Are Further Interventions Needed to Prevent and Manage Hospital-Acquired Hyponatraemia? A Nationwide Cross-Sectional Survey of IV Fluid Prescribing Practices

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Setting and Study Population
2.2. Recruitment
2.3. Development of the Questionnaire
2.4. Outcome Measures
- A high-risk (potentially increased intracranial pressure) patient with hypovolaemia.
- A child in need of maintenance intravenous fluids without hypovolaemia and hyponatraemia.
- A hypovolaemic and hyponatraemic (P-Na = 110 mmol/L) patient without severe symptoms of hyponatraemia.
- A hyponatraemic (P-Na = 118 mmol/L) patient with severe symptoms of hyponatraemia.
- Renal water excretion in the acutely ill patient.
- Intravenous fluids impact on P-Na in the acutely ill patient.
- Hyperglycaemia and P-Na.
- Severe symptoms of hyponatraemia.
- Patients at high risk of severe symptoms.
- Prevention and treatment of over-correction of hyponatraemia.
2.5. Data Analysis
3. Results
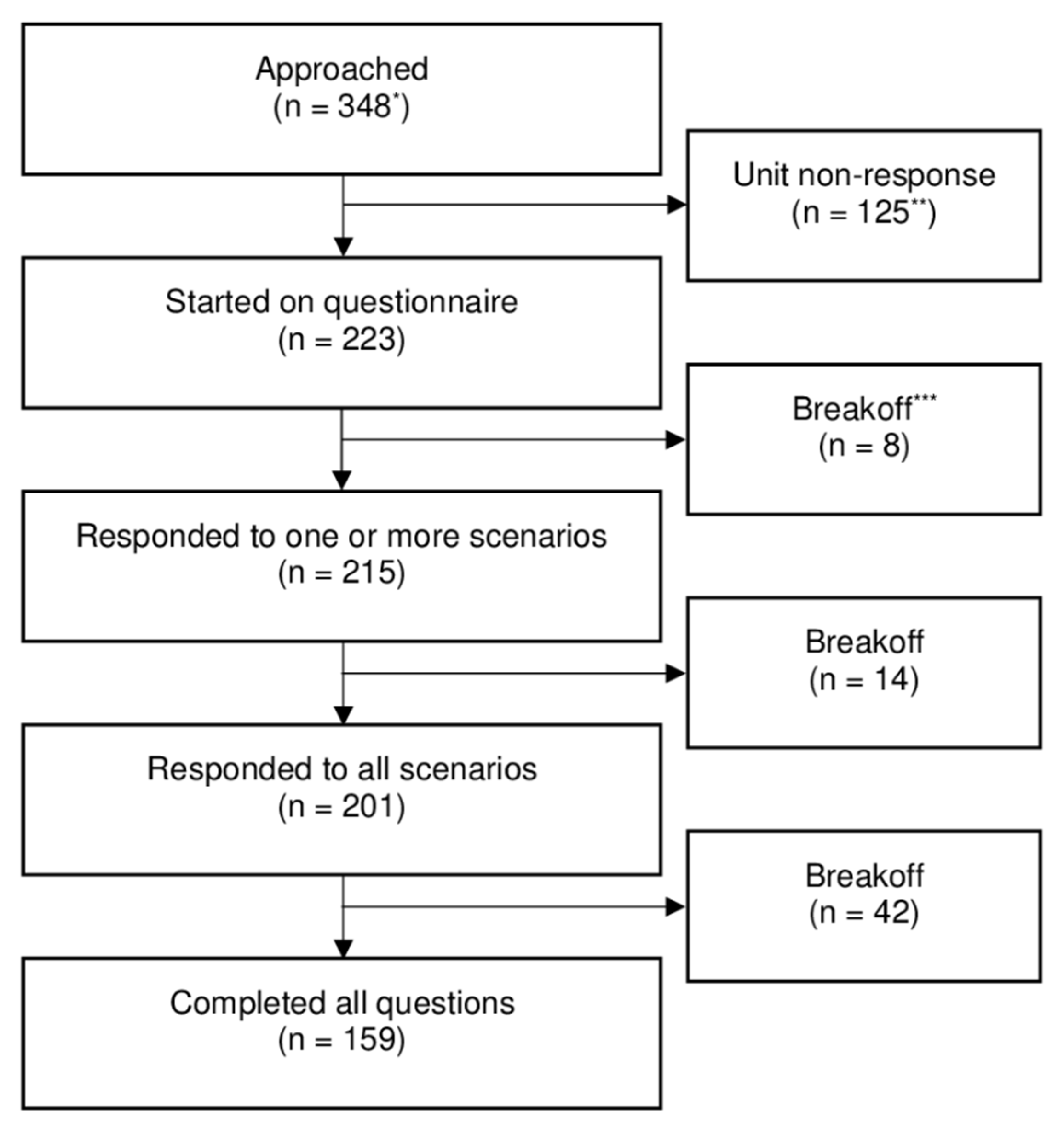
3.1. Characteristics of Respondents
3.2. Response to Scenario and Knowledge Questions
3.3. Analyses of Prescribing Practice by Demographical Variables and Characteristics of EDs
4. Discussion
4.1. Main Findings
4.1.1. Use of Hypotonic Intravenous Fluids
4.1.2. Linking Hypotonic Intravenous Fluid Treatment and Hyponatraemia
4.1.3. Treatment of Hyponatraemia with Severe Symptoms
4.2. Strengths and Limitations
4.3. Clinical Implications
- The association between hyponatraemia and hypotonic intravenous fluids.
