Effects of Physical Rehabilitation on Spatiotemporal Gait Parameters and Ground Reaction Forces of Patients with Intermittent Claudication

 , , , ,
, , , ,
Abstract
1. Introduction
Study Aim
2. Materials and Methods
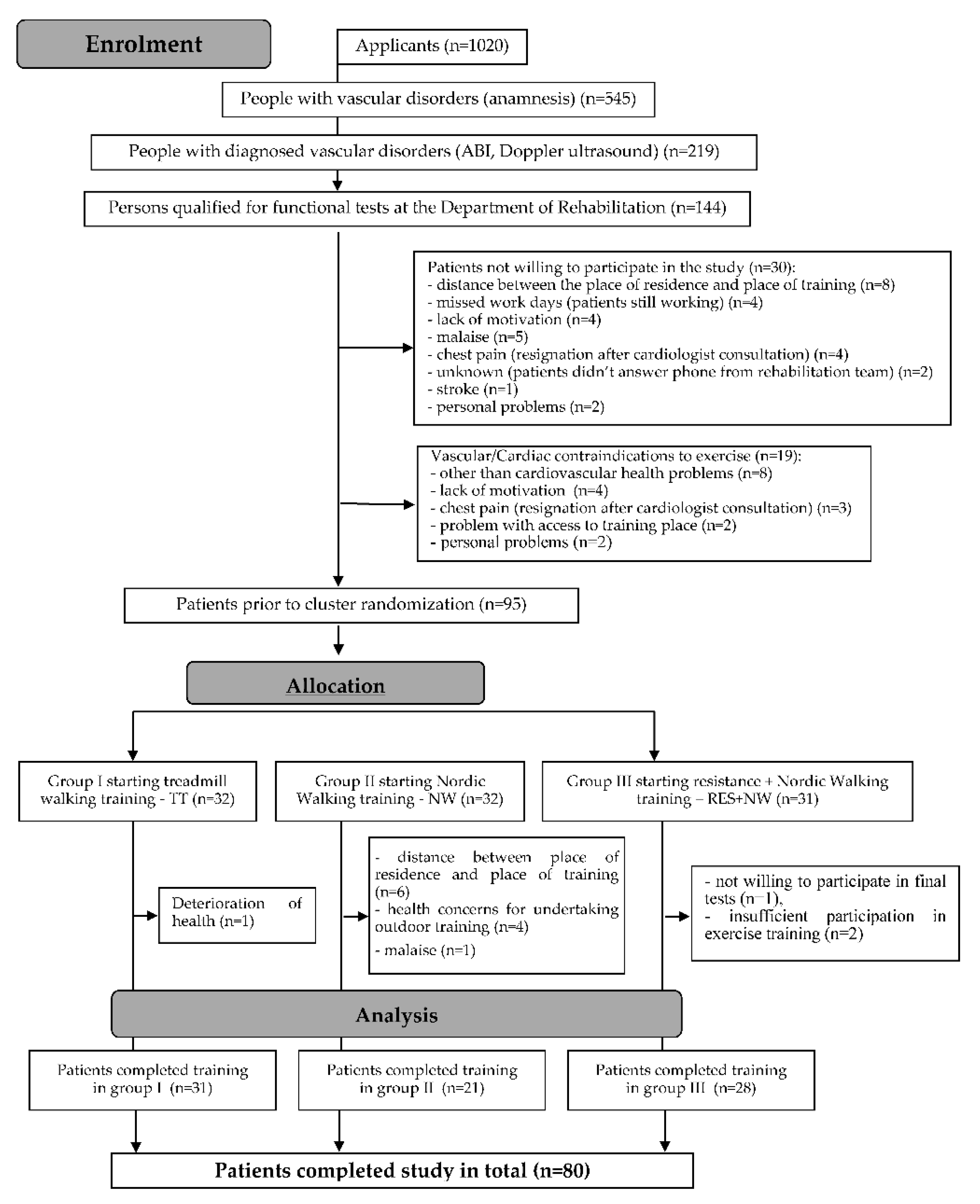
Sample Characteristics
3. Study Methods
3.1. Gait Tests
3.1.1. Gait Biomechanics Tests
3.1.2. Six-Minute Walk Test (6MWT)
3.2. Physical Rehabilitation of Patients
3.3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
- Nordic walking training led to greater improvements in the gait pattern of patients with PAD compared to combined and standard training.
- Combined training (NW + ISO) corrected the walking pattern to a lesser extent than NW training. However, by strengthening the muscles of the lower extremities, it increased the amplitude of the general center of gravity oscillation to the greatest extent.
