; Nawar, R.; et al. Gaps to bridge: Misalignment between perception, reality and actions in obesity. Diabetes Obes. Metab. 2019, 21, 1914–1924. [Google Scholar] [CrossRef] [PubMed]
- International Society for Pharmacoepidemiology (ISPE). Guidelines for Good Pharmacoepidemiology Practices (GPP). Available online: https://www.pharmacoepi.org/resources/policies/guidelines-08027/ (accessed on 15 January 2020).
- World Medical Association (WMA). World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Lecube, A.; Monereo, S.; Rubio, M.A.; Martínez-De-Icaya, P.; Marti, A.; Salvador, J.; Masmiquel, L.; Goday, A.; Bellido, D.; Lurbe, E.; et al. Prevention, diagnosis, and treatment of obesity. 2016 position statement of the Spanish Society for the Study of Obesity. Endocrinol. Diabetes Nutr. 2017, 64, 15–22. [Google Scholar] [CrossRef]
- Mawardi, G.; Kirkland, E.B.; Zhang, J.; Blankinship, D.; Heincelman, M.E.; Schreiner, A.D.; Moran, W.P.; Schumann, S. Patient perception of obesity versus physician documentation of obesity: A quality improvement study. Clin. Obes. 2019, 9, e12303. [Google Scholar] [CrossRef]
- Yaemsiri, S.; Slining, M.M.; Agarwal, S.K. Perceived weight status, overweight diagnosis, and weight control among US adults: The NHANES 2003–2008 study. Int. J. Obes. 2011, 35, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, N.E.; Collins, K.J.; Himmelfarb, C.R.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- American Diabetes Association (ADA). Standards of Medical Care in Diabetes-2019 Abridged for Primary Care Providers. Clin. Diabetes 2019, 37, 11–34. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Somers, V.K.; Clark, M.M.; Vickers, K.; Hensrud, D.D.; Korenfeld, Y.; Lopez-Jimenez, F. Physician diagnosis of overweight status predicts attempted and successful weight loss in patients with cardiovascular disease and central obesity. Am. Heart J. 2010, 160, 934–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, A.M.; Keppel, G.A.; Andrilla, H.A. Primary care patients' willingness to participate in comprehensive weight loss programs: From the WWAMI Region Practice and Research Network. J. Am. Board Fam. Med. 2016, 29, 572–580. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Servicios Sociales e Igualdad; Agencia Española de Consumo, Seguridad Alimentaria y Nutrición. Estudio Aladino 2015: Estudio de Vigilancia del Crecimiento, Alimentación, Actividad Física, Desarrollo Infantil y Obesidad en España 2015. Available online: http://www.aecosan.msssi.gob.es/AECOSAN/web/nutricion/detalle/aladino_2015.htm (accessed on 7 January 2020).
- Willett, W.C.; Dietz, W.H.; Colditz, G.A. Guidelines for healthy weight. N. Engl. J. Med. 1999, 341, 427–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalle Grave, R.D.; Calugi, S.; Molinari, E.; Petroni, M.L.; Bondi, M.; Compare, A.; Marchesini, G. Weight loss expectations in obese patients and treatment attrition: An observational multicenter study. Obes. Res. 2005, 13, 1961–1969. [Google Scholar] [CrossRef] [PubMed]
- Buchwald, H.; Avidor, Y.; Braunwald, E.; Jensen, M.D.; Pories, W.; Fahrbach, K.; Schoelles, K. Bariatric surgery: A systematic review and meta-analysis. JAMA 2004, 292, 1724–1737. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Prevalence of Obesity * | Total Population Estimates | Estimated Number of PwO | PwO Sample Size Recommendation | Sample Size of Population with Obesity | Margin of Error † |
|---|---|---|---|---|---|---|
| Spain | 24% | 47,400,000 | 11,376,000 | 1500 | 0.013% | 2.5% |
| PwO (n = 1500) | HCPs (n = 306) | |
|---|---|---|
| Age, years (range) | 45 (18–81) | 50 (30–69) |
| Gender, n (%) | ||
| Female | 776 (52) | 218 (71) |
| Male | 721 (48) | 88 (29) |
| Other | 3 (<1) | 0 |
| BMI classification, n (%) | ||
| Respondents | 1500 (100) | 264 (86) |
| Underweight or healthy range (<25 kg/m2) | – | 150 (57) |
| Overweight (25–29.9 kg/m2) | – | 107 (41) |
| Obesity Class I (30–34.9 kg/m2) | 1029 (69) | 6 (2) |
| Obesity Class II (35–39.9 kg/m2) | 282 (18) | 0 |
| Obesity Class III (≥40 kg/m2) | 189 (12) | 1(<1) |
| Number of comorbidities, n (%) | ||
| 0 | 326 (17) | – |
| 1 | 370 (21) | – |
| 2 | 335 (24) | – |
| 3 | 242 (19) | – |
| ≥4 | 227 (19) | – |
| HCP category, n (%) | ||
| PCP | – | 156 (51) |
| Specialist | – | 150 (49) |
| Endocrinologist | – | 73 (24) |
| Internal medicine (non-PCP) | – | 23 (8) |
| Other * | – | 54 (18) |
| Obesity specialist, n (%) † | ||
| Yes | – | 247 (81) |
| No | – | 59 (19) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvador, J.; Vilarrasa, N.; Poyato, F.; Rubio, M.Á. Perceptions, Attitudes, and Barriers to Obesity Management in Spain: Results from the Spanish Cohort of the International ACTION-IO Observation Study. J. Clin. Med. 2020, 9, 2834. https://doi.org/10.3390/jcm9092834
Salvador J, Vilarrasa N, Poyato F, Rubio MÁ. Perceptions, Attitudes, and Barriers to Obesity Management in Spain: Results from the Spanish Cohort of the International ACTION-IO Observation Study. Journal of Clinical Medicine. 2020; 9(9):2834. https://doi.org/10.3390/jcm9092834
Chicago/Turabian StyleSalvador, Javier, Nuria Vilarrasa, Francisco Poyato, and Miguel Ángel Rubio. 2020. "Perceptions, Attitudes, and Barriers to Obesity Management in Spain: Results from the Spanish Cohort of the International ACTION-IO Observation Study" Journal of Clinical Medicine 9, no. 9: 2834. https://doi.org/10.3390/jcm9092834
APA StyleSalvador, J., Vilarrasa, N., Poyato, F., & Rubio, M. Á. (2020). Perceptions, Attitudes, and Barriers to Obesity Management in Spain: Results from the Spanish Cohort of the International ACTION-IO Observation Study. Journal of Clinical Medicine, 9(9), 2834. https://doi.org/10.3390/jcm9092834