- Intravenous fluids’ impact on P-Na in patients with reduced water excretion.
- Treatment of patients with severe symptoms of hyponatraemia.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moritz, M.L.; Ayus, J.C. Maintenance intravenous fluids in acutely Ill patients. N. Engl. J. Med. 2015, 373, 1350–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoorn, E.; Geary, D.; Robb, M.; Halperin, M.L.; Bohn, D. Acute hyponatremia related to intravenous fluid administration in hospitalized children: An observational study. Pediatrics 2004, 113, 1279–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overgaard-Steensen, C.; Ring, T. Clinical review: Practical approach to hyponatraemia and hypernatraemia in critically ill patients. Crit. Care 2013, 17, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spasovski, G.; Vanholder, R.; Allolio, B.; Annane, D.; Ball, S.; Bichet, D.; Decaux, G.; Fenske, W.; Hoorn, E.; Ichai, C.; et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Intensiv. Care Med. 2014, 40, 320–331. [Google Scholar] [CrossRef]
- Moritz, M.L.; Ayus, J.C. Prevention of hospital-acquired hyponatremia: A case for using isotonic saline. Pediatrics 2003, 111, 227–230. [Google Scholar] [CrossRef]
- Choong, K.; Kho, M.E.; Menon, K.; Bohn, D. Hypotonic versus isotonic saline in hospitalised children: A systematic review. Arch. Dis. Child. 2006, 91, 828–835. [Google Scholar] [CrossRef]
- Foster, B.A.; Tom, D.; Hill, V. Hypotonic versus isotonic fluids in hospitalized children: A systematic review and meta-analysis. J. Pediatr. 2014, 165, 163–169.e2. [Google Scholar] [CrossRef]
- Wang, J.; Xu, E.; Xiao, Y. Isotonic versus hypotonic maintenance IV fluids in hospitalized children: A meta-analysis. Pediatrics 2013, 133, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Karageorgos, S.A.; Kratimenos, P.; Landicho, A.; Haratz, J.; Argentine, L.; Jain, A.; McInnes, A.D.; Fisher, M.; Koutroulis, I. Hospital-acquired hyponatremia in children following hypotonic versus isotonic intravenous fluids infusion. Children 2018, 5, 139. [Google Scholar] [CrossRef] [Green Version]
- Velasco, P.; Alcaraz, A.; Oikonomopoulou, N.; Benito, M.; Moya, R.; Sánchez, Á. Hiponatremia adquirida en el hospital: Does the type of fluid therapy affect children admitted to intensive care? Rev. Chil. Pediatría 2018, 89, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Hoorn, E.; Lindemans, J.; Zietse, R. Development of severe hyponatraemia in hospitalized patients: Treatment-related risk factors and inadequate management. Nephrol. Dial. Transplant. 2005, 21, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, A.; Verbalis, J.G.; Amin, A.N.; Burst, V.R.; Chiodo, J.A., III; Chiong, J.R.; Dasta, J.F.; Friend, K.E.; Hauptman, P.J.; Peri, A.; et al. Current treatment practice and outcomes. Report of the hyponatremia registry. Kidney Int. 2015, 88, 167–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Institute for Safe Medication Practices Canada (ISMP Canada). Hospital-Acquired Acute Hyponatremia: Two Reports of Pediatric Deaths. Available online: https://www.ismp-canada.org/download/safetyBulletins/ISMPCSB2009-7-HospitalAcquiredAcuteHyponatremia.pdf (accessed on 23 September 2019).