- Treadmill training had little effect on the gait pattern of PAD patients.
- Nordic walking training should be included in the rehabilitation of patients with PAD as a form of gait training, which can be conducted under supervised or unsupervised conditions.
Author Contributions
Funding
Conflicts of Interest
References
- Gardner, A.; Parker, D.E.; Montgomery, P.S. Predictors of Improved Walking after a Supervised Walking Exercise Program in Men and Women with Peripheral Artery Disease. Int. J. Vasc. Med. 2016. Available online: https://www.hindawi.com/journals/ijvm/2016/2191350/ (accessed on 21 February 2020).
- Simon, F.; Oberhuber, A.; Floros, N.; Düppers, P.; Schelzig, H.; Duran, M. Pathophysiology of chronic limb ischemia. Gefässchirurgie 2018, 23, 13–18. [Google Scholar] [CrossRef]
- Pipinos, I.I.; Judge, A.R.; Selsby, J.T.; Zhu, Z.; Swanson, S.A.; Nella, A.A.; Dodd, S.L. Basic science review: The myopathy of peripheral arterial occlusive disease: Part 2. Oxidative stress, neuropathy, and shift in muscle fiber type. Vasc. Endovasc. Surg. 2008, 42, 101–112. [Google Scholar] [CrossRef]
- Chen, S.-J.; Pipinos, I.; Johanning, J.; Radovic, M.; Huisinga, J.M.; Myers, S.A.; Stergiou, N. Bilateral claudication results in alterations in the gait biomechanics at the hip and ankle joints. J. Biomech. 2008, 41, 2506–2514. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.; Montgomery, P.S.; Ritti-Dias, R.M.; Forrester, L. The effect of claudication pain on temporal and spatial gait measures during self-paced ambulation. Vasc. Med. 2009, 15, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Myers, S.A.; Applequist, B.C.; Huisinga, J.M.; Pipinos, I.I.; Johanning, J.M. Gait kinematics and kinetics are affected more by peripheral arterial disease than by age. J. Rehabil. Res. Dev. 2016, 53, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Szymczak, M.; Krupa, P.; Oszkinis, G.; Majchrzycki, M. Gait pattern in patients with peripheral artery disease. BMC Geriatr. 2018, 18, 52. [Google Scholar] [CrossRef]
- Gardner, A.W.; Forrester, L.; Smith, G.V. Altered gait profile in subjects with peripheral arterial disease. Vasc. Med. Lond. Engl. 2001, 6, 31–34. [Google Scholar] [CrossRef]
- Koutakis, P.; Pipinos, I.I.; Myers, S.A.; Stergiou, N.; Lynch, T.G.; Johanning, J.M. Joint torques and powers are reduced during ambulation for both limbs in patients with unilateral claudication. J. Vasc. Surg. 2010, 51, 80–88. [Google Scholar] [CrossRef]
- Dziubek, W.; Bulińska, K.; Stefańska, M.; Woźniewski, M.; Kropielnicka, K.; Jasiński, T.; Jasiński, R.; Pilch, U.; Dabrowska, G.; Skórkowska-Telichowska, K.; et al. Peripheral arterial disease decreases muscle torque and functional walking capacity in elderly. Maturitas 2015, 81, 480–486. [Google Scholar] [CrossRef]
- Prevention and Treatment of PAD. Available online: https://www.heart.org/en/health-topics/peripheral-artery-disease/prevention-and-treatment-of-pad. (accessed on 4 March 2020).
- McDermott, M.M.; Kibbe, M.R.; Guralnik, J.M.; Ferrucci, L.; Criqui, M.H.; Domanchuk, K.; Tian, L.; Zhao, L.; Li, L.; Patel, K.; et al. Durability of benefits from supervised treadmill exercise in people with peripheral artery disease. J. Am. Hear. Assoc. 2018, 8, e009380. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Balady, G.J.; Amsterdam, E.A.; Chaitman, B.; Eckel, R.; Fleg, J.; Froelicher, V.F.; Leon, A.S.; Piña, I.L.; Rodney, R.; et al. Exercise standards for testing and training. Circulation 2001, 104, 1694–1740. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, W.R.; Wolfel, E.E.; Meier, R.H.; Regensteiner, J.G. Superiority of treadmill walking exercise versus strength training for patients with peripheral arterial disease. Implications for the mechanism of the training response. Circulatuion 1994, 90, 1866–1874. [Google Scholar] [CrossRef] [PubMed]
- Konik, A.; Kuklewicz, S.; Rosloniec, E.; Zając, M.; Spannbauer, A.; Nowobilski, R.; Mika, P.M.S.C. Effects of 12-week supervised treadmill training on spatio-temporal gait parameters in patients with claudication. Disabil. Rehabil. 2016, 38, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Schieber, M.N.; Pipinos, I.I.; Johanning, J.M.; Casale, G.P.; Williams, M.A.; Despiegelaere, H.K.; Senderling, B.; Myers, S.A. Supervised walking exercise therapy improves gait biomechanics in patients with peripheral artery disease. J. Vasc. Surg. 2020, 71, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; Maarij, K.; Moxon, J.V.; Beard, J.D.; Girold, S.; Wrang, H.; Morris, D.R. Systematic review and meta-analysis of clinical trials examining the benefit of exercise programmes using nordic walking in patients with peripheral artery disease. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Wee, I.J.; Syn, N.L.; Choong, A.M.T.L. Nordic walking in patients with peripheral artery disease. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 465. [Google Scholar] [CrossRef]
- WROVASC. Ośrodek Badawczo-Rozwojowy. Available online: http://www.wssobr-wroc.pl/projekty/wrovasc/. (accessed on 21 February 2020).
- Kropielnicka, K.; Dziubek, W.; Bulińska, K.; Stefańska, M.; Wojcieszczyk-Latos, J.; Jasiński, R.; Pilch, U.; Dąbrowska, G.; Skórkowska-Telichowska, K.; Kałka, D.; et al. Influence of the physical training on muscle function and walking distance in symptomatic peripheral arterial disease in elderly. BioMed Res. Int. 2018. Available online: https://www.hindawi.com/journals/bmri/2018/1937527/. (accessed on 21 February 2020).
- Izquierdo-Porrera, A.M.; Gardner, A.W.; Bradham, U.D.; Montgomery, P.S.; Sorkin, J.D.; Powell, C.C.; Katzel, L.I. Relationship between objective measures of peripheral arterial disease severity to self-reported quality of life in older adults with intermittent claudication. J. Vasc. Surg. 2005, 41, 625–630. [Google Scholar] [CrossRef]
- Aronow, W.S. Peripheral arterial disease of the lower extremities. Arch. Med Sci. 2012, 8, 375–388. [Google Scholar] [CrossRef]
- Msc, J.B.; Aparicio, L.S.; Waisman, G.D. Challenges associated with peripheral arterial disease in women. Vasc. Heal. Risk Manag. 2014, 10, 115–128. [Google Scholar]
- Criqui, M.H.; Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef]
- Muller, M.D.; Reed, A.B.; Leuenberger, U.A.; Sinoway, L.I. Physiology in medicine: Peripheral arterial disease. J. Appl. Physiol. 2013, 115, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Herman, S.D.; Liu, K.; Tian, L.; Guralnik, J.M.; Ferrucci, L.; Criqui, M.H.; Liao, Y.; McDermott, M.M. Baseline lower extremity strength and subsequent decline in functional performance at 6-year follow-up in persons with lower extremity peripheral arterial disease. J. Am. Geriatr. Soc. 2009, 57, 2246–2252. [Google Scholar] [CrossRef]
- Myers, S.A.; Johanning, J.M.; Stergiou, N.; Celis, R.I.; Robinson, L.; Pipinos, I.I. Gait variability is altered in patients with peripheral arterial disease. J. Vasc. Surg. 2009, 49, 924–931.e1. [Google Scholar] [CrossRef] [PubMed]
- Scott-Pandorf, M.M.; Stergiou, N.; Johanning, J.M.; Robinson, L.; Lynch, T.G.; Pipinos, I.I. Peripheral arterial disease affects ground reaction forces during walking. J. Vasc. Surg. 2007, 46, 491–499. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Donelan, J.M.; Kram, R.; Kuo, D.A. Mechanical and Metabolic Determinants of the Preferred Step Width in Human Walking. In Proceedings of the Royal Society B: Biological Sciences; The Royal Society: London, UK, 2001; Volume 268, pp. 1985–1992. [Google Scholar]
- England, J.D.; Regensteiner, J.G.; Ringel, S.P.; Carry, M.R.; Hiatt, W.R. Muscle denervation in peripheral arterial disease. Neurology 1992, 42, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Konik, A.; Mika, P.; Nowobilski, R.; Andrzejczak, A.; Szczeklik, A. Mechanisms responsible for reducing intermittent claudication as a result of treadmill training. Acta Angiol. 2010, 16, 49–66. [Google Scholar]
- McDermott, M.M.; Ferrucci, L.; Guralnik, J.; Tian, L.; Liu, K.; Hoff, F.; Liao, Y.; Criqui, M.H. Pathophysiological changes in calf muscle predict mobility loss at 2-year follow-up in men and women with peripheral arterial disease. Circulation 2009, 120, 1048–1055. [Google Scholar] [CrossRef]