- National Patient Safety Agency. Patient Safety Alert 22: Reducing the Risk of Hyponatraemia when Administering Intravenous Infusions to Children. Available online: https://webarchive.nationalarchives.gov.uk/20171030124309/http://www.nrls.npsa.nhs.uk/resources/?entryid45=59809&p=14 (accessed on 23 September 2019).
- Neilson, J.; O’Neill, F.; Dawoud, D.; Crean, P. Intravenous fluids in children and young people: Summary of NICE guidance. BMJ 2015, 351. [Google Scholar] [CrossRef] [PubMed]
- Feld, L.G.; Neuspiel, D.R.; Foster, B.A.; Leu, M.G.; Garber, M.D.; Austin, K.; Basu, R.K.; Conway, E.E.; Fehr, J.J.; Hawkins, C.; et al. Clinical practice guideline: Maintenance intravenous fluids in children. Pediatrics 2018, 142, e20183083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pharmacovigilance Risk Assessment Committee Recommendations on Signals Adopted at the 3–6 July 2017 PRAC. Available online: https://www.ema.europa.eu/en/committees/prac/prac-agendas-minutes-highlights#minutes-section (accessed on 11 August 2020).
- National Clinical Guideline Centre (UK). Intravenous Fluid Therapy: Intravenous Fluid Therapy in Adults in Hospital; National Institute for Health and Clinical Excellence: Guidance, Royal College of Physicians: London, UK, 2013. [Google Scholar]
- Drennan, J. Cognitive interviewing: Verbal data in the design and pretesting of questionnaires. J. Adv. Nurs. 2003, 42, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Peabody, J.; Luck, J.; Glassman, P.; Jain, S.; Hansen, J.; Spell, M.; Lee, M. Measuring the quality of physician practice by using clinical vignettes: A prospective validation study. Ann. Intern. Med. 2004, 141, 771–780. [Google Scholar] [CrossRef]
- Veloski, J.; Tai, S.; Evans, A.S.; Nash, D.B. Clinical vignette-based surveys: A tool for assessing physician practice variation. Am. J. Med Qual. 2005, 20, 151–157. [Google Scholar] [CrossRef]
- Sundhedsstyrelsen Faglig gennemgang af akutmodtagelserne [Professional Review of the Emergency Departments]. Available online: https://www.sum.dk/~/media/Filer%20-%20Publikationer_i_pdf/2014/Faglig-gennemgang-af-akutmodt-juni-2014/Faglig-gennemgang-af-akutmodtagelserne-juni-2014.ashx (accessed on 23 September 2019).
- Myburgh, J.A.; Mythen, M.G. Resuscitation fluids. N. Engl. J. Med. 2013, 369, 1243–1251. [Google Scholar] [CrossRef]
- Liamis, G.; Filippatos, T.; Elisaf, M. Correction of hypovolemia with crystalloid fluids: Individualizing infusion therapy. Postgrad. Med. 2015, 127, 405–412. [Google Scholar] [CrossRef]
- Bhave, G.; Neilson, E.G. Volume depletion versus dehydration: How understanding the difference can guide therapy. Am. J. Kidney Dis. 2011, 58, 302–309. [Google Scholar] [CrossRef] [Green Version]
- Lunøe, M.; Overgaard-Steensen, C. Prevention of hospital-acquired hyponatraemia: Individualised fluid therapy. Acta Anaesthesiol. Scand. 2015, 59, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Dansk Endokrinologisk Selskab NBV Endokrinologi: Hyponatriæmi [National Treatment Guideline Endocrinology: Hyponatraemia]. Available online: http://www.endocrinology.dk/index.php/6-andre-endokrinologiske-sygdomme/2-hyponatriaemi (accessed on 23 September 2019).
- Verbalis, J.G.; Goldsmith, S.R.; Greenberg, A.; Korzelius, C.; Schrier, R.W.; Sterns, R.H.; Thompson, C.J. Diagnosis, evaluation, and treatment of hyponatremia: Expert panel recommendations. Am. J. Med. 2013, 126, S1–S42. [Google Scholar] [CrossRef] [PubMed]
- Overview of the Treatment of Hyponatremia in Adults—UpToDate. Available online: https://www.uptodate.com/contents/overview-of-the-treatment-of-hyponatremia-in-adults?search=hyponatremia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H2818747047 (accessed on 11 August 2020).