- Gommans, L.N.; Scheltinga, M.R.; Van Sambeek, M.R.; Maas, A.H.; Bendermacher, B.L.; Teijink, J. Gender differences following supervised exercise therapy in patients with intermittent claudication. J. Vasc. Surg. 2015, 62, 681–688. [Google Scholar] [CrossRef]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R. Fowkes on behalf the TASC II Worker Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef]
- Treat-Jacobson, D.; McDermott, M.M.; Bronas, U.G.; Campia, U.; Collins, T.C.; Criqui, M.H.; Gardner, A.W.; Hiatt, W.R.; Regensteiner, J.G.; Rich, K.; et al. Optimal exercise programs for patients with peripheral artery disease: A scientific statement from the American Heart Association. Circulation 2019, 139, e10–e33. [Google Scholar] [CrossRef]
- Bulińska, K.; Kropielnicka, K.; Jasiński, T.; Wojcieszczyk-Latos, J.; Pilch, U.; Dąbrowska, G.; Skórkowska-Telichowska, K.; Kałka, D.; Zywar, K.; Paszkowski, R.; et al. Nordic pole walking improves walking capacity in patients with intermittent claudication: A randomized controlled trial. Disabil. Rehabil. 2015, 38, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Greig, C.A.; Butler, F.; A Skelton, D.; Mahmud, S.; Young, A. Treadmill walking in old age may not reproduce the real life situation. J. Am. Geriatr. Soc. 1993, 41, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Hidler, J. Biomechanics of overground vs. treadmill walking in healthy individuals. J. Appl. Physiol. 2008, 104, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Collins, E.G.; McBurney, C.; Butler, J.; Jelinek, C.; O’Connell, S.; Fritschi, C.; Reda, M. The Effects of Walking or Walking-With-Poles Training on Tissue Oxygenation in Patients with Peripheral Arterial Disease. Int. J. Vasc. Med. 2012. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3463188/ (accessed on 4 March 2020).
- Oakley, C.; Zwierska, I.; Tew, G.; Beard, J.; Saxton, J.M. Nordic poles immediately improve walking distance in patients with intermittent claudication. J. Vasc. Surg. 2008, 36, 689–694. [Google Scholar]
- Church, T.S.; Earnest, C.P.; Morss, G.M. Field testing of physiological responses associated with nordic walking. Res. Q. Exerc. Sport 2002, 73, 296–300. [Google Scholar] [CrossRef]
- Morss, G.M.; Church, T.S.; Earnest, C.P.; Jordan, A.N. Field test comparing the metabolic cost of normal walking versus nordic walking. Med. Sci. Sports Exerc. 2001, 33, S23. [Google Scholar] [CrossRef]
- Girold, S.; Rousseau, J.; Le Gal, M.; Coudeyre, E.; Le Henaff, J. Nordic walking versus walking without poles for rehabilitation with cardiovascular disease: Randomized controlled trial. Ann. Phys. Rehabil. Med. 2017, 60, 223–229. [Google Scholar] [CrossRef]
- McGuigan, M.R.; Bronks, R.; Newton, R.U.; Sharman, M.J.; Graham, J.C.; Cody, D.V.; Kraemer, W.J. Resistance training in patients with peripheral arterial disease: Effects on myosin isoforms, fiber type distribution, and capillary supply to skeletal muscle. J. Gerontol. Ser. A: Boil. Sci. Med Sci. 2001, 56, B302–B310. [Google Scholar] [CrossRef]
- Wang, E.; Helgerud, J.; Loe, H.; Indseth, K.; Kaehler, N.; Hoff, J. Maximal strength training improves walking performance in peripheral arterial disease patients. Scand. J. Med. Sci. Sports 2010, 20, 764–770. [Google Scholar] [CrossRef]
- Parmenter, B.; Mavros, Y.; Dias, R.R.; King, S.; Singh, M.F. Resistance training as a treatment for older persons with peripheral artery disease: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 452–461. [Google Scholar]
- King, S.L.; Vanicek, N.; Mockford, K.A.; Coughlin, P.A. The effect of a 3-month supervised exercise programme on gait parameters of patients with peripheral arterial disease and intermittent claudication. Clin. Biomech. 2012, 27, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Kocur, P.; Wiernicka, M.; Wilski, M.; Kaminska, E.; Furmaniuk, L.; Maslowska, M.F.; Lewandowski, J. Does Nordic walking improves the postural control and gait parameters of women between the age 65 and 74: A randomized trial. J. Phys. Ther. Sci. 2015, 27, 3733–3737. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Yang, D.J.; Kang, Y.H.; Kim, J.H.; Uhm, Y.H.; Lee, Y.S. Effects of Nordic walking and walking on spatiotemporal gait parameters and ground reaction force. J. Phys. Ther. Sci. 2015, 27, 2891–2893. [Google Scholar] [CrossRef] [PubMed]
- Tschentscher, M.; Niederseer, D.; Niebauer, J. Health benefits of nordic walking a systematic review. Am. J. Prev. Med. 2013, 44, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.D.; Booth, J.; Taylor, J.L.; Barry, B.K. Aerobic training increases pain tolerance in healthy individuals. Med. Sci. Sports Exerc. 2014, 46, 1640–1647. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group TT (n = 31) | Group NW (n = 21) | Group ISO + NW (n = 28) | p | ||||
|---|---|---|---|---|---|---|---|
| Average | SD | Average | SD | Average | SD | ||
| Age [years] | 67.00 | 7.43 | 67.00 | 9.32 | 67.82 | 8.49 | 0.92 |
| Height [cm] | 168.03 | 8.56 | 166.81 | 7.40 | 169.54 | 9.07 | 0.53 |
| Body weight [kg] | 79.02 | 14.31 | 74.44 | 12.44 | 78.84 | 15.43 | 0.47 |
| ABI R | 0.68 | 0.19 | 0.76 | 0.17 | 0.76 | 0.19 | 0.14 |
| ABI L | 0.68 | 0.16 | 0.71 | 0.22 | 0.70 | 0.19 | 0.84 |
| Group TT (n = 31) | Group NW (n = 21) | Group ISO + NW (n = 28) | Chi2 Test p | |
|---|---|---|---|---|
| Smoking: | ||||
| smokers | 9(29%) | 9(42.9%) | 7(25%) | 0.5030 |
| active/past smokers | 6/3 | 5/4 | 5/2 | |
| Diabetes type 2 | 12(38.7%) | 8(38.1%) | 12(42.9%) | 0.5630 |
| Hypertension | 26(83.9%) | 14(66.7%) | 20(71.4%) | 0.0016 * |
| Revascularisation | 11(35.5%) | 7(33.3%) | 8(28.6%) | 0.8442 |
| Degenerative changes of the spine and/or peripheral joints | 12(38.7%) | 4(19.0%) | 8(28.6%) | 0.2180 |
| PAD type (n) | 26 FP (83.9%) 4 AI (12.9%) 1 ML (3.2%) | 16 FP (76.2%) 3 AI (14.3%) 1 ML (4.89%) 1 P (4.8%) | 23 FP (82.1%) 2 AI (7,1%) 1 ML (3.6%) 2 P (7.1%) |
| Group TT | Group NW | Group ISO + NW | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before | AFter | Before | After | |||||||
| Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | |
| velMEAN [m/s] | 0.92 | 0.14 | 0.95 | 0.13 | 0.87 | 0.11 | 0.97 | 0.16 | 0.94 | 0.16 | 0.99 | 0.18 |
| CADENCE (step/min) | 99.22 | 10.84 | 101.09 | 9.16 | 101.22 | 11.08 | 104.09 | 8.81 | 100.66 | 10.81 | 99.88 | 8.45 |
| velSTRIDE R [m/s] | 0.93 | 0.14 | 0.96 | 0.13 | 0.88 | 0.13 | 0.98 | 0.16 | 0.96 | 0.16 | 1.01 | 0.18 |
| velSTRIDE L [m/s] | 0.93 | 0.14 | 0.96 | 0.13 | 0.88 | 0.12 | 0.98 | 0.16 | 0.96 | 0.16 | 1.01 | 0.18 |
| velSWING R [m/s] | 2.30 | 0.29 | 2.36 | 0.29 | 2.23 | 0.27 | 2.49 | 0.32 | 2.31 | 0.40 | 2.5 | 0.37 |
| velSWING L [m/s] | 2.28 | 0.30 | 2.35 | 0.28 | 2.18 | 0.26 | 2.46 | 0.31 | 2.34 | 0.41 | 2.51 | 0.40 |
| tSTRIDE R [s] | 1.20 | 0.11 | 1.18 | 0.11 | 1.20 | 0.12 | 1.15 | 0.10 | 1.24 | 0.12 | 1.19 | 0.12 |
| tSTRIDE L [s] | 1.20 | 0.11 | 1.19 | 0.11 | 1.20 | 0.11 | 1.15 | 0.10 | 1.24 | 0.12 | 1.18 | 0.12 |
| tSWING R [s] | 0.43 | 0.05 | 0.42 | 0.04 | 0.42 | 0.06 | 0.40 | 0.04 | 0.43 | 0.03 | 0.42 | 0.04 |
| tSWING L [s] | 0.43 | 0.04 | 0.42 | 0.04 | 0.42 | 0.05 | 0.40 | 0.04 | 0.42 | 0.03 | 0.41 | 0.04 |
| tSTANCE R [s] | 0.77 | 0.08 | 0.76 | 0.08 | 0.77 | 0.06 | 0.76 | 0.07 | 0.77 | 0.08 | 0.79 | 0.09 |
| tSTANCE L [s] | 0.78 | 0.08 | 0.76 | 0.09 | 0.78 | 0.09 | 0.76 | 0.08 | 0.77 | 0.09 | 0.79 | 0.09 |
| tdoubleSTRIDE R [s] | 1.20 | 0.11 | 1.18 | 0.12 | 1.19 | 0.12 | 1.16 | 0.10 | 1.20 | 0.13 | 1.21 | 0.11 |
| tdoubleSTRIDE L [s] | 1.20 | 0.11 | 1.18 | 0.12 | 1.19 | 0.12 | 1.16 | 0.10 | 1.21 | 0.13 | 1.21 | 0.11 |
| lenght STRIDE R [m] | 0.50 | 0.05 | 0.51 | 0.05 | 0.47 | 0.06 | 0.50 | 0.08 | 0.53 | 0.05 | 0.51 | 0.08 |
| lenght STRIDE L [m] | 0.51 | 0.05 | 0.52 | 0.06 | 0.47 | 0.06 | 0.51 | 0.07 | 0.53 | 0.06 | 0.52 | 0.07 |
| widht STRIDE R [m] | 0.16 | 0.02 | 0.16 | 0.02 | 0.15 | 0.02 | 0.15 | 0.02 | 0.16 | 0.02 | 0.16 | 0.02 |
| widht STRIDE L [m] | 0.16 | 0.02 | 0.16 | 0.02 | 0.15 | 0.02 | 0.15 | 0.02 | 0.16 | 0.02 | 0.16 | 0.02 |
| TT | NW | ISO + NW | |
|---|---|---|---|
| velMEAN [m/s] | 0.1043 | 0.0066 * | 0.0237 * |
| CADENCE (step/min) | 0.0718 | 0.2577 | 0.4658 |
| velSTRIDE R [m/s] | 0.1305 | 0.0074 * | 0.0356 * |
| velSTRIDE L [m/s] | 0.1539 | 0.0040 * | 0.0584 |
| velSWING R [m/s] | 0.1676 | 0.0027 * | 0.0133 * |
| velSWING L [m/s] | 0.1495 | 0.0010 * | 0.0295 * |
| tSTRIDE R [s] | 0.1001 | 0.0272 * | 0.0167 * |
| tSTRIDE L [s] | 0.0386 * | 0.0366 * | 0.0108 * |
| tSWING R [s] | 0.4291 | 0.0198 * | 0.0608 |
| tSWING L [s] | 0.4069 | 0.0150 * | 0.2339 |
| tSTANCE R [s] | 0.0922 | 0.1980 | 0.4125 |
| tSTANCE L [s] | 0.0474 * | 0.7493 | 0.3870 |
| tdoubleSTRIDE R [s] | 0.0889 | 0.2687 | 0.4018 |
| tdoubleSTRIDE L [s] | 0.0378 * | 0.3148 | 0.3555 |
| length STRIDE R [m] | 0.9314 | 0.0126 * | 0.8037 |
| length STRIDE L [m] | 0.6693 | 0.0041 * | 0.7205 |
| width STRIDE R [m] | 0.7868 | 0.7245 | 0.6898 |
| width STRIDE L [m] | 0.7868 | 0.7245 | 0.6898 |
| TT | NW | ISO + NW | |
|---|---|---|---|
| velMEAN [m/s] | 0.1043 | 0.0066 * | 0.0237 * |
| CADENCE (step/min) | 0.0718 | 0.2577 | 0.4658 |