- Evaluation and Management of Elevated Intracranial Pressure in Adults—UpToDate. Available online: https://www.uptodate.com/contents/evaluation-and-management-of-elevated-intracranial-pressure-in-adults?search=icp%20management&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 5 April 2020).
- Maintenance Intravenous Fluid Therapy in Children—UpToDate. Available online: https://www.uptodate.com/contents/maintenance-intravenous-fluid-therapy-in-children?search=maintenance%20fluids%20children&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 12 August 2020).
- Girdwood, S.T.; Parker, M.W.; Shaughnessy, E.E. Clinical guideline highlights for the hospitalist: Maintenance intravenous fluids in infants and children. J. Hosp. Med. 2019, 14, 170–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peris, J.M.R.; Rivas-Juesas, C.; Pérez, A.I.M.; Pérez, R.P.; Alapont, V.M.I.; Mallea, J.M.; De León, A.C. Use of hypotonic fluids in the prescription of maintenance intravenous fluid therapy. An. Pediatría Engl. Ed. 2019, 91, 158–165. [Google Scholar] [CrossRef]
- Freeman, M.; Ayus, J.C.; Moritz, M.L. Maintenance intravenous fluid prescribing practices among paediatric residents. Acta Paediatr. 2012, 101, e465–e468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Self, W.H.; Semler, M.W.; Wanderer, J.P.; Wang, L.; Byrne, D.W.; Collins, S.P.; Slovis, C.M.; Lindsell, C.J.; Ehrenfeld, J.M.; Siew, E.D.; et al. Balanced crystalloids versus saline in noncritically Ill adults. N. Engl. J. Med. 2018, 378, 819–828. [Google Scholar] [CrossRef]
- Carandang, F.; Anglemyer, A.; Longhurst, C.A.; Krishnan, G.; Alexander, S.R.; Kahana, M.; Sutherland, S.M. Association between maintenance fluid tonicity and hospital-acquired hyponatremia. J. Pediatr. 2013, 163, 1646–1651. [Google Scholar] [CrossRef] [Green Version]
- Mazzoni, M.B.; Milani, G.P.; Bernardi, S.; Odone, L.; Rocchi, A.; D’Angelo, E.A.; Alberzoni, M.; Agostoni, C.; Bianchetti, M.G.; Fossali, E.F. Hyponatremia in infants with community-acquired infections on hospital admission. PLoS ONE 2019, 14, e0219299. [Google Scholar] [CrossRef]
- Arampatzis, S.; Frauchiger, B.; Fiedler, G.-M.; Leichtle, A.B.; Buhl, D.; Schwarz, C.; Funk, G.-C.; Zimmermann, H.; Exadaktylos, A.K.; Lindner, G. Characteristics, symptoms, and outcome of severe dysnatremias present on hospital admission. Am. J. Med. 2012, 125, 1125.e1–1125.e7. [Google Scholar] [CrossRef]
- Huda, M.S.B.; Boyd, A.; Skagen, K.; Wile, D.; Van Heyningen, C.; Watson, I.D.; Wong, S.; Gill, G. Investigation and management of severe hyponatraemia in a hospital setting. Postgrad. Med. J. 2006, 82, 216–219. [Google Scholar] [CrossRef] [Green Version]
- Movig, K.L.L.; Leufkens, H.G.M.; Lenderink, A.W.; Egberts, T.C.G. Validity of hospital discharge International Classification of Diseases (ICD) codes for identifying patients with hyponatremia. J. Clin. Epidemiology 2003, 56, 530–535. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, M.J.; Alcaraz, A.; Solana, M.J.; García, A. Neurological symptoms in hospitalised patients: Do we assess hyponatraemia with sufficient care? Acta Paediatr. 2013, 103, e7–e10. [Google Scholar] [CrossRef] [PubMed]