| velSTRIDE R [m/s] | 0.1305 | 0.0074 * | 0.0356 * |
| velSTRIDE L [m/s] | 0.1539 | 0.0040 * | 0.0584 |
| velSWING R [m/s] | 0.1676 | 0.0027 * | 0.0133 * |
| velSWING L [m/s] | 0.1495 | 0.0010 * | 0.0295 * |
| tSTRIDE R [s] | 0.1001 | 0.0272 * | 0.0167 * |
| tSTRIDE L [s] | 0.0386 * | 0.0366 * | 0.0108 * |
| tSWING R [s] | 0.4291 | 0.0198 * | 0.0608 |
| tSWING L [s] | 0.4069 | 0.0150 * | 0.2339 |
| tSTANCE R [s] | 0.0922 | 0.1980 | 0.4125 |
| tSTANCE L [s] | 0.0474 * | 0.7493 | 0.3870 |
| tdoubleSTRIDE R [s] | 0.0889 | 0.2687 | 0.4018 |
| tdoubleSTRIDE L [s] | 0.0378 * | 0.3148 | 0.3555 |
| length STRIDE R [m] | 0.9314 | 0.0126 * | 0.8037 |
| length STRIDE L [m] | 0.6693 | 0.0041 * | 0.7205 |
| width STRIDE R [m] | 0.7868 | 0.7245 | 0.6898 |
| width STRIDE L [m] | 0.7868 | 0.7245 | 0.6898 |
| Group TT | Group NW | Group ISO + NW | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | AFter | Before | After | Before | After | |||||||
| Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | Mean | ±SD | |
| VE max1 R [%BW] | 98.06 | 4.30 | 98.02 | 4.10 | 99.19 | 5.11 | 100.06 | 5.30 | 101.27 | 5.57 | 99.79 | 5.06 |
| VE max2 R [%BW] | 104.28 | 5.82 | 105.87 | 4.99 | 104.43 | 6.85 | 104.96 | 8.80 | 105.30 | 4.47 | 104.32 | 4.57 |
| VE min R [%BW] | 86.65 | 4.33 | 85.85 | 3.93 | 86.31 | 4.88 | 84.22 | 6.58 | 89.40 | 5.32 | 83.89 | 5.98 |
| VE max1 L [%BW] | 99.22 | 3.89 | 99.09 | 3.78 | 98.20 | 4.30 | 100.19 | 4.64 | 99.62 | 5.43 | 101.9 | 5.55 |
| VE max2 L [%BW] | 103.97 | 4.51 | 104.94 | 4.70 | 103.22 | 5.82 | 105.01 | 8.31 | 104.75 | 5.07 | 104.72 | 5.15 |
| VE min L [%BW] | 85.87 | 4.38 | 86.23 | 4.69 | 87.88 | 3.75 | 84.63 | 6.54 | 88.38 | 4.78 | 82.70 | 5.36 |
| AP max R [%BW] | 13.53 | 2.42 | 14.06 | 2.76 | 12.70 | 3.27 | 14.09 | 2.71 | 14.83 | 3.57 | 14.88 | 2.74 |
| AP min R [%BW] | −11.10 | 2.83 | −11.87 | 2.78 | −10.45 | 2.39 | −12.10 | 2.45 | −12.01 | 3.76 | −12.26 | 3.15 |
| AP max L [%BW] | 13.33 | 2.31 | 13.75 | 2.31 | 12.55 | 2.56 | 13.93 | 3.86 | 13.65 | 3.80 | 14.8 | 3.01 |
| AP min L [%BW] | −11.56 | 2.42 | −11.99 | 2.51 | −9.71 | 1.83 | −11.56 | 2.79 | −12.11 | 3.15 | −12.71 | 3.04 |
| ML max R [%BW] | 5.77 | 1.47 | 5.79 | 1.58 | 5.55 | 1.32 | 5.68 | 1.65 | 6.44 | 1.38 | 6.14 | 1.37 |
| ML min R [%BW] | −2.35 | 0.98 | −2.45 | 1.09 | −2.35 | 0.95 | −2.76 | 1.39 | −2.52 | 1.20 | −2.69 | 1.19 |
| ML max L [%BW] | 5.77 | 1.47 | 5.79 | 1.58 | 5.55 | 1.32 | 5.68 | 1.65 | 6.44 | 1.38 | 6.14 | 1.37 |
| ML min L [%BW] | −2.35 | 0.98 | −2.45 | 1.09 | −2.35 | 0.95 | −2.76 | 1.39 | −2.52 | 1.20 | −2.56 | 1.31 |
| TT | NW | ISO + NW | |
|---|---|---|---|
| VE max1[%BW]R | 0.8324 | 0.5827 | 0.3778 |
| VE max2[%BW]R | 0.0198 * | 0.5844 | 0.4051 |
| VE min[%BW]R | 0.2547 | 0.2364 | 0.0030 * |
| VE max1[%BW]L | 0.8488 | 0.0536 | 0.2537 |
| VE max2[%BW]L | 0.1284 | 0.1341 | 0.9672 |
| VE min[%BW]L | 0.6223 | 0.0092 * | 0.0035 * |
| AP max[%BW]R | 0.1425 | 0.0455 * | 0.6995 |
| AP min[%BW]R | 0.1342 | 0.0216 * | 0.5901 |
| AP max[%BW]L | 0.2990 | 0.0151 * | 0.1678 |
| AP min[%BW]L | 0.3950 | 0.0006 * | 0.7195 |
| ML max[%BW]R | 0.9008 | 0.7549 | 0.5326 |
| ML min[%BW]R | 0.6001 | 0.1927 | 0.8457 |
| ML max[%BW]L | 0.9008 | 0.7549 | 0.5326 |
| ML min[%BW]L | 0.6001 | 0.1927 | 0.9201 |
| ANOVA. | TRAINING | TEST | INTERACTION (Training&Test) |
|---|---|---|---|
| VE max1 R [%BW] | NS | NS | NS |
| VE max2 R [%BW] | NS | NS | NS |
| VE min R [%BW] | NS | 0.0003 * | 0.0180 * |
| VE max1 L [%BW] | NS | 0.0466 * | NS |
| VE max2 L [%BW] | NS | NS | NS |
| VE min L [%BW] | NS | 0.0000 * | 0.0014 * |
| AP max R [%BW] | NS | 0.0201 * | NS |
| AP min R [%BW] | NS | 0.0132 * | NS |
| AP max L [%BW] | NS | 0.0017 * | NS |
| AP min L [%BW] | 0.0453 * | 0.0031 * | 0.0178 * |
| ML max R [%BW] | NS | NS | NS |
| ML min R [%BW] | NS | NS | NS |
| ML max L [%BW] | NS | NS | NS |
| ML min L [%BW] | NS | NS | NS |
| Before | After | p | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Median | SD | Mean | Median | SD | |||
| TT | Total distance [m] | 343.50 | 358.00 | 66.46 | 375.11 | 380.00 | 69.79 | 0.0002 * |
| CI distances ** [m] | 167.35 | 155.00 | 111.23 | 182.27 | 200.00 | 122.82 | 0.6406 | |
| NW | Total distance [m] | 354.00 | 350.00 | 56.07 | 392.52 | 397.00 | 63.88 | 0.0011 * |
| CI distances ** [m] | 149.07 | 125.00 | 92.15 | 181.62 | 200.00 | 103.21 | 0.0290 * | |
| ISO + NW | Total distance [m] | 374.18 | 368.00 | 69.01 | 422.77 | 406.50 | 64.65 | 0.0007 * |
| CI distances ** [m] | 155.82 | 138.50 | 114.81 | 193.68 | 200.00 | 125.04 | 0.3507 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziubek, W.; Stefańska, M.; Bulińska, K.; Barska, K.; Paszkowski, R.; Kropielnicka, K.; Jasiński, R.; Rachwalik, A.; Woźniewski, M.; Szuba, A. Effects of Physical Rehabilitation on Spatiotemporal Gait Parameters and Ground Reaction Forces of Patients with Intermittent Claudication. J. Clin. Med. 2020, 9, 2826. https://doi.org/10.3390/jcm9092826
Dziubek W, Stefańska M, Bulińska K, Barska K, Paszkowski R, Kropielnicka K, Jasiński R, Rachwalik A, Woźniewski M, Szuba A. Effects of Physical Rehabilitation on Spatiotemporal Gait Parameters and Ground Reaction Forces of Patients with Intermittent Claudication. Journal of Clinical Medicine. 2020; 9(9):2826. https://doi.org/10.3390/jcm9092826
Chicago/Turabian StyleDziubek, Wioletta, Małgorzata Stefańska, Katarzyna Bulińska, Katarzyna Barska, Rafał Paszkowski, Katarzyna Kropielnicka, Ryszard Jasiński, Anna Rachwalik, Marek Woźniewski, and Andrzej Szuba. 2020. "Effects of Physical Rehabilitation on Spatiotemporal Gait Parameters and Ground Reaction Forces of Patients with Intermittent Claudication" Journal of Clinical Medicine 9, no. 9: 2826. https://doi.org/10.3390/jcm9092826
APA StyleDziubek, W., Stefańska, M., Bulińska, K., Barska, K., Paszkowski, R., Kropielnicka, K., Jasiński, R., Rachwalik, A., Woźniewski, M., & Szuba, A. (2020). Effects of Physical Rehabilitation on Spatiotemporal Gait Parameters and Ground Reaction Forces of Patients with Intermittent Claudication. Journal of Clinical Medicine, 9(9), 2826. https://doi.org/10.3390/jcm9092826