- Berkman, K.; Haigh, K.; Li, L.; Lockett, J.; Dimeski, G.; Russell, A.W.; Inder, W.J. Investigation and management of moderate to severe inpatient hyponatraemia in an Australian tertiary hospital. BMC Endocr. Disord. 2018, 18, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forryan, J.; Mishra, V. Optimisation of intravenous fluid prescribing: Framework for changing practice through education and audits. BMJ Open Qual. 2017, 6, e000187. [Google Scholar] [CrossRef]
- Powell, A.G.M.T.; Paterson-Brown, S.; Drummond, G. Undergraduate medical textbooks do not provide adequate information on intravenous fluid therapy: A systematic survey and suggestions for improvement. BMC Med Educ. 2014, 14, 35. [Google Scholar] [CrossRef] [Green Version]
- Milani, G.P.; Edefonti, V.; De Santis, R.; Agostoni, C.; Spolidoro, G.C.; Pelucchi, C.; Bianchetti, M.G.; Fossali, E.F. Disagreement between direct and indirect potentiometric Na+ determination in infancy and childhood. Clin. Chem. Lab. Med. 2020, 58, e117–e119. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Fluid Response Choices of the Scenarios * | Sodium Concentration | Tonicity After Injection |
|---|---|---|
| Glucose 5% isotonic | 0 mmol/L | Strongly hypotonic |
| Darrow-glucose | 31 mmol/L | Strongly hypotonic |
| Potassium-sodium-glucose | 40 mmol/L | Strongly hypotonic |
| 0.45% sodium chloride with 2.5% glucose isotonic | 77 mmol/L | Strongly hypotonic |
| Ringer’s acetate | 130 mmol/L | Moderately hypotonic |
| Isotonic saline solution | 154 mmol/L | Isotonic |
| 0.9% NaCl with 5% glucose | 154 mmol/L | Isotonic |
| 3% NaCl | 513 mmol/L | Strongly hypertonic |
| Responded to One or More Scenarios | Responded to All Scenarios | Completed All Questions | ||||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | |
| All | 215 | (100.0) | 201 | (93.4) | 159 | (74.0) |
| Characteristics of respondents | ||||||
| Gender | ||||||
| Female | 126 | (58.6) | 119 | (59.2) | 88 | (55.3) |
| Male | 89 | (41.4) | 82 | (40.8) | 71 | (44.7) |
| Age | ||||||
| 18–34 years | 88 | (40.9) | 80 | (39.8) | 64 | (40.3) |
| 35–44 years | 57 | (26.5) | 54 | (26.9) | 43 | (27.0) |
| ≥45 years | 70 | (32.6) | 67 | (33.3) | 52 | (32.7) |
| Number of weekly treated patients with intravenous fluids | ||||||
| 0 patients | 29 | (13.5) | 28 | (13.9) | 21 | (13.2) |
| 1–5 patients | 72 | (33.5) | 68 | (33.8) | 58 | (36.5) |
| >5 patients | 113 | (52.6) | 104 | (51.7) | 80 | (50.3) |
| Unknown | 1 | (0.5) | 1 | (0.5) | 0 | (0) |
| Years of practice | ||||||
| ≤5 years | 86 | (40.0) | 78 | (38.8) | 61 | (38.4) |
| >5 years | 127 | (59.1) | 121 | (60.2) | 97 | (61.0) |
| Unknown | 2 | (0.9) | 2 | (1.0) | 1 | (0.6) |
| Position | ||||||
| Junior doctor | 121 | (56.3) | 111 | (55.2) | 89 | (56.0) |
| FY1 * | 30 | (14.0) | 25 | (12.4) | 18 | (11.3) |
| FY2 ** | 27 | (12.6) | 26 | (12.9) | 23 | (14.5) |
| Specialty registrar | 50 | (23.3) | 47 | (23.4) | 39 | (24.5) |
| Other *** | 14 | (6.5) | 13 | (6.5) | 9 | (5.7) |
| Senior doctor (Consultant) | 94 | (43.7) | 90 | (44.8) | 70 | (44.0) |
| Characteristics of EDs **** | ||||||
| Size | ||||||
| Large | 84 | (39.1) | 79 | (39.3) | 61 | (38.4) |
| Medium | 111 | (51.6) | 104 | (51.7) | 85 | (53.5) |
| Small | 20 | (9.3) | 18 | (9.0) | 13 | (8.2) |
| Complexity | ||||||
| High | 65 | (30.2) | 62 | (30.8) | 44 | (27.7) |
| Medium | 150 | (69.8) | 139 | (69.2) | 115 | (72.3) |
| Low | 0 | (0) | 0 | (0) | 0 | (0) |
| Type | ||||||
| Combined general population ED ***** | 31 | (14.4) | 29 | (14.4) | 23 | (14.5) |
| Adult ED | 76 | (35.3) | 69 | (34.3) | 52 | (32.7) |
| Pediatric ED | 106 | (49.3) | 101 | (50.2) | 82 | (51.6) |
| Trauma center | 2 | (0.9) | 2 | (1.0) | 2 | (1.3) |
| n | (%) | |
|---|---|---|
| Scenario 1 (n = 201) An otherwise healthy 18-year-old girl is hospitalised on suspicion of meningitis. She has thrown up and has diarrhoea. On examination, she appears pale with cold skin, a slightly increased heart rate, normal blood pressure, and with decreased level of consciousness (Glasgow Coma Scale = score 14). Laboratory tests are normal. | ||
| Correct fluid | ||
| Isotonic saline, [Na+] = 154 mmol/L | 144 | (76.1) |
| Inappropriate fluids | ||
| 0.9% NaCl with 5% glucose, [Na+] = 154 mmol/L | 5 | (2.5) |
| 3% NaCl, [Na+] = 513 mmol/L | 0 | (0) |
| Incorrect hypotonic fluids | ||
| Glucose 5% isotonic | 1 | (0.5) |
| Darrow-glucose, [Na+] = 31 mmol/L | 1 | (0.5) |
| Potassium-sodium-glucose, [Na+] = 40 mmol/L | 14 | (7.0) |
| 0.45% sodium chloride with 2.5% glucose isotonic, [Na+] = 77 mmol/L | 6 | (3.0) |
| Ringer’s acetate, [Na+] = 130 mmol/L | 28 | (13.9) |
| Do not know | 2 | (1.0) |
| Scenario 2 (n = 201) A 5-year-old boy arrives at the emergency department with a head injury after falling from a bike. He has headache and nausea, but no vomiting or signs of hypovolaemia. He has been unconscious for half an hour; however, the CT scan, clinical examination and laboratory results are all normal. | ||
| Correct fluid | ||
| 0.9% NaCl with 5% glucose, [Na+] = 154 mmol/L | 21 | (10.4) |
| Inappropriate fluid | ||
| Isotonic saline, [Na+] = 154 mmol/L | 83 | (41.3) |
| Ringer’s acetate, [Na+] = 130 mmol/L | 22 | (10.9) |
| 3% NaCl, [Na+] = 513 mmol/L | 1 | (0.5) |
| Incorrect hypotonic fluids | ||
| Glucose 5% isotonic | 3 | (1.5) |
| Darrow-glucose, [Na+] = 31 mmol/L | 6 | (3.0) |
| Potassium-sodium-glucose, [Na+] = 40 mmol/L | 42 | (20.9) |
| 0.45% sodium chloride with 2.5% glucose isotonic, [Na+] = 77 mmol/L | 8 | (4.0) |
| Do not know | 15 | (7.5) |
| Scenario 3 (n = 201) A 75-year-old woman arrives at the emergency department with hip fracture after a fall. There are no signs of head injury. The patient has had a poor appetite for a long time. Medical history includes thiazide diuretics for hypertension, but otherwise she is healthy. Clinical examination shows symptoms of hypovolaemia: cold and pale skin, heart rate at 100 bpm, and a slightly increased respiratory rate. Laboratory tests show P-Na = 110 mmol/L. | ||
| Correct fluids | ||
| Isotonic saline, [Na+] = 154 mmol/L | 120 | (59.7) |
| Ringer’s acetate, [Na+] = 130 mmol/L | 16 | (8.0) |
| Inappropriate fluids | ||
| 0.9% NaCl with 5% glucose, [Na+] = 154 mmol/L | 11 | (5.5) |
| 3% NaCl, [Na+] = 513 mmol/L | 16 | (8.0) |
| Incorrect hypotonic fluids | ||
| Glucose 5% isotonic | 4 | (2.0) |
| Darrow-glucose, [Na+] = 31 mmol/L | 0 | (0) |
| Potassium-sodium-glucose, [Na+] = 40 mmol/L | 10 | (5.0) |
| 0.45% sodium chloride with 2.5% glucose isotonic, [Na+] = 77 mmol/L | 7 | (3.5) |
| Do not know | 17 | (8.5) |
| Scenario 4 (n = 201) A 28-year-old woman is hospitalised on suspicion of medication poisoning and large intake of water. She vomits and complains about headaches. She exhibits strange behavior, has muscle rigidity, and a Glasgow Coma Scale score of 14. ABC is normal. Arterial blood gas shows P-Na = 118 mmol/L. | ||
| Correct fluid | ||
| 3% NaCl, [Na+] = 513 mmol/L | 59 | (29.4) |
| Inappropriate fluids | ||
| Isotonic saline, [Na+] = 154 mmol/L | 76 | (37.8) |
| 0.9% NaCl with 5% glucose, [Na+] = 154 mmol/L | 6 | (3.0) |
| Incorrect hypotonic fluids | ||
| Glucose 5% isotonic | 3 | (1.5) |
| Darrow-glucose, [Na+] = 31 mmol/L | 0 | (0) |
| Potassium-sodium-glucose, [Na+] = 40 mmol/L | 12 | (6.0) |
| 0.45% sodium chloride with 2.5% glucose isotonic, [Na+] = 77 mmol/L | 4 | (2.0) |
| Ringer’s acetate, [Na+] = 130 mmol/L | 14 | (7.0) |
| Do not know | 27 | (13.4) |
| n | (%) | |
|---|---|---|
| Q10: Which of the following sentences are correct? (n = 198) | 158 | (79.8) |
| Most often acutely ill patients in need of IV fluids have increased renal water excretion Most often acutely ill patients in need of IV fluids have decreased renal water excretion Most often acutely ill patients in need of IV fluids have normal renal water excretion | ||
| Q11a: How will Darrow-glucose ([Na+] = 31 mmol/L) affect the P-Na in a patient with decreased water excretion? (n = 184) | 85 | (46.2) |
| Large increase in P-Na with a risk of sodium overload Slight increase in P-Na Unchanged Slight decrease in P-Na Large decrease in P-Na with a risk of hyponatriaemia | ||
| Q11b: How will Potassium-sodium-glucose ([Na+] = 40 mmol/L) affect the P-Na in a patient with decreased water excretion? (n = 179) | 56 | (31.3) |
| Large increase in P-Na with a risk of sodium overload Slight increase in P-Na Unchanged Slight decrease in P-Na Large decrease in P-Na with a risk of hyponatriaemia | ||
| Q11c: How will Ringer’s lactate ([Na+] = 130 mmol/L) affect the P-Na in a patient with decreased water excretion? (n = 179) | 43 | (24.0) |
| Large increase in P-Na with a risk of sodium overload Slight increase in P-Na Unchanged Slight decrease in P-Na Large decrease in P-Na with a risk of hyponatriaemia | ||
| Q11d: How will 0.9% NaCl with 5% glucose ([Na+] = 154 mmol/L) affect the P-Na in a patient with decreased water excretion? (n = 176) | 55 | (31.1) |
| Large increase in P-Na with a risk of sodium overload Slight increase in P-Na Unchanged Slight decrease in P-Na Large decrease in P-Na with a risk of hyponatriaemia | ||
| Q12 (n = 173): In case of increased blood sugar (above 12 mmol/L), the measured plasma sodium (P-Na) must be corrected because the measured P-Na is: | 52 | (30.1) |
| “Falsely low” “Falsely high” There is no need for correction Do not know | ||
| Q13: Which of the following diseases/symptoms may be indicative of potentially increased intracranial pressure (ICP)? (n = 164) | 23 | (14.0) |
| Meningitis Shortness of breath Concussion Chest pain Seizure Acute liver failure Acute abdomen Hip fracture | ||
| Q14: Which of the following symptoms are indicative of severe symptoms of hyponatraemia and require acute treatment of hyponatraemia? (n = 163) | 71 | (43.6) |
| Altered level of consciousness Seizure Infection Chest pain Muscle rigidity Anaemia | ||
| Q15a: What is the maximum correction of P-Na for a patient at high risk of osmotic demyelination? (n = 162) | 54 | (33.3) |
| 6 mmol/L 8 mmol/L 16 mmol/L 20 mmol/L | ||
| Q15b: What is the maximum correction of P-Na for a patient without high risk of osmotic demyelination? (n = 162) | 48 | (29.6) |
| 6 mmol/L 8 mmol/L 16 mmol/L 20 mmol/L | ||
| Q16: How would you prevent plasma sodium from rising too rapidly and thus exceeding the recommended limits for P-Na correction? (n = 161) | 62 | (38.5) |
| I record the administration of IV fluids I recommend fluid restriction I record the first low P-Na level I monitor P-Na regularly I administer 5% glucose I record the maximum recommended increase of P-Na I encourage the patient to drink water | ||
| Q17: Which of the following treatments would you initiate if a patient’s plasma sodium raises too rapidly? (n = 159) | 89 | (56.0) |
| Water per os Fluid restriction (fluid intake is limited to less than 1 L/day) Isotonic saline (1 L contains 9 g [154 mmol] sodium chloride) Ringer’s acetate (1 L contains 130 mmol sodium [4.1 g sodium acetate and 5.9 g sodium chloride], 0.295 g calcium chloride, 0.3 g potassium chloride, 0.2 g magnesium chloride) 3% NaCl (1 L contains 30 g [513 mmol] sodium chloride) Glucose 5% isotonic (1 L contains 55 g [278 mmol] glucose) | ||
| Q18: What is the most common cause of over-correction? (n = 159) | 14 | (8.8) |
| Large diuresis Increased sodium secretion Increased water intake Inadequate water intake Increased sodium intake Reduced renal water excretion |
| Variable | Prescribing Practice (Correct Responses) | Odd Ratio | 95%CI | p-Value | |||
|---|---|---|---|---|---|---|---|
| Critical (correct < 2) n (%) | Non-critical (correct ≥ 2) n (%) | ||||||
| Age | |||||||
| 18–34 years | 31 | (38.8) | 49 | (61.3) | 1.4 | 0.8–2.5 | 0.3 |
| ≥35 years | 38 | (31.4) | 83 | (68.6) | (ref *) | ||
| Number of weekly treated patients with intravenous fluids ** | |||||||
| 0–5 patients | 36 | (37.5) | 60 | (62.5) | 1.4 | 0.8–2.4 | 0.3 |
| >5 patients | 32 | (30.8) | 72 | (69.2) | (ref) | ||
| Years of practice ** | |||||||
| ≤5 years | 29 | (37.2) | 49 | (62.8) | 1.2 | 0.6–2.2 | 0.6 |
| >5 years | 40 | (33.1) | 81 | (66.9) | (ref) | ||
| Position *** | |||||||
| Junior | 39 | (35.1) | 72 | (64.9) | 1.1 | 0.6–1.9 | 0.8 |
| Senior | 30 | (33.3) | 60 | (66.7) | (ref) | ||
| Size | |||||||
| Small/Medium | 43 | (35.2) | 79 | (64.8) | 1.1 | 0.6–2.0 | 0.7 |
| Large | 26 | (32.9) | 53 | (67.1) | (ref) | ||
| Complexity | |||||||
| Medium | 52 | (37.4) | 87 | (62.6) | 1.6 | 0.8–3.0 | 0.2 |
| High | 17 | (27.4) | 45 | (72.6) | (ref) | ||
| Type **** | |||||||
| Pediatric ED | 35 | (34.7) | 66 | (65.3) | 1.0 | 0.4–2.4 | 1.0 |
| Adult ED | 23 | (33.3) | 46 | (66.7) | 1.0 | 0.4–2.4 | 0.9 |
| Combined general population ED ***** | 10 | (34.5) | 19 | (65.5) | (ref) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sindahl, P.; Overgaard-Steensen, C.; Wallach-Kildemoes, H.; De Bruin, M.L.; Leufkens, H.G.; Kemp, K.; Gardarsdottir, H. Are Further Interventions Needed to Prevent and Manage Hospital-Acquired Hyponatraemia? A Nationwide Cross-Sectional Survey of IV Fluid Prescribing Practices. J. Clin. Med. 2020, 9, 2790. https://doi.org/10.3390/jcm9092790
Sindahl P, Overgaard-Steensen C, Wallach-Kildemoes H, De Bruin ML, Leufkens HG, Kemp K, Gardarsdottir H. Are Further Interventions Needed to Prevent and Manage Hospital-Acquired Hyponatraemia? A Nationwide Cross-Sectional Survey of IV Fluid Prescribing Practices. Journal of Clinical Medicine. 2020; 9(9):2790. https://doi.org/10.3390/jcm9092790
Chicago/Turabian StyleSindahl, Per, Christian Overgaard-Steensen, Helle Wallach-Kildemoes, Marie Louise De Bruin, Hubert GM Leufkens, Kaare Kemp, and Helga Gardarsdottir. 2020. "Are Further Interventions Needed to Prevent and Manage Hospital-Acquired Hyponatraemia? A Nationwide Cross-Sectional Survey of IV Fluid Prescribing Practices" Journal of Clinical Medicine 9, no. 9: 2790. https://doi.org/10.3390/jcm9092790